1425
Fish Oil Improves Arterial Compliance in
Non-Insulin-Dependent Diabetes Mellitus
Gary E. McVeigh, Geraldine M. Brennan, Jay N. Cohn, Stanley M. Finkelstein,
Randal J. Hayes, George D. Johnston
Downloaded from http://atvb.ahajournals.org/ by guest on October 2, 2016
Abstract In a double-blind, placebo-controlled study we
investigated the effects of dietary fish oil supplementation on
arterial wall characteristics in 20 patients with non-insulindependent diabetes mellitus. Estimates reflecting compliance
values in the large arteries and more peripheral vasculature, as
measured by pulse-contour analysis, improved significantly
after 6 weeks of fish oil therapy compared with values recorded
at baseline and after 6 weeks' administration of olive oil. The
large-artery compliance estimate increased from 1.50 (confidence interval [CI], 1.31 to 1.69) mL/mm Hg at baseline to 1.68
(CI, 1.52 to 1.84) mL/mm Hg after fish oil administration
(P<.01). The oscillatory compliance value increased from
0.015 (CI, 0.011 to 0.019) mL/mm Hg at baseline to 0.022 (CI,
0.016 to 0.028) mL/mm Hg after fish oil ingestion (P<.05). No
changes occurred in arterial blood pressure, cardiac output,
stroke volume, or systemic vascular resistance with either
intervention. The improved compliance estimates with fish oil
ingestion occurred without altering fasting blood glucose and
cholesterol concentrations. These results support the hypothesis that fish oils alter vascular reactivity and favorably influence arterial wall characteristics in patients with non-insulindependent diabetes mellitus. These direct vascular effects,
expressed at the level of the vessel wall, may contribute to the
cardioprotective actions of fish oil in humans. (Arterioscler
Thromb. 1994;14:1425-1429.)
T
contour.7'8 Changes in waveform morphology that occur
with disease and with pharmacologic interventions can
be quantified by pulse-contour analysis and reflect alterations in the compliance characteristics of the arterial system.910 Such changes in arterial compliance may
provide an index of early vascular damage that predisposes affected individuals to the development of major
vascular disease. Fish oil therapy can influence vascular
tone and reactivity and alter the functional properties of
the systemic circulation,1113 and changes in vascular
tone influence the compliance characteristics of the
arterial blood vessels.14 We therefore investigated the
effects of dietary fish oil administration on arterial
compliance estimates in patients with non-insulin-dependent diabetes mellitus (NIDDM) by using the pulsecontour analysis technique.
he metabolic abnormalities associated with diabetes mellitus produce structural and functional changes in the arterial vasculature that
account for the increased cardiovascular morbidity
found in diabetic subjects. The accelerated atherosclerotic vascular disease in large arteries has been partially
attributed to the excess of conventional cardiovascular
risk factors in the diabetic population.1 The development of microangiopathy involves concentric hyaline
thickening of arteriolar walls, capillary basement membrane thickening, nonenzymatic glycosylation of tissue
proteins, and abnormalities of the endothelial cells.2
Diets rich in fish oils appear to be associated with a
low incidence of atherosclerosis and acute thrombotic
complications due to atherosclerosis.34 Because fish oils
favorably influence many of the mechanisms involved in
atherogenesis, they are attractive candidates for therapy
in diabetic subjects.5 Recent evidence also supports a
role for a direct action of fish oils on the microvasculature in diabetes that may delay complications attributable to microvascular disease.6
The widespread changes in arterial wall properties
that occur with diabetes modify the ventricular-vascular
interaction and alter the shape of the pressure-pulse
Received February 28, 1994; revision accepted June 13, 1994.
From the Department of Medicine (G.E.McV.), Health Computer Sciences Division, the Department of Laboratory Medicine
and Pathology (S.M.F.), Cardiovascular Division, and the Department of Medicine (J.N.C.), University of Minnesota; and the
Departments of Therapeutics and Pharmacology (G.M.B., G.D.J.)
and Medicine (R.J.H.), Belfast City Hospital, Queens University
of Belfast, Ireland.
Correspondence to Dr Gary McVeigh, Department of Medicine, University of Minnesota Medical School, Box 741 UMHC,
420 Delaware St SE, Minneapolis, MN 55455.
© 1994 American Heart Association, Inc.
