Food Establishment

Food
Establishment
Plan Review
Application
Plan Review fee of $235 due at time of submission.
Step-by-Step Procedures for Obtaining a Food Safety License
Please be aware that:
• Plan Review Applications should be submitted — at minimum — one month prior to opening.
• Local zoning regulations require that properties are properly zoned to operate a food establishment. Please verify that the property is properly zoned.
• Building permits may not be issued by the City of Peoria until plans are approved by this department. Please plan accordingly.
• A Food Safety License from this department is required before the City of Peoria will issue a liquor license.
• All Plan Review Applications and any additional information or revisions will be reviewed in the order in which they are received.
• All food service establishments except Category III facilities shall have a Certified Food Service Sanitation Manager from the initial day of operation or shall provide documentation of enrollment in an approved course to be completed within three (3) months of opening.
• All payments must be made by check, cash, money order, or credit or debit card. Service fees will be assessed when using a credit or debit card.
Step One – Initial Inquiry
• Contact Environmental Health for a Plan Review Application Packet and a copy of the current Peoria County Food
Safety Code.
Step Two – Submit Plans
The following items must be submitted before your plans will be evaluated: o A completed Plan Review Application (yellow).
o A labeled, scale drawing of your food establishment showing the location of major appliances, sinks, employee break areas, restrooms, etc.
o A copy of your proposed menu.
o Water well inspection/sample (if applicable).
o Septic inspection (if applicable).
o Plan Review Fee – $235.
Step Three – Review Process
• The plans will be reviewed ONLY after all the above required documents and fees have been submitted.
• An incomplete Plan Review Application Packet will be returned. This will delay the approval process.
• Please allow up to ten (10) business days to review the plans once all required documents are received.
Step Four – Approval Process
• Changes to your plans or additional information may be required prior to plan approval.
• Any changes to the submitted plans must be pre-approved by this department before construction begins.
• You must notify this department for approval should a change be made during construction.
Step Five – Preliminary Inspection and Final Approval
• After your plans have been approved and interior work has begun, contact the Environmental Health Practitioner I to schedule a preliminary inspection (optional). A Preliminary Inspection Report will be provided to you at this inspection.
Items that require correction will be noted.
• When the establishment is finished and all equipment is in place and operational, a final inspection can be scheduled.
All equipment must be on and functioning properly during this inspection. If the establishment meets code and no major corrections are needed, final approval to operate will be given.
• Annual license fee must be paid prior to final approval to operate.
• Please allow at least one week to schedule preliminary or final inspections.
10
3
5
5
6
1
2
4
7
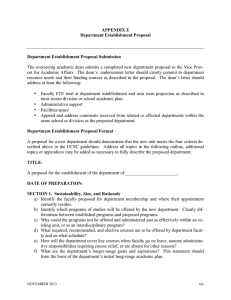
Cooks Line
SAMPLE
Establishment Floor Plan
Dining Area
12
13 13 7
14
Beverage Area
15
9
12
10
10
Bakery
Area
10
8 12
12
12
7
17
11
10
12
12
12
20
7
10
12
Ware-Wash Area
12
12
Dry Storage Room
12
18
Walk-In Cooler
15
Walk-In Freezer
16
19
Locker/Break Area Rest
Room
7
60 ft.
Equipment (Make and Model #)
1. Microwave (ABC #123)
2. Steamtable (HOT #A1)
3. Stove (AOK #22)
4. Griddle (AOK #Q17)
5. Fryer (ABC #55)
6. Charbroiler (HOT #A7)
7. Hand Sink
8. Mixer (EZ #99)
9. Refrigerator/Freezer Make-
Table Unit w/ pass-thru and shelf (COLD #1P)
10. Stainless Steel Table
11. Sliding 3 Door Refrigeration
Unit (COLD #2A)
12. Shelving Unit
13. Coffee Maker (ABC #16)
14. Soda Machine (PDQ #2A)
15. Walk-In Cooler (COLD#AZ1)
16. Walk-In Freezer (COLD #AZ3)
17. Dish Machine (Magic #15)
18. 3-Compartment Sink w/
36” drainboards
19. Mop Sink
20. Prep Sink
Please include (at minimum): Major appliances; sinks; break areas; restrooms; prep areas; coolers; bar areas; server areas; utility sinks.
Food Establishment Requirements
What is a Food Establishment?
