Diagnosis And Management Of
Urinary Tract Infections In The
Emergency Department
Urinary tract infections are a heterogeneous group of disorders,
involving infection of all or part of the urinary tract, and are defined by bacteria in the urine with clinical symptoms that may
be acute or chronic. Approximately 1 million urinary tract infections are treated every year in United States emergency departments. The female-to-male ratio is 6:1. Urinary tract infections
are categorized as upper versus lower tract involvement and
as uncomplicated versus complicated. The emergency clinician
must carefully categorize the infection and take into account
patient host factors to optimally treat and disposition patients.
A working knowledge of local or at least national susceptibility patterns of the most likely pathogens is essential. A variety
of special populations exist that require special management,
including pregnant females, patients with anatomic abnormalities, and instrumented patients.
Andy Jagoda, MD, FACEP
Professor and Chair, Department of
Emergency Medicine, Icahn School
of Medicine at Mount Sinai, Medical
Director, Mount Sinai Hospital, New
York, NY
Associate Editor-In-Chief
Kaushal Shah, MD, FACEP
Associate Professor, Department of
Emergency Medicine, Icahn School
of Medicine at Mount Sinai, New
York, NY
Editorial Board
William J. Brady, MD
Professor of Emergency Medicine
and Medicine, Chair, Medical
Emergency Response Committee,
Medical Director, Emergency
Management, University of Virginia
Medical Center, Charlottesville, VA
Mark Clark, MD
Assistant Professor of Emergency
Medicine, Program Director,
Emergency Medicine Residency,
Mount Sinai Saint Luke's, Mount
Sinai Roosevelt, New York, NY
Peter DeBlieux, MD Professor of Clinical Medicine,
Interim Public Hospital Director
of Emergency Medicine Services,
Louisiana State University Health
Science Center, New Orleans, LA
Nicholas Genes, MD, PhD
Assistant Professor, Department of
Emergency Medicine, Icahn School
of Medicine at Mount Sinai, New
York, NY
Authors
Jessica Best, MD
Department of Emergency Medicine, University of Texas
Southwestern at Austin, Austin, TX
Derek Ou, MD
Department of Emergency Medicine, University Medical Center
Brackenridge, Austin, TX
Abstract
Editor-In-Chief
July 2014
Volume 16, Number 7
Michael A. Gibbs, MD, FACEP
Professor and Chair, Department
of Emergency Medicine, Carolinas
Medical Center, University of North
Carolina School of Medicine, Chapel
Hill, NC
Steven A. Godwin, MD, FACEP
Professor and Chair, Department
of Emergency Medicine, Assistant
Dean, Simulation Education,
University of Florida COMJacksonville, Jacksonville, FL
Gregory L. Henry, MD, FACEP
Clinical Professor, Department of
Emergency Medicine, University
of Michigan Medical School; CEO,
Medical Practice Risk Assessment,
Inc., Ann Arbor, MI
John M. Howell, MD, FACEP
Clinical Professor of Emergency
Medicine, George Washington
University, Washington, DC; Director
of Academic Affairs, Best Practices,
Inc, Inova Fairfax Hospital, Falls
Church, VA
Andrew David Kitlowski, MD
Assistant Professor of Emergency Medicine, University of Texas
Southwestern at Austin, Austin, TX
John Bedolla, MD
Assistant Director of Research Education, University of Texas
Southwestern at Austin, Austin, TX
Peer Reviewers
Lauren Grossman, MD, SM
Attending Physician, First Choice ER, Arvada, CO
Nicole Lazarciuc, MD, MPH
Assistant Clinical Professor, Icahn School of Medicine at Mount
Sinai, New York, NY
Prior to beginning this activity, see “Physician CME Information”
on the back page.
Charles V. Pollack, Jr., MA, MD,
Scott Silvers, MD, FACEP
Chair, Department of Emergency
FACEP
Medicine, Mayo Clinic, Jacksonville, FL
Professor and Chair, Department of
Emergency Medicine, Pennsylvania
Corey
M. Slovis, MD, FACP, FACEP
Hospital, Perelman School of
Professor and Chair, Department
Medicine, University of Pennsylvania,
of Emergency Medicine, Vanderbilt
Philadelphia, PA
University Medical Center, Nashville,
Michael S. Radeos, MD, MPH
TN
Assistant Professor of Emergency
Stephen H. Thomas, MD, MPH
Medicine, Weill Medical College
George Kaiser Family Foundation
of Cornell University, New York;
Professor & Chair, Department of
Research Director, Department of
Emergency Medicine, University of
Emergency Medicine, New York
Oklahoma School of Community
Hospital Queens, Flushing, NY
Medicine, Tulsa, OK
Ali S. Raja, MD, MBA, MPH
Ron M. Walls, MD
Director of Network Operations and
Professor and Chair, Department of
Business Development, Department
Emergency Medicine, Brigham and
of Emergency Medicine, Brigham
Women’s Hospital, Harvard Medical
and Women’s Hospital; Assistant
School, Boston, MA
Professor, Harvard Medical School,
Boston, MA
Scott D. Weingart, MD, FCCM
Associate Professor of Emergency
Robert L. Rogers, MD, FACEP,
Medicine, Director, Division of
FAAEM, FACP
ED Critical Care, Icahn School of
Assistant Professor of Emergency
Medicine at Mount Sinai, New Medicine, The University of
York, NY
Maryland School of Medicine,
Baltimore, MD
Shkelzen Hoxhaj, MD, MPH, MBA
Chief of Emergency Medicine, Baylor
College of Medicine, Houston, TX
Alfred Sacchetti, MD, FACEP
Assistant Clinical Professor,
Eric Legome, MD
Department of Emergency Medicine,
Chief of Emergency Medicine,
Thomas Jefferson University,
King’s County Hospital; Professor of
Philadelphia, PA
Clinical Emergency Medicine, SUNY
Downstate College of Medicine,
Robert Schiller, MD
Brooklyn, NY
Chair, Department of Family
Medicine, Beth Israel Medical
Keith A. Marill, MD
Center; Senior Faculty, Family
Research Faculty, Depatment of
Medicine and Community Health,
Emergency Medicine, University of
Icahn School of Medicine at Mount
Pittsburgh Medical Center, Pittsburgh,
Sinai, New York, NY
PA
Senior Research Editors
James Damilini, PharmD, BCPS
Clinical Pharmacist, Emergency
Room, St. Joseph’s Hospital and
Medical Center, Phoenix, AZ
Research Editor
Michael Guthrie, MD
Emergency Medicine Residency,
Icahn School of Medicine at Mount
Sinai, New York, NY
International Editors
Peter Cameron, MD
Academic Director, The Alfred
Emergency and Trauma Centre,
Monash University, Melbourne,
Australia
Giorgio Carbone, MD
Chief, Department of Emergency
Medicine Ospedale Gradenigo,
Torino, Italy
Amin Antoine Kazzi, MD, FAAEM
Associate Professor and Vice Chair,
Department of Emergency Medicine,
University of California, Irvine;
American University, Beirut, Lebanon
Hugo Peralta, MD
Chair of Emergency Services,
Hospital Italiano, Buenos Aires,
Argentina
Dhanadol Rojanasarntikul, MD
Attending Physician, Emergency
Medicine, King Chulalongkorn
Memorial Hospital, Thai Red Cross,
Thailand; Faculty of Medicine,
Chulalongkorn University, Thailand
Suzanne Y.G. Peeters, MD
Joseph D. Toscano, MD
Emergency Medicine Residency
Chairman, Department of Emergency
Director, Haga Teaching Hospital,
Medicine, San Ramon Regional
The Hague, The Netherlands
Medical Center, San Ramon, CA
tract and those of the upper tract. Lower tract infection is confined primarily to the urinary bladder
and is termed cystitis. Infection of the upper urinary tract is termed pyelonephritis, and it involves
the kidneys and ureter. Pyelonephritis is characteristically more severe than cystitis, and patients with
pyelonephritis frequently have systemic symptoms
and appear more ill.
UTIs are also classified as uncomplicated versus
complicated. This classification is not specifically
anatomic or physiologic, but more generally attempts to discern which patients are most likely to
recover uneventfully with therapy (uncomplicated)
versus patients who are at an increased risk of treatment failure (complicated). Patient comorbidities
are the primary determinants of whether a UTI is
complicated versus uncomplicated.1
The frequency and relatively benign course of
most UTIs may lull the emergency clinician into
the false sense that these are easy cases. While most
UTIs are straightforward to diagnose, patient comorbidities, local bacterial susceptibility patterns, and
available antibiotic choices and costs must be taken
into account to assure an optimal outcome.
This issue of Emergency Medicine Practice takes
an evidence-based approach to answering the key
questions for the patient with a possible UTI:
• Is this an uncomplicated or a complicated UTI?
• What is the appropriate antibiotic to use?
• Is the patient a normal host?
• Is there an anatomic or functional abnormality?
• Is this a mimic? Could this be an abdominal
aortic aneurysm or another life-threatening
condition?
• Is this patient best treated as an inpatient or
outpatient?
• Could the patient be septic?
Case Presentations
It is a typical day in the ED: you finish taking sign out
from your partner, sign on to the computer, and see the
broad spectrum of complaints awaiting you on the tracking board. The first patient seems like a quick disposition:
a 21-year-old woman with dysuria. She describes 3 days
of dysuria and urgency and has mild suprapubic pain.
But before you write her for antibiotics, you ask if she is
having any gynecologic symptoms . . .
In the next room, you meet a pleasant 38-year-old
woman, mother of 4 boys. She has had kidney stones in
the past and a tubal ligation. She complains of persistent
fever with a recent UTI, despite starting a second course
of antibiotics. She has never complained of back pain, and
currently she is afebrile. The patient looks well and her vitals are normal except for a slight tachycardia. While you
say, “Let me grab our ultrasound machine, and I will be
right back,” you wonder if this is just a case of antibiotic
resistance or something else . . .
You sigh as you read the chief complaint on the next
patient to be seen: a 45-year-old nursing home patient
with weakness. He is a bed-bound patient with a history
of a spinal cord injury, who has a Foley catheter. His
vitals reveal a fever of 38.3°C, a pulse of 130 beats/min,
and a blood pressure of 100/50 mm Hg. The nursing home
note says only that he has become increasingly weak. The
Foley is not well cared for; there is foul-smelling urine
that is cloudy, with sediment in the collection bag. You
begin your physical examination while having the nurse
contact the nursing home for some more history. . .
You pick up 1 more patient, a 23-year-old woman
with fever, left flank pain, and recent dysuria. She denies
any previous medical problems, and she has no other
complaints. Her examination is benign except for a fever
of 39.2°C, pulse 110 beats/min, and slight costovertebral
tenderness on the left. You start her IV, send the necessary labs, and walk back to your desk wondering if she is a
simple UTI or more . . . .
Less than an hour into your shift and the theme is set:
UTIs. You reflect on the broad spectrum of clinical presentations for UTIs and the accompanying challenges.
Critical Appraisal Of The Literature
A literature search was performed on PubMed and
MEDLINE® using the following terms: urinary tract
infection, combined with imaging, diagnosis, treatment,
emergency department management, epidemiology, and
incidence of urinary tract infections. To limit the results,
filters were set: journal articles, review articles, and
practice guidelines. Titles, abstracts, and full articles were reviewed for content. Within the practice guidelines, primary sources of literature were
reviewed. The Cochrane Database of Systematic
Reviews were also referenced. Important practice
guidelines reviewed include the Infectious Diseases
Society of America (IDSA) publication on uncomplicated cystitis and pyelonephritis. Findings from
6 randomized controlled trials, 6 laboratory studies,
27 prospective observational studies, 15 retrospective studies, 2 meta-analyses, 2 systematic reviews,
6 guidelines, 26 reviews, 3 textbook chapters, 2 case
Introduction
The diagnosis and management of urinary tract
infection (UTI) seems, at first, like an ordinary task;
however, effective management of the full spectrum of urinary tract conditions and their mimics presents a variety of challenges even for the
most seasoned emergency clinician. Urinary tract
symptoms are frequent presenting complaints, and
knowing how to manage them properly will lower
failures, bounce-backs, and complications. Knowing the atypical presentations and when to do a
more extensive workup will maximize outcomes
and minimize errors in management.
UTIs are divided into those involving the lower
Copyright © 2014 EB Medicine. All rights reserved.
2
www.ebmedicine.net • July 2014
trophy, hospitalization, sexual intercourse, and recurrent UTIs (defined as 3 or more UTIs within a year).
UTI-causing organisms migrate from enteric
flora to colonize the perineum and urethra. E coli
is the dominant pathogen, causing 75% to 90% of
uncomplicated acute infections in all UTI infections.
S saprophyticus is the second most common organism, comprising 5% to 15% of cases of uncomplicated
acute infections in young, sexually active females;
however, it is present in low numbers on normal
skin and in the perineal region. Less frequent but
significant pathogens for acute uncomplicated UTIs
include: Proteus, Streptococcus, Klebsiella, Enterobacter,
Pseudomonas, Enterococcus, Staphylococcus, Providencia,
Serratia, Morganella, Citrobacter, Salmonella, Shigella,
Haemophilus, Mycobacterium tuberculosis, and fungi.8,9
Uncomplicated UTIs are infections without
structural or functional abnormalities in the urinary
tract/kidney. Typically, uncomplicated infections
are dominated by E coli, in contrast to complicated
UTIs, which are more likely to be caused by Enterobacteriaceae, Pseudomonas, Acinetobacter, and S aureus.
