B1-insensitive T2 preparation for improved coronary magnetic
advertisement

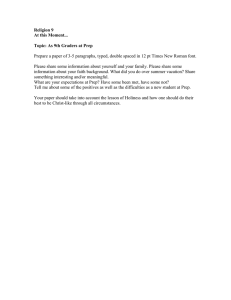
Magnetic Resonance in Medicine 55:858 – 864 (2006) B1-Insensitive T2 Preparation for Improved Coronary Magnetic Resonance Angiography at 3 T Reza Nezafat,1,2 Matthias Stuber,3,4*Ronald Ouwerkerk3 Ahmed M. Gharib,2 Milind Y. Desai,2,3 and Roderic I. Pettigrew2 At 3 T, the effective wavelength of the RF field is comparable to the dimension of the human body, resulting in B1 standing wave effects and extra variations in phase. This effect is accompanied by an increase in B0 field inhomogeneity compared to 1.5 T. This combination results in nonuniform magnetization preparation by the composite MLEV weighted T2 preparation (T2 Prep) sequence used for coronary magnetic resonance angiography (MRA). A new adiabatic refocusing T2 Prep sequence is presented in which the magnetization is tipped into the transverse plane with a hard RF pulse and refocused using a pair of adiabatic fast-passage RF pulses. The isochromats are subsequently returned to the longitudinal axis using a hard RF pulse. Numerical simulations predict an excellent suppression of artifacts originating from B1 inhomogeneity while achieving good contrast enhancement between coronary arteries and surrounding tissue. This was confirmed by an in vivo study, in which coronary MR angiograms were obtained without a T2 Prep, with an MLEV weighted T2 Prep and the proposed adiabatic T2 Prep. Improved quantitative and qualitative coronary MRA image measurement was achieved using the adiabatic T2 Prep at 3 T. Magn Reson Med 55:858 – 864, 2006. Published 2006 Wiley-Liss, Inc.† Key words: coronary MR angiography; T2 prep; adiabatic pulses, 3 T cardiac MR; contrast enhancement Coronary magnetic resonance angiography (MRA) at 1.5 T has shown promise for the assessment of significant coronary artery disease in proximal and mid segments of the coronary arteries (1). However, low signal-to-noise ratio (SNR) limits the utilization of this imaging technique for more distal and branching vessels at 1.5 T (1). At a higher magnetic field strength, an improved SNR is expected. However, the enhanced effect of magnetic field susceptibility leads to off-resonance effects, while B1 inhomogeneity, tissue dielectric constants, body dielectric resonances, and increased specific absorption rate (SAR) are additional limitations that must be considered at higher magnetic 1 Department of Biomedical Engineering, Johns Hopkins School of Medicine, Baltimore, Maryland, USA. 2 National Institutes of Health, Department of Health and Human Services, Bethesda, Maryland, USA. 3 Russell. H. Morgan Department of Radiology and Radiological Sciences, Johns Hopkins School of Medicine, Baltimore, Maryland, USA. 4 Department of Medicine and Department of Electrical and Computer Engineering, Johns Hopkins University Baltimore, Maryland, USA. Grant sponsor: Whitaker Foundation; Grant number: Biomedical Engineering Grant RG-02– 0745; Grant sponsor: Donald W. Reynolds Foundation. *Correspondence to: Matthias Stuber, Johns Hopkins University Medical School Department of Radiology; JHOC 4223 601 North Caroline Street, Baltimore, MD 21287, USA. E-mail mstuber@mri.jhu.edu Received 20 May 2005; revised 5 December 2005; accepted 9 December 2005 DOI 10.1002/mrm.20835 Published online 14 March 2006 in Wiley InterScience (www.interscience. wiley.com). field strength (2– 8). Therefore, to take full advantage of higher field strength and clinically realize the improved SNR, a careful sequence design that minimizes these effects is necessary. Three-dimensional (3D), free-breathing coronary MRA techniques can be used to image the tortuous path of the coronary arterial tree with improved SNR relative to twodimensional (2D) approaches. However, 3D imaging results in a lower contrast between the coronary blood and the myocardium. To overcome this problem, the use of contrast agents (9 –12) or magnetization preparation schemes (13–17) have been proposed. T2 Prep is used in 3D coronary imaging to increase the contrast between the coronary arterial blood-pool and the surrounding tissue (13,17,18). However, increased