Key Words • fish oil •
hemodynamics
compliance
•
resistance
•
Methods
Subjects
Sixteen male and four female patients with NIDDM were
recruited from diabetic clinics in the Belfast area. The patients' ages ranged from 45 to 61 years, and diabetic control
was achieved with diet alone or diet plus sulfonylurea,
biguanide preparations, or both. The mean fasting blood
glucose was 9.9 mmol/L (range, 5.4 to 15.7), and mean glycated
hemoglobin was 9.7% (range, 6.3% to 12.9%). The known
duration of diabetes was 5.2 years (range, 9 months to 16
years). Subjects were excluded if there was a history of
cerebrovascular disease, ischemic heart disease, hypertension
(blood pressure > 150/90 mm Hg), or significant renal impairment (creatinine clearance <30 mL/min) or if they were taking
cardiovascular drugs. No subjects took fish oil supplements
before the study.
Patients entered a double-blind, placebo-controlled crossover study with randomized allocation of treatments consisting
of three 6-week phases.12 During the first 6 weeks the patients
randomly received either 10 capsules per day of fish oil
1426
Arteriosclerosis and Thrombosis
Vol 14, No 9 September 1994
(MAXEPA; Duncan Flockhart) or identical-appearing olive
oil placebo capsules. After a 6-week washout period, patients
were assigned to the other therapy for a further 6-week period.
Fish oil capsules provided a daily intake of 1.8 g eicosapentaenoic acid and 1.2 g docosahexaenoic acid. Patients adhered
to their regular diets and medications throughout the study
period. Hemodynamic impedance data were collected at baseline and again on completion of each treatment phase.
Compliance with the medication was assessed by capsule
counts and by measurement of platelet membrane fatty acid
composition by gas chromatography. Venous blood was drawn
from each subject after a 30-minute supine rest during the
baseline study and on completion of the active treatment
phases for estimation of fasting glucose, platelet membrane
fatty acids, total cholesterol, and total triglyceride concentrations. Samples for lipid profiles were collected in EDTA tubes
and measured by ultracentrifugation. All participants gave
written informed consent for all procedures. This study was
approved by the Ethics Committee of the Queen's University
of Belfast.
Downloaded from http://atvb.ahajournals.org/ by guest on October 2, 2016
Procedures
Investigations were performed between 8 and 9 AM in a
quiet, temperature-controlled laboratory with the subjects
lying supine. Participants fasted for 14 hours before the study,
during which time alcohol, caffeine, and smoking were prohibited. Under local anesthesia (lidocaine 1%) and sterile conditions, a 20-gauge polyethylene catheter (Vygon Leader Cath)
was inserted into the left brachial artery. The catheter was
connected to a Bell and Howell pressure transducer with
24-inch fluid-filled pressure tubing. The transducer was
aligned with an amplifier on an Electromed physiological
recorder for the recording of arterial blood pressure. The
catheter-transducer-amplifier system introduced minimal distortion in the recorded signal. All subjects rested for 30
minutes after catheter placement to establish a stable baseline
before data collection. Saline (0.9%) was infused into the
brachial artery at a rate of 0.3 mL/min during the control
period.
A commercial pulse-wave Doppler flow-meter system
(Quantascope, Vital Science) based on the attenuated compensation volume-flow meter principle was used to measure
cardiac output.15 The Quantascope uses a 2-MHz two-element
annular-array transducer. The system automatically chooses
the appropriate aperture settings (amplitude and phase),
which allow wide and narrow ultrasound beams to be generated. The probe was positioned in the suprasternal notch of
patients lying in the supine position to insonate the ascending
aorta, and cardiac waveforms were averaged on a beat-to-beat
basis. Cardiac output, stroke volume, and flow acceleration
were computed from the averaged waveforms. Measurements
of cardiac output were obtained immediately after vascular
compliance recordings.
Beat Marking and Waveform Analysis
Brachial arterial waveforms were recorded for 30 seconds
for each subject in the supine position. The pressure-transducer-amplifier system was connected directly to a specially
designed board (kindly provided by Hypertension Diagnostics,
Inc) placed in an IBM personal computer. The pulse-wave
data were collected, digitized at 200 samples per second, and
stored in computer memory. The data were automatically
displayed on the computer screen for visual analysis to confirm
that recorded waveforms were uniform and showed no artifacts. The most consistent (by visual inspection) 10 consecutive
waveforms were selected for beat marking. A printout of the
marked points was checked for accuracy of the beat-marking
procedure.