Nosocomial UTIs are caused most commonly by S
epidermidis, S aureus, coagulase-negative Staphylococci, and Enterococcus faecalis.2,10
reports, and 2 editorials are included here. The total
number of patients enrolled in included prospective
and retrospective studies was 1,846,871.
The literature on UTI is extensive. No particular
specialty dominates the literature on UTI. The literature spans the disciplines of emergency medicine,
internal medicine, family practice, obstetrics and
gynecology, urology, and infectious disease. The
advantages of split ownership are volume and coverage: there is a large amount of literature, and most
scenarios have been addressed. The disadvantage of
split ownership is the lack of authoritative, multidisciplinary studies and consensus statements that
outline specific management options for clinicians.
Additionally, many of the studies of antibiotics compare in vitro susceptibilities between antibiotics but
do not compare clinical efficacy.
Future evidence-based clinical guidelines and
research for UTIs should include:
1. Authoritative multidisciplinary consensus statements on resistance patterns and recommended
empiric therapy.
2. Regional studies to establish the geography
of bacterial resistance patterns and changes in
resistance patterns.
3. Development and trials of new antibiotics.
4. More studies on the role of antibiotic stewardship programs.
Physiology Of Urination
Urine formation begins at the nephron, which consists of the renal tubule and glomerulus. The glomerulus, formed by the conglomeration of the renal
afferent and efferent arteriole, forms filtrate through
the receiving end of the renal tubule called the Bowman capsule. The filtrate is then concentrated in the
loop of Henle, and urine is formed in the collecting ducts where sodium and water are reabsorbed.
The formed urine then passes through the renal
cortex and empties into the renal pelvis. A series of
regular peristaltic contractions moves urine down
the ureters where it pools in the bladder. From an
anatomical standpoint, obstruction (either from an
extraureteral mass or intraureteral stone) can cause
urinary stasis and development of an infection.
Vesicoureteric reflux increases the risk of UTIs by
27% versus the 1% standard risk in males without
reflux. Vesicoureteric reflux is the result of abnormal
retrograde flow of urine into the ureters and kidneys from incompetent or misplaced valves, and it
increases the risk of recurrent UTIs, pyelonephritis,
and renal scarring.4
The act of urination is a complex series of neural
stimulation and feedback loops. The lower urinary
tract consists of parasympathetic, sympathetic, and
somatic nervous systems. Afferent stretch fibers of
the bladder wall sense increases in intravesicular
pressure and, once fully distended, will stimulate
the parasympathetic efferent nerve fibers. Parasympathetic axons then release acetylcholine, which
stimulates muscarinic bladder receptors leading
Anatomy And Pathophysiology
Bacteriology
The surface of the perineum is covered with normal
flora, predominantly Staphylococcus epidermidis, followed by its more virulent cousin, Staphylococcus aureus, and bacteria found in deeper structures, including Propionibacterium and Peptococcus species. Normally, urine remains sterile while in the bladder and
throughout the majority of the urinary tract. Once
urine passes through the urethra, it picks up organisms, including S epidermidis, nonhemolytic Streptococcus and Staphylococcus saprophyticus (found around
genitourinary tract skin), among others. Escherichia
coli, coliforms (E coli, Klebsiella, Enterobacter, Citrobacter, Serratia) and Enterococcus species are among the
most common UTI-causing organisms and are found
in high numbers on and around the perineum.2
A meta-analysis of the published data on the
effect of circumcision on the risk of UTIs in males
concluded that, although circumcision reduces the
risk of UTI, this net effect is more beneficial in those
with a high risk of developing a UTI, in particular,
males with recurrent UTI and those with vesicoureteric reflux.3 Skin conditions that promote increased
bacterial growth (such as immunosuppression and
diabetes) are associated with increased risk of UTI.
Other risk factors include pregnancy, neurogenic
bladder, indwelling Foley catheters, prostatic hyperJuly 2014 • www.ebmedicine.net
3
Reprints: www.ebmedicine.net/empissues
to bladder wall contractions through the detrusor
muscle. Sympathetic pathways are stimulated to
release norepinephrine-eliciting contractions of the
bladder base and urethral smooth muscle. Somatic
efferent neurons release acetylcholine and act on the
external striated urethral muscle (external urethral
sphincter) and pelvic floor muscles. During the act
of micturition, voluntary efforts relax the external
urethral sphincter and pelvic floor muscles, and
urine is relieved.5 Dysfunction in this process can
lead to urinary retention, decreased velocity of emptying, decreased bladder emptying, and consequent
development of a UTI. Common causes include
neurogenic bladder from a spinal cord injury or
peripheral neuropathy.
with normal flora from the skin, urethra, and vagina.
This is less of a problem with males, as it is easier to
sterilize the urethral meatus than it is with females.
Uncircumcised males are thought to have more
colonization of skin flora under the foreskin, but the
risk of a contaminated specimen is minimized when
the foreskin is retracted prior to obtaining a sample
and clean-catch guidelines are strictly adhered to.
Urine samples from females are frequently prone to
contamination from vaginal leukocytes and vaginal
secretions as well as normal flora.11
Sterile Pyuria
A urinalysis with white blood cells (WBCs) in the
absence of bacteria is referred to as sterile pyuria.
Sterile pyuria is a challenge to interpret and has a
wide differential of clinically significant pathologies. The differential diagnosis must be considered,
since some etiologies require specific additional
evaluation and treatment. For example, in a nonrandomized case series of 500 patients undergoing
surgery for acute appendicitis, one-third of these
subjects had urinary symptoms, including right
flank pain with dysuria with sterile pyuria, most
commonly in the group between 15 and 19 years
of age. The etiology is the presence of the inflamed
appendix lying on the ureter, causing irritation and
leukocytosis from the ureter.12 Any form of enteritis,
including diverticulitis, can also cause sterile pyuria
by causing external inflammation of the urinary
tract.11 Intrinsic renal pathologies causing this finding include perinephric abscess, renal tuberculosis,
renal papillary necrosis, renal sarcoidosis, polycystic
kidney disease, nephrolithiasis, nephropathy, transplant rejection, fungal infections, and nephritis.11
Certain infiltrative disorders (such as lymphoma or
leukemia) can involve the tubules and interstitium,
causing mild to moderate pyuria along with proteinuria and hematuria.
Physiology Of Bladder And Ureter Function
The ureters contain smooth, irregular muscles in a
helical arrangement and join the kidneys with the
bladder. These muscles are continuous with the
renal pelvis, and they undergo regular, peristaltic
contractions every 5 minutes, which helps transfer
urine to the bladder. The ureters are constricted in 3
different zones, which correspond with the common
areas of stone obstruction: (1) the renal pelvis, (2)
pelvic brim, and (3) ureterovesicular junction. The
ureters pass through the bladder posteroinferiorly
at an oblique angle, which helps to prevent urinal
reflux and opens up to the trigone of the bladder.6
The bladder is an extraperitoneal retropubic organ that serves as the reservoir for urine; under normal conditions, it can hold in excess of 750 mL, although the urge to urinate occurs around 300 to 450
mL. The apex of the bladder is dome-shaped, and
when it is distended, it extends superiorly toward
the pubic symphysis. The detrusor muscle contains
3 indistinguishable smooth muscle layers arranged
in circular and longitudinal orientation patterns that
are responsible for bladder wall contraction, once
stimulated. The neck is the inferior-most portion of
the bladder and marks the transition into origin of
the urethra.7 The bladder musculature is continuous
with the urethra and functions as the internal urethral sphincter.6 Infection-causing pathology in the
bladder includes urethral strictures, stones, bladder
cancer, or intravesicular blood clots.
Noninfectious Dysuria
On the other end of the spectrum, diagnosing dysuria without other signs or symptoms of UTI can be
a daunting task. In these cases, it is important to take
a thorough history and consider other variables in
your differential. In postmenopausal women, reduction in endogenous estrogen levels leads to atrophic
vaginitis, dryness, and vaginal inflammation that
causes dysuria and frequency.13 Other causes in
women include urethral trauma from intercourse
and irritation from commonly used scented soaps,
sprays, creams, or other hygiene products. In
men, consider that benign prostatic hypertrophy,
especially in men aged > 70 years, results in urethral obstruction which then leads to dysuria and
frequency.14 In both sexes, dysuria can also be the
result of urethral strictures from previous sexually
transmitted infections or prior urethral instrumenta-
Differential Diagnosis
Unclean Specimen
An accurate diagnosis of UTI requires having a good
urine sample. A “clean catch” urine specimen requires proper hand washing, sterilization of the urethra and glans penis (in males) or labia (in females)
with wipes, stopping the initial urine midstream,
and then catching the rest of the urine in the collecting cup until it is roughly half-full. When improperly performed, the urine can become contaminated
Copyright © 2014 EB Medicine. All rights reserved.
4
www.ebmedicine.net • July 2014
tion, neoplasms, renal calculi, or physical activities
like bicycling.2,5-11,15
the ED with a self-diagnosis of UTI. In a prospective
cohort study enrolling 50 patients, there was a poor
correlation between the emergency physician's clinical diagnosis and the patient's self-diagnosis.21
Prehospital Care
Lower Versus Upper Urinary Tract Infection
There have been studies of telemedicine protocols to
manage uncomplicated UTI. In a recent retrospective study of 273 women, approximately 50% were
successfully treated without urinalysis or culture or
visit to a healthcare facility.16 A recent case series of
499 women with uncomplicated UTI in Switzerland
showed 78% resolution after telemedicine consultation and treatment.17 To date, there have been no
studies of prehospital resources in the management of
UTI. That being said, prehospital personnel can provide valuable information to the emergency clinician
based on their history and physical examination, with
particular attention to septic patients with indwelling catheters, the immunocompromised, and the
elderly. In terms of indwelling catheters, emergency
medical services should focus on tubing and collecting systems; looking for buildup, sediment, or blood;
asking about decreased urine output; and noting the
color and any foul smelling odors from the bag. These
questions and findings can help guide the provider
towards a diagnosis and expedite patient care.18,19
Upper UTIs are often distinguished from lower
UTIs by the presence of systemic symptoms such
as fever, nausea, vomiting, chills, and back pain.20
However, in practice, there is often considerable
overlap between these entities. Understanding the
importance of a rectal temperature to diagnose fever
and a careful percussion of the costovertebral angle
is useful in diagnosing pyelonephritis. Fever is commonly present and, in a retrospective cohort study
of 304 patients from a single-center, patients without
fever were more likely to have other diagnoses, such
as pelvic inflammatory disease, diverticulitis, or
cholecystitis.22 Again, the emergency clinician must
be aware of the wide spectrum of clinical manifestations of pyelonephritis. Ask about recent antipyretics, the duration of illness, recent antibiotics, and
comorbidities. Patients can present with atypical
features, such as upper abdominal pain, no pain, or
headache. Because acute pyelonephritis is a clinical
diagnosis, consider that subclinical pyelonephritis
is seen more often in patients with recurrent UTIs,
prolonged symptoms ( > 7 days duration), male sex,
diabetes mellitus, pregnancy, immunosuppression,
and old age.23 Although this makes intuitive sense,
there is a paucity of evidence to support this.
Emergency Department Evaluation
Proper evaluation of emergency department (ED)
patients with suspected UTIs starts with a careful
history and physical examination. The evaluation is
directed at answering a number of key questions:
1. Is this patient’s symptom the result of a UTI, or
could there be an alternative diagnosis?
2. Does this patient have a lower or upper tract
UTI?
3. Is the patient possibly pregnant?
4. Has there been any exposure to sexually transmitted infections?
5. Is this an uncomplicated or complicated UTI?
6. What is the proper disposition?
Complicated Versus Uncomplicated Urinary
Tract Infection
Distinguishing between an uncomplicated and a
complicated UTI is important because it will influence management and patient disposition. An
uncomplicated UTI is acute cystitis or pyelonephritis
in a nontoxic, healthy, premenopausal, nonpregnant female with normal urogenital anatomy.24,25
(See Table 1, page 6.) All other patient subsets are
deemed to have complicated UTIs, such as the elderly,
males, patients with moderate to severe diabetes, the
immunocompromised, patients with kidney stones,
or patients who are pregnant. It should be routine
to screen every premenopausal woman with UTI
symptoms for pregnancy. In addition, all patients
should be asked about comorbidities or a history of
kidney stones, recent genitourinary procedures, or
recent antibiotic use in order to assess risk factors.
(See Table 2, page 6.)
