Spinal Cord Injury Facts and Figures at a Glance
advertisement

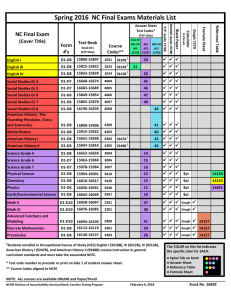
Spinal Cord Injury Facts and Figures at a Glance www.uab.edu/nscisc February 2013 This is a publication of the National Spinal Cord Injury Statistical Center, Birmingham, Alabama. Incidence: It is estimated that the annual incidence of spinal cord injury (SCI), not including those who die at the scene of the accident, is approximately 40 cases per million population in the U. S. or approximately 12,000 new cases each year. Since there have not been any incidence studies of SCI in the U.S. since the 1990's it is not known if incidence has changed in recent years. Prevalence: The number of people in the United States who are alive in 2013 who have SCI has been estimated to be approximately 273,000 persons, with a range of 238,000 to 332,000 persons. Note: Incidence and prevalence statistics are estimates obtained from several studies. These statistics are not derived from the National SCI Database. SCI is falls, followed by acts of violence (primarily gunshot wounds). The proportion of injuries that are due to sports has decreased over time while the proportion of injuries due to falls has increased. Violence caused 13.3% of spinal cord injuries prior to 1980, and peaked between 1990 and 1999 at 24.8% before declining to only 14.3% since 2010. CAUSES OF SCI SINCE 2010 The National Spinal Cord Injury Database has been in existence since 1973 and captures data from an estimated 13% of new SCI cases in the U.S. Since its inception, 28 federally funded SCI Model Systems have contributed data to the National SCI Database. As of December 2012, the database contained information on 29,096 persons who sustained traumatic spinal cord injuries. All the remaining statistics on this sheet are derived from this database or from collaborative studies conducted by the model systems. Detailed discussions of all topics on this sheet may be found in special issues of the journal Archives of Physical Medicine and Rehabilitation published in November 1999, November 2004, and March 2011. Age at injury: SCI primarily affects young adults. Nearly half of all injuries occurred between the ages of 16 and 30. From 1973 to 1979, the average age at injury was 28.7 years. As the median age of the general population of the United States has increased by approximately 9 years since the mid-1970, the average age at injury has also steadily increased over time. Since 2010, the average age at injury is 42.6 years. Other possible reasons for the observed trend toward older age at injury might include changes in either referral patterns to model systems, the locations of model systems, survival rates of older persons at the scene of the accident, or age-specific incidence rates. Gender: Overall, 80.7% of spinal cord injuries reported to the national database have occurred among males. Over the history of the database, there has been a slight trend toward a decreasing percentage of males. Prior to 1980, 81.8% of new spinal cord injuries occurred among males. Race/Ethnicity: A significant trend over time has been observed in the racial/ethnic distribution of persons in the database. Among persons injured between 1973 and 1979, 76.8% were Caucasian, 14.2% were African American, 1.9% were Native American and 0.9% were Asian. However, among those injured since 2010, 67.0% are Caucasian, 24.4% are African American, 0.8% are Native American and 2.1% are Asian. Hispanic origin increased from 5.9% in 1970’s to 12.5% in 2000-2004 and 7.9% since 2010. This trend is due in part to trends in the United States general population and also possibly explained by the changing locations of model systems, referral patterns to model systems, or race-specific incidence rates. Etiology: Since 2010, motor vehicle crashes account for 36.5% of reported SCI cases. The next most common cause of Neurologic level and extent of lesion: Persons with tetraplegia have sustained injuries to one of the eight cervical segments of the spinal cord; those with paraplegia have lesions in the thoracic, lumbar, or sacral regions of the spinal cord. Since 2010, the most frequent neurologic category at discharge of persons reported to the database is incomplete tetraplegia (40.6%), followed by incomplete paraplegia (18.7%), complete paraplegia (18.0%) and complete tetraplegia (11.6%). Less than 1% of persons experienced complete neurologic recovery by hospital discharge. Over the last 20 years, the percentage of persons with incomplete tetraplegia has increased while complete paraplegia and complete tetraplegia have decreased. Occupational status: More than half (57.1%) of those persons with SCI admitted to a model system reported being employed at the time of their injury. At one year after injury, 11.8% of persons with SCI are employed. By 20 years postinjury, 34.9% are employed and a similar level of employment is observed through post-injury year 35. Residence: Overall, 87.1% of all persons with SCI who are discharged from the system are sent to a private, noninstitutional residence (in most cases their homes before injury). Only 6.5% are discharged to nursing homes. The remaining are discharged to hospitals, group living situations or other destinations. Marital status: Considering the youthful age of most persons with SCI, it is not surprising that most (51.6%) are single when injured. Among those who were married at the time of injury, as well as those who marry after injury, the likelihood of their marriage remaining intact