A COMPARATIVE STUDY OF RAPID PALATAL EXPANSION
IN THE DECIDUOUS AND MIXED DENTITIONS
Andrew W. Foster, D.D.S.
A Thesis Presented to the Graduate Faculty of
Saint Louis University in Partial Fulfillment
Of the Requirements for the Degree of
Master of Science in Dentistry
2015
© Copyright by
Andrew Warren Foster
ALL RIGHTS RESERVED
2015
i
COMMITTEE IN CHARGE OF CANDIDACY:
Professor Eustaquio A. Araujo,
Chairperson and Advisor
Professor Rolf G. Behrents
Associate Professor Ki Beom Kim
ii
DEDICATION
This thesis represents the culmination of my entire
educational career. Of all the lessons I have learned over
that time, possibly the most important is that nothing of
any real worth can be done alone. So, for all those who
have influenced me, guided me, and inspired me along the
way, I will work my entire professional life to show you my
gratitude.
No one is more deserving of this gratitude than my
wife, who has been with me every step of the way. Kristen,
from kindergarten through high school you put up with me,
and from our marriage to now, you have kept me afloat. You
are my rock, my reason, my life. I dedicate this thesis and
all it represents to you. It’s been a long time coming!
Thank you also to our children: Melanie, Abigail,
Lacey, and Blakely for the added depth you have provided my
life. You balance and enrich everything I do.
Lastly, I dedicate and acknowledge the profound impact
my parents, my brothers, my sisters, my friends and my God
have had on the direction of my life. I know it wasn’t
always easy, but thank you for teaching me the principles I
hold so dear.
iii
ACKNOWLEDGEMENTS
This thesis could not have been completed without the
help and support of the following individuals:
Dr. Eustaquio Araujo for your guidance, laughter, and
experienced insights.
Dr. Rolf Behrents for your leadership and attention to
detail.
Dr. Ki Beom Kim for your friendship, unbiased analysis
and listening ear.
Dr. Bernardo Souki for providing the crucial samples
that made this project possible. You went the extra mile
for this project, and for that I am truly grateful.
Dr. Patrick Foley for going out of your way to see the
things I missed.
Jared Little for making the control sample extremely
accessible and for working in such a timely manner on all
my out-of-the-box requests.
Dr. James McNamara for maintaining such a powerful
resource as The Michigan Growth Study.
Dr. Heidi Israel for guiding me through the confusion
that is statistics.
The entire SLU CADE community for all the support,
work, and guidance. This really is a special place!
iv
TABLE OF CONTENTS
LIST OF TABLES........................................... vi
LIST OF FIGURES......................................... vii
CHAPTER 1: INTRODUCTION................................... 1
CHAPTER 2: REVIEW OF THE LITERATURE
HISTORY OF PALATAL EXPANSION .................. 4
INDICATIONS FOR EXPANSION WITH CROSSBITE ...... 6
INDICATIONS FOR EXPANSION WITHOUT CROSSBITE ... 8
ANATOMY OF THE MID-PALATAL SUTURE ............ 11
TIMING OF EXPANSION .......................... 13
EXPANSION EFFECTS ON MID-PALATAL SUTURE ...... 14
SKELETAL EFFECTS OF EXPANSION ................ 16
DENTAL EFFECTS OF EXPANSION .................. 18
LONG-TERM STABILITY .......................... 21
RPE USE IN THE DECIDUOUS DENTITION ........... 22
SUMMARY AND STATEMENT OF THESIS .............. 25
REFERENCES ................................... 27
CHAPTER 3: JOURNAL ARTICLE
ABSTRACT .....................................
INTRODUCTION .................................
MATERIALS AND METHODS ........................
Sample Description........................
RPE Protocol in Experimental Groups.......
Measurements..............................
Palatal Surface Area......................
Palatal Volume............................
ERROR OF METHODS .............................
STATISICAL ANALYSIS ..........................
RESULTS ......................................
Palatal Surface Area......................
Palatal Volume............................
DISCUSSION ...................................
CONCLUSIONS ..................................
REFERENCES ...................................
33
35
38
38
41
43
43
44
47
47
47
47
49
51
61
62
VITA AUCTORIS............................................ 66
v
LIST OF TABLES
Table 3.1:
Sample Demographics, Gender and Age.......39
Table 3.2:
Age Break Down at each time point.........40
Table 3.3:
Sample Demographics, Presence of
Crossbite.................................40
Table 3.4:
Expansion and Retention Protocol..........42
Table 3.5:
Palatal Surface Area, means...............49
Table 3.6:
Palatal Surface Area, mm2 increase ........49
Table 3.7:
Palatal Surface Area, percent increase....49
Table 3.8:
Palatal Volume, means.....................51
Table 3.9:
Palatal Volume, mm3 increase ..............51
Table 3.10:
Palatal Volume, percent increase..........51
vi
LIST OF FIGURES
Figure 2.1:
Sketch of Angell’s 1860 appliance..........4
Figure 2.2:
Representation of sutural anatomy.........12
Figure 2.3:
Diagrammatic illustration of frontal
sections through the mid-palatal suture
at different ages.........................14
Figure 2.4:
Reaction of central incisors to RPE.......20
Figure 3.1:
Example of appliances used in the
experimental groups.......................41
Figure 3.2:
Dental models as displayed in Geomagic
Control...................................43
Figure 3.3:
Examples of palatal surface area
measurement…..............................44
Figure 3.4:
Anterior point used to define the 3-point
plane for calculating palatal volume......45
Figure 3.5:
Example of palatal volume measurement.....46
vii
CHAPTER 1: INTRODUCTION
Transverse maxillary deficiency is a common problem
found in orthodontic patients of all ages.
Currently, a
myriad of appliances and techniques are used to correct it,
with most employing some form of rapid palatal expansion
(RPE).
In fact, in modern orthodontics RPE has become a
standard of treatment for many practitioners in the United
States and throughout world.1
Yet, even with this
widespread use, controversy and disagreement seem to follow
RPE.
Even at its recorded inception in 1860,2 controversy
and skepticism hindered its acceptance as many prominent
figures in dentistry of that time dismissed and discredited
the fundamental notion of palatal separation.3,4
Today,
although palatal separation is now unquestionably accepted
as possible,5-7 many other questions regarding RPE remain
undecided and often controversial.8,9
Of these, perhaps the most pertinent to an orthodontic
clinician is this: when is the proper time to employ RPE so
as to maximize transverse gain and minimize possible
complications, patient discomfort, and relapse?
Much has
been written on this topic and a consensus reached with
regard to the mixed dentition:
that with proper diagnosis,
the earlier expansion can be completed the better.10
1
This
notion is based on anatomical11,12 and clinical10 studies
showing that as a child ages, the mid-palatal suture
increases its resistance to separation.
So if earlier is
better, why not use RPE in the deciduous dentition?
In
other words, could there be advantages to using RPE in the
deciduous dentition versus employing it in the mixed
dentition?
Historically, studies concerned with RPE in the
deciduous dentition have focused on the presence and
subsequent correction of posterior crossbites as the only
reliable, measurable and consistent variable available to
them.13-18
This is most likely due to the inherent
difficulty in comparing the deciduous to the
mixed/permanent dentition because, by the time a child is
ready for phase II treatment, all deciduous teeth that were
present have been replaced by an entirely new set of
permanent teeth.
The variations in both size and position
of these new permanent teeth make the linear tooth-to-tooth
measurements traditionally used as measures in studies of
transverse gain by RPE (i.e. inter-molar or inter-canine)
essentially meaningless.
Recently a group of authors published a series of
articles on the topic of RPE in the deciduous dentition.19-22
With the advent of digital technology, these studies used
2
the relatively new variables of palatal surface area and
palatal volume to quantify the effects of RPE in the
deciduous dentition of children with posterior crossbites
as compared to children without posterior crossbites.
These studies showed a significant gain in both palatal
surface area and palatal volume, as well as increased
palatal and facial symmetry with RPE use in the deciduous
dentition.22
While quite useful, these studies did not directly
compare RPE use in the deciduous dentition to that in the
mixed dentition.
In addition, these studies did not follow
these children beyond 30 months post expansion to the time
point when most orthodontic clinicians would want to see
the effects of their phase I RPE treatment—the start of
phase II treatment.
In fact, no studies to date have
utilized the measures of palatal surface area and palatal
volume to see if significant differences in palatal vault
dimensions can be seen at the start of phase II
comprehensive treatment whether RPE was completed in the
deciduous dentition or the mixed dentition.
This present
study seeks to shed light on this important topic.
3
CHAPTER 2: REVIEW OF THE LITERATURE
HISTORY OF PALATAL EXPANSION
The origins of RPE can be traced back to Emerson Colon
Angell (1822-1903) who, following a short career as a
teacher, began studying dentistry in 1846.
In 1860, from
his dental practice in San Francisco, he published an
article entitled Treatment of irregularity of the permanent
or adult teeth.2
This article included a case report in
which a 14-year-old girl was fitted with an appliance that
featured two contra-rotating screws.
In many ways, this
appliance is strikingly similar to some of the appliances
commonly used today (See Figure 2.1).
Figure 2.1: A sketch taken directly from Angell's 1860 Dental
Cosmos article of his appliance design.2
4
In the article, Angell claimed that the correction he
achieved in the two weeks of appliance activation, which
correction was creating space for a labially blocked out
canine, was by separation of the maxilla along the midpalatal suture.
This finding was largely criticized and
dismissed by the orthodontic establishment of the time,
most vocally by J.H. McQuillen, a highly respected dentist
and a future American Dental Association president.
It
wasn’t until 1893 when Professor Clark Goddard presented a
paper to the World’s Columbian Dental Congress entitled
Separation of the Superior Maxilla at the Symphysis that
legitimacy of RPE began to be established.3
Even with this budding legitimacy, palatal separation
and expansion was not widely used or acknowledged as a
common treatment modality in the United States until the
mid-1960s, when Andrew Haas began to once again publish on
the subject.