B1 and B0 inhomogeneities at higher magnetic field strength pose significant challenges to uniform T2 preparation of the magnetization across the imaged volume, thereby limiting the value of coronary MRA in general. Therefore, a novel T2 preparation scheme in which adiabatic pulses are used to achieve B1 and B0 insensitive contrast enhancement was developed. Numerical simulations and an in vivo study were performed to characterize the efficacy of the technique. METHODS Background The T2 Prep sequence as proposed by Brittain et al. (13) was modified to minimize adverse effects of B1 and B0 field inhomogeneities at higher magnetic field strength. Figure 1 shows a schematic of the T2 Prep sequence. The isochromats experience a 90° pulse followed by train of refocusing pulses. The refocusing pulses are weighted in a MLEV opposing phase pairs scheme (19,20) to compensate for RF pulse shape imperfections. Composite refocusing pulses (90°x, 180°y, 90°x) were suggested to provide second-order corrections to variations in B1. A large spoiling gradient was used after the return of the magnetization to its equilibrium to dephase residual transverse magnetization. The degree of insensitivity of this type of T2 Prep sequence to field inhomogeneities depends on the number of the MLEV pulses, with a better response being achieved by using a larger number of pulses (20). However, increasing the number of MLEV weighted composite pulses results in an increase in SAR, precluding the use of a sufficient number of pulses necessary to achieve the desired B0 and B1 insensitivity at high magnetic field strength. Adiabatic RF pulses, characterized by the simultaneous modulation of the RF amplitude and frequency (or phase), are insensitive to B1 and B0 field inhomogeneities (21–28). Adiabatic pulses operate under the classic adiabatic passage principle, which states that the magnetization vectors † Published 2006 Wiley-Liss, Inc. 858 This article is a US Government work and, as such, is in the public domain in the United States of America. T2 Prep for Improved Coronary MRA 859 sequence, the longitudinal magnetization (Mz) is rotated into the transverse plane using a hard RF pulse. The magnetization decays as a function of the relaxation terms of T1 and T2 and precesses for total of TE/4 before experiencing the second RF pulse, an AFP pulse that results in an inversion of spins. However, only the spins in parallel with or anti-parallel to the effective B1 will experience an inversion while the perpendicular spins precess and remain in a plane normal to the effective B1 field. The transverse magnetization dephases during the AFP pulse and the refocused magnetization at TE/2 will have an extra phase at t ⫽ TE/2. The accumulated phase is determined by the duration T of the adiabatic pulse and the effective B1 field Beff(t) during the pulse: FIG. 1. Nonadiabatic T2 preparation sequence: MLEV weighted composite T2 Prep sequence with (a) four and (b) two composite 180°x pulses, each 180°x composite pulse consists of three hard RF pulse (90°x, 180°y, 90°x) parallel and anti-parallel to the effective B1 field stay parallel and anti-parallel, respectively, while magnetization vectors perpendicular to B1 will precess and remain perpendicular to the field. There are a variety of adiabatic modulation functions that satisfy the adiabacity condition such as sin/cos, tan/sec, sech/tanh (29), and numerically optimized modulations (26). One of the most commonly used adiabatic pulses is the Silver–Hoult (hyperbolic secant) (21) pulse in which the RF amplitude, B1(t), and frequency ⌬(t) can be expressed as 冉 冉 冊冊 冉 冉 冊冊 B1共t兲 ⫽ B1maxsech  2t ⫺1 T ⌬共t兲 ⫽ ⌬ maxtanh  1 ⫺ 2t T , [1] [2] in which  is a dimensionless truncation factor, typically set to sech⫺1(0.01) (21), t is time, T is total duration of the pulse, and B1max and ⌬max are the maximum amplitude and frequency modulation, respectively. B1max and ⌬max are determined by bandwidth, SAR deposition, RF amplifier constraints, and adiabacity conditions. Adiabatic fast passage (AFP) and adiabatic half-passage RF pulses are commonly used for in vivo NMR to induce B1 insensitive spin inversion and excitation. These