As defined in Chapter 10, Food Safety, of the Peoria County Code; a Food Establishment is any food service establishment; tavern; bar; nightclub; commissary; catering kitchen; bakery; bed and breakfast establishment; retail food store; mobile food unit; sidewalk and street food vending unit; temporary food establishment; private, public or nonprofit organization or institution routinely serving food; and any other eating or drinking establishment or operation where food or drink is prepared, served, or provided for human consumption with or without charge.
Do all Food Establishments need a Food Safety License?
Yes. All Food Establishments operating in Peoria County must have a Food Safety License issued by the Peoria City/
County Health Department.
What regulations apply to Food Establishments?
• Chapter 10, Food Safety, of the Peoria County Code.
• Illinois Department of Public Health Food Service Sanitation Code .
• Any other applicable local or state ordinances or codes, including City or Township ordinances, Zoning Codes,
Plumbing Code, Fire Code, etc.
What type of licenses are available for Food Establishments?
There are many types of licenses available for Food Establishments, such as Annual and Seasonal licenses,
Mobile Food Unit licenses, and Street and Sidewalk Vending Unit licenses. This application is specific to Annual and
Seasonal licenses for those establishments selling more than pre-packaged potentially hazardous foods. License fees are determined by the risk level of the establishment.
How is Risk Level determined?
The risk level is determined during the plan review process and is based on menu, population served, and food processing procedures. There are three risk levels: Category I, Category II, and Category III.
What are general requirements for a Food Establishment?
General: o All food must be from an approved source.
o Any special processes must have HACCP plan prior to operations.
o The Peoria City/County Health Department issues licenses at the retail level. Please contact the Illinois Department of Public Health or Department of Agriculture for wholesale operations.
o All establishments, except Category III, must have at least one Certified Food Service Sanitation Manager on staff or enrolled in a class before plans will be approved. A Certified Food Service Sanitation Manager must be present at all times in Category I establishments. A Certified Food Service Sanitation Manager must be available at least 30 hours a week or the length of time the establishment is open if less than 30 hours for all Cate g ory II establishments.
All other employees must have received approved Food Handler Training.
Plumbing: o All plumbing must meet Plumbing Code and be installed/repaired by a Licensed Plumber.
o Hot and cold running water must be available at all sinks.
o Hand washing sinks are required and must be convenient and easily accessible to all food handlers. Soap, paper towels, and a trash receptacle must be available at all hand washing sinks.
o A three compartment sink is required. It must be large enough that each compartment can accommo d ate the largest item to be cleaned. Drain boards are required on both sides.
o Grease traps may be required. Please consult the local plumbing inspector or sanitary district regarding if a grease trap is required and sizing.
o A mop sink or utility sink is required.
o At least one restroom must be available for employee use .
Equipment and Surfaces: o Enough refrigeration or freezer units must be available to keep food items at 41°F or less at all times.
o Enough cooking and hot holding units must be available to cook and hot hold foods. If reheating foods, appropriate equipment must be available. Foods cannot be reheated in crockpots, steam tables, or other equipment designed only to maintain food temperatures.
o All surfaces must be smooth, easily cleanable, and non-absorbent. All exposed wood must be sealed. Shelving must be free from rust and chipping paint.
o Walls and ceilings must be in good repair, smooth, light colored and easily cleanable.
o Floors in food preparation, food storage, dishwashing, walk-in refrigerator and freezer, toilet rooms, and dressing rooms must be smooth, durable, easily cleanable, in good repair, free of cracks and chips, and non-absorb e nt.
o Ventilation is required to keep establishments free of excessive heat, steam, condensation, vapors, obnoxious odors, smoke and fumes. The type of hood required is determined by the mechanical code; please consult your local building inspector for hood requirements. Fire suppression systems may also be required; please consult your local fire department for those requirements.
Pest Control: o Doors and windows must protect against the entrance of pests. Doors must be self-closing and rodent proof.
o If doors and windows are to remain open, they must be screened, air curtained, or some other approved form of pest control prevention measure must be used.
Water Supply: o An approved water supply must be available. If the establishment is on a water well, the well must be tested.
Depending on the number of people/days the well is used, it may also be considered a Non-Community Public
Water Supply and is subject to regulations under the Drinking Water Systems Code.
Wastewater Disposal: o The establishment must have an approved wastewater disposal system. If the establishment is served by a private onsite wastewater treatment system (septic system), the system must be inspected by a Private Sewage
Disposal Contractor.