The classic symptoms of acute cystitis are dysuria, frequency, urgency, and suprapubic discomfort. However, these symptoms are not specific to
UTIs and they overlap with other entities such as
sexually transmitted infections, vulvovaginitis, or
exposure to irritants such as allergens, chemicals, or
trauma. In a retrospective systematic review of the
literature looking at 9 of 464 studies published between 1966 and 2001, the combination of more than
2 of the classic symptoms of UTI, without vaginal
discharge or itching, make the probability of a UTI >
90%.20 Although this study has not been validated,
patients should be asked about symptoms suggesting a UTI mimic and a pelvic examination should
be considered. Female patients will often present to
July 2014 • www.ebmedicine.net
Recognizing Severity
A critical role of the emergency clinician when
evaluating the patient with a UTI is to recognize
the severity of the patient’s illness. Patients with
severe sepsis or shock need to be identified early, as
they will need intervention and source control. It is
5
Reprints: www.ebmedicine.net/empissues
important to recognize the signs of systemic inflammatory response syndrome (SIRS), which include
hyperthermia/hypothermia, leukocytosis, leukopenia, tachycardia, and tachypnea. These is especially
important for the at-risk patient populations, which
include the elderly, the immunocompromised, and
patients with comorbid conditions (such as indwelling catheters or urethral obstruction). Early imaging
studies are recommended in these patients.1,26,27
rule out a UTI in symptomatic women.28 This study
reported specificity ranging from 52% to 58% for
dysuria, 60% for frequency, 78% to 88% for urgency,
69% to 91% for fever, 19% for abdominal pain, and
76% to 77% for back pain. Evaluation for fever
(including a rectal temperature, when necessary) or
signs of systemic toxicity (including tachycardia)
can aid in differentiating lower UTI from a complicated UTI. A genitourinary examination may be
necessary in women who have vaginal complaints
and in all men with suspected UTIs. A careful abdominal examination may also help in diagnosing
other UTI/pyelonephritis mimics such as appendicitis or diverticulitis.1,20,22-27,29-31
Physical Examination
The physical examination of a patient with a suspected UTI should aid in confirming your pretest
probability of a UTI or in ruling in other entities.
A systematic review of the literature from 1965
to 2012 that included 948 studies confirmed that
there is no specific historical symptom or physical
examination finding that can accurately rule in or
Diagnostic Studies
Laboratory Studies
Basic Laboratory Tests
A WBC count may be warranted if the emergency
clinician suspects systemic illness, as this may
guide treatment regimens. A creatinine level may
be required before sending a patient for a computed tomography (CT) scan with contrast. If prior
laboratory values have been obtained, the trending
creatinine and blood urea nitrogen (BUN) values
may give the emergency clinician insight as to the
severity of renal pathology. There is no support in
the literature to routinely order “basic” laboratory
testing for patients presenting to the ED suspected
of having an uncomplicated UTI. For complicated
UTIs, including patients with comorbidities and
immunosuppression, laboratory testing may be warranted, at the discretion of the emergency clinician.
Table 1. Adult Urinary Tract Infection
Definitions And Patient Subsets
Uncomplicated UTI*
• Lower UTI (cystitis) in nonpregnant female
Complicated UTI†
• Upper UTI (pyelonephritis)‡
• Male
• Pregnant female
• Moderate or severe diabetes mellitus
• Anatomic abnormalities
• Cancer, chemotherapy, immunosuppression
• Impaired micturition
• Catheter, stent, or tube in urinary system
• Obstructive stone
• Hospital-associated UTI
• Treatment failure
Urine Dipstick Versus Microscopic Urinalysis
The quick turn-around of the point-of-care urine
dipstick versus laboratory urinalysis has made
diagnosing a UTI in the ED more efficient. The urine
dipstick has a sensitivity and specificity comparable to microscopic urinalysis.32-34 The most sensitive value from the urine dipstick is the leukocyte
esterase, while the presence of nitrates is the most
specific. When combining these 2 pieces of data
from the urine dipstick, the specificity reaches 100%
and the positive likelihood ratio nears infinity.33 In a
prospective study of 343 patients by Lammers et al,
the diagnostic capabilities of the urine dipstick and
urinalysis were compared to a gold standard of a
urine culture with > 100,000 cfu/mL.32 Table 3 (page
7) summarizes the findings of this study.
Additional prospective studies also compared
urine dipstick and urinalysis.32-34 (See Table 4,
page 7.) The urine collected from each study was a
midstream clean-catch urine specimen. According
to the pooled data, the presence of blood, leukocyte
esterase, or protein from the urine dipstick was very
sensitive; the only specific finding from the urine
*Urine culture not necessary
†
Urine culture necessary
‡
Pyelonephritis in nontoxic, healthy, young women can be treated as
"uncomplicated." (See text, page 5.)
Abbreviation: UTI, urinary tract infection.
Table 2. Risk Factors For Complicated
Urinary Tract Infections1
•
•
•
•
Pregnancy
Male sex
Moderate to severe diabetes or other immunosuppressed state
Structural abnormalities of urinary tract (kidney stones, renal and
perinephric abscess, emphysematous pyelonephritis, or polycystic
kidney disease)
• Functional abnormality of urinary tract (vesicoureteral reflux, spinal
cord injury, neurogenic bladder)
• Hospital-acquired infections
• Presence of external catheters (urethral, suprapubic, or nephrostomy tubes)
Copyright © 2014 EB Medicine. All rights reserved.
6
www.ebmedicine.net • July 2014
dipstick was nitrate. The microscopic urinalysis
had high sensitivities for individual measurements
of WBCs, red blood cells (RBCs), and bacteria. The
microscopic urinalysis was highly specific if both
WBCs and bacteria were present. When determining when to order a microscopic urinalysis, there is
no component that is more sensitive or specific. The
positive predictive value is equally high for a positive nitrate on dipstick or positive WBC and bacteria
on the microscopic urinalysis. Both modalities are
poor at ruling out UTI. If there is a suspicion for UTI
with a negative urine dipstick, the microanalysis
can help to rule in disease.35,36 A prospective study
of 3889 patients showed that, with a strong pretest
probability for a UTI, testing can be deferred and
treatment initiated.37
Urine Culture
Urine culture has been the gold standard for the
diagnosis of UTI, but due to the length of time to return results, it is difficult for a urine culture to be the
gold standard for ED decision making. According to
2010 IDSA guidelines, urine cultures were ordered
on patients with treatment failure, the complicated
UTI, or the pyelonephritis patient.38 Historically,
urine cultures have proven to be cost-ineffective and
would rarely change patient outcomes.39 In the past
several decades, resistance to standard UTI therapies has increased. In a retrospective study of 12,870
patients, there was a treatment failure in 441 patients
due to resistance to commonly prescribed antibiotics.40 Treatment failure was most prevalent in the
high-risk population. Commonly, hospital antibiograms are based on urine cultures obtained from
Table 3. Positive And Negative Predictive Values Of Urine Dipstick And Microscopic Urinalysis
With Corresponding Overtreatment And Undertreatment Rates
Testing Modality
PPV (%)
NPV (%)
Overtreatment Rate (%)
Undertreatment Rate (%)
LE or N or blood
51
94
49
6
LE > 2 and N
88
52
13
48
Urine Dipstick
Microscopic Urinalysis
RBC or WBC
50
93
50
7
RBC > 50 or WBC > 10
64
74
37
25
Abbreviations: LE, leukocyte esterase; N, nitrate; NPV, negative predictive value; PPV, positive predictive value; RBC, red blood cell; WBC, white blood
cell.
Reprinted from Annals of Emergency Medicine, Volume 38, Issue 5. Richard L. Lammers, Scott Gibson, Dave Kovacs, Wade Sears, and Gary Strachan. Comparison of test characteristics of urine dipstick and urinalysis at various test cutoff points. Pages 505-512. Copyright 2001, with permission
from Elsevier.
Table 4. Sensitivity, Specificity, And Likelihood Ratio For Urine Dipstick And Microscopic
Urinalysis
Testing Modality
Sensitivity (%)
Specificity (%)
Positive LR (%)
Negative LR (%)
Urine Dipstick
LE32-34
75-91
41-87
1.59-5.6
0.2-0.4
32-34
34-42
94-98
7.5-24.6
0.6-0.7
Blood33
92
42
2.6
0.2
Protein33
83
44
2.1
0.3
LE + N32,33
30-38
91-100
3.4 to infinity
0.6-0.8
LE or N32,33,43
91-92
39-41
1.5-1.6
0.2
N
Microscopic Urinalysis
32,34
WBC > 5
Bacteria > 0
RBC > 5
33,34
34
WBC or bacteria
33
WBC and bacteria
33,44
57-90
47-89
1.7-5
0.2-0.5
9-83
59-72
2.3-2.9
0.1-0.5
59-63
67-74
1.8-2.4
0.5-0.6
100
39
1.6
0
58
81
3
0.5
Abbreviations: LE, leukocyte esterase; LR, likelihood ratio; N, nitrate; NPV, negative predictive value; PPV, positive predictive value; RBC, red blood
cell; WBC, white blood cell.
July 2014 • www.ebmedicine.net
7
Reprints: www.ebmedicine.net/empissues
Imaging
the high-risk patient who presents to the ED and is
admitted to the hospital. Although not cost-effective,
the argument has been made to better tailor treatment to the general population, with antibiograms
representing all patients who present to the ED.41
Imaging is not necessary in cases of uncomplicated
UTIs. If a renal pathology is suspected, the options
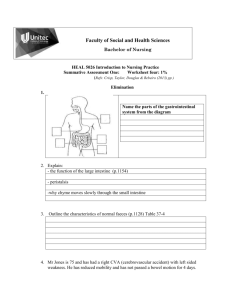
for imaging include plain-film abdominal radiography, ultrasound, and CT scan. Plain-film abdominal
radiography (kidneys, ureters, and bladder [KUB])
is of limited use by itself, with a sensitivity of 45%
to 59% and specificity of 77% for detecting renal
pathology.50 An abdominal radiograph may show
the presence of renal calculi or gas; however, the
sensitivity is lower than that of CT scan (92%-96%)5154
and does not demonstrate complications such
as ureteral obstruction or hydronephrosis.48 (See
Figure 1.)
When To Get A Urine Culture
When to obtain a urine culture in an uncomplicated
UTI varies in the literature. The general consensus is
to obtain a urine culture if symptoms do not resolve
following treatment.24,41,42 If the pretest probability
is high and a urine dipstick is negative, it is advisable to obtain a urine culture.24 It is generally agreed
in the literature that, when a patient is considered to
have a complicated UTI or pyelonephritis, cultures
should be obtained.24,41,42 A positive urine culture is
defined as > 105 colony-forming units.1
Intravenous Urethrogram
Intravenous urethrogram has fallen out of favor,
but it may have a place in diagnosing the pregnant
female with a renal stone and an equivocal ultrasound.55 The intravenous urethrogram is conducted
by injecting contrast intravenously and taking abdominal x-rays at 1 minute and 15 minutes, and then
any additional films needed.56 There is also support
for only a 30-minute single-shot film.57 An intravenous urethrogram has a higher sensitivity and
specificity than an abdominal radiograph in diag-
Blood Culture
In the uncomplicated UTI, blood cultures are not
warranted. For the patient with uncomplicated
pyelonephritis, blood cultures have not proven to
change the course of treatment, including in pregnant patients.45-47 For patients who are considered to
have complicated infections or are postmenopausal,
blood cultures have proven beneficial.48 A large recent meta-analysis of studies on the utility of blood
cultures concluded that they are of limited benefit
except in patients with pneumonia and sepsis.49 This
is due to the overwhelming mortality associated
with bacteremic patients, so tailoring antibiotics can
aid in targeted therapy.49
Figure 1. X-Ray Displaying Bilateral Renal
Calculi
Testing For Sexually Transmitted Infections
The patient's history will play a key part in determining whether to look beyond a diagnosis of simple cystitis. Diagnoses to be considered are urethritis
in men and women and pelvic inflammatory disease, cervicitis, tubal ovarian abscess, and vaginitis
in women. Characteristics for each infectious process
and historical clues are:35
• Cystitis: Dysuria, hematuria, increased urinary
frequency, abrupt onset of symptoms, severe
symptoms, suprapubic/low back pain or suprapubic tenderness.
• Other infections: Gradual onset of symptoms,
mild symptoms, vaginal discharge/bleeding,
lower abdominal pain, new sexual partner,
cervicitis/vulvovaginal herpetic lesions on
examination, vaginal discharge/odor, pruritus,
dyspareunia, external dysuria, and absence of
increased frequency or urgency.
For patients with signs, symptoms, physical
findings, or historical clues inconsistent with cystitis,
further investigations are warranted. This would
include investigations for sexually transmitted
diseases, vaginitis, yeast infections, and urethritis or
prostatitis in men.
Copyright © 2014 EB Medicine. All rights reserved.
Arrows point to calculi.