pulses cannot generate plane rotation, in which the magnetization is rotated about an axis. Conolly et al. (22) proposed a low power adiabatic refocusing method in which the echo could be generated by any pair of identical AFP pulses. Using this technique, the second AFP RF pulse fully compensates for the phase variations generated by the first AFP pulse. In this study, we exploit such a pair of adiabatic pulses to achieve a plane rotation in the T2 Prep. ⫽ 冕 T ␥兩B eff共t兲兩dt. [3] 0 This phase dispersion results in a signal loss if the magnetization is returned to the longitudinal axis. However, this can be compensated for by using an additional adiabatic inversion pulse. This pulse is applied TE/2 after the first adiabatic inversion pulse to accomplish a plane rotation. Subsequently, the isochromats return to the longitudinal direction using a tip-up hard-RF pulse (⫺90°x) TE/4 after the second adiabatic pulse. A spoiling gradient is used to dephase all the remaining transverse isochromats (not shown in Fig. 2). Numerical simulations of the Bloch equations [30] were performed to calculate the normalized longitudinal magnetization (Mz/Meq) as a function of offresonance and B1 field variations for both the nonadiabatic and the adiabatic T2 Prep. The MLEV weighted composite T2 Prep sequence (Fig. 1) has duration of TE ⫽ 50 ms, and the simulation was performed for two and four composite refocusing pulses. The RF pulse in the simulation was a rectangular hard pulse with duration of 0.43 and 0.96 ms for a 90 ° and 180 °, respectively, with maximum bandwidth. Similar numerical simulations were performed for the adiabatic T2 Prep sequence shown in Fig. 2 with duration of TE ⫽ 50 ms. The hard RF pulses, similar to one used in the MLEV weighted sequence, were used excitation and tip-up pulses. Adiabatic sech/tanh inversion pulses with a bandwidth of 1 kHz and a duration of 11.2 ms were used. For all simulations, T1 and T2 for arterial blood were 1650 and 100 ms, for venous blood 1575 and 20 ms, and for myocardium 1114 and 55 ms, respectively. All simulations were performed in Matlab (The MathWorks, Natick, MA, USA). Proposed Adiabatic T2 Prep In order to suppress the imaging artifacts associated with MLEV weighted composite T2 Prep in coronary MRA at 3 T, we propose a novel adiabatic T2 Prep. Figure 2 shows a schematic of amplitude (Fig. 2a) and frequency modulations (Fig. 2b) of such an adiabatic T2 Prep. During this FIG. 2. Adiabatic T2 Prep: the T2 preparation sequence consists of a hard pulse excitation with a pair of identical adiabatic inversion pulses to accomplish a plane rotation. Magnetization is returned to its equilibrium by a (⫺90°x) hard pulse. A large spoiling gradient is used in the slice selection direction (after the RF pulses, not shown). 860 FIG. 3. Coronary imaging sequence: a T2 prep is applied followed by a 2D selective navigator and spectrally selective fat-sat. The shading in “Acq.” corresponds to different k-space lines. Nezafat et al. Image analysis was performed on a stand-alone PC, where images were multiplanar reconstructed using the “Soapbubble” tool (35). Contrast-to-noise ratio (CNR) and SNR were quantified for each dataset using the original, nonreformatted images. Regions of interest (ROI) were selected in the proximal right coronary artery for the measurement of the mean blood signal (Sblood) and SD (blood). The mean muscle signal (Smuscle) and its SD (muscle) were obtained from an ROI in the ventricular septum. SNR and CNR were calculated as follows: Imaging Sequence and in Vivo Study The adiabatic T2 Prep with a pair of sech/tanh pulses (typical duration of 12 ms for a maximum B1 of 13.5 T) with variable TE was implemented on a Philips 3 T Intera MR system (Philips Medical Systems, Best, The Netherlands) equipped with Quasar dual gradients (maximum amplitude 80 mT/m, maximum slew rate 200 mT/m/ms), a six-element cardiac phased-array receiver coil, and vector electrocardiographic (VCG) R-wave triggering (31). In vivo right coronary MR angiography was performed on 15 healthy adult subjects (6 males, 29 ⫾ 6 years old) with no known history of cardiovascular disease. Written informed