Restrooms: o The number of restrooms required is determined by the Illinois Plumbing Code. Please consult your local plumbing inspector for those requirements.
o At least one restroom (can also be the public restroom) must be available for employee use.
o Restrooms must have self-closing doors, mechanical ventilation, and handwashing sinks with hot and cold running water, soap, and paper towels.
Miscellaneous: o All lighting must be shielded to protect food and surfaces from the possibility of contamination due to broken glass.
o Working surfaces and food preparation areas must have at least 20 foot candles of light.
o Dumpsters must be stored on concrete or asphalt.
Special Circumstances: o Variances: A variance request may be submitted to modify or waive compliance with the IDPH Food Service
Sanitation Code. The variance will be approved if a health hazard or nuisance will not result from the approval.
o Open Air Dining: An establishment is considered to have open air dining if it leaves doors, windows, or other openings to the outside open with no active pest control (screens, air curtains, etc.).
a copy of the Open Air Dining Requirements.
Establishments that would like to engage in open air dining should contact the Health Department as soon as possible and request o Outdoor Grilling/Food Service/Bar. If an establishment would like to prepare food or drinks outside, but still on the premises of the establishment, a variance request must be submitted. Temporary Event requirements must be followed in addition to any other conditions placed on the variance request. Variance requests for outdoor food service must be renewed on a yearly basis.
Peoria City/County Health Department
Food Service Establishment Licensee Identification Form
Establishment Name: __________________________________________________________________________________________
Establishment Address: ________________________________________________________________________________________
City: _____________________________________________________ State: ________ ZIP Code: ___________________
Mailing Address (if different than above) ___________________________________________________________________________
City: _____________________________________________________ State: ________ ZIP Code: ___________________
Main Contact Person: _________________________________________________________________________________________
Phone Number: ________________________________________ E-mail Address: ____________________________________
Address: ___________________________________________________________________________________________________
City: _____________________________________________________ State: ________ ZIP Code: ___________________
State of Illinois IBT Number (Sales Tax Number) : ____________________________________________________________________
FEIN: ______________________________________________________________________________________________________
Type of Ownership: o Sole Proprietorship o Corporation (provide additional information below) o Partnership o Other ____________________________
Corporation Name: ________________________________________________________________________________________
Date of Incorporation: ________________________________ State of Incorporation: _______________________________
Address of Corporate Office_________________________________________________________________________________
City: _________________________________________________ State: ________ ZIP Code: ___________________
List Owner, Corporate Officers or General Partners (use additional sheets if necessary) :
Name Title Residential Address
I declare that I have examined this form, and to the best of my knowledge and belief, the information entered on this form is true, correct, and complete.
_________________________________________________________________ ____________________________
Signature of Owner or Officer empowered to sign for Corporate Entity Date
_________________________________________________________________
Print or type name signed above
For Corporations:
_________________________________________________________________ ____________________________
Signature of Corporate Secretary Date page 1
Plan Review Application
The undersigned hereby makes application for a permit to operate a Food and/or
Beverage Establishment and/or Retail Food Establishment in the County of Peoria.
o Remodel of existing licensed Food Service Establishment
Establishment:
Establishment Name: __________________________________________________________________________________________
Establishment Address: ________________________________________________________________________________________
City: _____________________________________________________ State: ________ ZIP Code: ___________________
Phone Number: ________________________________________ FAX Number: ______________________________________
E-mail Address: ______________________________________________________________________________________________
Licensee (Owner) : _______________________________________________________________________________________
Address: ___________________________________________________________________________________________________
City: _____________________________________________________ State: ________ ZIP Code: ___________________
Phone Number: ________________________________________ FAX Number: ______________________________________
E-mail Address: ______________________________________________________________________________________________
Send mailings to: o Establishment o Licensee (Owner)
Contact Person: _______________________________________________ Phone: ___________________________
Manager: ______________________________________________________ Phone: ___________________________
Type of Establishment: o Restaurant o Bar/Tavern o o
Assisted Living
Bed & Breakfast o Retail o Daycare o School o o o
Catering
Commissary
Concession Stand o o o o o
Corrections Facility
Farmers’ Market
Hospital
Lodging
Long Term Care Facility o o o o
Mobile
Satellite Food Distribution
Seasonal
Other:
_________________________
Days and Hours of Operation:
Hours of Operation What time does someone arrive to prepare food?
