Development of Low-Frequency Tone Burst versus the Click
advertisement

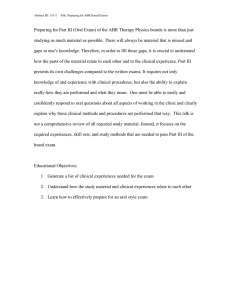
J Am Acad Audiol 16:114–121 (2005) Development of Low-Frequency Tone Burst versus the Click Auditory Brainstem Response Raymond M. Hurley* Annette Hurley† Charles I. Berlin‡ Abstract Often ABR threshold testing employs clicks to assess high-frequency hearing, and low-frequency tone bursts to assess low-frequency sensitivity. While a maturation effect has been shown for click stimuli, similar data are lacking for low-frequency toneburst stimuli. Thus, 305 infants ranging in conceptional age (CA) from 33 weeks to 74 weeks were tested. Absolute latencies were measured for wave V at 55, 35, and 25 dB nHL in response to a click and for wave V500 in response to a 500 Hz tone burst. Major wave latency in response to 500 Hz tone bursts decreases with age and do not stabilize by 70 weeks CA. Likewise, waves III and V latencies in response to clicks decrease with age, as has been reported by others, and do not stabilize by 70 weeks CA. Wave I latency produced by clicks did not decrease with age, being mature by 33 weeks CA. Key Words: Auditory brainstem response, auditory development, click, tone bursts Abbreviations: ABR = Auditory brainstem response; CA = conceptional age Sumario A menudo, la evaluación de umbrales de ABR emplea clicks para estimar la audición en altas frecuencias y bursts tonales de baja frecuencia para la sensibilidad en las bajas frecuencias. En tanto que se ha mostrado un efecto de maduración para los estímulos de tipo click, se carece de datos similares para los estímulos de tipo burst tonal de baja frecuencia. Así, se evaluó a 305 infantes con edad de concepción (CA) de 33 a 74 semanas. Se midieron las latencias absolutas para la onda V a 55, 35 y 25 dB nHL en respuesta a un click, y para la onda V500 en respuesta a un burst tonal de 500 Hz. La latencia de las ondas principales en respuesta a los bursts tonales de 500 Hz disminuyó con la edad y no se estabiliza antes de la semana 70 de CA. Asimismo, las latencias de las ondas III y V en respuesta a clicks disminuyen con la edad, como ha sido reportado por otros, y no se estabiliza antes de la semana 70. La latencia de la onda I producida por clicks no disminuye con la edad, alcanzando la madurez a la semana 33 de CA. Palabras Clave: Respuesta auditiva del tallo cerebral, desarrollo auditivo, click, bursts tonales Abreviaturas: ABR = respuesta auditiva de tallo cerebral, CA = edad de concepción *Department of Communication Sciences and Disorders, University of South Florida; †Department of Communication Disorders, Louisiana State University Health Sciences Center; ‡Kresge Hearing Research Laboratory, Department of Otorhinolaryngology and Biocommunication, Louisiana State University Health Sciences Center Raymond M. Hurley, Ph.D., Department of Communication Sciences and Disorders, University of South Florida, 4202 East Fowler Avenue—PCD 1017, Tampa, FL 33620-8150; Phone: 813-974-9784; Fax: 813-974-0822; E-mail: rhurley@chuma1.cas.usf.edu 114 Development of ABR/Hurley et al A uditory brainstem response (ABR) testing has been widely used to assess peripheral auditory sensitivity and synchrony in neonates and infants. Often ABR testing employs clicks to assess highfrequency hearing (2000–4000 Hz), and lowfrequency tone bursts (500 Hz) to assess lowfrequency hearing (Hood, 1998; Goldstein and Aldrich, 1999; Sininger and Cone-Wesson, 2002). A click-produced ABR does not just represent hearing in the 2000–4000 Hz zone of the cochlea but is an excellent (r = .98) predictor of average hearing loss (Sininger and Abdala, 1996). Further, a click ABR corresponds best to the zone of hearing above 500 Hz (Sininger and Cone-Wesson, 2002); however, the contour of a hearing loss cannot be ascertained by a click-produced ABR alone. To estimate low-frequency sensitivity and hearing loss contour, a low-frequency test paradigm must be utilized. Common paradigms to access more frequency-specific hearing include the derived band procedure (Ponton et al, 