consent was obtained from all participants and the protocol was approved by the NHLBI IRB. A scout scan was acquired for localization and navigator positioning using a gradient echo imaging sequence (18,32). Subsequently, a 3D low-resolution, navigatorgated scan for localization of the coronaries was acquired during free breathing. A 2D-selective RF pulse with 12 revolutions in k-space and a beam radius of 15 mm was used for gating and tracking of respiratory motion (32). The navigator beam was positioned at the dome of the right hemidiaphragm with an acceptance window of 5 mm and RF excitation angle of 30° (34). After the 3D scout scan, an ECG-triggered, segmented steady-state free precession cine images (TR ⫽ 3.8 ms, TE ⫽ 1.8 ms, ␣ ⫽ 45°, and temporal resolution of 39.6 ms) at the level of the proximal-to-mid right coronary artery (RCA) for visual determination of the most quiescent period was added (33). Subsequently, coronary MRA was performed. A schematic of the coronary MRA sequence is shown in Fig. 3. T2 Prep and fat suppression were used for contrast enhancement and realtime navigator technology (5-mm gating window, slice tracking) for respiratory motion compensation. Three sets of 3D segmented gradient echo, VCG-gated, free breathing navigator-gated, and corrected right coronary MRA images were acquired in each volunteer. Images were acquired using the proposed adiabatic T2 Prep, nonadiabatic T2 Prep with two composite 180° pulses (as shown in Fig. 1b), and no T2 Prep for contrast enhancement. A TE of 50 ms was used for both MLEV and adiabatic T2 Prep. Twenty slices with a measured slice thickness of 3 mm and a reconstructed slice thickness of 1.5 mm (zero-filling) were acquired per 3D dataset. Ten RF excitations with a spoiled gradient echo readouts (␣ ⫽ 25 0, TR ⫽ 7.5 ms, TE ⫽ 2.1 ms) were performed during each R–R interval. A field of view (FOV) of 270 ⫻ 270 mm was imaged with a scan matrix of 380 ⫻ 245 leading to an in-plane resolution of 1.1 ⫻ 0.7 mm. The images were reconstructed to a matrix size of 512 ⫻ 512 with a resultant voxel size of 0.53 ⫻ 0.53 ⫻ 1.5 mm3. Sblood blood [4] Sblood⫺Smuscle 0.5⫻(blood⫹muscle) [5] SNR ⫽ CNR ⫽ Special attention was paid to standardize ROI size and placement for better comparison between image sets. Furthermore, vessel sharpness of the proximal segments of right coronary artery was measured utilizing a Deriche algorithm (35). In addition to the quantitative analysis, qualitative visual grading of the images was performed on a consensus reading by three of the authors (R.N., M.Y.D., and M.S.) blinded to the acquisition method. Each 3D data set was graded based on observation of any B1 inhomogeneity artifacts. The image was assigned a grade as follows: (1) major artifacts in the observed FOV and the coronary arteries, (2) major artifacts in FOV with minor or none visible in the coronary arteries, and (3) no observed artifacts. Statistical Analysis A two-tailed, paired sample t test was used for comparing image quality in all the measurements except the visual grading. A paired two-sided Wilcoxon test was performed for the visual grading. A P value of ⬍0.05 was considered statistically significant. RESULTS Figures 4 and 5 demonstrate the longitudinal magnetization, Mz/Meq, calculated from the numerical simulation of the Bloch equations for arterial and venous blood and for the myocardium for two and four MLEV weighted composite refocusing pulses. The colormap in the image corresponds to the normalized longitudinal magnetization after the T2 Prep sequence as a function of off-resonance (x axis) and normalized B1 amplitude (y axis). The B1 amplitude was normalized to that required to achieve a 90° excitation. In an ideal field with no inhomogeneity, the magnetization should return to the equilibrium state (red color) with a loss in magnitude only due to relaxation terms. However, in the presence of inhomogeneity, the isochromats will experience additional gradients that induce more variable longitudinal magnetization after the T2 Prep. These results demonstrate that the magnetization does not consistently and fully return to its equilibrium in the presence of strong B1 