Sunday
Monday
Tuesday
Wednesday
Thursday
Friday
Saturday
Water Supply: o Public o Semi-Private Well o Non-Community Well
Sewage Disposal: o Public o Private (Septic System)
Does this establishment cater?
........................................................................................................
o Yes .................
o No page 2
I. General
Projected Opening Date _______________________________________________________________________________________
Number of Seats _____________________________________ Number of Staff (maximum per shift) ______________________
Total Square Feet of Establishment _______________________ Number of floors on which operations are conducted _________
Approximate number of meals to be served: Breakfast _____________ Lunch
Will a highly susceptible population (elderly, young children, and/or immuno-compromised people) be served as the primary consumers? .........................................................................................................................
o Yes ...........
o No
Will food be transported to another location as with a catering operation or satellite kitchen? ....................................
o Yes ...........
o No
If YES, please list all locations food will be transported to on a regular basis: ______________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
Will the establishment be seasonal? (Seasonal establishments operate for 8 or fewer months per year) ...................
o Yes ...........
o No
If YES, please provide the dates of operation: ______________________________________________________________________
II. Food
Are all food supplies from inspected and approved sources? ......................................................
o Yes ...............
o No
Will all shellfish tags and invoices be maintained for 90 days? ....................................................
o Yes ...............
o No .................
o N/A
Will game animals be prepared or sold? ......................................................................................
o Yes ...............
o No
Will canning or use of home-canned goods take place at the establishment? .............................
o Yes ...............
o No
Will frozen dairy desserts such as ice cream, gelato, or popsicles be made at the establishment? ...................................................................................................................
o Yes ...............
o No
Special Processing:
If any of the following special processes will occur at the establishment, HACCP plans must be submitted as part of the plan review process. Failure to provide HACCP plans with the plan review application WILL delay the plan review process.
Will any reduced oxygen packaging, such as vacuum packaging, cook/chill packaging, or sous vide take place at the establishment?
....................................................
o Yes ...............
o No
Will smoking of meat for preservation take place at the establishment?
............................
o Yes ...............
o No
Will any foods be cured or dried at the establishment?
........................................................
o Yes ...............
o No
Will the fermentation of sausages or other foods (such as in the making of kimchi, sauerkraut, pickles, yogurt, cheese, kefir, kombucha, miso or soybean paste) occur at the establishment?
.....................................................................................................
o Yes ...............
o No
Will any sprouting of seeds take place in the establishment?
..............................................
o Yes ...............
o No
Will the making of sushi or sushi rice take place in the establishment?
.............................
o Yes ...............
o No
*Will juicing and the packaging of juice take place in the establishment?
..........................
o Yes ...............
o No
*A warning statement on the package and written procedures may be submitted in lieu of a HACCP plan.
Storage:
Is adequate and approved freezer and refrigeration available to store frozen foods, frozen and refrigerated foods at 41°F and below? ........................................................................
o Yes ...............
o No page 3
Storage
(continued)
:
Does each refrigerator have a thermometer? ...............................................................................
o Yes ...............
o No
Will raw meats, poultry (including eggs) and seafood be stored in the same refrigerators and freezers with cooked and/or ready-to-eat foods? ..............................................
o Yes ...............
o No .................
o N/A
Will dry goods and single use items be stored at least 6 inches off the floor? .............................
o Yes ...............
o No
Is appropriate storage space provided for, based upon menu, meals, and frequency of deliveries? ................................................................................................................
o Yes ...............
o No
Are containers constructed of safe materials to store bulk food products? ..................................
o Yes ...............
o No .................
o N/A
Number of refrigeration units: _______________ Number of freezer units: ______________
How will cross-contamination be prevented during storage?____________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
Preparation:
List all foods prepared more than 12 hours in advance of service (examples: coleslaw, sauces, dressings, potato salad, tuna salad, etc.):
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
Will ingredients for cold ready-to-eat foods such as tuna, mayonnaise and eggs for salads and sandwiches be pre-chilled before being mixed and/or assembled? ...........................
o Yes ...............
o No .................
o N/A
Will all produce be washed on site prior to use? ..........................................................................
o Yes ...............
o No .................
o N/A
If YES, what sink will be used? ________________________________________________________________________________
Will disposable gloves and/or utensils be used to prevent bare hand contact with ready-to-eat foods? ......................................................................................................................
o Yes ...............
o No .................
o N/A
All potentially hazardous foods which have been prepared or opened and will be held under refrigeration for more than
24 hours must be date marked to ensure the product is not held longer than 7 days, including the date of preparation.