1992), tone bursts with a Blackman windowing function (Gorga et al, 1987; Gorga et al, 1988; Gorga et al, 1989), and tone burst in notched noise (Stapells et al, 1995; Sininger et al, 1997). The derived band procedure provides excellent frequency specificity but is time-consuming and can lack response clarity; thus, it has fallen out of favor, being replaced by the use of tone bursts. While some investigators recommend the use of tone bursts tapered by a Blackman gating function (Gorga et al, 1988; Gorga and Thornton, 1989; Hurley et al, 1996), others favor tone bursts in notched noise for improved frequency specificity (Picton et al, 1979; Purdy et al, 1989; Stapells et al, 1990; Stapells et al, 1995). Like a click-produced ABR, a toneburst ABR is an excellent (r = .94–.97) predictor of hearing at the nominal toneburst frequencies in neonates and infants (Stapells et al, 1995; Sininger et al, 1997). Numerous reports have shown a maturation effect of the ABR from birth to approximately two years of age when using click stimuli (Hecox and Galambos, 1974; Mokotoff et al, 1977; Cox et al, 1981; Salamy, 1984; Rotteveel et al, 1986; Gorga et al, 1987; Gorga et al, 1989; Ponton et al, 1992). However, similar data are lacking for lowfrequency stimuli, that is, 500 Hz. Further, there are conflicting data concerning frequency specific development with one data set (Ponton et al, 1992; Sininger et al, 1997), suggesting that low-frequency sensitivity development occurs more slowly than midfrequency sensitivity development, while other data sets (Teas et al, 1982; Folsom and Wynne, 1986) suggest that frequency development occurs more rapidly for lower than for higher frequency stimulation. Age-equivalent ABR norms are important when predicting hearing levels in neonates and infants. Moreover, because the ABR is a test of neurosynchrony, delayed absolute latencies can often indicate other pathologies or unique conditions (Murray, 1988; Sininger et al, 1995; Starr et al, 1996; Berlin et al, 1998). Therefore, it is useful to have ageequivalent norms for low-frequency toneburst stimuli. In the present paper, we provide age-equivalent norms for a 500 Hz toneburst evoked ABR obtained from a large group of children ranging in conceptional age from 33 weeks to 74 weeks and compare these toneburst norms to age-equivalent norms for click-evoked ABR. In addition, we investigate further the issue of low-frequency sensitivity development. METHODS Subjects Three hundred five infants ranging in conceptional age (CA) from 33 weeks to 74 weeks were referred for ABR testing as they had met with one or more high risk factors for hearing loss. CA was determined by adding the gestational age (GA) and the elapsed time from birth to ABR testing. GA was based on neuromuscular and physical maturity (Dubowitz et al, 1970; Ballard et al, 1977). Because of the previously reported lack of independent latency values between ears (Gorga et al, 1987), correlation analyses were carried on four ABR parameters and are displayed in Table 1. While these correlation values are not as high and consistent as previously reported (Gorga et al, 1987), they do demonstrate the lack of ear independence and support using the latency value obtained from only one ear. Thus, only the latency data from the right ear were used for analyses. All infants had ABR responses at 25 dB nHL to clicks. The infants were divided into 11 CA groups as outlined in Table 2. For comparison purposes, ABR data were obtained from 20 subjects, 22–30 years of 115 Journal of the American Academy of Audiology/Volume 16, Number 2, 2005 Table 1. Latency Correlation Values between the Right and Left Ears at 55 dB nHL ABR Parameter Correlation Wave I Latency 0.65 Wave III Latency 0.76 Wave V Latency 0.86 Wave V500 0.76 age, with HTLs ≤10 dB for the octave frequencies of 250–8000 Hz. Procedures The infants were tested in a sedated stable physiological state just prior to hospital discharge and were medically cleared of middle ear disease. Testing was performed in a quiet test room using Nicolet