Used with permission under the Creative Commons Attribution 2.0
license by Bill Rhodes from Asheville [CC-BY-2.0 (http://creativecommons.org/licenses/by/2.0)], via Wikimedia Commons. Available at:
http://upload.wikimedia.org/wikipedia/commons/6/66/Kidney_stones_
abdominal_X-ray.jpg
8
www.ebmedicine.net • July 2014
nosing urinary calculus disease as the cause of acute
flank pain (64% vs 97% and 92% vs 94%, respectively).55,58,59 Compared to a CT scan, the intravenous
urethrogram does have a lower level of radiation exposure, but due to the nature of the examination, the
intravenous urethrogram can take longer to conduct,
advocating for the CT scan.60 (See Figure 2.)
echo (HASTE) MRU, without contrast, is a technique
that has emerged in the last decade as an accurate
method for stone diagnosis, and it is safe during
pregnancy. HASTE MRU sensitivity and specificity
for stone diagnosis is comparable to CT scan.65 The
gA gadolinium-enhanced MRU has better diagnostic
capabilities than the unenhanced MRU (with respect
to calculus identification), but it comes with increased
cost and risk of allergic reactions.62
Magnetic Resonance Imaging
MRI has been considered a second-line imaging modality if ultrasound is equivocal in the pregnant patient.61 MRI cannot directly identify calcifications, and
it relies on signal void for the diagnosis of calculi.62
MRI is also very expensive, can take several hours to
conduct and to be read, and may not be available in
all facilities. Unenhanced magnetic resonance urography (MRU) can accurately assess for the presence,
degree, and level of urinary tract obstruction, but
it has low sensitivity and specificity in identifying
stones.63,64 The half-fourier single-shot turbo-spin
Ultrasound
Ultrasound is noninvasive, does not involve irradiation, is cost-effective, and can provide valuable
clinical information immediately. Ultrasound can
reveal complications such as hydronephrosis, renal
or extrarenal abscesses, and distal hydroureter.31,66,67
(See Figure 3.) In 2 prospective studies of > 125
patients examined by an emergency physician with
bedside ultrasound for confirmation of nephrolithiasis, the sensitivities and specificities were 72%
to 80% and 37% to 73%, respectively.67,68 This argues
that ultrasound is a good option for a patient who
cannot undergo a CT scan, but the ultrasound must
be performed by skilled personnel, as diagnostic accuracy varies based on the provider’s skill.
For men who are at risk for benign prostatic hypertrophy, ultrasound should be part of the work-up
to determine whether there is obstructive uropathy.
Benign prostatic hypertrophy is common in elderly
males, and it can lead to obstruction uropathy
resulting in hydronephrosis, placing the patient at
higher risk for a UTI.69 Common characteristics of
benign prostatic hypertrophy include men over the
age of 60 years with lower urinary tract symptoms.
Lower urinary tract symptoms include urgency,
Figure 2. Intravenous Urethrogram
Demonstrating Contrast Filling The Renal
Pelvis, Ureters, And Bladder
Figure 3. Ultrasound Displaying
Hydronephrosis
Arrows point out the contrast filling of the renal pelvis, ureters, and
bladder.
Image used under the terms of the Creative Commons GNU Free
Documentation License, Version 1.3, courtesy of Glitzy queen00,
available at: http://upload.wikimedia.org/wikipedia/commons/f/f5/
Ivu_1.jpg
July 2014 • www.ebmedicine.net
Image courtesy of Dr. Bruno Di Muzio. www.radiopaedia.org (original
file here). Used with permission.
9
Reprints: www.ebmedicine.net/empissues
hesitancy, frequency, pain with urination, nocturia, weak stream, dribbling, or incomplete voiding.
Before starting any medications, infection should
be ruled out and imaging should be performed to
assess for the degree of obstruction.69,70 Ideal imaging modalities for the prostate and urinary include
ultrasound.69,70
high cost, collateral damage to the patient’s normal
bacterial biome, and resistance development. Indiscriminate use of broad-spectrum antibiotics is associated with higher incidence of general resistance in
a community and with Clostridium difficile infection.
National guidelines, books or pamphlets, or mobile
device applications are not likely to reflect all community environments.8,77-79
Resistance to trimethoprim-sulfamethoxazole
(TMP-SMX) and fluoroquinolones is now very
common, and according to multiple comprehensive
literature reviews, varies between 10% and 20%
in many communities.79,80 This trend is common
around the world, with resistance to TMP-SMX in
Turkey peaking at 50%, and drugs such as ampicillin having resistance rates up to 100% in Europe
and Africa.81 Resistance patterns change over time,
and they also vary from community to community,
so it is important for the emergency clinician to be
acquainted with local antibiograms for pathogens
associated with UTI. National antibiogram reports
lag behind local antibiograms and may not even be
representative of local antibiograms.
A recent study covering 16 European countries
and Canada showed clinical resistance to trimethoprim approaching 30% and sulfamethoxazole
approaching 50%. Another investigation in Seattle
demonstrated an increase in TMP-SMX resistance
from 8% to 16% in 4 years, and Michigan found
similar numbers over a 6-year period. Those at risk
for resistance included patients with recent antibiotic exposure, recent hospitalization, diabetes, 3 or
more UTIs in the past year and, possibly, the use of
oral contraceptives.82
Computed Tomography
A noncontrast CT scan can accurately localize renal
calculi, hydroureter, hydronephrosis, gas, and renal
abscesses. The addition of contrast can better assess
renal perfusion and for renal artery occlusion, renal
vein thrombosis, and renal infarction and abscess.
The literature has shown that, for the evaluation of
flank pain, ultrasound has better sensitivity (24%77%) versus CT (92%-96%).51-54 Given the increased
sensitivity and ability to diagnose a multitude of
pathologies, compared to ultrasound, a CT scan
has proven to be the imaging modality of choice for
renal pathology.53,55,71-73 In pregnancy, a low-dose CT
scan is an attractive newer modality, with a lower
fetal radiation dose than standard CT (4 mGy vs 25
mGy); however, it does still entail the use of radiation, which is preferably avoided in the pregnant
state. In a prospective study of 109 pregnant women,
the sensitivity and specificity of low-dose unenhanced helical CT were 96% and 97%, respectively,
with a 99% positive predictive value and 90% negative predictive value, respectively.74
Imaging Pearls
Overall, there are no formal guidelines for when
to use imaging to diagnose a UTI or for the type
of imaging to use. If a structural abnormality or a
renal pathology (such as renal abscess, urolithiasis,
emphysematous pyelonephritis, or pyelonephrosis),
is suspected, imaging is warranted. An abdominal
plain film will accurately diagnose a renal stone only
59% of the time.50 An ultrasound has variable sensitivity and is dependent on the size of the stone for
more accurate diagnosis,75 but it is a first-line option
for a pregnant woman. An intravenous urethrogram
should be reserved for women with a negative ultrasound who are strongly suspected of having nephrolithiasis.72 A CT scan has the highest sensitivity and
specificity and has the capability to diagnose other
pathology, unlike other imaging modalities.26,72,76
The clinical utility and cost-effectiveness of performing routine imaging in all patients with UTI with
suspected renal involvement needs further prospective evaluation.
Treatment Of Lower Urinary Tract Infection
Treatment for UTIs depends on a multitude of different variables, including host factors, presentation,
degree of infection, and local resistance patterns.
Traditionally, the literature shows that a 3-day
course of trimethoprim is the first-line choice of
drug therapy for uncomplicated UTI. A 3-day course
eliminates 94% of infections. Single-dose treatment
is less effective than the 3-day course, eliminating only 87% of cases, and longer courses have not
been shown to be more effective.24,83,84 Interestingly,
trimethoprim can cause hypersensitivity reactions
that may be falsely attributed to sulfa when given
in combination. Fluoroquinolones are an acceptable
alternative if local TMP-SMX resistance reaches 15%
to 20%, as they are found to be active against the
main offending bacteria, including gram-negative
organisms and S saprophyticus. However, small studies of TMP-SMX have shown clinical cure rates of
up to 60% in patients with known resistant strains.24
Ofloxacin (or ciprofloxacin) is also an accepted
form of treatment, but there are concerns about
promoting bacterial resistance and the high cost
Treatment
Several factors must be considered when choosing
antibiotic therapy. Indiscriminate use of “big gun”
broad-spectrum antibiotics is not advised due to
Copyright © 2014 EB Medicine. All rights reserved.
10
www.ebmedicine.net • July 2014
Treatment With Intravenous Fluids
burden to the patient.24 With increasing resistance
to TMP-SMX and fluoroquinolones, nitrofurantoin (Macrodantin®, Macrobid®, Furadantin®) and
fosfomycin have emerged as first-line therapies in
many communities.38 With the exception of patients
with an allergy, nitrofurantoin is the first-line agent
in pregnant patients with cystitis. Although nitrofurantoin typically has very low resistance patterns, it
is known to be active predominantly toward E coli
and less active toward other gram-negative organisms. A single 3 g dose of fosfomycin is approved for
use to treat uncomplicated UTIs, but the efficacy is
lower than TMP-SMX or fluoroquinolones.85 However, resistance is extremely rare, so it may serve as
a useful drug in the patient with multidrug allergies
or who has a multidrug-resistant UTI. Outside of
obstetrics-gynecology circles, fosfomycin is not as
well known as the other agents. That being said, it is
on many hospital formularies and can be ordered at
commercial outpatient pharmacies. Fosfomycin has
an attractive compliance profile because it is a 1-time
dose, and it has demonstrated good effectiveness.
Typically, a 3-day course of antibiotics for uncomplicated cystitis cures the infection; however, in
situations where the therapy fails, urine cultures and
a 14-day course of antibiotics are recommended.84
For example, prostatitis is a complication of an
ascending UTI requiring a minimum of 2 weeks of
outpatient antibiotics. Treatment typically involves
a fluoroquinolone (such as ciprofloxacin 500 mg
twice per day). Another example of a complication
requiring an extended duration of treatment is with
hospital-acquired UTIs.
Acute pyelonephritis can be treated with oral
ciprofloxacin 500 mg twice per day for 7 to 14 days
with or without an initial 400 mg intravenous dose.
As an alternative to a fluoroquinolone, 1 g IV ceftriaxone dosed every 24 hours or gentamicin dosed
every 24 hours can also be used until the patient can
be converted to oral therapy. Generally, this treatment regimen is recommended over oral or intravenous fluoroquinolones if the local resistance pattern
exceeds 10%. If there is a known susceptibility to
TMP-SMX, a 14-day course may be appropriate as
well. When local resistance to TMP-SMX and fluoroquinolones is higher than 10% to 20%, cefuroxime
500 mg twice daily for 7 to 10 days or cefpodoxime
400 mg twice daily for 7 to 10 days may be used.84,86
Cranberry juice is a strategy commonly employed for treatment and prevention of UTIs. Studies show that there may be some beneficial effect to
this strategy, as the cranberry contains 3 proanthocyanidin chemical compounds that were shown in
the laboratory to prevent adherence of E coli to the
uroepithelial cells.24,87 Randomized studies demonstrate that 200 to 750 mL of cranberry juice daily or
daily cranberry tablets can reduce infection rates by
up to 20%.24
July 2014 • www.ebmedicine.net
Intravenous fluids (IVF) are generally indicated for
pyelonephritis with vomiting, when a fluid deficit
is present on physical examination, when a patient
appears dehydrated, or if systemic infection is being
considered. To date, no trials of intravenous hydration in pyelonephritis are available. It is important
to consider that tachycardia is one of the criteria
for sepsis, so IVF are useful in helping distinguish
dehydration from sepsis in pyelonephritis.88 Resolution of the tachycardia with IVF makes the patient
feel better, and it is also important in screening for
sepsis, as persistent tachycardia is one of the criteria
for the diagnosis of sepsis.
Pain And Nausea Control
UTIs can be painful and, when severe, they are often
accompanied with nausea. Acute uncomplicated UTIs
do not cause renal insufficiency, so nonsteroidal antiinflammatory drugs as well as opioids are reasonable
treatments for pain. Nausea frequently accompanies
pyelonephritis, and it is best to treat it aggressively
so that the patient can start drinking and taking the
appropriate medications as soon as possible.
Phenazopyridine HCl (Pyridium®) is used to
treat the urethral and bladder irritation associated
with a UTI, and it is fairly effective, although it loses
effectiveness in 2 to 3 days. It can cause methemoglobinemia, and overdose is very serious, thus it is
generally prescribed for only 2 to 3 days.89,90 Other
potential side effects of phenazopyridine include
urine discoloration, pruritus, nausea, and contact
lens discoloration. Anaphylactoid reaction is a rare,
but serious, reaction to phenazopyridine.24,84-86
Treatment For Men
UTIs are uncommon in men, due to the longer length
and narrower caliber of the male urethra. Because
UTIs are atypical in males, prostatitis and sexually
transmitted infections must be considered. The gestalt
from the literature is that UTIs in men are considered complicated and, therefore, cultures are generally indicated even in equivocal cases (such as trace
leukocytes or just trace blood). In sexually active men,
urethral swabs for gonorrhea and Chlamydia trachomatis should be considered when urethritis is the
predominant symptom.14,91-93
Another complicating factor with a UTI in males
is the development of acute bacterial prostatitis as a
result of an ascending infection. E coli is the causative organism in 87% of these cases, with Proteus
mirabilis, Pseudomonas, Klebsiella, and Enterococcus
comprising roughly the remainder of cases. Neisseria
gonorrhoeae should typically be considered in young
sexually active men. In rare cases and in immunocompromised patients, tuberculosis has been implicated in acute infection. Males with prostatitis will
generally present as a febrile UTI with pain reported
11
Reprints: www.ebmedicine.net/empissues
Clinical Pathways For Antibiotics For Urinary Tract Infection
In The Emergency Department
Lower urinary tract infection
YES
NO
Local TMP-SMX
susceptibility 80%-90%?
NO OR UNKNOWN
YES
Nitrofurantoin-allergic?