Describe the date marking procedures that will be utilized: _____________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________ page 4
Preparation
(continued)
:
Describe the procedure used for minimizing the length of time potentially hazardous foods will be kept in the temperature danger zone
(41°F – 135°F) during preparation:
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
Thawing:
Food must be thawed using one of the following methods. Next to the thawing method, list which food items will be thawed using that method.
o Check here if no foods will be thawed.
Thawing Method:
Refrigeration
Food Items:
Under Running Water less than 70°F
Microwave (as part of the cooking process)
Cooked from Frozen State
Other (describe)
Cooking:
Will food thermometers be used to measure the final cooking and reheating temperatures? ......
o Yes ...............
o No .................
o N/A
Will a consumer advisory be posted or added to the menu for all foods which are raw or under cooked? ..........................................................................................................................
o Yes ...............
o No .................
o N/A page 5
Cooking
(continued)
:
List all potentially hazardous foods which will routinely be served raw or under cooked such as sushi, steak tartar, oysters, hollandaise or béarnaise sauce, Caesar dressing, meringue, or egg-fortified beverages:
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
List all equipment that will be used for cooking: _____________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
Hot and Cold Holding:
List the equipment that will be used to maintain a temperature of 135°F or above for all potentially hazardous foods being hot held during service:
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
List the equipment that will be used to maintain a temperature of 41°F or below for all potentially hazardous foods being cold held during service:
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________ page 6
Hot and Cold Holding
(continued)
:
If you will be using ice, as a supplement, for keeping food cold (such as in a salad bar) how will the food be stored in the ice? Describe the procedure to maintain ice levels:
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
If food is going to be transported and/or served off site, how will food temperatures (hot and cold) be maintained? List specific equipment and procedures:
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
Cooling:
All potentially hazardous foods must be cooled from 135°F to 70°F within 2 hours and to 41°F within another 4 hours. List the food items that will be cooled next to the cooling method to be used.
o Check here if no foods will be cooled.
Cooling Method:
Shallow Pans
Food Items:
Ice Baths
Reduce Volume or Size of Food
(smaller portions or containers)
Rapid Chill
Other (describe) page 7
Reheating:
List the equipment that will be used to rapidly reheat food to a temperature of 165°F within 2 hours for hot holding:
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
III. Personnel
Food Handlers:
Will all Food Handlers (those employees engaged in handling food or food contact surfaces) receive ANSI approved Food Handler Training or Illinois Department of Public Health approved Food Handler Training? (Records of this training must be available on site.) ...............
o Yes ...............
o No
Is there a written policy to exclude or restrict food workers who are sick or have infected lesions? ...........................................................................................................................
o Yes ...............
o No
Are dressing rooms or lockers provided for employees’ personal belongings? ............................
o Yes ...............
o No
If NO, where will personal belongings be stored? __________________________________________________________________
Will hand antiseptics (“sanitizers”) be used? ................................................................................
o Yes ...............
o No
If YES , attach proof of compliance with Code and procedures for use.
Will employees be required to use effective hair restraints? .........................................................
o Yes ...............
o No .................
o N/A
Certified Food Service Sanitation Managers:
State of Illinois certificates are printed on green squares with the words “State of Illinois Department of Public Health” at the top. The State of Illinois certificate is the ONLY Certified Food Service Sanitation Manager certificate valid in the State of Illinois.
List all employees certified in food safety by the State of Illinois (if enrolled in a class, please attach proof of enrollment) :
Name Certification Number Expiration Date
IV. Structure
Floors, Walls, and Ceilings:
Are all floors constructed of a smooth, durable, easily cleaned material? ....................................................................
o Yes ...........
o No
Is carpeting used as flooring in any area other than the dining area? ..........................................................................
o Yes ...........
o No
Are all walls and ceilings light-colored, smooth, non-absorbent, and easily cleanable?...............................................
o Yes ...........
o No
Are all light fixtures, vent covers, wall-mounted fans, decorative materials, and similar equipment attached to walls and ceilings, easily cleanable?..........................................................................................................
o Yes ...........