Pathfinder II and Spirit evoked potential systems. The stimuli were 75, 55, 35, and 25 dB nHL (re: 30 dB peak equivalent SPL) condensation 100 µsec clicks at a rate of 27.7/sec with the filter band pass at 100–3000 Hz and the time base at 12–15 msec. For the 500 Hz toneburst testing, the band pass was 30–1500 Hz with a 15 msec time base. The stimuli were 75, 55, 45, and 35 dB nHL alternating 500 Hz bursts having a "2-0-2" cycle envelope using a Blackman gating function at a rate of 27.7/sec. All ABRs were two-channel recordings from Cz-A2 and Cz-A1. Each ABR was replicated and the result of 1500 stimulus presentation. Testing 20 young adults with normal hearing (thresholds for 500–8000 Hz were ≤10 dB HL) indicated that the average and modal psychophysical threshold for the 500 Hz ABR stimuli was 25 dB HL, which is consistent with other reported psychophysical thresholds at 500 Hz for similar toneburst durations (Beattie and Boyd, 1985; Purdy et al, 1989). The reason that toneburst ABR threshold estimates do not often match psychophysical thresholds as depicted on the audiogram, particularly at 500 Hz, is related to stimulus duration. Data collected with standard audiometric procedures use relatively long duration stimuli compared to the short duration stimuli used to obtain ABRs. Signal duration needs to be approximately 200 msec for the lowest hearing thresholds as stimulus duration interacts with threshold because of temporal integration. The default dB nHL reference values provided by the manufacturer were obtained using a stimulus envelope different than the optimal one for toneburst ABR testing. For example, Nicolet’s dB nHL values were obtained using stimuli with a 5-10-5 cycle envelope, which for 500 Hz means a stimulus duration of 40 msec. In contrast, our 500 Hz toneburst stimuli had a 4 msec rise/fall and a zero plateau for a total duration of 8 msec. Thus, temporal integration factors account for the elevation in tone psychophysical threshold; however, stimulus presentation rate does not appear to significantly alter psychophysical threshold Table 2. Breakdown of Infant Groups by Conceptional Age and Number of Infants in Each Group 116 Conceptional Age Number in Group 33–36 wks 27 37–38 wks 27 39–40 wks 27 41–42 wks 44 43–44 wks 32 45–47 wks 26 48–50 wks 25 51–55 wks 24 56–60 wks 25 61–65 wks 24 66–74 wks 24 Development of ABR/Hurley et al a b Figure 1. (a) Comparison of our present click stimulus wave V latency data to previously published data for 33–40 weeks conceptional age (Gorga et al, 1987, 1989). (b) Comparison of present click stimulus wave V latency data to previously published data for 41–65 weeks conceptional age (Gorga et al, 1987, 1989). if the rate is kept between 10/sec and 40/sec (Stapells et al, 1985; Purdy et al, 1989). If the default dB nHL values were adjusted to the psychophysical threshold for our shorter duration tone burst, 75, 55, and 45 dB nHL would be 55, 35, and 25 dB nHL, respectively. In order to remain consistent with the click reference values, we will use the adjusted dB HL values throughout this paper. RESULTS I n order to insure that our data were consistent with previously published data, we compared our click stimulus wave V latency data to previously published data (Gorga et al, 1987, 1989). These graphic comparisons are displayed in Figure 1. In reviewing this figure, note that for all age groups our wave V latency data falls well within the mean (±2 SDs) of the previous data (Gorga et al, 1987, 1989). Thus, we feel confident that our data were obtained from a representative sample of neonates. Absolute latencies were measured for waves I, III, and V at 75 and 55 dB nHL and for wave V at 35 and 25 dB nHL in response to a click, and for wave V at 55, 35, and 25 dB nHL in response to a 500 Hz tone burst. The mean latency data were analyzed by CA group for significant changes using an analysis of variance (ANOVA) with the post 117 Journal of the American Academy of Audiology/Volume 16, Number 2, 2005 Table 3. Mean (SD) Latency Values by Conceptional Age (CA) for Click and 500 Hz Toneburst Stimuli CA Click 75 dB Click 55 dB Click 35 dB Click 25 dB .5k 55 dB .5k 35 dB .5k 25 dB 35 7.33 (0.41) 7.96 (0.47) 8.78 (0.15) 9.50 (0.70) 9.35 (0.73) 10.91 (0.82) 14.42 (0.48) 37 7.29 (0.46) 7.81 (0.46) 8.62 (0.47) 9.35 (0.60) 9.60 (0.53) 11.47 (0.84) 13.83 (0.70) 39 7.05 (0.40) 7.56 (0.38) 8.43 (0.64) 9.08 (0.61) 9.37 (0.75) 11.26 (0.61) 13.03 (0.47) 41 6.94 (0.35) 7.56 (0.39) 8.29 (0.40) 8.98 (0.54) 9.27 (0.61) 10.85 (0.92) 13.11 (1.33) 43 6.90 (0.38) 7.41 (0.40) 8.22 (0.46) 8.84 (0.58) 9.21 (0.71) 10.90 (0.84) 12.85 (0.96) 45 6.90 (0.38) 7.48 (0.38) 8.32 (0.42) 9.02 (0.52) 9.35 (0.52) 11.28 (0.86) 14.11 (0.74) 48 6.70 (0.31) 7.16 (0.41) 8.03 (0.57) 8.58 (0.65) 8.95 (0.71) 10.82 (1.06) 14.03 (1.19) 51 6.64 (0.46) 7.20 (0.48) 7.87 (0.64) 8.47 (0.76) 8.82 (0.70) 10.42 (0.99) 13.14 (0.57) 56 6.40 (0.36) 7.00 (0.31) 7.71 (0.44) 8.36 (0.50) 8.64 (0.45) 10.33 (0.74) 13.83 (1.09) 61 6.44 (0.41) 7.00 (0.42) 7.77 (0.50) 8.41 (0.72) 8.70 (0.52) 10.60 (0.98) 13.04 (1.42) 70 6.23 (0.33) 6.97 (0.38) 7.89 (0.40) 8.60 (0.48) 8.61 (0.50) 10.55 (0.73) 13.00 (0.98) hoc analyses utilizing the Scheffé procedure and the alpha level set at <0.01. Table 3 lists the means (±1 SDs) of wave V data by conceptional age for the click and 500 Hz toneburst stimuli. To determine if the latency values were normally distributed for each CA group at 55 dB nHL, the data were analyzed using the Kolmogorov-Smirnov Figure 2. Mean (±1 SD) latency of waves I, III, and V for a click, and wave V500 for a 500 Hz tone burst at 55 dB nHL. 118 statistic. The results of these analyses were not significant (p = > 0.50), indicating that the distributions for each CA were not different from normal. The latency values of waves I, III, and V at 55 dB nHL are displayed in Figure 2. Note the significant (F = 18.86, p < 0.0001) decrease in wave V latency until after 70 weeks CA. Further note the significant (F = 3.98, p < 0.01) decrease in wave III latency until 70 weeks CA. Wave I latency did not significantly (F = 0.98, p > 0.05) change across all the age groups. Thus, waves III and V do not reach maturity until after 70 weeks CA while wave I is mature by 36 weeks CA. Additionally, Figure 2 displays the latency values for the 500 Hz toneburst stimuli at 55 dB nHL. Wave V latency for the 500 Hz tone burst significantly (F = 6.83, p < 0.0001) decreases until 61 weeks CA. Figure 3 shows the individual latency values for waves I, III, and V, and 500 Hz for wave V plotted as a function of CA. Linear regression analyses indicated the r2 values to be 0.06, 0.22, and 0.38, respectively, for waves I, III, and V, produced by a click, and 0.28 for wave V produced by the 500 Hz tone burst. Since wave I latency did not significantly change across the CA groups, the low r2 value is not unexpected. However, the remaining r2 values indicate that CA is not heavily accountable for the recorded variance in latency values across CAs for waves III and V and the 500 Hz tone burst. Figure 4 Development of ABR/Hurley et al Figure 3. Scattergrams of the latency values for waves I, III, and V at 55 dB nHL and the latency values for wave V500 at 55 dB nHL. Figure 4. The best-fit functions from Figure 3 replotted on log-linear coordinates. displays the best-fit functions from Figure 3 replotted on log-linear coordinates. The slopes of these lines indicate that the rate of maturation of wave V for both click and 500 Hz tone burst is the same while wave III maturation proceeds at a different rate. Again, the flatness of the wave I log-linear best-fit line is consistent with a nonmaturation cochlear development. In order to determine whether intensity affects the developmental sequence, the wave V latency/intensity functions produced by click stimuli for the CA groups were analyzed at lower intensity levels. These data are displayed in Figure 5. While the characteristics of these latency/intensity functions follow the predicted developmental sequence at all intensity levels, at higher intensity levels, the decrease in wave V latency becomes significant at an earlier CA Figure 5. Mean wave V latency/intensity functions by conceptional age group for click stimuli. Figure 6. Mean wave V500 latency/intensity functions by conceptional age group. 