Penicillin-allergic?
YES (ANAPHYLAXIS)
TMP/SMX-allergic?
OR
NO OR MILD
First or second-generation
cephalosporin,
3-5 day course*
(Class II)
TMP-SMX,
3-5 day course*
(Class II)
NO
• Ciprofloxacin or
ofloxacin, 3-5 day
course† or
• Fosfomycin PO, 1
dose
(Class II)
Nitrofurantoin,
3-5 day course (Class II)
Outpatient upper
urinary tract infection
YES
NO
TMP-SMX-allergic?
NO
TMP-SMX PO,
10-14 day course*
(Class II)
Local TMP-SMX
susceptibility > 90%?
YES
YES/SEVERE
Ciprofloxacin-allergic?
Ciprofloxacin or ofloxacin PO, 10-14 day
course† (Class II)
NO/UNKNOWN
Penicillin-allergic?
NO OR MILD
YES
Gentamicin IV, qd
5-7 days (Class II)
Second- or third-generation cephalosporin PO,
10-14 days (Class II)
*Do not use in third trimester of pregnancy.
†
Do not use in pregnancy.
Abbreviations: bid, 2 times per day; IV, intravenous; PO, by mouth; qd, 1 time per day; TMP-SMX, trimethoprim-sulfamethoxazole.
Adapted with permission from SafetyCore™. © SafetyCore™ 2014.
For Class of Evidence Definitions, see page 13.
Copyright © 2014 EB Medicine. All rights reserved.
12
www.ebmedicine.net • July 2014
in the abdomen, perineum, or rectum. They may
also present with chills, or vomiting. Severe cases
may include changes in mentation.94 If changes in
mentation are present, sepsis should be considered.
that address the risk of treatment to the fetus using
common antibiotic regimens in UTI, such as nitrofurantoin, TMP-SMX, penicillins, or cephalosporins.
TMP-SMX is a Category C drug in pregnancy and
should not be used in the first trimester because it
inhibits folate metabolism and may lead to neural
tube defects. Also, in the third trimester, TMP-SMX
has shown a clear link to the development of kernicterus. Aminoglycoside, a Category D drug, will cross
the placenta and could, theoretically, lead to renal
and ototoxicity. Fluoroquinolones and tetracycline
are Category C and D, respectively, and are also not
recommended due to their potential for toxicity to
the fetus. Adherence to local resistance patterns applies as in nonpregnant women.
Special Circumstances
Pregnant Patients
Pregnancy is associated with decreased ureteral
motility and mild hydronephrosis. Therefore, there
is an increased risk of both lower and upper UTI.
Given the increased materno-fetal morbidity associated with pyelonephritis, traditional practice calls
for inpatient treatment. Due to the considerable risk
to patient/fetus, most emergency clinicians and
obstetricians admit pregnant women for parenteral
antibiotics such as a second- or third-generation
cephalosporin, gentamicin, or aztreonam.84,86,95
There is some evidence (1b) to suggest an outpatient
option for these patients.96 The patients were mild
to moderately ill, and received 2 doses of intramuscular ceftriaxone prior to discharge with very close
follow-up (48-72 hours).19,24,83-86,95-100
Duration Of Therapy in Pregnancy
A 2011 Cochrane systematic review looked at
duration of treatment of asymptomatic bacteriuria
in pregnant patients.19 The 1622 subjects from 13
studies were compared with single-dose versus 4- to
7-day treatments. Although the studies were of limited quality, it was generally found that single-dose
drug therapy was less effective than short- or fullcourse treatments, even when trials were compared
with the similar antibiotics.19 The current recommendation is to continue standard treatment for 5 to 7
days, depending on the antibiotic.
Upper Urinary Tract Infection In Pregnancy
Bacteriuria with or without symptoms has been
reported to be as high as 20% in pregnancy,101 and,
if left untreated, it is associated with a 20% to 30%
risk of developing pyelonephritis, which can be a
serious threat to mother and fetus, increasing the
risk of premature labor and low birth weight.102
Given the significant risk of maternal/fetal morbidity, a consensus guideline recommends treatment,
as well as a culture, for all pregnant women with
suspected UTIs.103 Asymptomatic bacteriuria is also
treated, generally with a 3-day course of antibiotics,
and a urine culture is generally indicated.99,100,103
The recommended antibiotic treatment regimens for
pregnant women are similar to nonpregnant women, as there is no clear evidence that any particular
antibiotic or dosing regimen has any advantage
in pregnancy.19 There are no prospective studies
Patients With Indwelling Catheters
Catheter-associated UTI (CA-UTI) is the most common cause of nosocomial infections and the leading
cause of gram-negative sepsis in hospitals. A large
number of these patients are asymptomatic; however, 10% to 25% may develop signs and symptoms
of infection and would require treatment. Candida
is becoming a common complication in indwelling
catheter-related infections, especially in ICU patients receiving broad-spectrum antibiotics. Again,
treatment of candiduria should be reserved for all
symptomatic patients and should include the use of
fluconazole for simple infection and amphotericin
Class Of Evidence Definitions
Each action in the clinical pathways section of Emergency Medicine Practice receives a score based on the following definitions.
Class I
Class II
• Always acceptable, safe
• Safe, acceptable
• Definitely useful
• Probably useful
• Proven in both efficacy and effectiveness
Level of Evidence:
Level of Evidence:
• Generally higher levels of evidence
• One or more large prospective studies
• Nonrandomized or retrospective studies:
are present (with rare exceptions)
historic, cohort, or case control studies
• High-quality meta-analyses
• Less robust randomized controlled trials
• Study results consistently positive and
• Results consistently positive
compelling
Class III
• May be acceptable
• Possibly useful
• Considered optional or alternative treatments
Level of Evidence:
• Generally lower or intermediate levels
of evidence
• Case series, animal studies, consensus panels
• Occasionally positive results
Indeterminate
• Continuing area of research
• No recommendations until further
research
Level of Evidence:
• Evidence not available
• Higher studies in progress
• Results inconsistent, contradictory
• Results not compelling
This clinical pathway is intended to supplement, rather than substitute for, professional judgment and may be changed depending upon a patient’s individual
needs. Failure to comply with this pathway does not represent a breach of the standard of care.
Copyright © 2014 EB Medicine. 1-800-249-5770. No part of this publication may be reproduced in any format without written consent of EB Medicine.
July 2014 • www.ebmedicine.net
13
Reprints: www.ebmedicine.net/empissues
Patients With Nephrolithiasis
for severely ill patients. All patients with catheter-related infections should have their catheters replaced
and reevaluated for necessity.84
Patients with indwelling catheters frequently
present to the ED, and UTIs in these patients represent the most common healthcare-associated infection worldwide.104 The diagnosis of UTIs in these
patients can be quite challenging for a number of
reasons. Patients with indwelling catheters will often
have bacteriuria and pyuria, and all patients with
catheters indwelling for more than 1 month will
be colonized.105,106 Furthermore, these patients are
more frequently elderly or nursing home patients
with a number of comorbidities and are often not
able to verbalize their symptoms. This patient population will also often present atypically or will have
other sources for fever. The IDSA has developed
evidence-based guidelines for the diagnosis and
treatment of UTIs in patients with indwelling catheters.107 These guidelines suggest that the presence
or degree of pyuria and the presence of odorous or
cloudy urine should not be used to diagnose UTI.
Ideally, if a UTI is suspected, the catheter should be
replaced before the urine is analyzed or the culture
is sent, although this may not always be practical in
the ED setting. Also, patients who have their catheters replaced prior to treatment of their UTI will
get better faster and are more likely to be cured.37
(Grade B recommendation from the Scottish Intercollegiate Network.103)
Signs and symptoms compatible with CAUTI include new-onset or worsening fever, rigors,
altered mental status, or malaise or lethargy with
no other identifiable cause; flank pain or costovertebral angle tenderness; acute hematuria; or pelvic
discomfort. In patients with spinal cord injury,
UTI can present as increased spasticity, autonomic
dysreflexia, or a sense of unease. As with all patients with complicated UTIs, it is difficult to make
specific antibiotic recommendations, but the IDSA
recommends a 7-day course in patients with prompt
clinical response (> 48 hours) to antibiotics, and they
recommend extending the regimen to 10 to 14 days
for a delayed response.107 Patients with CA-UTI are
more often hospitalized and exposed to antibiotics
and will have a higher rate of multidrug-resistant
species (such as vancomycin-resistant Enterococcus)
or extended-spectrum beta-lactamase producers.
Selection of empiric antibiotics should be individualized and should take into account prior urine culture
results, recent hospitalization, prior antimicrobial
exposure, or suspected institutional susceptibilities.
Because resistant microorganisms may be acquired
by transfer from other patients, urine catheter
systems should be carefully disposed of, and hands
must be properly washed and decontaminated before and after insertion and management.
Copyright © 2014 EB Medicine. All rights reserved.
Patients who have kidney stones associated with
UTIs will have a broader range of pathogens as a
possible etiology. In contrast to simple UTIs, this
subset of patients will more often have infection
from Proteus and Pseudomonas species.108 Diagnosing a UTI in these patients can be difficult due to
a wide spectrum of clinical presentations and a
variable degree of pyuria. In a single-center prospective observational study with 360 patients, the
probability of infection increased as the degree of
pyuria increased.41 Additionally, in a prospective
study including 73 patients with a ureteral obstruction, the midstream urine culture was not reliable
when the infection was proximal to the stone.109
Treatment strategies will depend on the severity of
illness. Given the potential for significant complications (such as severe sepsis and abscess formation),
a more liberal antibiotic strategy seems reasonable.
Empiric antibiotics should address the broader
range of pathogens. In patients with pyelonephritis who are obstructed, emergent consultation for
proximal decompression is necessary. In the sickest
subset of patients, one should be attempting to rule
out an obstruction because, without a source control
strategy, these patients will not get better. On the
other hand, nonobstructive stones with concurrent
UTI may be treated with outpatient antibiotics and
outpatient urologic follow-up, depending on the
clinical scenario.41,86,108,109
Patients With Diabetes Mellitus/Renal
Transplant/Immunosuppression
Patients with complex comorbidities have UTIs with
a broad spectrum of pathogens, and they lack host
defense mechanisms, making them more susceptible
to treatment failure.110 These patients are also prone
to a number of complications.
Diabetic patients are more susceptible to acute
cystitis and pyelonephritis when compared to their
nondiabetic counterparts. This is thought to be
secondary to bladder dysfunction from neuropathy.
More concerning in diabetic patients is the development of emphysematous pyelonephritis, a fulminant
necrotizing infection of the renal parenchyma. This
infection will require parenteral antibiotics and surgical intervention for possible nephrectomy.84,86,95,111
Renal transplant patients are at risk for graft failure and, like other immunosuppressed patients, they
are more susceptible to viral and fungal infections.
Treatment in these patients is more complicated for
a number of reasons. The potential danger of antibiotics in renal impairment must be considered. Nitrofurantoin is contraindicated in renal insufficiency,
and there is a substantial risk of nephrotoxicity
with aminoglycosides.112 There are also important
interactions to consider between immunosuppressive agents and antibiotics. Because of these factors
14
www.ebmedicine.net • July 2014
and the broad range of pathogens, there are no
published consensus guidelines for these patients.
In these complicated cases, it is especially important
to send a urine culture in all suspected UTIs, and
consider specialist consultation before beginning
empiric treatment.
Antibiotic stewardship programs are established
to optimize treatment options for overtreated conditions. These programs include recommending types
of therapy, dosing regimens, and duration of treatment in an effort to minimize healthcare costs, maximize patient outcome, and limit antibiotic-resistant
bacteria strains. Antibiotic stewardship programs
exist for asymptomatic bacteriuria, catheter-associated infections, multidrug-resistant gram-negative
urinary infections, simple cystitis, and pyelonephritis. These programs focus on the frequency of
overtreatment, proper diagnostic modalities, who to
screen and who not to screen, and recommendations
for management. 114,116-118
Antibiograms demonstrate local resistance patterns and help to guide the practitioner on which
antibiotics may be ineffective on their local patient
population. However, antibiograms encompass data
from both the outpatient and inpatient setting and
they may actually overestimate antibiotic resistance.
A recent study conducted in New Zealand showed
19% trimethoprim resistance in hospital isolates of
E coli but only 11% in the community. Similarly, in
Singapore, 46% of hospital isolates of E coli were resistant to TMP-SMX but only 21% from community
clinics. This suggests that, although hospital antibiograms are helpful in assessing inpatient antibiotic
resistance, they may also overestimate community
resistance patterns.8,10,77-79,82
Controversies And Cutting Edge
Familial disposition to UTI and pyelonephritis has
been documented.113 This relationship is thought
to be secondary to a predisposition to persistent
vaginal colonization with E coli. Pedigree studies
suggest that more than 1 gene may be involved in
the inheritance of UTI susceptibility, and that both
maternal and paternal sides of the family can pass
this gene. This same study found that although the
disease penetrance was higher in females, males also
had a higher frequency of pyelonephritis.113 Based
on data from animal models and family pedigrees,
low expression of the host defense gene, CXCR1,
is thought to be a predisposing factor in the development of acute pyelonephritis. This can become
important in the context of pediatric patients,
especially those with mechanical defects (such as
urinary reflux), as identification may make it possible to decrease the risk of recurrent pyelonephritis
and subsequent renal scarring through more intense
follow-up and therapy. CXCR1 expression may
be quantified after a child’s first episode of febrile
UTI (using approaches similar to those used with
suspected cystic fibrosis patients) to detect polymorphisms in gene expression.113 The clinical use of such
information needs further research and development
and may be purely academic at this point, but as we
delve further into personalized medicine, it has the
potential to add to the disposition decision-making
process for patients who are suspected of having
subclinical or early UTI or pyelonephritis in whom
you are considering empiric treatment.