The passive, transient response of the arterial vasculature to
the initial loading conditions produced during systole by left
ventricular ejection was determined by analyzing the diastolic
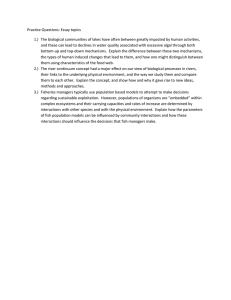
FIG 1. The passive and transient response of the arterial system
to the stroke volume produced during systole, which occurs after
aortic valve closure, is determined by analyzing the diastolic
portion of the pressure-pulse waveform. Pulse-contour analysis
segments the diastolic interval into an exponential decay curve
that reflects the compliance characteristics predominantly of the
larger arteries and an oscillatory dicrotic wave that results from
peripheral pulse-wave reflections and a damped resonance
occurring in the arterial tree. The first term in the third-order
equation (A,e-A 2 t) fits to the exponential decay; the second
term [A3e-A4t cosfAst+Ae)] represents a decaying sinusoid that
fits to the oscillatory dicrotic wave.
portion of the pressure-pulse waveform. A detailed description
of the curve-fitting procedures and a derivation of the model
elements Q , C 2 , R, and L (see Table 3) calculated from a
four-element Windkessel model of the arterial circulation have
been described.10-1617 Briefly, the curve-fit software program
uses a third-order equation to represent the time course of the
diastolic pressure decay and to produce a set of A constants
that describes an average waveform that accurately fits to each
marked pressure-pulse contour (Fig 1). Elements in the Windkessel model are calculated from the systemic resistance
(mean brachial arterial pressure divided by cardiac output)
and the six A constants (A, through A^), which are determined
from the pulse-wave analysis by equating the A constants with
comparable coefficients from the solution to the circuit equations. Based on the circuit equation analysis only the A2
(exponentially decaying pressure), A4 (damping of the diastolic
oscillation), and As (frequency of the oscillation) constants are
required to determine the compliance and inertance model
elements.
Statistical Analysis
ANOVA was used to compare changes from baseline in
hemodynamic impedance parameters and metabolic variables
for each treatment and to compare differences between treatments. Results are expressed as means with a 95% confidence
interval (CI).
Results
Adherence to the prescribed regimens was confirmed
by capsule counts and by measurement of platelet
membrane fatty acid composition. Incorporation of
eicosapentaenoic acid and docosahexaenoic acid into
platelet membranes occurred at the expense of arachidonic acid (Fig 2). Assessment of platelet lipid fractions
showed an increase in the percent membrane constituent of eicosapentaenoic acid after fish oil administration
(2.9; CI, 2.2 to 3.6) compared with values recorded at
baseline (1.2; CI, 0.2 to 2.2) and after olive oil administration (1.1; CI, 0.8 to 1.4) (/'<.001 for both). The
membrane percentage constituent of docosahexaenoic
acid also increased significantly after fish oil
administration.
Neither intervention significantly altered heart rate,
arterial blood pressure, cardiac output, or stroke volume compared with baseline values (Table 1). Metabolic parameters are outlined in Table 2. Compared
with baseline values, fish oil ingestion increased fasting
glucose levels from 10.2 (CI, 8.9 to 11.4) to 11.4 (CI, 9.7
McVeigh et al
Fish Oil and Arterial Compliance
1427
TABLE 2. Metabolic Parameters at Baseline and After 6
Weeks of Olive Oil and Fish Oil Ingestion
Baseline
Olive Oil
Variable
Baseline
Olive Oil
Fish Oil
Fasting
glucose
11.4(9.7-13.3)
10.2(8.9-11.4)
11.0(9.3-12.7)
Total
cholesterol
5.3 (4.9-5.7)
5.3 (4.9-5.7)
5.3
(4.9-5.7)
Total
triglycerides
1.8 (1.4-2.2)
1.6 (1.4-1.9)
1.4
(1.1-1.8)
Values are given as millimoles per liter and are mean (95%
confidence interval). There were no significant differences.