inhomogeneity. The myocardium appears to be more sensitive to the field inhomogeneities T2 Prep for Improved Coronary MRA 861 FIG. 4. Mz/Meq after T2 Prep with two composite MLEV weighted refocusing pulses as a function of off-resonance and B1 variations. While in the ideal case Mz/Meq should uniformly return to Meq (red), large variations of the magnetization occur as a function of both B0 and B1 inhomogeneity as shown by the different colors. compared to the arterial blood as seen in Figs. 4a and c and 5a and c. Note that there are regions where magnetization is almost inverted after the preparation sequence (blue shading in Figs. 4 and 5). The comparison between the results shown in Figs. 4 and 5 shows an improvement of the sequence response with respect to field inhomogeneity by increasing the number of refocusing pulses. Results from the simulation of Mz/Meq for the proposed adiabatic T2 Prep are shown in Fig. 6. The results suggest that compared to the MLEV weighted composite T2 Prep, there is less sensitivity to field inhomogeneities. Therefore, the magnetization returns to its equilibrium more uniformly in the presence of field inhomogeneity at 3 T. Sample reformatted images of the RCA of a normal volunteer are shown in Fig. 7. The coronary MRA image in Fig. 7a was acquired without any T2 magnetization preparation sequence. The image shows no B1 inhomogeneity artifacts. However, there is no or minor contrast between coronary arteries and the surrounding tissue. Figure 7b shows the same image acquired with the T2 Prep sequence that includes two MLEV weighted composite refocusing pulses. The result shows an enhancement of the contrast between coronary arteries and the surrounding tissue. However, an enhanced artifact level is also visible in the liver, the myocardium, and the coronary arteries, as indicated by the arrows in Fig. 7b. These banding artifacts originate from the increase in field inhomogeneity at higher magnetic field strength. Figure 7c was acquired with the new adiabatic T2 Prep and the local signal variations are no longer visible. However, the contrast between the coronary arteries and the surrounding tissues is still preserved. Figure 8 shows coronary MR angiograms of an RCA obtained in a healthy adult subject. Nonreformatted slices from the 3D acquisition (Fig. 8a– g) are displayed together with the reformated version obtained from the same data- FIG. 5. Mz/Meq after T2 Prep with four composite MLEV weighted refocusing pulses as a function of off-resonance and B1 variations. When compared to two refocusing pulses, the plot demonstrates an improved insensitivity to magnetic field variations. This is evidenced by the larger homogeneous area in which the magnetization returns to its equilibrium (red color) after the T2 Prep. However, by using four refocusing pulses, the total SAR level increases to ⬎4 W/kg body wt. 862 Nezafat et al. FIG. 6. Mz/Meq after an adiabatic T2 Prep incorporating two adiabatic inversion pulses as a function of off-resonance and B1 variations for three different tissue types. Each adiabatic inversion included a sech/tanh pulse with duration of 11.2 ms and a bandwidth of 1 kHz. The result demonstrates an improved insensitivity to magnetic field inhomogeneity. set (Fig. 8h). Images acquired with the nonadiabatic T2 Prep (with two composite MLEV weighted refocusing pulses) are visualized in Fig. 8 while those obtained using the adiabatic T2 Prep are shown in Fig. 9. An enhanced level of image artifacts can be observed in most of the slices (arrows in Fig. 8a– g) and also in the reformatted version if the nonadiabatic T2 Prep is used. By using the adiabatic T2 Prep, however, a siginificantly reduced artifact level is observed in both the individual slices (Fig. 9a– g) and in the reformatted image (Fig. 9h). Statistical comparisons of both objective and subjective measures are shown in Table 1. When comparing the image data obtained with the nonadiabatic and the new adiabatic T2 Prep, there was a significant increase (P ⬍ 0.002) in the CNR between blood and muscle if the proposed adiabatic T2 Prep was used. Vessel sharpness did not change significantly. Similarly, no