is slightly lower when compared to the general population. The likelihood of getting married after injury is also reduced. Length of stay: Overall, median days hospitalized in the acute care medical/surgical unit for those who enter a model system immediately following injury has declined from 24 days between 1973 and 1979 to 11 days since 2010. Substantial downward trends are noted for days in the rehab unit (from 98 to 36 days). Overall, median days hospitalized (during acute care and rehab) were greater for persons with neurologically complete injuries. Lifetime costs: The average yearly health care and living expenses and the estimated lifetime costs that are directly attributable to SCI vary greatly according to severity of injury. These figures do not include any indirect costs such as losses in wages, fringe benefits and productivity which average $70,575 per year in February 2013 dollars, but vary substantially based on education, severity of injury and pre-injury employment history. Average Yearly Expenses (in February 2013dollars) Severity of Injury Estimated Lifetime Costs by Age At Injury (discounted at 2%) First Year Each Subsequent Year 25 years old 50 years old High Tetraplegia (C1-C4) AIS ABC $1,044,197 $181,328 $4,633,137 $2,546,294 Low Tetraplegia (C5-C8) AIS ABC $754,524 $111,237 $3,385,259 $2,082,237 Paraplegia AIS ABC $508,904 $67,415 $2,265,584 $1,486,835 Incomplete Motor Functional at Any Level AIS D $340,787 $41,393 $1,547,858 $1,092,521 Data Source: Economic Impact of SCI published in the journal Topics in Spinal Cord Injury Rehabilitation Volume 16 Number 4 in 2011. Life expectancy is the average remaining years of life for an individual. Life expectancies for persons with SCI are still significantly below life expectancies for those with no SCI and have not improved since the 1980’s. Mortality rates are significantly higher during the first year after injury than during subsequent years, particularly for severely injured persons. Age at Injury 20 No SCI 59.0 Life expectancy (years) for post-injury by severity of injury and age at injury For persons who survive the first 24 hours For persons surviving at least 1 year post-injury AIS D - Motor Low High Ventilator AIS D - Motor Low High Ventilator Functional at Tetra Tetra Dependent- Functional at Tetra Tetra DependentAny Level Para (C5-C8) (C1-C4) Any Level Any Level Para (C5-C8) (C1-C4) Any Level 52.0 44.6 39.6 35.3 18.6 52.4 45.1 40.4 36.6 24.9 40 40.0 33.7 27.2 23.1 19.7 8.4 34.0 27.7 23.7 20.7 12.3 60 22.7 17.5 12.7 9.9 7.8 2.0 17.7 13.0 10.3 8.4 3.7 Cause of death: In years past, the leading cause of death among persons with SCI was renal failure. Today, however, significant advances in urologic management have resulted in dramatic shifts in the leading causes of death. Persons enrolled in the National SCI Database since its inception in 1973 have now been followed for 40 years after injury. During that time, the causes of death that appear to have the greatest impact on reduced life expectancy for this population are pneumonia and septicemia. Find additional information in the Annual Report on the NSCISC website: https://www.nscisc.uab.edu/reports.aspx Presently, there are 14 systems and 5 Form II centers sponsored by the National Institute on Disability and Rehabilitation Research, Office of Special Education and Rehabilitative Services, U.S. Department of Education SCI MODEL SYSTEM CENTERS FORM II CENTERS Collect follow-up data only Santa Clara Valley Medical Center Univ of AL-B’ham Spain Rehab SCIMS New England Regional SCI Center San Jose, CA (408) 885-2383 Birmingham, AL (205) 934-3283 Boston, MA (617) 638-7380 So California SCIMS at Rancho Los Amigos Downey, CA (562) 401-8111 Spaulding-Harvard SCI System Boston, MA (617) 573-2754 Mount Sinai School of Medicine New York, NY (212) 659-9340 Rocky Mountain Regional SCI System Englewood, CO (303) 789-8306 Univ of Michigan SCI Model System Ann Arbor, MI (734) 763-0971 Institute for Rehabilitation and Research Houston, TX (713) 797-5972 South Florida SCIMS Miami, FL (305) 243-9516 Northern New Jersey SCI System West Orange, NJ (973) 243-6973 Univ of Missouri Columbia, MO (collected by UAB (205) 934-3283) Southeastern Regional SCIMS at Shepherd Atlanta, GA (404) 352-2020 Regional SCI Center of the Delaware Valley Philadelphia, PA (215) 955-6579 Woodrow Wilson Rehab Center Fishersville, VA (collected by UAB (205) 934-3283) Midwest Regional SCI Care System Chicago, IL (312) 238-6207 U of Pittsburgh Model System on SCI Pittsburgh, PA (412) 232-7949 Kentucky Regional Model SCI System Louisville KY (502) 582-7443 Northwest Regional SCI System Seattle, WA (800) 366-5643 This is a publication of the National Spinal Cord Injury Statistical Center, Birmingham, Alabama, which is funded by the National Institute on Disability and Rehabilitation Research (grant #H133A110002), Office of Special Education and Rehabilitative Services, U.S. Department of Education, Washington, DC. The opinions contained in this publication are those of the grantee and do not necessarily reflect those of the U.S. Department of Education. ©2012, Board of Trustees, University of Alabama Suggested Citation: National Spinal Cord Injury Statistical Center, Facts and Figures At a Glance. Birmingham, AL: University of Alabama at Birmingham, March 2013. The National SCI Statistical Center 1717 6th Avenue South, SRC 515, Birmingham, AL 35233-7330 For Statistics: (205) 934-3342; For Business: (205) 934-3320; TDD: (205) 934-4642; FAX: (205) 934-2709; E-mail: NSCISC@uab.edu