Additional Resources And Applications
There are a variety of resources to help the emergency clinician.
1. Android and iPhone applications: CD Antibiotics Pocket, EMRA Antibiotic Guide, and Infectious Disease Compendium. They are available
in trial form on Google Play and iTunes app
stores. They are easy to access and quick to use,
but they lack local data for the emergency clinician’s particular setting.
2. Local antibiograms: This will give the emergency clinician the most up-to-date information on
local susceptibility patterns. The most common
organisms to consider in UTI are E coli, Klebsiella,
Proteus, and E faecalis.
3. Local antibiotic stewardship programs: A welldesigned antibiotic stewardship program gives
best-practice recommendations for the local setting and constitutes the local standard of care.
Antibiotic Stewardship Programs
Antibiotic stewardship programs, far from presenting a barrier to the clinician, have been demonstrated to be a positive tool. They are associated with
decreased inappropriate antibiotic use, decreased
resistance, decreased complications, improved outcomes, and lower cost of care. Antibiotic stewardship programs take into account local antibiograms
and the site of infection to give recommendations
for optimal therapy. They can enforce best practices
by developing hard-to-override electronic order
sets and by referral for peer review. In our view,
antibiotic stewardship program recommendations
constitute the local standard of care for antibiotic
prescribing. Emergency clinicians who practice in a
setting with no antibiotic stewardship program are
encouraged to institute and/or adopt this tool.114-118
July 2014 • www.ebmedicine.net
Timing Of First Dose Of Antibiotic
There are no studies on the optimal timing of the first
dose of antibiotic for UTI. Drawing from the improvements in outcomes associated with protocols for early
antibiotics in community-acquired pneumonia119
and sepsis,120 it is reasonable to extrapolate that early
treatment of UTIs with antibiotics in the ED should
also be associated with improved outcomes. A 2007
15
Reprints: www.ebmedicine.net/empissues
prospective study of 278 infants with UTI demonstrated decreased renal inflammation when antibiotic
therapy was instituted within 24 hours of onset of
symptoms.121 Administering the first dose of antibiotic in the ED prior to discharge has not been compared
with administration at home once the patient has
picked up the prescription at the pharmacy; however,
given the basic principle of bacterial doubling time
and the available literature, administration of the first
dose in the ED prior to discharge is likely a beneficial
and low-risk intervention.
These studies included initial observation and treatment with parenteral antibiotics; however, no outpatient trials have been done in pregnant patients in
whom oral therapy was used alone.
Criteria For Safe Discharge
A patient may be safely discharged from the ED
provided the patient has/is:
1. Stable vital signs
2. Tolerating oral fluids
3. First time visit for this infection
4. No obstruction to voiding
5. No complication (such as perinephric abscess or
sepsis or SIRS)
6. Not pregnant
7. Reliable means for obtaining prescription
8. Reliable follow-up provider or can return to the
ED in case of complications
Obtaining Cultures
It bears repeating that indications for cultures in an
uncomplicated UTI vary in the literature. The general consensus is to obtain cultures if symptoms do
not resolve following treatment.24,41,42 If the pretest
probability is high and a urine dipstick is negative, it
is advisable to obtain a urine culture.24 It is generally
agreed upon in the literature that if a patient is male
or considered to have immunosuppression, comorbid conditions, a complicated UTI or pyelonephritis,
cultures should be obtained.24,41,42 It can be argued
that liberally culturing UTIs is best for determining
local resistance patterns.
Predischarge Checklist
1.
2.
3.
4.
5.
6.
All necessary samples have been obtained
Patient is hemodynamically stable
Pain is well controlled
Patient is tolerating oral fluids
Patient has access to obtain medications
Patient has given a reliable follow-up contact
number
7. Patient has a place to follow up for complications
8. The patient has met the criteria for an uncomplicated UTI or pyelonephritis
Disposition
When To Admit
The main indications for hospitalization are intractable nausea or vomiting (ie, inability to tolerate
fluids), hemodynamic instability (including severe
sepsis/septic shock), and the presence of complications (eg, obstruction, emphysematous pyelonephritis). Other reasons for hospitalization may include
the existence of concomitant immunocompromised
states (eg, diabetes mellitus, cancer), the presence of
indwelling catheters, failure of outpatient therapy,
and poor social support (eg, inability to purchase
medications or follow up as recommended, or
homelessness).41 Patients who present with nausea
and vomiting who improve with treatment in the
ED may be safe to discharge without an inpatient
stay.122,123 The patient should be immunocompetent
and have adequate follow-up.124 There is also literature to support a single-dose treatment with intravenous antibiotics prior to discharge.125,126 The patient
should give a reliable way to be contacted for culture
results, if obtained.
Pregnant women with pyelonephritis are generally admitted to the hospital (or observation unit)
for intravenous antibiotics, due to the complications
that could ensue for the mother and fetus. They can
be discharged from the ED selectively when well
hydrated, well appearing, tolerating oral intake, and
with good follow-up. Oral outpatient therapy has
been shown to be safe and effective for the treatment
of selected pregnant patients with pyelonephritis.
Copyright © 2014 EB Medicine. All rights reserved.
Follow-Up
The patient should have adequate follow-up to ensure resolution of disease and address any complications. Their primary care physician may also obtain
culture results for the patient.
Summary
The diagnosis of UTI is relatively simple, but the
management of UTI is relatively complex. The
cornerstone of therapy is determining whether the
patient has a lower UTI or an upper UTI and whether the patient has a complicated or uncomplicated
UTI. These 2 factors will determine whether antibiotic therapy is necessary, for how long, and whether
cultures are indicated.
Choosing antibiotic therapy is best done using
up-to-date and local antibiograms or, when available, the recommendations of the local antibiotic
stewardship program. Antibiotic stewardship
programs have been shown to be beneficial, and
they constitute the best-practice/standard of care
for the practice environment. The drug of choice for
lower UTI at this time is, generally, nitrofurantoin.
Fosfomycin is a very good and well-studied alternative, but it is not widely available in the USA. If
16
www.ebmedicine.net • July 2014
the UTI is uncomplicated and a lower, no cultures
are necessary. If the UTI is complicated and lower,
then cultures are indicated. Most pyelonephritis
cases should have cultures obtained. The oral drugs
of choice for pyelonephritis vary from community
to community. Gentamicin, in the once-daily dosing, remains highly effective for pyelonephritis in
the admitted patient with normal renal function.
Second- and third-generation cephalosporins are
generally favored over fluoroquinolones. In the case
of TMP-SMX allergy and severe penicillin allergy,
fluoroquinolones at about a 50% increased dosing
may be the only option.
The emergency clinician should be aware that
a percentage of patients with pyelonephritis have
early sepsis and should be aware of the diagnostic
criteria for sepsis from the Surviving Sepsis Campaign. Patients with UTI meeting criteria for sepsis
should be considered for admission to rule out
progression to sepsis. Sepsis guidelines have become
much more inclusive.88 Under the Surviving Sepsis
Campaign, most patients with pyelonephritis meet
criteria for early sepsis, at least upon arrival, if they
have an elevated heart rate and an elevated temperature. A full discussion of the sepsis guidelines
is beyond the scope of this article, and the reader is
encouraged the review the 2014 article, "The Surviving Sepsis Campaign Guidelines 2012: Update for
Emergency Physicians," in the Annals of Emergency
Medicine, by Jones et al.88 Additional helpful resources for understanding the latest guidelines and
for screening include the “Bellevue Severe Sepsis
Protocol” and “Sepsis Clinical Guide” mobile device
applications to screen for sepsis.
spectrum antibiotics and admitted him to the hospital.
In your final patient, you informed her that she was
pregnant prior to initiating treatment. She was surprised,
even though you weren’t. You told her that you perform a
urine pregnancy check in every childbearing-aged women
because it changes your treatment plan. You chose an
appropriate antibiotic for her, and then you discussed the
need for admission with the obstetrician.
References
Evidence-based medicine requires a critical appraisal of the literature based upon study methodology and number of subjects. Not all references are
equally robust. The findings of a large, prospective,
random­ized, and blinded trial should carry more
weight than a case report.
To help the reader judge the strength of each
reference, pertinent information about the study
will be included in bold type following the ref­
erence, where available. In addition, the most informative references cited in this paper, as determined
by the authors, will be noted by an asterisk (*) next
to the number of the reference.
1.* Takhar SS, Moran GJ. Diagnosis and management of urinary
tract infection in the emergency department and outpatient
settings. Infect Dis Clin North Am. 2014;28(1):33-48. (Review)
2. Moore KN, Day RA, Albers M. Pathogenesis of urinary tract
infections: a review. J Clin Nurs. 2002;11(5):568-574. (Review)
3. Singh-Grewal D, Macdessi J, Craig J. Circumcision for the
prevention of urinary tract infection in boys: a systematic
review of randomised trials and observational studies. Arch
Dis Child. 2005;90(8):853-858. (Meta-analysis; 12 studies,
402,908 children)
4. Celik O, Ipekci T, Aydogdu O, et al. Current medical diagnosis and management of vesicoureteral reflux in children.
Nephrourol Mon. 2014;6(1):e13534. (Review)
5. Yoshimura N, Chancellor MB. Neurophysiology of lower
urinary tract function and dysfunction. Rev Urol. 2003;5
Suppl 8:S3-S10. (Review)
6. Cooper CS, Joudi FN, Williams RD. Urology. In: Doherty
GM, editor. Current Diagnosis and Treatment: Surgery. 13th ed.
New York: McGraw-Hill Companies, Inc; 2010. (Textbook)
7. Morton DA, Foreman KB, Albertine KH, eds. Pelvis and
Perineum. In: The Big Picture: Gross Anatomy. New York: The
McGraw-Hill Companies, Inc.; 2011. (Textbook)
8. Andrade SS, Sader HS, Jones RN, et al. Increased resistance
to first-line agents among bacterial pathogens isolated from
urinary tract infections in Latin America: time for local
guidelines? Mem Inst Oswaldo Cruz. 2006;101(7):741-748.
(Laboratory research; 611 samples)
9. Lau SM, Peng MY, Chang FY. Resistance rates to commonly
used antimicrobials among pathogens of both bacteremic
and non-bacteremic community-acquired urinary tract infection. J Microbiol Immunol Infect. 2004;37(3):185-191. (Casecontrol; 201 cases)
10. Karlowsky JA, Jones ME, Thornsberry C, et al. Prevalence
of antimicrobial resistance among urinary tract pathogens
isolated from female outpatients across the US in 1999. Int J
Antimicrob Agents. 2001;18(2):121-127. (Laboratory research)
11. Dieter RS. Sterile pyuria: a differential diagnosis. Compr Ther.
2000;26(3):150-152. (Review)
12. Bermudez T, Amado Diequez, and Montes Mastrapa.
Urological manifestations of acute appendicitis. Archivos
Case Conclusions
The first patient was having vaginal discharge and, given
your understanding of the substantial overlap of UTI
symptoms and urethritis, you performed a pelvic examination and sent cultures for STIs. You decided to give her an
IM dose of ceftriaxone and a subsequent levofloxacin prescription to cover for cystitis and Chlamydia trachomatis.
For your second patient, you were not deterred by
her lack of fever or symptoms. She admitted to taking
ibuprofen prior to arrival and you recognized her risk for
pyelonephritis with concurrent antibiotics. Surprisingly,
your bedside ultrasound revealed an acute obstruction
in her right kidney. The urologist was impressed by your
clinical acumen and she said she would see her for an
acute urolithiasis obstruction and pyelonephritis.
For your nursing home patient, your investigation uncovered that he had not had his catheter changed
in months. After a thorough physical examination and
careful evaluation to rule out other sources for fever, you
had the nurse replace the Foley catheter before sending a
urinalysis and urine culture. Your workup was consistent
with a complicated UTI. You began appropriate broadJuly 2014 • www.ebmedicine.net
17
Reprints: www.ebmedicine.net/empissues
Espanoles De Urologica. 2005;58(3):207-212. (Retrospective
case-control; 500 patients)
13. Pandit L, Ouslander JG. Postmenopausal vaginal atrophy
and atrophic vaginitis. Am J Med Sci. 1997;314(4):228-231.
(Review)
14. Lipsky BA. Prostatitis and urinary tract infection in men:
what’s new; what’s true? Am J Med. 1999;106(3):327-334.
(Review)
15. Easter JS. Selected Urologic Problems. In: Rosen’s Emergency
Medicine: Concepts and Clinical Practice. 7th ed. Philadelphia,
PA: Mosby Elsevier. 2010;1297-1298. (Textbook)
16. Schauberger CW, Merkitch KW, Prell AM. Acute cystitis in
women: experience with a telephone-based algorithm. WMJ.