Haas credits such names as Goddard (1893),
G.V. Black (1893), and Hawley (1912) with keeping
discussion of RPE alive in the orthodontic literature, yet
RPE remained largely unused and unappreciated in the United
States. This was partially because of opposition from
McQuillen (1890), Farrar (1888), and Federspiel (1914), as
well as general indifference to the procedure provided by
such notable names as Angle, Case, Ketcham, and Dewey.
5
All
of these individuals generally believed that even if
palatal expansion was possible, the risk was too high given
that the same effect could be achieved with arch wire.23
Among European orthodontists, the utilization of RPE was
more common during this time period.
Haas credits one of these European practitioners, G.
Korkhaus, with reintroducing RPE again to the United
States.4
In 1956, Korkhaus visited The University of
Illinois (where Haas was employed at the time) and sparked
a curiosity in him.
This led Haas, with the advent of
photography and radiography, to begin a flood of research
on the topic of RPE.
This momentum, started largely by
Haas and carried over by other subsequent authors, is
responsible for RPE’s presently comfortable place among
accepted orthodontic treatments in the United States and
throughout the world.
INDICATIONS FOR EXPANSION WITH CROSSBITE
Traditionally, RPE has been used to correct maxillary
transverse discrepancies—arguably one of the most
persistent craniofacial problems encountered by
orthodontists.
Often the most obvious sign or symptom of
transverse maxillary deficiency is a posterior crossbite,
6
which can present clinically as either unilateral or
bilateral.
A posterior crossbite can have various causes:
skeletal (narrow maxillary or wide mandibular base),
dental, or a combination of both.
Many conditions have
been proposed as contributing factors to posterior
crossbites including genetics, congenital abnormalities
like cleft lip/palate, habits like prolonged pacifier use,
early cessation of breastfeeding, short lingual frenulum
resulting in low tongue posture, early loss of teeth and
incorrect sleep posture.24,25
Whatever the etiology may be,
a proper and thorough diagnosis is imperative before
prescribing any treatment.
Once diagnosed properly, the presence of a functional
shift and its possible adverse side effects has been cited
as reasons to treat posterior crossbites as early as
possible.
These side effects include: asymmetrical growth
of the condyles and associated facial structures, facial
asymmetries, possible adverse temporomandibular joint
effects, and disturbed masticatory musculature
activity.14,22,26-28
Others provide normalizing growth as a
reason for early correction.29
7
INDICATIONS FOR EXPANSION WITHOUT CROSSBITE
Although the majority of practitioners will cite
posterior crossbites as the main diagnostic criterion when
deciding to use RPE, there are other clinical conditions
that may merit RPE consideration even in the absence of a
posterior crossbite.9,30,31
While predominantly associated
with the mixed dentition, many of these same conditions may
also be present in the deciduous dentition.
One of these conditions is crowding.
McNamara31
suggests that in the mixed dentition “a maxillary arch with
a trans-palatal width of 36 to 39 mm can accommodate a
dentition of average size without crowding or spacing,
whereas maxillary arches less than 31 mm in width may be
crowded and thus in need of orthopedic or surgically
assisted expansion.”
He goes on to say that “other
factors, such as facial type, soft tissue profile, and
level of muscle tonus, also must be taken into
consideration” when considering RPE for crowding.
Adkins et al.30 sought to quantify exactly how much
arch perimeter gain one can expect through RPE.
In their
study of dental casts they found that 0.7 mm of perimeter
gain can be expected for every 1 mm of maxillary premolar
expansion.
Although not sufficient in severely crowded
8
cases, the authors suggest this predictive knowledge may
help facilitate more non-extraction treatments in
moderately crowded individuals.
While some concur,32,33
others question the long-term stability of RPE treatment
for crowding.8,9
The absence of a posterior crossbite does not exclude
transverse maxillary deficiency from being present.
It is
well understood that the dentition will camouflage skeletal
discrepancies by dentoalveolar compensation.
In the case
of transverse maxillary deficiency, this presents in the
form of laterally tipped maxillary posterior teeth and is
oftentimes accompanied by lingually inclined mandibular
teeth.
In addition, as the maxillary teeth flare bucally,
the prominence of the maxillary molar palatal cusps
increase, and an exaggerated curve of Wilson is expressed.
This may lead to balancing interferences during function.
It can be surmised then that although these persons may not
present clinically with posterior crossbites, they may
benefit from RPE nonetheless.
It has been suggested that another sign of transverse
maxillary deficiency is large negative space at the corners
of the mouth during smiling (commonly referred to as
“buccal corridors”).
Many factors may also be associated
with this clinical presentation: such as muscle tone, soft
9
tissue position, lip size, and dynamic smile
characteristics.
McNamara31 suggests though, that a
“tapered maxilla” may be a major contributor to exaggerated
buccal corridors.
He explains that:
Regardless of whether teeth are extracted, the maxilla
can be widened by means of RME (Rapid Maxillary
expansion), increasing transpalatal width and
eliminating or reducing the dark spaces in the ‘buccal
corridors’. This type of orthopedic intervention
results in what many consider a more pleasing frontal
facial smile.
While empirically obvious, there is scarce evidence to show
whether RPE alone can have any meaningful long-term effect
on buccal corridor width.
Lastly, while many perceive Class II and Class III
malocclusions as sagittal problems alone, some point to the
transverse deficiency commonly co-present as a point of
emphasis.
McNamara31 points to a “spontaneous Class II
correction” that often takes place 6-12 months after RPE.
He postulates that as “over expansion” is first performed
and then held via a transpalatal arch, the patient will
tend to hold the jaw forward in a more Class I relationship
to correct the newly introduced buccal crossbite.
Over
time, mandibular growth will then make this postural change
permanent. Gianelly9 questions the use of RPE for this
spontaneous correction by citing the lack of evidence of it
actually occurring, as well as the fact that 56% of
10
terminal plane relationships will convert to Class I during
the normal transition from deciduous to permanent dentition
without any orthodontic intervention.
ANATOMY OF THE MID-PALATAL SUTURE
In terms of anatomy, the mid-palatal suture varies
little from the other sutures of the facial skeleton.
Ten
Cate et al.34 suggested that sutural anatomy can best be
described in terms of the functionality of two cell
populations: the osteocytic and the fibrocytic. These
authors explained that individual differences in fiber
orientation, structure, and vascular distribution are
merely a representation of the functional state of that
particular suture at a certain time point of development,
rather than true anatomical characteristics.
In contrast, Pritchard et al.35 clearly defined suture
anatomy (See Figure 2.2) by describing distinct layers of
cells and fibers present in all facial sutures no matter
the stage of development, although each layer does change
depending on the level of maturity.
These layers were
divided into two broad groups, termed intervening and
uniting.
The intervening group consisted of two cambial
layers, two periosteal fibrous capsule layers and a loose
cellular mesenchyme between these termed the middle layer.
11
The uniting group was described as continuous with the
outer fibrous portions of periosteum from each
approximating bone.
Together, the intervening layers and
uniting layers bind the suture both internally and
externally.
Figure 2.2: Representation of sutural anatomy (adapted from
Pritchard et al.)35
The cambial layer, made up of collagen fibers running
radial from the bone to the fibrous capsule layer, is the
site of osteogenesis.
Early in development, this layer
includes multiple layers of cells within it.
As a person
ages and growth slows, the cambial layer is eventually
reduced until it consists of only a single layer of
flattened osteoblasts.
Because of this, during growth the
fibrous capsule layer must expand to keep pace with this
12
proliferating cambial layer.
Eventually obliteration and
synostosis occur, although there is wide variance in
specific timing for each individual suture.
Specific to
the mid-palatal suture, some persons may exhibit
obliteration earlier, but a marked degree of closure is
rarely present until the third decade of life.36
TIMING OF EXPANSION
Melsen and Melsen11,12 conducted a study in which they
utilized autopsy material to histologically examine the
maturation of the mid-palatal suture at different
developmental stages.
In the “infantile” stage (0-10
years) the suture was broad and smooth while the “juvenile”
stage (10-13 years) showed a more squamous suture with
overlapping sections.
In the “adolescent” stage (13-14
years) the suture showed an increase in interdigitation.
(See Figure 2.3)
Finally, in the “adult” stage synostosis
and boney bridge formations were present.
The implications
of these findings are obvious: that as a child ages, the
efficacy of RPE will decrease and eventually become a near
impossibility without surgery.
be true clinically.10
13
Others have shown this to
Figure 2.3: Diagrammatic illustrations of frontal sections
through the mid-palatal suture at the different stages. (A) Shows
an example of the “infantile” stage (0-10 years), (B) shows an
example of the “juvenile” stage (10-13 years) and (C) shows an
example of the “adolescent” stage (13-14 years). Notice not only
the increase in sutural interdigitation, but also the increase in
vertical height of the suture over time. Adapted from Melsen’s
study on human autopsy material.11
EXPANSION EFFECTS ON MID-PALATAL SUTURE
Is it possible then to influence the normal growth of
the mid-palatal suture?
Cleall et al.7 used rhesus monkeys
fitted with expanders to answer this question. They
demonstrated that soon after the application of force a
radiographic hypo-mineralized defect appeared in the midpalatal area.
This defect quickly filled in with new bone
until it became indistinguishable from that of the initial
radiographic and histologic appearance.
This normalcy
remained even after removal of the retention appliance.
Ten Cate et al.34 showed similar results, noting that in
other tissues of the human body this initial injurious
insult to the suture would heal with scar tissue, but due
14
to the connective tissue fibroblasts ability to remodel
within the mid-palatal suture, true regeneration takes
place instead.