significant change in the SNR of the blood at the level of the coronary ostia was found. Consensus visual grading shows significant differences (P ⬍ 0.0001) between the two different techniques and suggests that the proposed adiabatic T2 Prep pulse sequence substantially suppresses the artifacts originating from B1 inhomogeneity. Consistent with earlier finding at 1.5 T, the contrast between blood and muscle was significantly enhanced by adding both nonadiabatic and adiabatic T2 Prep to the sequence. DISCUSSION T2 Prep is commonly used in coronary MRA to improve the CNR and the vessel definition at 1.5 T (18). This se- FIG. 7. Sample reformatted right coronary MR angiography: (a) acquired with no T2 Prep; (b) with two MLEV weighted composite T2 Prep; (c) with adiabatic T2 Prep. Arrows in (b) point to the artifacts resulting from T2 Prep sequence; note the suppression of the banding artifacts in c and also the homogeneity of the signal. quence has been optimized for insensitivity to RF pulse imperfections and off-resonance (13,18) and has been extensively utilized at 1.5 T. To obtain insensitivity to residual field imperfections, this sequence includes four composite refocusing pulses weighted in an MLEV scheme. However, limitations related to SAR do not permit the use of four refocusing pulses unless the maximum amplitude of each hard pulse is substantially reduced. Our simulation demonstrates that even with four refocusing pulses, the sequence still shows sensitivity to field inhomogeneities. Therefore, we proposed a novel T2 Prep sequence in which the refocusing of spins is achieved with two identical adiabatic inversion pulses. In this study, we used hyperbolic secant (sech/tanh) adiabatic pulses as AFP pulses. However, there are various other adiabatic pulse pairs that could potentially be used, but the efficacy of these alternative pulses for contrast enhancement in coronary MRA remains to be investigated. Our simulations suggest that signal suppression might be expected at 420 Hz off-resonance. Therefore, T2 Prep may simultaneously support fat saturation, which is important for coronary MRA (16). However, this remains to be investigated more systematically. Consistent with earlier findings from others at 1.5 T, we also found a 20% reduction in blood signal, and a 30 – 40% improvement in blood-muscle CNR upon comparison of no T2 Prep and both versions of the T2 Prep. While no improvement in vessel sharpness was found when comparing the nonadiabatic T2 Prep versus no T2 Prep, a significant enhancement in vessel sharpness was obtained using the adiabatic T2 Prep. These findings may be attributed to the compromised T2 preparation T2 Prep for Improved Coronary MRA 863 FIG. 8. Right coronary MR angiography images acquired from a normal volunteer with two MLEV weighted composite T2 Prep sequence. Each slice (a– g) was extracted from the 3D imaging data set. The 3D reformatted image is shown in (h). Significant imaging artifact can be observed in the image as shown by arrows. characteristics of the nonadiabatic T2 Prep in the presence of enhanced B1 inhomogeneity. The visual analysis also shows an excellent suppression of the banding artifacts originating from increased field inhomogeneities at 3 T. The SAR of the current coronary MRA sequence (with the imaging parameters used in this study) without a T2 Prep ranges between 0.9 and 1.3 W/kg for a heart rate of 60 to 85 beats per minute. A T2 Prep with an MLEV phase cycling will increase the SAR by approximately 1.8 W/kg with two refocusing pulses and by ⬃3 W/kg with four refocusing pulses. The adiabatic T2 Prep sequence will add 2 W/kg to the total SAR of the sequence. Therefore, the total SAR of the coronary MRA sequence with a nonadiabatic T2 Prep (that includes four refocusing pulses) will exceed the allowed 4 W/kg for human use. The imaging parameters such as TR or maximum amplitude of the transmitted B1 of the body coil can be adjusted in order to decrease the SAR. This decrease in SAR can be exploited to increase the number of pulses in the phase cycling train. However, an increased sensitivity of the pulse to field imperfections must be considered, as shown by the