o No
Is there adequate lighting in all areas of the kitchen, walk-in coolers, ware washing areas, restrooms and storage areas? .......................................................................................................................................................
o Yes ...........
o No
Are shields provided for all lighting in food storage, preparation, service, and display units; as well as areas where utensils and equipment are cleaned and stored? ....................................................................................
o Yes ...........
o No page 8
IV. Structure
(continued)
Equipment:
Specify how many of each are available:
Small Equipment
Slicers
Cutting Boards
Can Openers
Mixers
Microwaves
Tabletop Pizza Ovens
Other (describe):
Other (describe):
Other (describe):
Number
Are all food contact surfaces smooth, easily cleanable, and nonabsorbent? ...............................................................
o Yes ...........
o No
Is all non-portable equipment that is placed on tables or counters either sealed to the table or counter or elevated on legs 4 inches off the table or counter? ........................................................................
o Yes ...........
o No
Is all floor-mounted equipment, unless readily moveable, sealed to the floor or elevated on legs to provide a 6 inch clearance? .........................................................................................................................
o Yes ...........
o No
Sinks:
Do all sinks have hot and cold running water? .............................................................................
o Yes ...............
o No
Is there a food preparation sink? ..................................................................................................
o Yes ...............
o No .................
o N/A
Is there a hand washing sink in each food preparation and ware washing area? .........................
o Yes ...............
o No
Do all hand washing sinks have a mixing valve or combination faucet? ......................................
o Yes ...............
o No
If applicable, do “push button” style hand sink faucets provide a flow of water for at least 15 seconds without reactivation? ................................................................................
o Yes ...............
o No .................
o N/A
Is soap available at all hand sinks? ..............................................................................................
o Yes ...............
o No
Are paper towels or air dryers available at all hand sinks? ...........................................................
o Yes ...............
o No
Are waste receptacles provided at each hand sink? ....................................................................
o Yes ...............
o No
Are dump sinks available at all bar and beverage stations? .........................................................
o Yes ...............
o No .................
o N/A
Is there a mop sink? .....................................................................................................................
o Yes ...............
o No
Is there a three compartment sink? ..............................................................................................
o Yes ...............
o No
Does the largest pot and pan fit into each compartment of the three compartment sink? ...........
o Yes ...............
o No .................
o N/A
Are there drain boards on both ends of the three compartment sink? .........................................
o Yes ...............
o No .................
o N/A
Is there a dish machine? ...............................................................................................................
o Yes ...............
o No page 9
Sinks
(continued)
:
If the dish machine is hot water sanitizing, is there a booster heater and mechanical ventilation? .........................................................................................................
o Yes ...............
o No .................
o N/A
Do all dish machines have temperature/pressure gauges as required that are accurately working? .........................................................................................................
o Yes ...............
o No .................
o N/A
Plumbing:
All plumbing, including repairs, must be completed by a licensed plumber.
Is the hot water generator sufficient for the needs of the establishment? ....................................................................
o Yes ...........
o No
Is there a water treatment device? ................................................................................................................................
o Yes ...........
o No
Are there backflow prevention devices where required? ..............................................................................................
o Yes ...........
o No
Plumber Name: ______________________________________________________________________________________________
License Number: _____________________________________________________________________________________________ o Check here if no plumbing work will be done.
Water Supply:
Is the water supply: o Public Name of District (as shown on bill) ________________________________________________ o Well NCPWS #: __________________________________________________________________
Sewage Disposal:
Is the sewage disposal: o Public Name of District (as shown on bill) ________________________________________________ o Septic System – a septic inspection conducted by a Licensed Private Sewage Disposal System
Installation Contractor must be submitted
Are grease traps provided? ..........................................................................................................................................
o Yes ...........
o No
If YES, where are they located? _______________________________________________________________________________
Hoods:
How is the ventilation hood system cleaned? Include how often it is cleaned. ______________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
Restrooms:
Do all restrooms have hand sinks with hot and cold running water, soap, and paper towels or air drying devices? ........................................................................................................................................................
o Yes ...........
o No
To avoid re-contamination of hands, are paper towels available for food employees to use when touching surfaces such as the faucet handles of hand washing sinks or the handles of rest room doors? ..................
o Yes ...........
o No
Are covered waste receptacles available in each rest room? .......................................................................................
o Yes ...........
o No
Are all rest room doors self-closing? ............................................................................................................................