Krebs37 was also able to demonstrate expansion of the
mid-palatal suture in humans by utilizing metallic implants
placed in the zygomatic process of the maxilla and hard
palate.
He compared expansion of the maxillary base (as
measured by the implants) and the dental arch (as measured
from casts).
A rapid increase was noted in both, but a
much higher amount of relapse occurred in the dental arch
versus the maxillary base.
He stated that:
The effect of rapid expansion on the suture appeared
to be dependent on sex and age, being greater during
the pubertal period. Apart from a slight but rapid
relapse, the attained increase in the width of the
maxillary base seemed to be stable. A further increase
in width of this zone after the active treatment took
place as a result of natural growth in the median
plane suture.
It appears then that forces applied by orthodontic
appliances can induce a real separation of the mid-palatal
suture and that this separation is quickly (within a few
months) filled in with new bone.
The anatomy of the
treated suture is nearly indistinguishable from that of an
untreated suture and is stable over time.
When the whole
dental facial complex is taken as a whole though, it is
clear that a tendency for relapse is present.
15
SKELETAL EFFECTS OF EXPANSION
In general, it is the goal of most treatments
utilizing RPE to minimize dental and maximize skeletal
effects.
While there are varying designs, a tooth-born
appliance, as opposed to an implant born appliance, has
historically been the appliance most widely used. This
study will not consider any implant supported RPE designs
or their effects.
RPE with a tooth-born type of expander occurs when
force is applied to the anchor teeth and transmitted to the
corresponding alveolar bone.
This force is then translated
to the mid-palatal suture as the periodontal ligaments of
the anchor teeth are compressed.
The teeth then tip, the
alveolar process bends, and gradual separation occurs.38
This separation, when viewed from beneath the occlusal
plane, is not parallel but wedge shaped, with more
expansion in the anterior. When measured at ANS and PNS,
the ratio of separation has been found to be 3 to 2, and
even 2 to 1 in some cases.6,37
This non-parallel opening has
been attributed to the buttressing effect of the zygomatic
arch. In addition, the absence of a mid-sagittal suture on
the sphenoid bone which lies directly posterior to the
maxilla has also been offered as an explanation. The
rigidity of the sphenoid bone is then transferred
16
anteriorly through the interlocking of the pyramidal
process of the palatine bone and pterygoid plates of the
sphenoid, making separation more difficult in the
posterior.6,38
When viewed from the front, separation is also seen as
a wedge, with the apex approximating the frontonasal
suture.
This results in more expansion at the level of the
occlusal plane than at the level of the maxillary alveolar
base or palatal shelves.
In fact, expansion of the suture
has been reported to be no more than half, and often below
one-fourth of dental expansion measured from molar to
molar.37-39
This wedge effect is at least partly responsible
for the differential expansion between dental and skeletal
units.
From a sagittal view, it has been found that
immediately following RPE the palate is displaced
inferiorly, more so at ANS than at PNS, causing a slight
clockwise rotation of the palatal plane.
Along with moving
down, most agree that A-point moves slightly forward.4,39-41
However, Sarver and Johnston42 reported some cases showing
either no anterior-posterior movement or even some
posterior movement.
In any case, the stability of these
movements in the long-term is at best questionable.33
17
With regards to the vertical dimension, it is
generally agreed upon that the mandibular plane angle will
increase secondarily to the mandible swinging down and
back, although some may argue the magnitude of this effect
can be controlled by appliance design.42
This tendency to
increase the lower facial height is most likely due to
interferences introduced by the accentuation of the Curve
of Wilson and lengthening of the palatal cusps of upper
posterior teeth due to tipping and alveolar bone bending.38
DENTAL EFFECTS OF EXPANSION
Chung and Font39 measured the exact amount of expansion
achieved in an expander screw and compared it to the
measured expansion on both radiographs and dental casts.
They found that inter-premolar and inter-molar expansion
was 110.7% and 104.5% respectively of the measured screw
expansion.
Yet, the inter-maxillary width, as measured
from buccal plate to buccal plate, was 30.1%. What could be
the reason for these differences?
The answer lies in the
fact that not only is RPE affecting the skeleton, but the
dentition as well.
In fact, dental effects play a
significantly larger role in the clinical presentation of
palatal expansion than skeletal effects.41,43
18
The teeth anchored to any type of expansion appliance
show buccal crown tipping.
Generally this tipping has been
measured to be between 3-8 degrees.30,39,41
This, along with
alveolar bone bending and the wedge effect of expansion,
help account for the difference of expansion between midpalatal suture expansion and clinically evident expansion
as noted by inter-molar or inter-premolar distances.
Along
with this dental and alveolar tipping, .5 mm of extrusion
of the anchor teeth is also seen.38,43
With regard to the anterior teeth, the maxillary
incisors tend to retrocline with a small amount of
extrusion, although some have reported proclination as
well.
This retroinclination is reported to be in the range
of 0.5° to 2.5° when measured from the maxillary incisors
to the sella-nasion plane.6,39,40,42,43
This palatal tipping is
thought to be caused by the stretched musculature of the
oral-facial complex on the newly aligned dentition.4,6,38
Perhaps the most distinctive indicator of RPE is the
formation of a maxillary midline diastema.
It is estimated
that during suture opening, the upper incisors separate
half the distance of screw expansion.4
Although this can be
quite shocking to a patient, within 4-5 months following
cessation of expansion, the incisors once again reestablish
their approximate pre-expansion angulation and orientation
19
within the dental arch (See Figure 2.4).
If a midline
diastema existed prior to RPE, then this space will be
maintained or perhaps slightly reduced.
It is postulated
that the elastic recoil of the trans-septal fibers running
between the maxillary central incisors accounts for this
mesial movement back to normal.4,38
Figure 2.4: Reaction of central incisors to RPE (adapted from
Haas)5
Although no active force is applied to the mandibular
arch, uprighting of the buccal segments has been
reported.4,44
As recently as 2001, Haas reported that “when
the maxillae are separated 12-14 mm, noticeable spontaneous
expansion will occur in the lower dental arch, due to
altered muscle balance between the tongue and buccinators
muscles.
That is, a permanent increase in maxillary apical
base leads to spontaneous, permanent and significant
increase in mandibular arch width.”44
20
Lima et al.44 showed this in a study where a sample of
30 patients, all in the early to mid-mixed dentition and
treated only with RPE, were longitudinally followed up to
the age of 20.
Even with no orthodontic appliance used in
the mandibular arch, these patients showed a statistically
significant increase in inter-molar width of 1.39 mm
attributable to RPE after normal growth was accounted for.
However no increase in inter-canine width was noted.
LONG-TERM STABILITY
Despite the many years of RPE use and the many studies
devoted to its effects, the stability of RPE remains up for
debate.
In the past 15 years several meta-analyses and
systemic reviews have been conducted seeking to shed light
on this issue.
Problems arise in the many confusing
definitions, lack of uniformity in study design and
measurement type, poorly explained reasons for RPE (i.e.
relief of crowding vs maxillary transverse deficiency) and
others.
Because of this, most reviews have not reached any
strong conclusions.
In the year 2000, Schiffman and Tuncay8 conducted a
meta-analysis and found that there is insufficient data to
conclude that any useful expansion beyond what can be
21
expected from normal growth is retained following RPE.
They concluded that:
A weighted expansion of 6 mm can be expected to
decrease by 40% within five years. The original 6 mm
will be between 3 and 4 mm by this time. An increase
of 3 mm can be expected due to growth between the ages
of 10 and 18, so that of the 3-4 mm [of] residual
expansion, no more than 1 mm can be attributed to
anything other than growth.
Others have reached different conclusions. In 2005
Lagravere at el.33 found, by way of a systematic review,
that a long-term maxillary intermolar increase of 3.7-4.8
mm can be seen after use of RPE.
In another study, Doyle32
found that “despite post retention relapse, treatment
changes, when compared to established referenced data,
showed significant increases for maxillary and mandibular
arch widths” after 15 years post RPE treatment.
RPE USE IN THE DECIDUOUS DENTITION
It is generally agreed upon that the younger a person
is, the more effective and predictable RPE will be.6,10
This
agreement though, is generally reserved for the mixed
dentition.
To date, very little has been written on the
subject of RPE in the deciduous dentition, with much of the
literature focused on early correction of and/or prevalence
22
of posterior crossbites in the deciduous
dentition.16,17,24,45,46
These investigations show the prevalence of crossbites
in the deciduous dentition to be between 7%-23%,17,24,45,46
making it one of the more common orthodontic problems
encountered in young children.
Wide variation exists in
reports of spontaneous self-correction as well (8%-45%)
when transitioning to the mixed dentition.13,24,47
Most
authors suggest that in the majority of cases, a posterior
crossbite will not correct without some form of orthodontic
intervention and that the treatment of choice for a
posterior crossbite in the deciduous dentition is selective
grinding on the teeth, followed by expansion with low
forces (i.e. quad helix) if grinding proves
unsuccessful.13,17,48
More recently, Primozic et al.20-22 has advocated for
the use of RPE in the deciduous dentition for correction of
posterior crossbites by showing the benefits in a
prospective clinical trial using children approximately
five years old.
With the use of 3D dental study casts as
well as laser scans of these same children’s faces, they
demonstrated not only a significant, long-lasting change in
palatal surface area and volume, but also a significant
reduction in facial and palatal asymmetries. These positive
23
changes made them nearly indistinguishable from the control
group.
Although the posterior crossbites relapsed at a
rate of 26.7% at 30 months post expansion, other
improvements were noted such as normalization of
masticatory pattern and function, as well as normalization
of palatal growth.
The lack of long-term follow-up (the
children are only 7 ½ years old at last records) leaves
unanswered whether these positive findings last beyond what
can be achieved by normal growth and development or by RPE
use later in the mixed dentition stage.
There are those who argue against the routine use of
RPE in the deciduous dentition as well.