2007;106(6):326-329. (Retrospective study; 273 patients)
17. Blozik E, Sommer-Meyer C, Cerezo M, et al. UTI in women.
Consider telemedical management. BMJ. 2010;340:c1464.
(Case series)
18. Widmeier K, Wesley K. Infection detection: Identifying &
understanding sepsis in the prehospital setting, part 1 of 2.
JEMS. 2014;39(1):34-37. (Review)
Risk Management Pitfalls For Urinary Tract Infection (Continued on page 19)
1. “Fever and tachycardia are routine with pyelonephritis, and I only need to screen for sepsis
if the patient looks septic.”
The definition of sepsis has recently been defined
much more broadly by the Surviving Sepsis
Campaign guidelines. A patient needs only to
have a source of infection and 2 of 24 criteria
positive to meet the current definition for the
diagnosis of sepsis. Fever and tachycardia, which
are frequently present in pyelonephritis, qualify
the patient as having sepsis by the Surviving
Sepsis Campaign guidelines. Nonetheless, in our
view, the criteria for sepsis cannot be interpreted
to mean that every patient who presents febrile
and tachycardic must be admitted. Rather, the
presence of fever and tachycardia should serve
as a trigger to treat the fever and tachycardia and
to consider further workup for the presence of
sepsis as a definite process. IV fluids are indicated
as well as treatment of the fever. Further
laboratory tests (such as a complete blood count,
a basic metabolic profile, and a lactate level) can
be considered to see if more criteria for sepsis are
present. Select patients can be safely sent home
on a case-by-case basis; the first dose of parenteral
antibiotics prior to discharge and mandatory
follow-up in 24 hours is warranted.
3. “Her heart rate is still 120 beats/min, but that is
just part of having a UTI. She will be fine.”
A certain percentage of patients will return, even
with sepsis, after being appropriately diagnosed
and treated. To decrease the risk of bounceback
or occult sepsis, emergency clinicians are
encouraged to resolve abnormal vital signs
before discharge. Pyrexia should be treated. If
the tachycardia is associated with dehydration,
intravenous fluids should be administered. It
should be clear to anyone reviewing the chart
that the practitioner searched for and reasonably
ruled out the presence of clinical sepsis.
4. "He has a positive urine dipstick, so my work
here is complete.”
When performing a fever workup, it can be
tempting to assume a diagnosis of UTI or pelvic
inflammatory disease in a patient with a fever
and trace or 1+ leukocytes. Particularly in the
case of a patient with high fever, abnormal vital
signs, or immunosuppression, it is important
to consider other possibilities. The emergency
clinician should also bear in mind that fever
is relatively uncommon in isolated cystitis.
Strategies to reduce risk include gathering
history and physical examination information to
rule out other causes of infection, catheterization
of the urinary bladder to obtain a more reliable
sample, and running a microscopic urinalysis to
confirm the presence of leukocytes and rule out
the presence of contamination.
2. “I don’t think about also prescribing pain and
nausea medications for home.”
Patients return to the ED for preventable and
unpreventable reasons. Unpreventable reasons
include new resistance patterns and poor
response to appropriate therapy. Preventable
reasons include use of an antibiotic with known
high resistance in the community, poor patient
compliance, and inadequate treatment of
pain and nausea. The emergency clinician can
reduce the preventable returns by reinforcing
the need to take the full course of antibiotics,
by prescribing according to local antibiotic
stewardship programs and antibiograms, and
by prescribing medications for pain and nausea
control in addition to antibiotics at discharge.
Copyright © 2014 EB Medicine. All rights reserved.
5. “I didn’t know that counted as a complicated
UTI.”
UTIs will behave differently in different patients.
It is important to consider the host patient as
well. Has the patient been recently hospitalized
or is the patient immunosuppressed? Does the
patient have diabetes mellitus? Conditions that
weaken the host should be considered.
18
www.ebmedicine.net • July 2014
cohort; 50 patients)
22. Pinson AG, Philbrick JT, Lindbeck GH, et al. Fever in the
clinical diagnosis of acute pyelonephritis. Am J Emerg Med.
1997;15(2):148-151. (Retrospective cohort; 304 patients)
23.* Fairley KF, Carson NE, Gutch RC, et al. Site of infection
in acute urinary-tract infection in general practice. Lancet.
1971;2(7725):615-618. (Prospective study; 78 patients)
24. Fihn SD. Clinical practice. Acute uncomplicated urinary tract
infection in women. N Engl J Med. 2003;349(3):259-266. (Case
report and review)
19. Widmer M, Gulmezoglu AM, Mignini L, et al. Duration of
treatment for asymptomatic bacteriuria during pregnancy.
Cochrane Database Syst Rev. 2011(12):CD000491. (Systematic
review)
20. Bent S, Nallamothu BK, Simel DL, et al. Does this woman
have an acute uncomplicated urinary tract infection? JAMA.
2002;287(20):2701-2710. (Review)
21. Donofrio JC, Weiner SG. Female patient self-diagnosis
compared with emergency physician diagnosis of urinary
tract infection. J Emerg Med. 2013;45(6):969-973. (Prospective
Risk Management Pitfalls For Urinary Tract Infection (Continued from page 18)
6. “I didn’t know appendicitis could cause pyuria.”
In the case of lower abdominal pain, the
presence of trace or 1+ leukocytes can lead
to premature closure in the evaluation of
abdominal pain. Cystitis characteristically causes
pain mostly with urination. Pyelonephritis
characteristically presents with fever and flank
pain (except in transplant patients where the
tenderness will be over the graft site) and
not with abdominal pain. When the inflamed
appendix is close to the ureter, it can cause
sterile pyuria. In patients with lower abdominal
pain and trace or 1+ leukocytes on a urine
dipstick, the diagnosis of appendicitis should
be at least considered, and it should be clearly
documented that the right lower quadrant is
nontender if no more workup is to be done.
9. “I will not let antibiotic stewardship programs
interfere with my practice.”
Antibiotic stewardship programs and local
antibiograms, when present, are a valuable
resource and represent the community
standard of care. Treating according to
a national application or booklet (which
lack local antibiogram data or antibiotic
stewardship program recommendation)
is a second-line choice. In our community,
adherence to antibiotic stewardship program
recommendations and local antibiogram data
have resulted in fewer treatment failures, fewer
complications (such as C difficile infection), and,
somewhat surprisingly, overall diminished
resistance pattern across the board. In our
institutions, practitioners who do not prescribe
according to antibiotic stewardship program
recommendations and do not document a
reason for exception are subject to peer review.
7. “She had lower abdominal pain and pyuria, so
I didn't think a pelvic examination was indicated.”
With pelvic inflammatory disease or tuboovarian abscess, irritation of the bladder can also
cause sterile pyuria. In women, the diagnosis
of pelvic inflammatory disease or tubo-ovarian
abscess should always be at least considered
when lower abdominal pain and mild or
minimal pyuria are present. It is recommended
to establish and document that there are no
concurrent pelvic symptoms in women with
UTI. Pelvic examination may be warranted.
10. “I just use the most broad-spectrum antibiotic,
so my treatment never fails.”
It may be tempting to use the “biggest gun,” but
it is not always best for the patient. Antibiotics
with relatively high anaerobic bactericidal
activity (such as amoxicillin clavulanate
or levofloxacin) are seldom the first-line
choice. By killing commensal organisms, they
may increase the risk of C difficile infection.
Additionally, antibiotics with extreme range but
not a lot of strength in any single area (such as
ciprofloxacin) are also considered second-line
choices, not just because of resistance patterns,
but because their weak activity against such a
broad spectrum tends not to be bactericidal but
to simply promote increased resistance across
the board. Practice environments can be unique,
and it is possible for fluoroquinolones to be firstline agents in some communities; it depends on
the local antibiogram and the local antibiotic
stewardship program recommendations.
8. “History and physical examination are of diminished value in the modern age.”
Appendicitis, tubo-ovarian abscess,
diverticulitis, nephrolithiasis, spinal epidural
abscess, and pelvic inflammatory disease can
mimic UTI. The key to picking these mimic
cases is not so much in testing as it is in careful
questioning and physical examination.
July 2014 • www.ebmedicine.net
19
Reprints: www.ebmedicine.net/empissues
25. Hooton TM. The current management strategies for community-acquired urinary tract infection. Infect Dis Clin North
Am. 2003;17(2):303-332. (Review)
26. Nguyen HB, Rivers EP, Abrahamian FM, et al. Severe sepsis
and septic shock: review of the literature and emergency
department management guidelines. Ann Emerg Med.
2006;48(1):28-54. (Review)
27. Talan DA, Krishnadasan A, Abrahamian FM, et al. Prevalence and risk factor analysis of trimethoprim-sulfamethoxazole- and fluoroquinolone-resistant Escherichia coli infection
among emergency department patients with pyelonephritis.
Clin Infect Dis. 2008;47(9):1150-1158. (Prospective case-control; 403 patients)
28. Meister L, Morley EJ, Scheer D, et al. History and physical examination plus laboratory testing for the diagnosis
of adult female urinary tract infection. Acad Emerg Med.
2013;20(7):631-645. (Systematic review)
29. Bugter-Maessen AM, Winkens RA, Grol RP, et al. Factors
predicting differences among general practitioners in test
ordering behaviour and in the response to feedback on test
requests. Fam Pract. 1996;13(3):254-258. (Interview and retrospective review; 75 subjects)
30. Nazareth I, King M. Decision making by general practitioners in diagnosis and management of lower urinary tract
symptoms in women. BMJ. 1993;306(6885):1103-1106. (Prospective cohort; 54 patients)
31. Gaspari RJ, Horst K. Emergency ultrasound and urinalysis in the evaluation of flank pain. Acad Emerg Med.
2005;12(12):1180-1184. (Prospective observational trial; 104
patients)
32. Lammers RL, Gibson S, Kovacs D, et al. Comparison of test
characteristics of urine dipstick and urinalysis at various test
cutoff points. Ann Emerg Med. 2001;38(5):505-512. (Prospective observational cohort; 343 patients)
33. Leman P. Validity of urinalysis and microscopy for detecting
urinary tract infection in the emergency department. Eur J
Emerg Med. 2002;9(2):141-147. (Prospective observational
cohort; 60 patients)
34. Walter FG, Knopp RK. Urine sampling in ambulatory
women: midstream clean-catch versus catheterization. Ann
Emerg Med. 1989;18(2):166-172. (Prospective observation
cohort; 105 patients)
35. Bent S, Saint S. The optimal use of diagnostic testing in
women with acute uncomplicated cystitis. Am J Med.
2002;113 Suppl 1A:20S-28S. (Review)
36. Berg AO, Heidrich FE, Fihn SD, et al. Establishing the cause
of genitourinary symptoms in women in a family practice.
Comparison of clinical examination and comprehensive
microbiology. JAMA. 1984;251(5):620-625. (Prospective
observational cohort; 204 patients)
37. Saint S, Scholes D, Fihn SD, et al. Am J Med. 1999;106(6):636641. (Retrospective cohort study; 3889 patients)
38.* Gupta K, Hooton TM, Naber KG, et al. International clinical
practice guidelines for the treatment of acute uncomplicated
cystitis and pyelonephritis in women: A 2010 update by the
Infectious Diseases Society of America and the European
Society for Microbiology and Infectious Diseases. Clin Infect
Dis. 2011;52(5):e103-e120. (Guideline)
39. Schultz HJ, McCaffrey LA, Keys TF, et al. Acute cystitis:
a prospective study of laboratory tests and duration of
Time- and Cost-Effective Strategies
1. The sensitivity and specificity of a urine dipstick
for the presence of leukocytes are very close to
that of a urinalysis with microanalysis, and it is
cheaper and faster. In low-risk scenarios (eg, uncomplicated lower UTI), a positive or negative
dipstick can safely be used without recourse to a
full urinalysis and microanalysis. In potentially
more complicated scenarios, if the dip is equivocal, then it may be best to add a full urinalysis
with microanalysis. Local protocols can be a
good guide when you are uncertain.
2. Blood cultures have been repeatedly demonstrated to be of little value, except in cases of
uncertain focus and in sepsis. In UTI, the emergency clinician has easy access to the body fluid
(urine) containing the causative organism in
large amounts. The authors could not find any
evidence to support routine use of blood cultures in most cases of upper or lower UTI.
3. Except in the case of emphysematous or necrotic
type pyelonephritis, UTIs are not associated
with renal failure. Chemistry testing (such as basic or complete metabolic panels) is unnecessary
for UTI unless the emergency clinician has other
reasons to suspect that there is renal dysfunction of electrolyte abnormalities or if screening
for sepsis is warranted. Blood counts are not
necessary to confirm or rule out the presence of
Copyright © 2014 EB Medicine. All rights reserved.
UTI. They are seldom necessary, though they
are useful in screening for sepsis, and high and
low WBC counts and bandemia are criteria for
sepsis .
4. Urine cultures are very useful for the individual
patient and for community surveillance of resistance patterns. We encourage their use in all
males, in complicated UTI, and in upper UTI. If
the local susceptibility patterns are known and
in uncomplicated lower UTI in females, they are
not necessary unless the treatment fails.