Fish Oil
FIG 2. Bar graph showing platelet membrane fatty acid content at baseline and after 6 weeks of dietary olive oil or fish oil
supplementation. Arachidonic acid (•), eicosapentaenoic acid
(s), and docosahexaenoic acid (s) are expressed as percentage constituents of the platelet membrane lipid. Data are
expressed as means with 95% confidence intervals. *P<.01,
tP<.OO1 vs values recorded at baseline and after olive oil
ingestion.
Downloaded from http://atvb.ahajournals.org/ by guest on October 2, 2016
lipoprotein metabolism.5 The direct vascular actions of
fish oils expressed at the level of the vessel wall after
incorporation into the phospholipids of cell membranes
may also contribute to their vascular protective effects.1113 Dietary supplementation with fish oil improved the large-artery and oscillatory compliance estimates compared with responses recorded at baseline
and after olive oil administration in patients with
NIDDM. In contrast, neither intervention influenced
the systemic vascular resistance compared with baseline
values.
The diastolic pulse contour is composed of an exponential decay and a superimposed oscillatory dicrotic
wave found in the proximal portion of the waveform.18
The pulse-contour analysis technique segments diastole
into two components, identifying the exponential decay
as a function of large-artery compliance and the dicrotic
wave as a measure of oscillations in the arterial system
that reflect altered compliance characteristics of the
more peripheral vasculature.16 From the earliest measurements of accurate arterial pressure waveforms, the
presence of diastolic fluctuations were believed to represent the effects of peripheral wave reflections producing a form of damped resonance superimposed on the
basic shape of the pressure waveform.19'20 Pressurepulse waveform reflections arise primarily from discontinuities in the caliber of or elastic properties along
vessels in the arterial system, with the major reflections
residing in the high-resistance arterioles.2021
to 13.3) mmol/L (P=.O7). Baseline levels of total cholesterol (5.3 [CI, 4.9 to 5.7] mmol/L) were unchanged by
either intervention. A reduction in fasting triglyceride
values occurred with fish oil ingestion compared with
baseline values (1.8 [CI, 1.4 to 2.2] versus 1.4 [CI, 1.1 to
1.8] mmol/L; P=.08).
No differences were recorded in the model parameters reflecting the steepness of the exponential decay
(A2) and damping of the diastolic oscillation (A4) when
baseline values were compared with those recorded
after olive oil administration. In contrast, fish oil ingestion significantly decreased values for A2 and At compared with estimates obtained at baseline and after
olive oil administration. This was reflected in the improved large-artery (Q) and oscillatory (Q) compliance
estimates (Table 3). Q increased from 1.50 (CI, 1.31 to
1.69) mL/mm Hg at baseline and 1.52 (CI, 1.35 to 1.69)
mL/mm Hg after olive oil administration to 1.68 (CI,
1.52 to 1.84) mL/mm Hg after fish oil administration
(P<M). Q increased from 0.015 (CI, 0.011 to 0.019)
mL/mm Hg at baseline to 0.022 (CI, 0.016 to 0.028)
mL/mm Hg after fish oil ingestion (P<.05). The increase in C2 after fish oil administration compared with
values recorded after olive oil ingestion were nonsignificant (P=.08). No changes occurred in systemic vascular
resistance values during the study.
Studies in populations from Japan that used pulsewave velocity as a measure of arterial stiffness in
large-artery segments have shown that subjects who
regularly consumed fish had a lower pulse-wave velocity
and more distensible vasculature than subjects whose
diets were virtually devoid of fish.22 Improved arterial
wall characteristics have also been described in fish-
Discussion
The cardioprotective actions of fish oil have largely
been attributed to its antiplatelet activity and effects on
TABLE 1. Hemodynamic Variables at Baseline and After 6 Weeks of Olive Oil and Fish
Oil Ingestion
Variable
Systolic BP, mm Hg
Baseline
Olive Oil
Fish Oil
108 (100-116)
107 (100-117)
103 (96-110)
Diastolic BP, mm Hg
71
(67-75)
70
(66-74)
68 (65-71)
Mean arterial pressure, mm Hg
83
(78-88)
82
(76-88)
79 (75-83)
(60-82)
71
Heart rate, beats/min
71
(61-81)
70 (60-80)
Cardiac output, L/min
6.0 (5.2-6.8)
5.9 (5.2-6.6)
5.9 (5.3-6.5)
Stroke volume, mL
92
89
91 (84-98)
(85-99)
(80-98)
BP indicates blood pressure. Values expressed are mean (95% confidence interval). P=NS for all
comparisons.