Profitt1 reports
that RPE performed too early may lead to deleterious
effects such as nasal humps and paranasal swelling. Others
point to reports that self-correction of posterior
crossbites may occur in up to 45% of children with
posterior crossbite, and that from a cost-benefit
standpoint, treatment of any kind at such a young age is
questionable.45
They point to the expense, the need for two
phases of treatment, less cooperation and maturity of
younger children, and lack of clinically significant
differences in results when compared to RPE performed at a
later stage as reasons to wait for treatment unless
function or esthetics are compromised.
24
SUMMARY AND STATEMENT OF THESIS
Since Angell first purposed the idea of maxillary
separation along the mid-palatal suture, there has been
skepticism and disagreement.
Although much study has been
devoted to the use of RPE in the mixed dentition (its
effects, stability, and cost effectiveness) far less has
been dedicated to its utilization in the deciduous
dentition.
The literature that does exist has been focused
almost exclusively on posterior crossbite correction and
the stability of that correction.
This is likely
attributable to the fact that linear measurements based off
teeth (i.e. inter-molar or intercanine) were not a reliable
way to measure the effects of RPE in the deciduous
dentition when compared to the mixed dentition because of
the natural changes that occur during the transition of
teeth.
But with the advent of laser and computer
technology, it is now possible to measure palatal changes
in both two and three dimensions, making comparisons not
only possible but meaningful.
Although palatal surface area and palatal volume have
been shown to be reliable and effective ways to measure
effects of RPE,29,49 it has yet to be used to directly
compare RPE in the deciduous dentition to that of RPE in
25
the mixed dentition.
The aim of this present study is to
use dental casts of patients who underwent RPE at two
specific time periods, the deciduous dentition (~5 years
old) and the mixed dentition (~8 years old), and compare
them when those same patients are deemed ready for phase II
orthodontic treatment (~12 years old).
With the use of a
control group, this study will attempt to not only show if
posterior crossbite correction is reliable in the deciduous
dentition, but also if at the start of comprehensive phase
II orthodontic treatment, there are differences in palatal
dimensions whether RPE was completed in the deciduous
dentition or the mixed dentition.
26
REFERENCES
1.
Profitt WR. Contemporary Orthodontics. 5 ed. St.
Louis, Missouri: Mosby; 2013.
2.
Angell E. Treatment of irregularity of the permanent
or adult teeth. Dental Cosmos. 1860;1:540-4, 99-600.
3.
Timms DJ. The dawn of rapid maxillary expansion. Angle
Orthod. 1999;69(3):247-50.
4.
Haas AJ. The treatment of maxillary deficiency by
opening the midpalatal suture. Angle Orthod.
1965;35:200-17.
5.
Haas AJ. Rapid expansion of the maxillary dental arch
and nasal cavity by opening the midpalatal suture.
Angle Orthod. 1961;31(2):73-90.
6.
Wertz RA. Skeletal and dental changes accompanying
rapid midpalatal suture opening. Am J Orthod.
1970;58(1):41-66.
7.
Cleall JF, Bayne DI, Posen JM, Subtelny JD. Expansion
of the midpalalal suture in the monkey. Angle Orthod.
1965;35:23-35.
8.
Schiffman PH, Tuncay OC. Maxillary expansion: a meta
analysis. Clin Orthod Res. 2001;4(2):86-96.
9.
Gianelly AA. Rapid palatal expansion in the absence of
crossbites: added value? Am J Orthod Dentofacial
Orthop. 2003;124(4):362-5.
10.
Baccetti T, Franchi L, Cameron CG, McNamara JA, Jr.
Treatment timing for rapid maxillary expansion. Angle
Orthod. 2001;71(5):343-50.
27
11.
Melsen B. Palatal growth studied on human autopsy
material. A histologic microradiographic study. Am J
Orthod. 1975;68(1):42-54.
12.
Melsen B, Melsen F. The postnatal development of the
palatomaxillary region studied on human autopsy
material. Am J Orthod. 1982;82(4):329-42.
13.
Lindner A. Longitudinal study on the effect of early
interceptive treatment in 4-year-old children with
unilateral cross-bite. Scand J Dent Res.
1989;97(5):432-8.
14.
Malandris M, Mahoney EK. Aetiology, diagnosis and
treatment of posterior cross-bites in the primary
dentition. Int J Paediatr Dent. 2004;14(3):155-66.
15.
Ninou S, Stephens C. The early treatment of posterior
crossbites: a review of continuing controversies. Dent
Update. 1994;21(10):420-6.
16.
Petren S, Bondemark L, Soderfeldt B. A systematic
review concerning early orthodontic treatment of
unilateral posterior crossbite. Angle Orthod.
2003;73(5):588-96.
17.
Thilander B, Wahlund S, Lennartsson B. The effect of
early interceptive treatment in children with
posterior cross-bite. Eur J Orthod. 1984;6(1):25-34.
18.
Tsarapatsani P, Tullberg M, Lindner A, Huggare J.
Long-term follow-up of early treatment of unilateral
forced posterior cross-bite. Orofacial status. Acta
Odontol Scand. 1999;57(2):97-104.
19.
Primozic J, Ovsenik M, Richmond S, Kau CH, Zhurov A.
Early crossbite correction: a three-dimensional
evaluation. Eur J Orthod. 2009;31(4):352-6.
28
20.
Primozic J, Perinetti G, Richmond S, Ovsenik M. Threedimensional longitudinal evaluation of palatal vault
changes in growing subjects. Angle Orthod.
2012;82(4):632-6.
21.
Primozic J, Baccetti T, Franchi L, Richmond S, Farcnik
F, Ovsenik M. Three-dimensional assessment of palatal
change in a controlled study of unilateral posterior
crossbite correction in the primary dentition. Eur J
Orthod. 2013;35(2):199-204.
22.
Primozic J, Richmond S, Kau CH, Zhurov A, Ovsenik M.
Three-dimensional evaluation of early crossbite
correction: a longitudinal study. Eur J Orthod.
2013;35(1):7-13.
23.
Dewey M. Development of the Maxillae with Reference to
the Opening the Median Suture. Dent Items Interest.
1913;35:189-208.
24.
Kutin G, Hawes RR. Posterior cross-bites in the
deciduous and mixed dentitions. Am J Orthod.
1969;56(5):491-504.
25.
Melink S, Vagner MV, Hocevar-Boltezar I, Ovsenik M.
Posterior crossbite in the deciduous dentition period,
its relation with sucking habits, irregular orofacial
functions, and otolaryngological findings. Am J Orthod
Dentofacial Orthop. 2010;138(1):32-40.
26.
Egermark-Eriksson I, Carlsson GE, Magnusson T,
Thilander B. A longitudinal study on malocclusion in
relation to signs and symptoms of cranio-mandibular
disorders in children and adolescents. Eur J Orthod.
1990;12(4):399-407.
27.
Troelstrup B, Moller E. Electromyography of the
temporalis and masseter muscles in children with
unilateral cross-bite. Scand J Dent Res.
1970;78(5):425-30.
29
28.
Ingervall B, Thilander B. Activity of temporal and
masseter muscles in children with a lateral forced
bite. Angle Orthod. 1975;45(4):249-58.
29.
Primozic J, Perinetti G, Contardo L, Ovsenik M.
Diagnostic performance of 3-dimensional evaluation of
palatal vault changes in assessing successful
treatment of constricted maxilla in growing subjects.
Am J Orthod Dentofacial Orthop. 2013;143(1):42-9.
30.
Adkins MD, Nanda RS, Currier GF. Arch perimeter
changes on rapid palatal expansion. Am J Orthod
Dentofacial Orthop. 1990;97(3):194-9.
31.
McNamara JA. Maxillary transverse deficiency. Am J
Orthod Dentofacial Orthop. 2000;117(5):567-70.
32.
Doyle R. Long-term stability in the maxillary and
mandibular arch dimensions using rapid palatal
expansion and edgewise mechanotherapy in growing
patients. [Masters Thesis]. In press 2012.
33.
Lagravere MO, Major PW, Flores-Mir C. Long-term
skeletal changes with rapid maxillary expansion: a
systematic review. Angle Orthod. 2005;75(6):1046-52.
34.
Ten Cate AR, Freeman E, Dickinson JB. Sutural
development: structure and its response to rapid
expansion. Am J Orthod. 1977;71(6):622-36.
35.
Pritchard JJ, Scott JH, Girgis FG. The structure and
development of cranial and facial sutures. J Anat.
1956;90(1):73-86.
36.
Persson M, Thilander B. Palatal suture closure in man
from 15 to 35 years of age. Am J Orthod.
1977;72(1):42-52.
37.
Krebs A. Midpalatal suture expansion studies by the
implant method over a seven-year period. Rep Congr Eur
Orthod Soc. 1964;40:131-42.
30
38.
Bishara SE, Staley RN. Maxillary expansion: clinical
implications. Am J Orthod Dentofacial Orthop.
1987;91(1):3-14.
39.
Chung CH, Font B. Skeletal and dental changes in the
sagittal, vertical, and transverse dimensions after
rapid palatal expansion. Am J Orthod Dentofacial
Orthop. 2004;126(5):569-75.
40.
Habeeb M, Boucher N, Chung CH. Effects of rapid
palatal expansion on the sagittal and vertical
dimensions of the maxilla: a study on cephalograms
derived from cone-beam computed tomography. Am J
Orthod Dentofacial Orthop. 2013;144(3):398-403.
41.
Ghoneima A, Abdel-Fattah E, Eraso F, Fardo D, Kula K,
Hartsfield J. Skeletal and dental changes after rapid
maxillary expansion: a computed tomography study. Aust
Orthod J. 2010;26(2):141-8.
42.