119 Journal of the American Academy of Audiology/Volume 16, Number 2, 2005 than at lower intensity levels. Similarly, in order to determine whether intensity affects the developmental sequence for the 500 Hz tone burst, the wave V500 latency/intensity functions by CA groups were analyzed at lower intensity levels. These data are displayed in Figure 6. There is a significant (F = 3.45, p < 0.01) decrease in latency at 55 and 35 dB nHL until after 70 weeks CA. Thus, the latency/intensity functions for the 500 Hz tone burst follow a predicted developmental sequence at 55 and 35 dB nHL but not at 25 dB nHL. In fact, groups of older infants had longer latencies than their younger counterparts at 25 dB nHL. Again, these data suggest the need for a large normative latency range at or near threshold. DISCUSSION with previously reported data (Gorga et al, 1987). The finding that wave III latency does decrease with age, being mature by 70 weeks CA, may be a new finding as we are not aware of any previously reported data on wave III development. Lastly, our data appear to be consistent with the model that the auditory development of the brain stem proceeds from peripheral to central, and proceeds from inferior to superior. Acknowledgment. Thank you to Tracey W. Smith for her help in obtaining these data and Richard A. Roberts for his comments on a previous version of this paper. Annette Hurley and Charles I. Berlin were supported by NIH-NIDCD P01-DC00379, and Raymond M. Hurley was supported by TC2 DC 00007 during the data collection phase of this investigation. Further, this investigation was supported by the Kam's Fund for Hearing Research. T his investigation had three purposes: (1) to provide age-equivalent norms for a 500 Hz toneburst evoked ABR obtained from a large group of infants; (2) to compare these toneburst norms to age-equivalent norms for click evoked ABR; and (3) to investigate the issue of low-frequency sensitivity development. Wave V500 latency in response to 500 Hz tone bursts decreased with age and did not stabilize by 70 weeks CA. Wave V latency in response to clicks decreased with age, as has been reported by others (Gorga et al, 1987; Gorga et al, 1989; Ponton et al, 1992), and did not stabilize by 70 weeks CA. These results are consistent with other investigations, which suggest a progressive decrease in wave V latency until 18–24 months of age postdelivery (Hecox and Galambos, 1974; Gorga et al, 1987, 1989; Ponton et al, 1992). Specifically, the data of Gorga et al (1987, 1989) and Ponton et al (1992) show that wave V latency stabilizes by 23–24 months postbirth, while the data of Hecox and Galambos (1974) show that wave V stabilizes by 18 months postbirth. The finding that wave V latency for clicks and lowfrequency tone bursts develop at the same rate is in keeping with other reports (Ponton et al, 1992; Sininger et al, 1997). While the Sininger et al (1997) paper does not directly address the development issue, Ponton and colleagues (1992) show that low-frequency toneburst development is complete by 23 months postbirth. Wave I latency produced by clicks did not decrease with age; it was mature by 33 weeks CA, which is consistent 120 REFERENCES Ballard JL, Kazmaier K, Drive M. (1977) A simplified assessment of gestational age. Pediatr Res 11:374. Beattie RC, Boyd RL. (1985) Early/middle evoked potentials to noise bursts in quiet, white noise and notched noise. Audiology 24:406–419. Berlin CI, Bordelon J, St. John P, Wilensky D, Hurley A, Kluka E, Hood LJ. (1998) Reversing click polarity may uncover auditory neuropathy in infants. Ear Hear 19:37–47. Cox C, Hack M, Metz D. (1981) Brainstem evoked response audiometry: normative data from the preterm infant. Audiology 20:53–64. Dubowitz LM, Dubowitz V, Goldberg C. (1970) Clinical assessment of gestational age in the newborn infant. J Pediatr 77:1–10. Folsom