1428
Arteriosclerosis and Thrombosis
Vol 14, No 9 September 1994
TABLE 3. Pulse-Contour and Impedance Parameters at Baseline and After 6 Weeks of
Olive Oil and Fish Oil Ingestion
Parameters
Pulse contour
EBaseline
Olive Oil
Fish Oil
A 2 ,s-'
0.76
(0.70-0.82)
0.75
(0.70-0.80)
0.68
(0.63-0.73)*
A4,s-'
86
(56-116)
80
(45-115)
45
(32-58)t
Aa.s- 1
23
(16-30)
21
(15-27)
27
(18-36)
1.50
(1.31-1.69)
1.52
(1.35-1.69)
1.68
(1.52-1.84)*
Impedance
C,, mL/mm Hg
C 2 , mL/mm Hg
0.015 (0.011-0.019)
R, dyne • s • cm~5
1
L, mL- mm Hg~ • s"
2
0.017 (0.013-0.021)*
0.022 (0.016-0.028)t
1268
(1144-1392)
1254
(1131-1377)
1210
(1128-1292)
0.02
(0.01-0.03)
0.02
(0.01-0.03)
0.02
(0.01-0.03)
A2 indicates exponentially decaying pressure; A4, damping of the diastolic oscillation; A5, frequency
of the diastolic oscillation; C,, larger-artery compliance estimate; C 2 , oscillatory compliance estimate;
Ft, systemic resistance; and L, inertance. Data are expressed as mean (95% confidence interval).
*P<.01 fish oil vs baseline and olive oil; tP<-05 fish oil vs baseline; tP=.O8 fish oil vs olive oil.
Downloaded from http://atvb.ahajournals.org/ by guest on October 2, 2016
eating compared with non-fish-eating patients with
NIDDM. 23 Fish consumption may favorably improve
arterial stiffness by retarding the progression of atherosclerosis. However, atherosclerosis is a patchy disease
and probably plays a relatively minor role in decreasing
arterial compliance,24-25 which suggests that direct vascular actions of polyunsaturated fatty acids may be of
greater importance in influencing arterial wall
characteristics.11-26
Fish oils may influence vascular reactivity through
effects on the endothelium, by altering the production
of substances by other cells that affect endothelial cell
function or by directly altering the activity of the smooth
muscle cell. Dietary marine oil supplementation suppresses forearm vasoconstrictor responses to the local
infusion of angiotensin II and norepinephrine,13 and
fish oil supplementation in patients with NIDDM augments stimulated and perhaps basal release of nitric
oxide from the vascular endothelium.12 In experimental
models of atherosclerosis and hypertension, fish oil
therapy improves endothelium-dependent relaxation in
large arteries.11-27-28 Simon et al9 report that administration of the exogenous nitric oxide donor nitroglycerin
alters vascular tone and improves arterial compliance
without significantly lowering the mean arterial pressure. Coupled with the known effects of fish oils on
prostaglandin metabolism,26 these data suggest that
polyunsaturated fatty acids exert direct vascular actions
that influence arterial function by altering the production, release, or breakdown of vasoactive substances
from blood vessel walls. Such actions probably account
for the improved compliance characteristics observed in
this study, as the short-term prescription of fish oils
would be unlikely to influence the structural properties
of the arterial vasculature. Although a trend for a
decrease in plasma triglyceride levels was apparent, the
improved compliance estimates occurred without significantly altering cholesterol or triglyceride concentrations, suggesting that possible vascular protective actions of fish oils may be dissociated from their effects on
lipid metabolism.
A major problem in assessing the direct effects of
pharmacological agents on arterial compliance has been
that the administration of vasoactive drugs often alters
blood pressure in addition to influencing vascular tone
and reactivity. This alteration in blood pressure makes
it difficult to know whether a change in compliance in
response to vasoactive compounds directly reflects an
alteration in vessel wall properties or occurs as a
consequence of the change in blood pressure.29 In this
study, fish oil administration improved the compliance
characteristics of the arterial vasculature independent
of effects on cardiac output and resistance to blood flow.