Sarver DM, Johnston MW. Skeletal changes in vertical
and anterior displacement of the maxilla with bonded
rapid palatal expansion appliances. Am J Orthod
Dentofacial Orthop. 1989;95(6):462-6.
43.
Lagravere MO, Heo G, Major PW, Flores-Mir C. Metaanalysis of immediate changes with rapid maxillary
expansion treatment. J Am Dent Assoc. 2006;137(1):4453.
44.
Lima AC, Lima AL, Filho RM, Oyen OJ. Spontaneous
mandibular arch response after rapid palatal
expansion: a long-term study on Class I malocclusion.
Am J Orthod Dentofacial Orthop. 2004;126(5):576-82.
45.
Kurol J, Berglund L. Longitudinal study and costbenefit analysis of the effect of early treatment of
posterior cross-bites in the primary dentition. Eur J
Orthod. 1992;14(3):173-9.
31
46.
Heikinheimo K, Salmi K. Need for orthodontic
intervention in five-year-old Finnish children. Proc
Finn Dent Soc. 1987;83(4):165-9.
47.
Leighton BC. Symposium on aspects of the dental
development of the child. 2. The early development of
cross-bites. Dent Pract Dent Rec. 1966;17(4):145-52.
48.
Ngan P, Fields H. Orthodontic diagnosis and treatment
planning in the primary dentition. ASDC J Dent Child.
1995;62(1):25-33.
49.
Gracco A, Malaguti A, Lombardo L, Mazzoli A, Raffaeli
R. Palatal volume following rapid maxillary expansion
in mixed dentition. Angle Orthod. 2010;80(1):153-9.
32
CHAPTER 3: JOURNAL ARTICLE
ABSTRACT
Introduction:
In the past, comparing the effects of
rapid palatal expansion (RPE) in the deciduous dentition
to those in the mixed dentition has proven difficult
because of the dental variability between the two
dentitions.
Purpose:
This study used digital technology
to determine if any differences in palatal dimensions can
be quantified at the start of phase II treatment whether
RPE is completed in the deciduous or mixed dentition.
Materials and Methods:
210 digital models were
collected, composed of 3 groups of 30 children each: a
deciduous expansion group (DE), a mixed expansion group
(ME), and a control group (CG).
These models were
compared at 3 time points: the deciduous dentition (T0),
the mixed dentition (T1) and the start of phase II
treatment (T2).
A single orthodontist treated each child
in the DE and ME groups by use of either a Hyrax or Haas
type expander.
Records were collected pre expansion (DE:
4y 11m, ME: 8y 1m) and when each child was considered
ready for phase II comprehensive treatment (DE: 11yr 0m,
ME: 11yr 11m).
The CG comprised of casts of untreated
33
children at corresponding time points (5y 4m, 8y 4m, and
11y 7m respectively).
The software Geomagic® Control™ was
utilized to calculate palatal surface area and palatal
volume as comparative measures.
Results:
Both palatal
surface area and palatal volume increased across all
groups, but were only significantly different (p<.05) at
T1.
Conclusions:
There were no differences in palatal
vault dimensions at the start of phase II orthodontic
treatment whether RPE was completed in the deciduous
dentition (T0) or the mixed dentition (T1). Results also
suggest that if posterior crossbites are allowed to
persist from childhood, measurable effects on the palate
may be present by the mixed dentition stage (T1).
Lastly, RPE is a reliable and stable method for
correction of posterior crossbites whether completed in
the deciduous (T0) or mixed (T1) dentition.
34
INTRODUCTION
Transverse maxillary deficiency is a common problem
found in orthodontic patients of all ages.
Currently, a
myriad of appliances and techniques are used to correct it,
with most employing some form of rapid palatal expansion
(RPE).
In fact, in modern orthodontics RPE has become a
standard of treatment for many practitioners in the United
States and throughout world.1
Yet, even with this
widespread use, controversy and disagreement seem to follow
RPE.
Even at its recorded inception in 1860,2 controversy
and skepticism hindered its acceptance as many prominent
figures in dentistry of that time dismissed and discredited
the fundamental notion of palatal separation.3,4
Today,
although palatal separation is now unquestionably accepted
as possible,5-7 many other questions regarding RPE remain
undecided and often controversial.8,9
Of these, perhaps the most pertinent to an orthodontic
clinician is this: when is the proper time to employ RPE so
as to maximize transverse gain and minimize possible
complications, patient discomfort, and relapse?
Much has
been written on this topic and a consensus reached with
regard to the mixed dentition:
that with proper diagnosis,
the earlier expansion can be completed the better.10
This
notion is based on anatomical11,12 and clinical10 studies
35
showing that as a child ages, the mid-palatal suture
increases its resistance to separation.
So if earlier is
better, why not use RPE in the deciduous dentition?
In
other words, could there be advantages to using RPE in the
deciduous dentition versus employing it in the mixed
dentition?
Historically, studies concerned with RPE in the
deciduous dentition have focused on the presence and
subsequent correction of posterior crossbites as the only
reliable, measurable and consistent variable available to
them.13-18
This is most likely due to the inherent
difficulty in comparing the deciduous to the
mixed/permanent dentition because, by the time a child is
ready for phase II treatment, all deciduous teeth that were
present have been replaced by an entirely new set of
permanent teeth.
The variations in both size and position
of these new permanent teeth make the linear tooth-to-tooth
measurements traditionally used as measures in studies of
transverse gain by RPE (i.e. inter-molar or inter-canine)
essentially meaningless.
Recently a group of authors published a series of
articles on the topic of RPE in the deciduous dentition.19-22
With the advent of digital technology, these studies used
the relatively new variables of palatal surface area and
36
palatal volume to quantify the effects of RPE in the
deciduous dentition of children with posterior crossbites
as compared to children without posterior crossbites.
These studies showed a significant gain in both palatal
surface area and palatal volume, as well as increased
palatal and facial symmetry with RPE use in the deciduous
dentition.22
While quite useful, these studies did not directly
compare RPE use in the deciduous dentition to that in the
mixed dentition.
In addition, these studies did not follow
these children beyond 30 months post expansion to the time
point when most orthodontic clinicians would want to see
the effects of their phase I RPE treatment—the start of
phase II treatment.
In fact, no studies to date have
utilized the measures of palatal surface area and palatal
volume to see if significant differences in palatal vault
dimensions can be seen at the start of phase II
comprehensive treatment whether RPE was completed in the
deciduous dentition or the mixed dentition.
This present
study seeks to shed light on this important topic.
37
MATERIALS AND METHODS
Sample Description
The sample consisted of 90 patients, each with two or
three different time points, for a total of 210 models.
Each model was received in a .stl file format and screened
for good palatal anatomy.
identified as Caucasian.
All patients in the sample were
Each of the 210 models was
divided into three groups: a deciduous expansion group, a
mixed expansion group and a control group.
The deciduous and mixed expansion groups contained
patients treated with RPE by a single clinician at two
distinct time points: in the deciduous expansion (T0) and
the mixed expansion (T1).
The deciduous expansion group
received RPE at a mean age of 4y 11m (±0y 6m) while the
mixed expansion group received RPE at a mean age of 8y 1m
(±0y 10m).
Both groups then had records taken at the time
when the treating orthodontist considered them ready for
the start of phase II comprehensive treatment (T2).
The
age at T2 for the deciduous expansion group was 11y 0m (±1y
4m), while the age for the mixed expansion group was 11y
11m (±1y 2m).
Each of these experimental groups consisted
of 30 subjects, accounting for 60 digital models each (See
table 3.1).
For a full breakdown of each group’s age see
38
table 3.2.
The presence/absence of a posterior crossbite
was also recorded (see table 3.3).
The control group also consisted of 30 subjects but,
unlike the experimental groups, each subject had models at
3 time points corresponding to the time points found in the
experimental groups of T0, T1, and T2 respectively.
mean ages were:
These
T0: 5y 4m (±0y 4m), T1: 8y4m (±0y 3m), and
T2: 11y 6m (±0y 3m). Gender was also matched.
All the
subjects in the control group were gathered from the
Michigan Growth Study with casts dated between the years
1936 to 1967.
None of these subjects received any
orthodontic treatment during the timeframe of data
collection, including RPE.
Consult tables 3.1, 3.2 and 3.3
for full demographics of each group.
Table 3.1: Sample Demographics, Gender and Age
Group
Total
Male/Female
Age
T0
Age
T1
Age
T2
Diff
T0-T2*
Diff
T0-T1¥
Diff
T1-T2£
Deciduous
Expansion
30
M=9
F=21
4y 11m
--
11y 0m
6y 1m
--
--
Mixed
Expansion
30
M=12
F=18
--
8y 1m
11y 11m
--
--
3y 10m
Control
30
M=20
F=10
5y 4m
8y 4m
11y 7m
6y 3m
3y 0m
3y 3m
* Age difference between T0 and T2
¥ Age difference between T0 and T1
£ Age difference between T1 and T2
39
Table 3.2: Age Break Down at each time point
Age T0
Age T1
Mean
Age
Median
Age
SD
4y 11m
5y 0m
ME¥
--
CG£
5y 4m
Group
DE*
Group
Mean
Age
Median
Age
SD
0y 6m
DE*
--
--
--
--
--
ME¥
8y 1m
8y 0m
0y 10m
5y 5m
0y 4m
CG£
8y 4m
8y 6m
0y 3m
Age T2
Group
Mean
Age
Median
Age
SD
DE*
11y 0m
11y 2m
1y 4m
ME¥
11y 11m
11y 8m
1y 2m
CG£
11y 7m
11y 7m
0y 3m
* Deciduous Expansion Group
¥ Mixed Expansion Group
£ Control Group
Table 3.3: Sample Demographics, Presence of Crossbite
Group
Deciduous
Expansion
Mixed
Expansion
Control
Total
#
30
30
30
Male/Female
M=9
F=21
M=12
F=18
M=20
F=10
X-bite
T0
%
X-bite
T1
%
Y=30
N=0
100
--
--
--
--
Y=3
N=27
10
40
Y=25
N=5
Y=3
N=27
83
10
X-bite
T2
Y=0
N=30
Y=0
N=30
Y=1
N=29
%
0
0
3
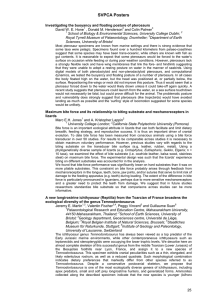
RPE Protocol in Experimental Groups
Protocol for expansion in the experimental groups
included the use of either a Hyrax or Haas type expander
using the deciduous 2nd molars as the anchor teeth (See
Figure 3.1).