RC, Wynne MK. (1986) Auditory brain stem responses from adults and infants: restriction of frequency contribution by notched-noise-masking. J Acoust Soc Am 81:1057–1064. Goldstein R, Aldrich WM. (1999) Evoked Potential Audiometry. Boston: Allyn and Bacon. Gorga MP, Kaminski JR, Beauchaine KL, Jesteadt W. (1988) Auditory brainstem responses to tone bursts in normally hearing subjects. J Speech Hear Res 31:87–97 Gorga MP, Kaminski JR, Beauchaine KL, Jesteadt W, Neely ST. (1989) Auditory brainstem responses from children three months to three years of age: normal patterns of response II. J Speech Hear Res 32:281–288. Development of ABR/Hurley et al Gorga MP, Reiland JK, Beauchaine KA, Worthington DW, Jesteadt W. (1987) Auditory brainstem responses from graduates of an intensive care nursery: normal patterns of response. J Speech Hear Res 30:311–318. Gorga MP, Thornton AR. (1989) The choice of stimuli for ABR measurements. Ear Hear 10:217–230. Hecox K, Galambos R. (1974) Brainstem auditory evoked response in human infants and adults. Arch Otolaryngol 99:30–33. Hood L. (1998) Clinical Applications of the Auditory Brainstem Response. San Diego: Singular Publishing Group. Hurley RM, Sells JP, Morehouse CR, Terral C, Spencer C. (1996) Auditory brain stem response (ABR) thresholds for tone bursts and tone bursts in notched noise. Paper presented at the annual meeting of the American Academy of Audiology, Salt Lake City. Mokotoff B, Schulman-Galambos C, Galambos R. (1977) Brain stem auditory evoked responses in children. Arch Otolaryngol 103:38–43. Murray AD. (1988) Newborn auditory brainstem evoked responses (ABRs): longitudinal correlates in the first year. Child Dev 59:1542–1554. Audiology. Philadelphia: Lippincott Williams and Wilkins, 298–322. Sininger YS, Hood LJ, Starr A, Berlin CI, Picton TW. (1995) Hearing loss due to auditory neuropathy. Audiol Today 7:10–13. Stapells DR, Gravel JS, Martin BA. (1995) Thresholds for auditory brainstem responses to tones in notched noise from infants and young children. Ear Hear 16:361–371. Stapells DR, Picton TW, Durieux-Smith A, Edwards CG, Morgan LM. (1990) Thresholds for short-latency auditory evoked potentials to tones in notched noise in normal-hearing and hearing-impaired subjects. Audiology 29:262–274. Stapells DR, Picton TW, Perez-Abalo M, Read D, Smith A. (1985) Frequency specificity in evoked potential audiometry. In: Jacobson JT, ed. The Auditory Brainstem Response. San Diego: College-Hill Press, 147–177. Starr A, Picton TW, Sininger YS, Hood LJ, Berlin CI. (1996) Auditory neuropathy. Brain 119:741–753. Teas DC, Klein AJ, Kramer SJ. (1982) An analysis of auditory brainstem responses in infants. Hear Res 7:19–54. Picton TW, Ouellette J, Hamel G, Smith AD. (1979) Brainstem evoked potentials to tone pips in notched noise. J Otolaryngol 8:289–314. Ponton CW, Eggermont JJ, Coupland SG, Winkelaar R. (1992) Frequency-specific maturation of the eight nerve and brain-stem auditory pathway: evidence from derived auditory brain-stem responses (ABRs). J Acoust Soc Am 91:1576–1586. Purdy SC, Houghton JM, Keith WJ, Greville KA. (1989) Frequency specific auditory brain responses effective masking levels and relationship to behavioral thresholds in normal-hearing adults. Audiology 28:82–91. Rotteveel JJ, Colon EJ, Notermans SLH, Stoelinga GBA, Visco Y, Graaf R. (1986) The central auditory conduction at term date and three months after birth. Scand Audiol 15:11–19. Salamy A. (1984) Maturation of the auditory brainstem response from birth through early childhood. J Clin Neurophysiol 1:293–329. Sininger YS, Abdala C. (1996) Hearing threshold as measured by auditory brain stem response in human neonates. Ear Hear 17:395–401. Sininger YS, Abdala C, Cone-Wesson B. (1997) Auditory threshold sensitivity of the human neonate as measured by the auditory brainstem response. Hear Res 104:27–38. Sininger YS, Cone-Wesson B. (2002) Threshold prediction using auditory brainstem response and steady-state evoked potentials with infants and young children. In: Katz J, ed. Handbook of Clinical 121