That changes in arterial compliance with fish oil ingestion occurred without alteration in systemic resistance
supports the observations of others in diabetic patients23 and suggests that the ability of a vessel to
distend in response to a pressure load is more sensitive
than its basal caliber in identifying abnormal structure
and tone.16 Pulse-contour analysis could therefore prove
to be a useful technique to follow disease progression in
patients and monitor the effects of drug interventions
on the arterial vasculature,10 especially as technological
advances now permit the recording of high-quality
waveforms noninvasively.30
In conclusion, short-term dietary supplementation
with fish oils improved the compliance characteristics of
the arterial circulation in patients with NIDDM. Improving arterial wall characteristics may represent an
additional mechanism whereby fish oils exert their cardioprotective action in humans.
Acknowledgments
This work was supported by a grant from the British
Diabetic Association. Dr Brennan is a research fellow supported by the British Diabetic Association.
References
1. Colwell JA, Lopes-Virella MF. A review of the development of large
vessel disease in diabetes mellitus. Am J Med. 1988;85(suppl 5A):
113-118.
2. Barnett AH. Pathogenesis of diabetic microangiopathy: an
overview. Am J Med. 1991;90(suppl 6A):673-735.
3. Kromhout D, Bosschieter EB, deLezenne Coulander C. The
inverse relation between fish consumption and 20 year mortality
from coronary heart disease. N EnglJ Med. 1985;312:1205-1209.
4. Burr ML, Fehily AM, Gilbert JF, Rogers S, Holliday RM,
Sweetnam PM, Elwood PC, Deadman NM. Effects of changes in
fat, fish, and fibre intakes on death and myocardial infarction: diet
and reinfarction trial (DART). Lancet. 1989;2:757-761.
McVeigh et al Fish Oil and Arterial Compliance
Downloaded from http://atvb.ahajournals.org/ by guest on October 2, 2016
5. Malasanos TH, Stacpoole PW. Biological effects of W-3 fatty acids
in diabetes mellitus. Diabetes Care. 1991;14:1160-1179.
6. Jensen T, Stender S, Goldstein K, Holmer G, Deckert T. Partial
normalisation by dietary cod-liver oil of increased microvascular
albumin leakage in patients with insulin-dependent diabetes and
alburninuria. N Engl J Med. 1989;321:1572-1577.
7. Pillsbury HC, Hung W, Kyle MC, Fries ED. Arterial pulse waves
and velocity and systolic time intervals in diabetic children. Am
Heart 1. 1973;87:783-790.
8. McVeigh G, Brennan G, Hayes R, Cohn J, Finkelstein S, Johnston
D. Vascular abnormalities in non-insulin dependent diabetes
mellitus identified by arterial waveform analysis. Am J Med. 1993;
95:424-450.
9. Simon ACh, Levenson JA, Levy BI, Bouthier JE, Peronneau PP,
Safar ME. Effect of nitroglycerin on peripheral large arteries in
hypertension. Br J Clin Pharmacol. 1982;14:241-246.
10. Finkelstein SM, Collins VR, Cohn JN. Arterial vascular compliance response to vasodilators by Fourier and pulse contour
analysis. Hypertension. 1988;12:380-387.
11. Shimokawa H, Vanhoutte PM. Dietary cod-liver oil improves endothelium-dependent responses in hypercholesterolernic and atherosclerotic porcine coronary arteries. Circulation. 1988;78:
1421-1430.
12. McVeigh GE, Brennan GM, Johnston GD, McDermott BJ, McGrath
LT, Henry WE, Andrews JW, Hayes RJ. Dietary fish oils augments
nitric oxide production or release in patients with Type 2 (noninsulin-dependent) diabetes mellitus. Diabetobgza. 1993;36:33-38.
13. Chin JPF, Gust AP, Nestel PJ, Dart AM. Marine oils dose dependently inhibit vasoconstriction of forearm resistance vessels in
humans. Hypertension. 1993;21:22-28.
14. Safar M. Therapeutic trials and large arteries in hypertension. Am
Heart J. 1988;115:702-710.
15. Silke B, Zezulka AV, Verma SP, Taylor SH. Hemodynamic
assessment of nicardipine alone and with atenolol in coronary
artery disease using a modified echo-Doppler device. Am J Cardiol.