Only one orthodontist diagnosed and treatment
planned all children in the experimental groups. The
majority of children diagnosed with a posterior crossbite
presented with unilateral posterior crossbite of all teeth
on the affected side while positioned in centric occlusion.
Figure 3.1: Examples of the appliances utilized in the deciduous
dentition: Hyrax (A) and Haas Type (B) and in the mixed
dentition: Hyrax (C) and Haas type (D). Photos provided by Dr.
Bernardo Souki (Belo Horizonte, Brazil).
41
On the same day as appliance delivery, each subject
received an activation of two turns, or an approximate
expansion of 0.4 mm.
Each subject was then instructed to
turn the screw twice each subsequent day until instructed
to cease.
The decision to cease expansion was made when
the palatal cusp of the maxillary deciduous 2nd molar or
permanent 1st molar (depending on what dentition RPE was
performed) was occluding on the most superior portion of
the lingual-buccal incline of the corresponding mandibular
tooth. On average, activation continued for 12 days and 13
days in the deciduous and mixed expansion groups
respectively.
The expander was then left in place
approximately four months for retention (See Table 3.4).
No other appliance, fixed or removable, was given to any of
the subjects until the start of phase II comprehensive
orthodontic treatment (T2).
Table 3.4: Expansion and Retention Protocol
Group
Appliance
type
Deciduous
Expansion
Mixed
Expansion
Hyrax=17
Haas=13
Hyrax=27
Haas=3
# of
turns
Total
expansion
(mm)
T0/T1-Act
time
difference*
Retention
(days)
26
5.2
100
119
28
5.6
116
130
*Time (days) between pre-expansion impression (T0 or T1) and actual
appliance delivery and activation
42
Measurements
The 3D inspection software Geomagic® Control™ (Rock
Hill, South Carolina, USA) was used to process each scan.
Any resultant palatal imperfections remaining from the
impression or scanning process were removed.
Figure 3.2
shows how scans appeared when ready for measurement.
Figure 3.2: Maxillary dental models as displayed in Geomagic®
Control™. Examples shown are the same subject at Time point T0
(A) and time point T2 (B).
Palatal Surface Area
Except where noted, protocol consistent with previous
studies19-22 for defining palatal surface area and palatal
volume consistent to both the deciduous and mixed dentition
were utilized.
In contrast to the previous studies where a
single point on the palatal gingival margin for each tooth
was used, in this present study, the contour of the palatal
gingival anatomy for each maxillary tooth was followed.
43
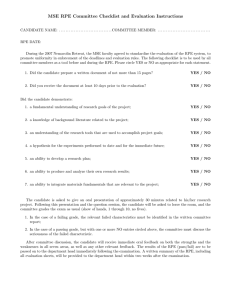
Distally, a plane was constructed by a straight line
connecting either the distal surfaces of the deciduous 2nd
molars for the deciduous dentition or mesial surfaces of
the permanent 1st molars for the mixed/permanent dentitions
(See figure 3.3).
Where a tooth had recently exfoliated and the
permanent successor had either not erupted or was in the
process of erupting, the area was defined as where the
contact point would be expected if the tooth were present.
The same protocol was used for severely rotated or block
out teeth.
Palatal surface area was reported in mm2.
Figure 3.3: Examples of palatal surface area as measured at T0
(A) and T2 (B). Notice the line connecting the distal surfaces of
the deciduous 2nd molars or permanent 1st molars depending on the
stage of dental development.
Palatal Volume
The same area used to define the palatal surface area
was used to measure the palatal volume.
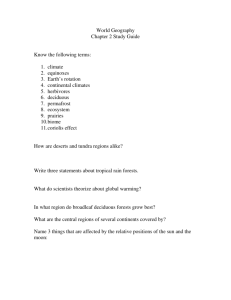
In addition, a
plane approximating the occlusal plane at the level of the
44
gingival margins was constructed.
This plane was found by
connecting three defined points. The anterior point was a
point that bisected the incisive papilla (See Figure 3.4).
Figure 3.4: The anterior point used to define the 3-point plane
for calculating palatal volume (A) is placed on the incisive
papilla so that the resulting plane (B) will bisect the papilla.
In contrast to the previous studies mentioned above
where the palatal gingival margins were used as references
for construcing this plane, the present study used the
incisive papilla as the anterior point.
This was done
because as a child transitions from the deciduous to mixed
dentition, the gingival anatomy palatal to the upper
incisors can vary significantly.
This variation is most
pronounced in the vertical deminsion, and in calculating
palatal volume, a small change in the vertical position of
this plane can have a large effect on the final volumetric
measurement.
The incisive papilla on the other hand, has
45
been shown to be stable, especially in the vertical
dimension, even after the loss of teeth.23,24
The two most distal points of the plane were defined
as the most palatal point on the gingival margin of the 2nd
deciduous molars, or in the case of the mixed or permanent
dentition, the most palatal point on the gingival margin of
the permanent 2nd premolars (see Figure 3.5).
Palatal
volume was reported in mm3.
Figure 3.5: To measure palatal volume, three points (A) were used
to make a plane (B)(C)(D) approximating the occlusal plane at the
height of the gingival margins.
46
ERROR OF METHODS
To test the reliability of these measurements, a
random number generator25 was utilized to select 10% of the
models for re-measurement.
Intraclass correlation was
estimated using Cronbach’s alpha.
Reliability is commonly
considered “adequate” when Cronbach’s alpha is equal to or
greater than 0.80.
For all variables, Cronbach’s alpha was
above this 0.80, with a range of 0.89-0.99.
STATISICAL ANALYSIS
SPSS® 23 software (IBM®, Armonk, New York, USA) was
used to calculate all descriptive and inferential
statistics.
The Shapiro-Wilk test was used to determine
the normality of each group.
To compare means, independent
t-tests were used where only two independent variables were
present (T0 and T1) and where three independent variables
were present, a one-way ANOVA was used (T2).
A
significance level of p<.05 was set.
RESULTS
Palatal Surface Area
An increase was seen in palatal surface area for all
groups from T0 to T2.
In the deciduous expansion group, a
47
mean increase from 851.8 mm2 (±75.4 mm2) to 1011.1 mm2
(±91.4 mm2) accounting for a 159.3 mm2 (±96.3 mm2) or 18.7%
increase in palatal surface area between time points T0-T2
was seen.
In the mixed expansion group, a mean increase
from 930.5 mm2 (±86.5 mm2) to 999.7 mm2 (±106.1 mm2)
accounting for a 69.2 mm2 (±63.7 mm2) or 7.4% increase
between time points T1 and T2 was also described.
In the control group, a mean increase from 890.4 mm2
(±83.1 mm2) to 980.6 mm2 (±77.3 mm2) accounting for 90.2 mm2
(±51.8 mm2) or 10.1% of increased surface area between T0
and T1 was seen.
Between time points T1 and T2, a mean
increase to 1017.5 mm2 (±92.5 mm2) and a mean increase of
37.0 mm2 (±50.1) or 4.2% was noted.
Overall, between time
points T0 and T2, a mean increase of 127.1 mm2 (±53.8 mm2)
or 14.3% was seen.
Between groups, T1 is the only time point that saw a
significant (α<.05) difference.
The mixed expansion group
and control group mean palatal surface areas were
statistically different (p=.021) at T1 and the subsequent
increase to T2 was also statistically different (p=.033).
See Table 3.5, 3.6, and 3.7 for complete results.
48
Table 3.5: Palatal Surface Area, means
Group
T0 (mm2)
SD (mm2)
T1 (mm2)
SD (mm2)
T2 (mm2)
SD (mm2)
851.8
75.4
--
--
1011.1
91.4
--
--
930.5*
86.5
999.7
106.1
890.4
83.1
980.6*
77.3
1017.5
92.5
Deciduous
Expansion
Mixed
Expansion
Control
*Statistically significant difference (p=.021)
Table 3.6: Palatal Surface Area, mm2 increase
Group
T1-T0
(mm2)
SD
T2-T1
(mm2)
SD
T2-T0
(mm2)
SD
Deciduous
Expansion
--
--
--
--
159.3
96.3
--
--
69.2*
63.7
--
--
90.2
51.8
37.0*
50.1
127.1
53.8
Mixed
Expansion
Control
*Statistically significant difference (p=.033)
Table 3.7: Palatal Surface Area, percent increase
Group
Deciduous
Expansion
Mixed
Expansion
Control
T1-T0 %
Increase
T2-T1 %
Increase
T2-T0 %
Increase
--
--
18.7%
--
7.4%
--
10.1%
4.2%
14.3%
Palatal Volume
An increase was also seen in all groups for palatal
volume.
In the deciduous expansion group, a mean increase
from 2821.7 mm3 (±427.6 mm3) to 3694.2 mm3 (±585.4 mm3)
accounting for an 872.5 mm3 (±519.1 mm3) or 30.9% increase
in palatal volume between time points T0-T2 was seen.
49
In
the mixed expansion group, a mean increase from 2920.5 mm3
(±522.8 mm3) to 3632.8 mm3 (±656.5 mm3) accounting for a
712.3 mm3 (SD: 477.0 mm3) or 24.4% increase between time
points T1 and T2 was seen as well.