o Yes ...........
o No
Are all restrooms equipped with mechanical ventilation? .............................................................................................
o Yes ...........
o No page 10
IV. Structure
(continued)
Pest Control:
Will all outside doors be self-closing and rodent proof? ...............................................................
o Yes ...............
o No
Are screen doors provided on all entrances left open to the outside? ..........................................
o Yes ...............
o No .................
o N/A
Do all openable windows have a minimum #16 mesh screening?................................................
o Yes ...............
o No .................
o N/A
Will all pipes and electrical conduit chases be sealed; ventilation systems exhaust and intakes protected? .................................................................................................................
o Yes ...............
o No .................
o N/A
Is area around building clear of unnecessary brush, litter, boxes and other harborage? .............
o Yes ...............
o No .................
o N/A
Will air curtains be used? .............................................................................................................
o Yes ...............
o No .................
o N/A
If YES, where? ______________________________________________________________________________________________
Who will be the pest control provider for the establishment? ___________________________________________________________
Garbage and Refuse:
Do all garbage containers, located inside, have lids? ...................................................................
o Yes ...............
o No
Is there an area designated for garbage can or floor mat cleaning? ............................................
o Yes ...............
o No .................
o N/A
Will a dumpster be used? .............................................................................................................
o Yes ...............
o No
If YES, how many will be used and how frequent is pickup? ___________________________________________________________
Do all dumpsters have closeable lids? ..........................................................................................
o Yes ...............
o No .................
o N/A
Will garbage cans be stored outside? ...........................................................................................
o Yes ...............
o No .................
o N/A
Will a compactor be used? ...........................................................................................................
o Yes ...............
o No .................
o N/A
Are all dumpsters, compactors, cans, and grease disposal containers located on concrete or asphalt? ................................................................................................................
o Yes ...............
o No
Is the dumpster shared by more than one business? ...................................................................
o Yes ...............
o No .................
o N/A
If YES, list all businesses utilizing dumpster: _______________________________________________________________________
___________________________________________________________________________________________________________
V. Miscellaneous
Laundry:
Will linens be laundered on site? ..................................................................................................
o Yes ...............
o No .................
o N/A
Is a laundry dryer available? .........................................................................................................
o Yes ...............
o No .................
o N/A
Where will clean linen be stored? ________________________________________________________________________________
Where will dirty linen be stored? _________________________________________________________________________________ page 11
V. Miscellaneous
(continued)
Sanitizing:
(PPM = parts per million)
How will utensils and equipment be sanitized (list the concentration) in the three compartment sink?
........................
o Chlorine ______ ppm
How will utensils and equipment be sanitized (list the concentration) in the dish machine?
...........................................
o Other _____________________, ______ ppm o o
Chlorine ______ ppm o Quat ______ ppm o Quat ______
Other _____________________, ______ ppm ppm o o
Hot Water ______°F
N/A o Hot Water ______°F o N/A
How will cooking equipment, cutting boards, counter tops, and other food contact surfaces which cannot be submerged in sinks or put through the dish machine be sanitized (list the concentration)? ........................................
o Chlorine ______ ppm o Quat ______ ppm o Other _______________________, ______ ppm
Will test strips be provided to measure the concentration strength? ............................................................................
o Yes ...........
o No
Toxics:
Are insecticides/rodenticides/herbicides stored separately from cleaning and sanitizing agents? ...............................
o Yes ...........
o No
Are all toxics for use on the premises or for retail sale (this includes personal medication), stored away from food preparation and storage areas? ...............................................................................................
o Yes ...........
o No
Are all containers of toxics including spray bottles clearly labeled? .............................................................................
o Yes ...........
o No
By signing, I certify that the above information is correct and I fully understand the following:
• The plan review expires one year from the date of approval. If construction or remodeling is not started within that time period, it may be necessary to resubmit for a new review of the plans.
• Any changes or alterations to plans must have prior approval by the Peoria
City/County Health Department.
• Approval of these plans by the Peoria City/County Health Department does not indicate compliance with any other code, law, or regulation that may be required. It further does not constitute endorsement or acceptance of the completed establishment.
• A final inspection of the establishment with equipment in place and operational will be necessary to determine if it complies with the Illinois
Department of Public Health Food Service Sanitation Code, before operations can begin.
page 12
________________________________________________________ ________________
Owner Signature Date
Revised 11/15