1989;64:28H-34H.
16. McVeigh GE, Burns DE, Finkelstein SM, McDonald KM, Mock
JE, Feske W, Carlyle PF, Flack J, Grimm R, Cohn JN. Reduced
vascular compliance as a marker for essential hypertension. Am J
Hypertens. 1991;4:245-257.
1429
17. Watt TB Jr, Burrus CS. Arterial pressure contour analysis for
estimating human vascular properties. J Appl Physiol. 1976;40:
171-176.
18. Simon ACh, Safar ME, Levenson JA. An evaluation of large
arteries compliance in man. Am J Physiol. 1979;237:H550-H554.
19. Hamilton WF. The arterial pulse. In: Luisada AA, ed. Cardiovascular Functions, Part 2. New York, NY: McGraw-Hill; 1962:
2-132-2-138.
20. Nichols WW, O'Rourke MF. Contours of pressure and flow waves
in arteries. In: Nichols WW, O'Rourke MF, eds. McDonald's Blood
Flow in Arteries. 3rd ed. Philadelphia, Pa: Lea and Febiger; 1990:
216-245.
21. Van den Bos GC, Westerhof N, Randall 0 s . Pulse wave reflection:
can it explain the differences between systemic and pulmonary
pressure and flow waves? Circ Res. 1982;51:479-485.
22. Hamazaki T, Urakaze M, Sawazaki S, Yamazaki K, Taki H, Yano
S. Comparison of pulse wave velocity of the aorta between inhabitants of fishing and farming villages in Japan. Atherosclerosis. 1988;
73:157-160.
23. Wahlqvist ML, Lo CS, Myers KA. Fish intake and arterial wall
characteristics in healthy people and diabetic patients. Lancet.
1989;2:944-946.
24. Hickler RB. Aortic and large artery stiffness: current methodology
and clinical correlations. Clin Cardiol. 1990;13:314-322.
25. Avolio AP, Chen S-G, Wang R-P, Lang C-L, Li M-F, O'Rourke
MF. Effects of aging on changing arterial compliance and left
ventricular load in a Northern Chinese urban community.
Circulation. 1983;68:50-68.
26. Leaf A. Cardiovascular effects of fish oils: beyond the platelet.
Circulation. 1990;82:624-628.
27. Yin K , Chu ZM, Beilin LI. Blood pressure and vascular reactivity
changes in spontaneously hypertensive rats fed fish oil. Br J
Pharmacol. 1991;102:991-997.
28. Beilin U.Dietary fats, fish, and blood pressure.Ann N YAcad Sci.
1993;683:35-45.
29. McVeigh GF, Finkelstein SM, Cohn JN. Assessment of arterial
compliance in hypertension. Curr Opin Nephrol Hypertens. 1993;2:
82-86.
30. Kelly R, Hayward C, Avolio A, O'Rourke M. Noninvasive determination of age-related changes in the human arterial pulse.
Circulation. 1989;80:1652-1659.
Fish oil improves arterial compliance in non-insulin-dependent diabetes mellitus.
G E McVeigh, G M Brennan, J N Cohn, S M Finkelstein, R J Hayes and G D Johnston
Downloaded from http://atvb.ahajournals.org/ by guest on October 2, 2016
Arterioscler Thromb Vasc Biol. 1994;14:1425-1429
doi: 10.1161/01.ATV.14.9.1425
Arteriosclerosis, Thrombosis, and Vascular Biology is published by the American Heart Association, 7272 Greenville
Avenue, Dallas, TX 75231
Copyright © 1994 American Heart Association, Inc. All rights reserved.
Print ISSN: 1079-5642. Online ISSN: 1524-4636
The online version of this article, along with updated information and services, is located on the
World Wide Web at:
http://atvb.ahajournals.org/content/14/9/1425
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in
Arteriosclerosis, Thrombosis, and Vascular Biology can be obtained via RightsLink, a service of the Copyright
Clearance Center, not the Editorial Office. Once the online version of the published article for which permission
is being requested is located, click Request Permissions in the middle column of the Web page under Services.
Further information about this process is available in the Permissions and Rights Question and Answerdocument.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Arteriosclerosis, Thrombosis, and Vascular Biology is online
at:
http://atvb.ahajournals.org//subscriptions/