simulation in Fig. 5. CONCLUSIONS In this study, a novel T2 Prep contrast enhancement scheme for free breathing 3D coronary MRA at high magnetic field strength was proposed. This technique includes the use of adiabatic plane rotation pulses and is more insensitive to B1 and B0 inhomogeneities than regular MLEV refocusing schemes. In vivo human coronary MR angiograms were acquired in 15 healthy adult subjects to compare three sets of images including no T2 Prep, nonadiabatic T2 Prep, and the new adiabatic T2 Prep. Consistent with our findings from the numerical simulations, the results suggest that the new technique not only yields an improved blood-muscle CNR similar to the nonadiabatic T2 Prep, but also successfully removes the image artifacts originating from B1 and B0 inhomogeneity without exceeding the SAR limit. FIG. 9. Right coronary MR angiography images acquired from the same volunteer shown in Fig. 8 with the adiabatic T2 Prep sequence. Significant improvement in the quality of the image is achieved by replacing the nonadiabatic T2 Prep with the adiabatic T2 Prep. 864 Nezafat et al. TABLE 1 Statistical Comparison: Effect of Adiabatic T2 Prep, MLEV Weighted Composite T2 Prep (non-adiabatic), and No T2 Prep Sequences on SNR of Blood, CNR of Myocardium-Blood, Vessel Sharpness, and Visual Grading SNRblood CNRblood-muscle Vessel sharpness Visual grading Adiabatic T2 Non-adiabatic T2 No T2 Pc1c2 Pc1c3 Pc2c3 16.54 ⫾ 3.37 14.73 ⫾ 3.36 38.6 ⫾ 4.0 2.93 ⫾ 0.25 16.97 ⫾ 4.21 13.17 ⫾ 4.37 36.5 ⫾ 6.0 1.8 ⫾ 0.56 19.61 ⫾ 4.63 10.40 ⫾ 4.34 32.9 ⫾ 6.0 2.93 ⫾ 0.25 NS NS NS ⬍ 0.0001 ⬍ 0.01 ⬍ 0.002 ⬍ 0.01 NS ⬍ 0.01 ⬍ 0.06 NS ⬍ 0.0001 Note.The visual grading on presence of artifacts is performed by a consensus reading and each image is assigned (1) if there is B1 inhomogeneity artifacts on FOV and coronary arteries (2) if B1 affect the FOV but not coronary arteries (3) no inhomogeneity artifacts. c1, c2, and c3 correspond to the adiabatic T2 Prep, non-adiabatic T2 Prep, and no T2 Prep columns in the table. ACKNOWLEDGMENTS Reza Nezafat gratefully acknowledges the discussion with Dr. Michael Garwood and Dr. Doug Morris on adiabatic pulses and Dr. King Li for providing access to the Philips scanner. Dr. Matthias Stuber is compensated as a consultant by Philips Medical Systems, NL, the manufacturer of the equipment described in this presentation. The terms of this agreement have been approved by the Johns Hopkins University in accordance with its conflict of interest policies. REFERENCES 1. Kim WY, Danias PG, Stuber M, Flamm SD, Plein S, Nagel E, Langerak SE, Weber OM, Pedersen EM, Schmidt M, Botnar RM, Manning WJ. Coronary magnetic resonance angiography for the detection of coronary stenoses. N Engl J Med 2001;345:1863–1869. 2. Wen H, Jaffer FA, Denison TJ, Duewell S, Chesnick AS, Balaban RS. The evaluation of dielectric resonators containing H2O or D2O as RF coils for high-field MR imaging and spectroscopy. J Magn Reson B 1996;110:117–123. 3. Bottomley PA, Andrew ER. RF magnetic field penetration, phase shift and power dissipation in biological tissue: implications for NMR imaging. Phys Med Biol 1978;23:630 – 643. 4. Singerman RW, Denison TJ, Wen H, Balaban RS. Simulation of B1 field distribution and intrinsic signal-to-noise in cardiac MRI as a function of static magnetic field. J Magn Reson 1997;125:72– 83. 5. Schenck JF. Safety of strong, static magnetic fields. J Magn Reson Imaging 2000;12:2–19. 6. Noeske R, Seifert F, Rhein KH, Rinneberg H. Human cardiac imaging at 3 T using phased array coils. Magn Reson Med 2000;44:978 –982. 7. Hinton DP, Wald LL, Pitts J, Schmitt F. Comparison of cardiac MRI on 1.5 and 3.0 Tesla clinical whole body systems. Invest Radiol 2003;38: 436 – 442. 8. Stuber M, Botnar RM, Fischer SE, Lamerichs R, Smink J, Harvey P, Manning WJ. Preliminary report on in-vivo coronary MRA at 3 Tesla in humans. Magn Reson Med 2002;48:425– 429. 9. Goldfarb JW, Edelman RR. Coronary arteries: breath-hold, gadoliniumenhanced, three-dimensional MR angiography. Radiology 1998;206: 830 – 834. 