In the control group, a mean increase from 2949.8 mm3
(±514.8 mm3) to 3311.2 mm3 (±443.1 mm3) accounting for 361.4
mm3 (±395.0 mm3) or 12.3% of increased palatal volume
between T0 and T1 was seen.
Between time points T1 and T2,
a mean increase to 3758.3 mm3 (±497.8 mm3) and a mean
increase of 447.1 mm3 (±348.4 mm3) or 15.2% was noted.
Overall, between time points T0 and T2, a mean increase of
808.5 mm3 (±495.9 mm3) or 27.4% was seen.
As with palatal surface area, T1 is the only time
point that had a significant (α<.05) difference between
groups.
The mixed expansion group and control group mean
palatal volumes at T1 were statistically different (p=.03)
and the subsequent increase to T2 was also statistically
different (p=.017).
See Table 3.8, 3.9, and 3.10 for
complete results.
50
Table 3.8: Palatal Volume, means
Group
T0 (mm3)
SD (mm3)
T1 (mm3)
SD (mm3)
T2 (mm3)
SD (mm3)
2821.7
427.6
--
--
3694.2
585.4
--
--
2920.5*
522.8
3632.8
656.5
2949.8
514.8
3311.2*
443.1
3758.3
497.8
Deciduous
Expansion
Mixed
Expansion
Control
*Statistically significant difference (p=.03)
Table 3.9: Palatal Volume, mm3 increase
Group
Deciduous
Expansion
Mixed
Expansion
Control
T1-T0
(mm3)
SD
T2-T1
(mm3)
SD
T2-T0
(mm3)
SD
--
--
--
--
872.5
519.1
--
--
712.3*
477.0
--
--
361.4
395
447.1*
348.4
808.5
495.9
*Statistically significant (p=.017)
Table 3.10: Palatal Volume, percent increase
Group
Deciduous
Expansion
Mixed
Expansion
Control
T0-T1 %
Increase
T1-T2 %
Increase
T2-T0 %
Increase
--
--
30.9%
--
24.4%
--
12.3%
15.2%
27.4%
DISCUSSION
Rapid palatal expansion in the deciduous dentition has
long been a topic of controversy.
Advocates are quick to
point to the possible adverse side effects of transverse
maxillary deficiency if allowed to persist from childhood.
51
The possible side effects of untreated transverse maxillary
deficiency include: posterior crossbite, dental trauma,
asymmetrical growth of the condyles and associated facial
structures, future facial asymmetries, possible adverse
temporomandibular joint effects, and disturbed masticatory
musculature activity.14,22,26-28
Others provide normalizing
growth as a reason for early correction.29
On the other hand, critics of RPE use in the deciduous
dentition question its utility based on reports of
spontaneous self-correction of posterior crossbites as a
child transitions from the deciduous to the permanent
dentition.14,30
In addition, these same critics argue the
likely need for two phases of treatment, the possibility of
inducing adverse facial effects such as paranasal swelling
and nasal humps,1 enamel decalcifications, possible
sensations of dizziness associated with early RPE, reports
of limited cooperation of young patients, and transient
opening of midline diastemas as reasons to avoid RPE in the
deciduous dentition.14
Yet what is missing in all of this is discussion on
whether measurable and significant differences in the
dentition and/or skeleton exist in adolescence whether RPE
is completed in the deciduous versus in the mixed/permanent
dentitions.
The literature is non-existent in its attempts
52
to quantify these possible skeletal and dental differences.
This scarcity is most likely due to the inherent difficulty
in comparing the deciduous to the mixed/permanent
dentitions.
In large part, this is because of the natural
changes that take place during transition in dentitions.
Because of this difficulty, studies have historically
focused on the presence and subsequent correction of
posterior crossbites as the only reliable, measurable and
consistent variable available to them.
Today though, with
the advent of digital technology, it is now possible to
utilize variables such as palatal surface area and palatal
volume.
Although relatively new, these measures have been
shown to be a reliable way to quantify changes to the
palate.29,31
This is especially true of palatal surface
area.20
The present comparative study utilized the software
Geomagic® Control™ to analyze 3-D digital scans of maxillary
dental models for both palatal surface area and palatal
volume in children who underwent RPE in the deciduous
dentition versus those who underwent RPE in the mixed
dentition.
These were compared to children who received no
orthodontic intervention of any kind at corresponding time
points.
It is important to remember that although the
groups were matched closely for race, gender, and age, the
53
majority of children treated with RPE in this study were
treated because of the presence of a posterior crossbite
(100% in the deciduous expansion group and 83% in the mixed
expansion group), whereas the majority of children in the
control group did not present initially with posterior
cross bites (10% at T0 and T1, 3% at T2).
This is not
surprising due to the fact that the presence of a posterior
crossbite is often associated with transverse maxillary
deficiency and is likely the reason RPE treatment is
prescribed, but this difference in groups does add some
unwanted variability to the groups.
A second control group
of orthodontically untreated children with posterior
crossbites would have been of great benefit to this study,
but was ultimately not necessary for the purpose of
answering the question this study sought to answer.
At T0 (~5 years) and T2 (~11-12 years) no statistical
differences in palatal surface area or palatal volume
between any of the groups was noted.
Yet at T1 (~8yr 6m)
there was a significant difference in both measures. The
mixed expansion group at T1 demonstrated significantly
lower values in both palatal surface area and palatal
volume when compared to the control group at T1.
This
finding suggests that in the deciduous dentition, the
effects of a posterior crossbite and/or transverse
54
maxillary deficiency may not yet be realized, but if left
uncorrected, the effects may begin to be seen by the mixed
dentition stage.
This cannot be commented on further due
to the lack of a second control group as mentioned
previously.
If a second control group of untreated
children showed this same trend of deficient values in both
palatal surface area and palatal volume continued into the
permanent dentition, this finding would be confirmed.
Regardless, based on this study’s results, it can be
concluded that whether a child receives RPE in the
deciduous dentition (T0) or RPE in the mixed dentition
(T1), the palatal vault anatomy will be nearly
indistinguishable when that child is ready for phase II
comprehensive treatment in early adolescence (T2).
In
addition, it can also be concluded that after RPE in the
deciduous dentition (T0) or mixed dentition (T1), a child’s
palatal vault will resemble that of a child with normal
occlusion (absence of a posterior crossbite and/or
transverse maxillary deficiency) who received no
orthodontic intervention.
These results are in partial agreement with the few
studies currently present in the literature utilizing
similar methods.
Recently, Primozic et al. published a
series of papers19-22,29 and, like this study, found no
55
statistically significant differences after RPE in either
palatal surface area or palatal volume between a control
group with no posterior crossbites and a treated
experimental group with posterior crossbites.
Yet, at
baseline (5yr 4m), a significant difference was noted in
palatal volume (not palatal surface area) between these
groups.
In contrast to what this present study found, this
suggests the effects caused by a posterior crossbite may
already be present in the deciduous dentition.
It has also been suggested by these authors that early
correction of a posterior crossbite in the deciduous
dentition results in improved facial symmetry of the lower
face.
This analysis was undertaken using methods similar
to this study’s, as well as the use of 3 dimensional facial
scans of the same children. It seems reasonably obvious, as
their study found, that correction of a posterior crossbite
might improve facial asymmetry, especially if associated
with a functional shift, yet what their study lacked was a
mixed dentition experimental group to compare with.
What remains unanswered then, and what merits further
investigation, is if early correction of a posterior
crossbite in the deciduous dentition results in greater
facial symmetry and less asymmetrical mandibular growth
than if correction is undertaken at a later age (i.e. in
56
the mixed/permanent dentitions).
This study cannot comment
on the impact early correction of maxillary deficiency
and/or associated posterior crossbites may have on the
entire facial skeleton and its growth.
In addition,
although it seems intuitive to assume that palatal surface
area and palatal volume may be strong indicators of true
skeletal change and correction, no studies to date have
shown this to be clinically true.
The results of this study do suggest a “normalization”
effect on palatal growth and morphology by RPE.
This
“normalization” is seen in the percent increase between the
control and experimental groups across all time points.
Although only T1-T2 tested statistically significant, the
percent difference was greater for those who received RPE
when compared to those who did not across all 3 groups and
across all 3 time points.
By virtue of this
“normalization” effect on growth with RPE, those children
diagnosed with transverse maxillary deficiency in the
deciduous dentition or mixed dentition had nearly
indistinguishable palatal measurements by early
adolescence.
In support of this “normalization” effect finding,
Primozic et al. reported in their studies that “an increase
in palatal volume of at least 13.5% at 18 months after
57
treatment is a good indicator to assess the reestablishment of normal growth in subjects treated for
maxillary constriction in the deciduous dentition.”29
Although the time points differ significantly in this
present study from these other studies (~3 years versus 18
months), a regular interval of increase in palatal volume
for untreated children with no posterior crossbite was seen
in the control group.
These increments included 12.3%
between T0-T1, and 15.2% between T1-T2.
Alternatively, the
change noted when RPE was completed in the mixed dentition
(24.4%) as compared to the control group (15.2%) was
statistically significant.
The lack of a second control
group with posterior crossbites limits the strength and use
of this finding though.
It should be noted that another study by Primozic et
al. was able utilize this second untreated control group
with posterior crossbites.
In that study it was shown that
while there were some significant differences in initial
presentation of palatal volume between those with posterior
crossbites and those without, this difference became much
greater at one year post RPE treatment.20
While the
weakness of this particular study is in the lack of
long-term follow-up, it does seem to reinforce the notion
of the “normalization” effect on growth described above by
58
demonstrating that if left untreated, a posterior crossbite
may hinder growth in the transverse dimension of the
maxilla.
This hindrance would only seem to worsen the
maxillary transverse deficiency most likely already
present.