10. Paetsch I, Huber ME, Bornstedt A, Schnackenburg B, Boesiger P, Stuber M, Fleck E, Cavagna F, Nagel E. Improved three-dimensional freebreathing coronary magnetic resonance angiography using gadocoletic acid (b-22956) for intravascular contrast enhancement. J Magn Reson Imaging 2004;20:288 –293. 11. Stuber M, Botnar RM, Danias PG, McConnell MV, Kissinger KV, Yucel EK, Manning WJ. Contrast agent-enhanced, free-breathing, three-dimensional coronary magnetic resonance angiography. J Magn Reson Imaging 1999;10:790 –799. 12. Green JD, Schirf BE, Omary RA, McCarthy RM, Carr JC, Li D. Projection imaging of the right coronary artery with an intravenous injection of contrast agent. Magn Reson Med 2004;52:699 –703. 13. Brittain JH, Hu BS, Wright GA, Meyer CH, Macovski A, Nishimura DG. Coronary angiography with magnetization-prepared T2 contrast. Magn Reson Med 1995;33:689 – 696. 14. Li D, Paschal CB, Haacke EM, Adler LP. Coronary arteries: threedimensional MR imaging with fat saturation and magnetization transfer contrast. Radiology 1993;187:401– 406. 15. Stuber M, Botnar RM, Spuentrup E, Kissinger KV, Manning WJ. Threedimensional high-resolution fast spin-echo coronary magnetic resonance angiography. Magn Reson Med 2001;45:206 –211. 16. Edelman RR, Manning WJ, Burstein D, Paulin S. Coronary arteries: breath-hold MR angiography. Radiology 1991;181:641– 643. 17. Shea SM, Deshpande VS, Chung YC, Li D. Three-dimensional true-fisp imaging of the coronary arteries: improved contrast with T2-preparation. J Magn Reson Imaging 2002;15:597– 602. 18. Botnar RM, Stuber M, Danias PG, Kissinger KV, Manning WJ. Improved coronary artery definition with T2-weighted, free-breathing, three-dimensional coronary MRA. Circulation 1999;99:3139 –3148. 19. Shaka AJ, Rucket SP, Pines A. Iterative Carr–Purcell trains. J Magn Reson 1988;77:606 – 612. 20. Levitt M, Freeman R, Frenkiel T. Broadband heteronuclear decoupling. J Magn Reson 1982;47:328 –330. 21. Silver MS, Joseph RI, Hoult DI. Highly selective /2 and pulse generation. J Magn Reson 1984;59:347–351. 22. Conolly S, Glover G, Nishimura D, Macovski A. A reduced power selective adiabatic spin-echo pulse sequence. Magn Reson Med 1991; 18:28 –38. 23. Garwood M, Ugurbil KB. 1 insensitive adiabatic RF pulses. NMR Basic Princ Progr 1992;26:109 –147. 24. de Graaf RA, Nicolay K. Adiabatic RF pulses: applications to in-vivo NMR. Concepts Magn Reson 1997;9:247–268. 25. Garwood M, DelaBarre L. The return of the frequency sweep: designing adiabatic pulses for contemporary NMR. J Magn Reson 2001;153:155–177. 26. Ugurbil K, Garwood M, Rath AR, Bendall MR. Amplitude and frequency/phase modulated refocusing pulses that induce plane rotation even in the presence of inhomogeneous B1 fields. J Magn Reson 1988;78:472–497. 27. Conolly S, Nishimura D, Macovski A. Sweep-diagram analysis of selective adiabatic pulses. J Magn Reson 1989;83:549 –564. 28. Kim D, Cernicanu A., Axel L, B0 and B1 insensitive saturation pulse for accurate T1 estimation for first-pass perfusion MRI, In: Proceedings of the 13th Annual Meeting of ISMRM, Miami, 2006. p 520. 29. Ugurbil K, Garwood M, Robin Bendall M. Amplitude- and frequencymodulated pulses to achieve 90° plane rotations with inhomogeneous B1 fields. J Magn Reson 1987;72:177–185. 30. Bloch F. Nuclear induction. Phys Rev 70:460 – 474, 1946. 31. Fischer SE, Wickline SA, Lorenz CH. Novel real-time R-wave detection algorithm based on the vector cardiogram for accurate gated magnetic resonance acquisitions. Magn Reson Med 1999;42:361–370. 32. Stuber M, Botnar RM, Danias PG, Sodickson DK, Kissinger KV, Van CM, De BJ, Manning WJ. Double-oblique free-breathing high resolution three-dimensional coronary magnetic resonance angiography. J Am Coll Cardiol 1999;34:524 –531. 33. Wang Y, Vidan E, Bergman GW. Cardiac motion of coronary arteries: variability in the rest period and implications for coronary MR angiography. Radiology 1999;213:751–758. 34. Oshinski JN, Hoffand L, Mukundan S, Dixon WJ, Parks WJ, Pettigrew RI. Two-dimensional coronary MR angiography without breath holding. Radiology 1996;201:737–743. 35. Etienne A, Botnar RM, Van Muiswinkel AM, Boesiger P, Manning WJ, Stuber M. “soap-bubble” visualization and quantitative analysis of 3D coronary magnetic resonance angiograms. Magn Reson Med 2002;48: 658 – 666.