More research is needed with longer follow-up
intervals and proper controls to show if this finding is
only transient or permanent.
Lastly, it should be pointed out that the decision to
use RPE in the deciduous dentition is likely not for
correction of transverse maxillary deficiency alone, but
more realistically, it is based on the presence of a
posterior crossbite.
In this study, RPE in the deciduous
dentition (T0) proved to be an extremely effective
treatment for correction of posterior crossbites, with 100%
of children remaining without crossbites at the start of
phase II comprehensive treatment (T2).
This high rate of
retentive posterior crossbite correction by RPE is in
agreement with some,32 while being higher than others.13,17,18
These differences may partially be explained by the wide
array of treatment modalities utilized in these studies:
including selective grinding of deciduous teeth, removable
expansion plates or fixed expansion appliances not
utilizing an expansion screw (i.e. quad helix or w-arch).
59
The lack of long-term follow up and varying definitions of
posterior crossbites may also explain some differences.
Lindner et al.13 directly compared expansion (by means
of a quad helix appliance) to selective grinding in the
deciduous dentition and found that although all subjects
treated with expansion were corrected initially, nearly 40%
relapsed prior to age 12.18
Even when compared to studies
that used a similar appliance as this present study, the
rate of relapse was still higher (26.7% vs 0%).22
The
reason for this could be many, including clinician case
selection and diagnostic criteria for posterior crossbite,
but this present study’s results confirm what many have
found:
that RPE in the deciduous dentition is generally as
reliable, if not more reliable, than other methods of
posterior crossbite correction.
The relevance and strength of this study resides in
the direct comparison between expansion in the deciduous
and mixed dentition, as well as in the time points selected
and their pertinence to an orthodontic clinician.
no such study has been conducted.
To date,
Previous studies on RPE
in the deciduous dentition have focused on describing
changes at time points anywhere between six months to three
years post RPE treatment; with few going beyond that.
While helpful in describing what changes to expect or
60
anticipate, these time points have little relevance to
everyday clinical orthodontics.
This study was able to
directly compare effects for both RPE in the deciduous
dentition (T0) and RPE in the mixed dentition (T1) at a
time when most orthodontic clinicians should be interested
in seeing the fruits of phase I RPE treatment:
at the
start of comprehensive phase II orthodontic treatment (T2).
CONCLUSIONS
1. Whether rapid palatal expansion is completed in the
deciduous (T0) or in the mixed dentition (T1), the
palatal vault dimensions are nearly indistinguishable at
the start of phase II orthodontic treatment (T2) and will
be similar to those of children with no history of
transverse orthodontic correction or transverse maxillary
deficiency.
2. Results suggest that if posterior crossbites are allowed
to persist from childhood, measurable effects on palatal
vault dimensions may be present by the mixed dentition
stage (T1).
3. Rapid palatal expansion is a reliable and stable
treatment modality, whether completed in the deciduous or
mixed dentition, when seeking to correct posterior
crossbites prior to the start of phase II treatment.
61
REFERENCES
1.
Profitt WR. Contemporary Orthodontics. 5 ed. St.
Louis, Missouri: Mosby; 2013.
2.
Angell E. Treatment of irregularity of the permanent
or adult teeth. Dental Cosmos. 1860;1:540-4, 99-600.
3.
Timms DJ. The dawn of rapid maxillary expansion. Angle
Orthod. 1999;69(3):247-50.
4.
Haas AJ. The treatment of maxillary deficiency by
opening the midpalatal suture. Angle Orthod.
1965;35:200-17.
5.
Haas AJ. Rapid expansion of the maxillary dental arch
and nasal cavity by opening the midpalatal suture.
Angle Orthod. 1961;31(2):73-90.
6.
Wertz RA. Skeletal and dental changes accompanying
rapid midpalatal suture opening. Am J Orthod.
1970;58(1):41-66.
7.
Cleall JF, Bayne DI, Posen JM, Subtelny JD. Expansion
of the midpalalal suture in the monkey. Angle Orthod.
1965;35:23-35.
8.
Schiffman PH, Tuncay OC. Maxillary expansion: a meta
analysis. Clin Orthod Res. 2001;4(2):86-96.
9.
Gianelly AA. Rapid palatal expansion in the absence of
crossbites: added value? Am J Orthod Dentofacial
Orthop. 2003;124(4):362-5.
10.
Baccetti T, Franchi L, Cameron CG, McNamara JA, Jr.
Treatment timing for rapid maxillary expansion. Angle
Orthod. 2001;71(5):343-50.
62
11.
Melsen B. Palatal growth studied on human autopsy
material. A histologic microradiographic study. Am J
Orthod. 1975;68(1):42-54.
12.
Melsen B, Melsen F. The postnatal development of the
palatomaxillary region studied on human autopsy
material. Am J Orthod. 1982;82(4):329-42.
13.
Lindner A. Longitudinal study on the effect of early
interceptive treatment in 4-year-old children with
unilateral cross-bite. Scand J Dent Res.
1989;97(5):432-8.
14.
Malandris M, Mahoney EK. Aetiology, diagnosis and
treatment of posterior cross-bites in the primary
dentition. Int J Paediatr Dent. 2004;14(3):155-66.
15.
Ninou S, Stephens C. The early treatment of posterior
crossbites: a review of continuing controversies. Dent
Update. 1994;21(10):420-6.
16.
Petren S, Bondemark L, Soderfeldt B. A systematic
review concerning early orthodontic treatment of
unilateral posterior crossbite. Angle Orthod.
2003;73(5):588-96.
17.
Thilander B, Wahlund S, Lennartsson B. The effect of
early interceptive treatment in children with
posterior cross-bite. Eur J Orthod. 1984;6(1):25-34.
18.
Tsarapatsani P, Tullberg M, Lindner A, Huggare J.
Long-term follow-up of early treatment of unilateral
forced posterior cross-bite. Orofacial status. Acta
Odontol Scand. 1999;57(2):97-104.
19.
Primozic J, Ovsenik M, Richmond S, Kau CH, Zhurov A.
Early crossbite correction: a three-dimensional
evaluation. Eur J Orthod. 2009;31(4):352-6.
63
20.
Primozic J, Perinetti G, Richmond S, Ovsenik M. Threedimensional longitudinal evaluation of palatal vault
changes in growing subjects. Angle Orthod.
2012;82(4):632-6.
21.
Primozic J, Baccetti T, Franchi L, Richmond S, Farcnik
F, Ovsenik M. Three-dimensional assessment of palatal
change in a controlled study of unilateral posterior
crossbite correction in the primary dentition. Eur J
Orthod. 2013;35(2):199-204.
22.
Primozic J, Richmond S, Kau CH, Zhurov A, Ovsenik M.
Three-dimensional evaluation of early crossbite
correction: a longitudinal study. Eur J Orthod.
2013;35(1):7-13.
23.
Harper RN. The incisive papilla: the basis of a
technic to reproduce the positions of key teeth in
prosthodontia. J of Dent Res. 1948;27(6):661-8.
24.
Solomon EGR, Arunachalam KS. The incisive papilla: A
significant landmark in prosthodontics. J Indian
Prosthodont Soc. 2012;12(4):236-47.
25.
Haahr M. True Random Number Service www.random.org:
Randomness and Integrity Services Ltd.; 1998 [cited
2015 9/4/2015].
26.
Egermark-Eriksson I, Carlsson GE, Magnusson T,
Thilander B. A longitudinal study on malocclusion in
relation to signs and symptoms of cranio-mandibular
disorders in children and adolescents. Eur J Orthod.
1990;12(4):399-407.
27.
Troelstrup B, Moller E. Electromyography of the
temporalis and masseter muscles in children with
unilateral cross-bite. Scand J Dent Res.
1970;78(5):425-30.
64
28.
Ingervall B, Thilander B. Activity of temporal and
masseter muscles in children with a lateral forced
bite. Angle Orthod. 1975;45(4):249-58.
29.
Primozic J, Perinetti G, Contardo L, Ovsenik M.
Diagnostic performance of 3-dimensional evaluation of
palatal vault changes in assessing successful
treatment of constricted maxilla in growing subjects.
Am J Orthod Dentofacial Orthop. 2013;143(1):42-9.
30.
Kurol J, Berglund L. Longitudinal study and costbenefit analysis of the effect of early treatment of
posterior cross-bites in the primary dentition. Eur J
Orthod. 1992;14(3):173-9.
31.
Gracco A, Malaguti A, Lombardo L, Mazzoli A, Raffaeli
R. Palatal volume following rapid maxillary expansion
in mixed dentition. Angle Orthod. 2010;80(1):153-9.
32.
Kutin G, Hawes RR. Posterior cross-bites in the
deciduous and mixed dentitions. Am J Orthod.
1969;56(5):491-504.
65
VITA AUCTORIS
Andrew Warren Foster was born on January 31, 1985 in
Columbia, Missouri to Michael and Margaret Foster. He is
the seventh of eight children.
When he was 4, Andrew moved from Missouri to
Littleton, Colorado where he eventually graduated from
Chatfield Senior High School in 2003. After graduation, he
attended Brigham Young University in Provo, Utah on a track
scholarship. After his freshman year, he served a two year
mission to West Africa (Ghana and Sierra Leone) for The
Church of Jesus Christ of Latter Day Saints.
Upon his return, he completed his studies at BYU and
matriculated at The University of Colorado School of Dental
Medicine where he graduated in May of 2013 with a D.D.S.
degree. He anticipates receiving a Master of Science in
dentistry along with a specialty certificate in
orthodontics from Saint Louis University in December 2015.
He will be moving to Grand Junction, Colorado to begin his
career in orthodontics.
Andrew met his future wife Kristen in kindergarten.
They were married in December of 2006 and are the parents
of four daughters: Melanie, Abigail, Lacey, and Blakely.
66