5. Imaging is rarely indicated in adult women
with UTI. The course of the female urethra is
straight and short, and it is seldom anatomically
abnormal. In males, imaging (such as bladder
scanning or scrotal ultrasound) may occasionally be necessary in complex or difficult cases.
For the most part, urinary retention and UTI are
treated with bladder decompression and outpatient imaging. A few scenarios warrant imaging,
including patients with signs and symptoms of
emphysematous pyelonephritis. Patients with
typical signs and symptoms of pyelonephritis
but with a paucity of leukocytes will probably
also benefit from imaging to rule out the presence of a perinephric abscess or psoas abscess
mimicking pyelonephritis.
20
www.ebmedicine.net • July 2014
40.
41.
42.*
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
therapy. Mayo Clin Proc. 1984;59(6):391-397. (Prospective
randomized controlled clinical trial; 200 patients )
Gagliotti C, Nobilio L, Moro ML. Emergence of ciprofloxacin
resistance in Escherichia coli isolates from outpatient urine
samples. Clin Microbiol Infect. 2007;13(3):328-331. (Retrospective cohort; 11,428 patients)
Abrahamian FM, Krishnadasan A, Mower WR, et al. Association of pyuria and clinical characteristics with the
presence of urinary tract infection among patients with
acute nephrolithiasis. Ann Emerg Med. 2013;62(5):526-533.
(Prospective observational case-control; 360 patients)
Naber KG, Bergman B, Bishop MC, et al. EAU guidelines for
the management of urinary and male genital tract infections.
Urinary Tract Infection (UTI) Working Group of the Health
Care Office (HCO) of the European Association of Urology
(EAU). Eur Urol. 2001;40(5):576-588. (Guideline)
MacFarlane DE. Catheter-associated urinary tract infections.
Part I: epidemiology, pathogenesis and bacteriology. West
Indian Med J. 1984;33(3):146-150. (Review)
Hurlbut TA 3rd, Littenberg B. The diagnostic accuracy of
rapid dipstick tests to predict urinary tract infection. Am J
Clin Pathol. 1991;96(5):582-588. (Systematic review)
MacMillan MC, Grimes DA. The limited usefulness of urine
and blood cultures in treating pyelonephritis in pregnancy.
Obstet Gynecol. 1991;78(5 Pt 1):745-748. (Retrospective case
control; 156 cases)
Velasco M, Martinez JA, Moreno-Martinez A, et al. Blood
cultures for women with uncomplicated acute pyelonephritis: are they necessary? Clin Infect Dis. 2003;37(8):1127-1130.
(Retrospective case-control; 583 cases)
Wing DA, Park AS, Debuque L, et al. Limited clinical utility of blood and urine cultures in the treatment of acute
pyelonephritis during pregnancy. Am J Obstet Gynecol.
2000;182(6):1437-1440. (Retrospective case-control; 391
cases)
Hsu CY, Fang HC, Chou KJ, et al. The clinical impact of bacteremia in complicated acute pyelonephritis. Am J Med Sci.
2006;332(4):175-180. (Retrospective case-control; 128 cases)
Coburn B, Morris AM, Tomlinson G, et al. Does this adult
patient with suspected bacteremia require blood cultures?
JAMA. 2012;308(5):502-511. (Meta-analysis; 35 articles)
Levine JA, Neitlich J, Verga M, et al. Ureteral calculi in
patients with flank pain: correlation of plain radiography
with unenhanced helical CT. Radiology. 1997;204(1):27-31.
(Retrospective cohort; 178 patients)
Catalano O, Nunziata A, Altei F, et al. Suspected ureteral
colic: primary helical CT versus selective helical CT after
unenhanced radiography and sonography. AJR Am J Roentgenol. 2002;178(2):379-387. (Prospective randomized 3-armed
clinical trial; 277 patients)
Fowler KA, Locken JA, Duchesne JH, et al. US for detecting
renal calculi with nonenhanced CT as a reference standard.
Radiology. 2002;222(1):109-113. (Retrospective cohort; 123
patients)
Sheafor DH, Hertzberg BS, Freed KS, et al. Nonenhanced
helical CT and US in the emergency evaluation of patients with renal colic: prospective comparison. Radiology.
2000;217(3):792-797. (Prospective cohort; 45 patients)
Tublin ME, Dodd GD 3rd, Verdile VP. Acute renal colic: diagnosis with duplex Doppler US. Radiology. 1994;193(3):697701. (Retrospective cohort; 32 patients)
Miller OF, Kane CJ. Unenhanced helical computed tomography in the evaluation of acute flank pain. Curr Opin Urol.
2000;10(2):123-129. (Review)
Boridy IC, Maklad N, Sandler CM. Suspected urolithiasis in
pregnant women: imaging algorithm and literature review.
AJR Am J Roentgenol. 1996;167(4):869-875. (Review)
Butler EL, Cox SM, Eberts EG, et al. Symptomatic nephrolithiasis complicating pregnancy. Obstet Gynecol. 2000;96(5 Pt
1):753-756. (Retrospective case-control; 57 patients)
July 2014 • www.ebmedicine.net
58. Niall O, Russell J, MacGregor R, et al. A comparison of
noncontrast computerized tomography with excretory
urography in the assessment of acute flank pain. J Urol.
1999;161(2):534-537. (Prospective observational cohort; 40
patients)
59. Yilmaz S, Sindel T, Arslan G, et al. Renal colic: comparison of
spiral CT, US and IVU in the detection of ureteral calculi. Eur
Radiol. 1998;8(2):212-217. (Prospective cohort; 112 patients)
60. Kenney PJ. CT evaluation of urinary lithiasis. Radiol Clin
North Am. 2003;41(5):979-999. (Review)
61. Masselli G, Derme M, Laghi F, et al. Imaging of stone disease
in pregnancy. Abdom Imaging. 2013;38(6):1409-1414. (Review)
62. Mandeville JA, Gnessin E, Lingeman JE. Imaging evaluation in the patient with renal stone disease. Semin Nephrol.
2011;31(3):254-258. (Review)
63. Karabacakoglu A, Karakose S, Ince O, et al. Diagnostic value
of diuretic-enhanced excretory MR urography in patients
with obstructive uropathy. Eur J Radiol. 2004;52(3):320-327.
(Prospective comparative study; 45 patients)
64. Blandino A, Minutoli F, Scribano E, et al. Combined
magnetic resonance urography and targeted helical CT in
patients with renal colic: a new approach to reduce delivered
dose. J Magn Reson Imaging. 2004;20(2):264-271. (Prospective
comparative study; 51 patients)
65. Mullins JK, Semins MJ, Hyams ES, et al. Half Fourier singleshot turbo spin-echo magnetic resonance urography for the
evaluation of suspected renal colic in pregnancy. Urology.
2012;79(6):1252-1255. (Prospective; 9 patients)
66. Henderson SO, Hoffner RJ, Aragona JL, et al. Bedside emergency department ultrasonography plus radiography of the
kidneys, ureters, and bladder vs intravenous pyelography in
the evaluation of suspected ureteral colic. Acad Emerg Med.
1998;5(7):666-671. (Prospective; 108 patients)
67. Kartal M, Eray O, Erdogru T, et al. Prospective validation
of a current algorithm including bedside US performed by
emergency physicians for patients with acute flank pain
suspected for renal colic. Emerg Med J. 2006;23(5):341-344.
(Prospective cohort; 227 patients)
68. Rosen CL, Brown DF, Sagarin MJ, et al. Ultrasonography by
emergency physicians in patients with suspected ureteral
colic. J Emerg Med. 1998;16(6):865-870. (Prospective cohort;
126 patients)
69. Homma Y, Gotoh M, Yokoyama O, et al. Outline of JUA
clinical guidelines for benign prostatic hyperplasia. Int J
Urol. 2011;18(11):741-756. (Guidelines)
70. Grossfeld GD, Coakley FV. Benign prostatic hyperplasia:
clinical overview and value of diagnostic imaging. Radiol
Clin North Am. 2000;38(1):31-47. (Review)
71. Dalrymple NC, Verga M, Anderson KR, et al. The value
of unenhanced helical computerized tomography in the
management of acute flank pain. J Urol. 1998;159(3):735-740.
(Prospective cohort; 417 patients)
72. Jindal G, Ramchandani P. Acute flank pain secondary to
urolithiasis: radiologic evaluation and alternate diagnoses.
Radiol Clin North Am. 2007;45(3):395-410. (Review)
73. Miller OF, Rineer SK, Reichard SR, et al. Prospective
comparison of unenhanced spiral computed tomography
and intravenous urogram in the evaluation of acute flank
pain. Urology. 1998;52(6):982-987. (Prospective cohort; 106
patients)
74. Hamm M, Knopfle E, Wartenberg S, et al. Low-dose unenhanced helical computerized tomography for the evaluation
of acute flank pain. J Urol. 2002;167(4):1687-1691. (Prospective; 109 patients)
75. Middleton WD, Dodds WJ, Lawson TL, et al. Renal calculi:
sensitivity for detection with US. Radiology. 1988;167(1):239244. (Prospective cohort; 100 patients)
76. Shen Y, Brown MA. Renal imaging in pyelonephritis.
Nephrology (Carlton). 2004;9(1):22-25. (Retrospective casecontrol; 60 patients)
21
Reprints: www.ebmedicine.net/empissues
tract infection. Nurs Times. 2006;102(36):25-26. (SIGN guidelines review)
98. Schnarr J, Smaill F. Asymptomatic bacteriuria and symptomatic urinary tract infections in pregnancy. Eur J Clin Invest.
2008;38 Suppl 2:50-57. (Review)
99. Chandel LR, Kanga A, Thakur K, et al. Prevalance of pregnancy associated asymptomatic bacteriuria: a study done in
a tertiary care hospital. J Obstet Gynaecol India. 2012;62(5):511514. (Prospective cohort; 463 patients)
100. Jain V, Das V, Agarwal A, et al. Asymptomatic bacteriuria
& obstetric outcome following treatment in early versus
late pregnancy in north Indian women. Indian J Med Res.
2013;137(4):753-758. (Prospective cohort; 109 patients)
101. Vazquez JC, Abalos E. Treatments for symptomatic urinary
tract infections during pregnancy. Cochrane Database Syst
Rev. 2011(1):CD002256. (Systematic review)
102. Wing DA, Fassett MJ, Getahun D. Acute pyelonephritis in
pregnancy: an 18-year retrospective analysis. Am J Obstet
Gynecol. 2014;210(3):219 e211-216. (Retrospective cohort;
546,092 cases)
103. Scottish Intercollegiate Guidelines Netowrk (SIGN). Management of suspected bacterial urinary tract infection in
adults. (SIGN publication no. 88.) Edinburgh: SIGN; 2012.
(Guideline)
104. Siddiq DM, Darouiche RO. New strategies to prevent
catheter-associated urinary tract infections. Nat Rev Urol.
2012;9(6):305-314. (Review)
105. Maki DG, Tambyah PA. Engineering out the risk for infection with urinary catheters. Emerg Infect Dis. 2001;7(2):342347. (Review)
106. Saint S, Lipsky BA, Goold SD. Indwelling urinary catheters:
a one-point restraint? Ann Intern Med. 2002;137(2):125-127.
(Editorial)
107. Hooton TM, Bradley SF, Cardenas DD, et al. Diagnosis,
prevention, and treatment of catheter-associated urinary
tract infection in adults: 2009 International Clinical Practice
Guidelines from the Infectious Diseases Society of America.
Clin Infect Dis. 2010;50(5):625-663. (Guideline)
108. Dobardzic AM, Dobardzic R. Epidemiological features of
complicated UTI in a district hospital of Kuwait. Eur J Epidemiol. 1997;13(4):465-470. (Retrospective case-control; 225
patients)
109. Mariappan P, Loong CW. Midstream urine culture and
sensitivity test is a poor predictor of infected urine proximal to the obstructing ureteral stone or infected stones: a
prospective clinical study. J Urol. 2004;171(6 Pt 1):2142-2145.
(Prospective cohort; 73 patients)
110. Nicolle LE, AMMI Canada Guidelines Committee. Complicated urinary tract infection in adults. Can J Infect Dis Med
Microbiol. 2005;16(6):349-360. (Guideline)
111. Joshi N, Caputo GM, Weitekamp MR, et al. Infections in patients with diabetes mellitus. N Engl J Med.
1999;341(25):1906-1912. (Review)
112. Sachs J, Geer T, Noell P, et al. Effect of renal function on urinary recovery of orally administered nitrofurantoin. N Engl J
Med. 1968;278(19):1032-1035. (Laboratory study)
113. Lundstedt AC, Leijonhufvud I, Ragnarsdottir B, et al. Inherited susceptibility to acute pyelonephritis: a family study
of urinary tract infection. J Infect Dis. 2007;195(8):1227-1234.
(Retrospective case-control; 150 patients)
114.*Antibiotic stewardship programs curb resistance. Healthcare
Benchmarks Qual Improv. 2008;15(11):114-115. (Review)
115. Gerber JS, Prasad PA, Fiks AG, et al. Effect of an outpatient
antimicrobial stewardship intervention on broad-spectrum
antibiotic prescribing by primary care pediatricians: a randomized trial. JAMA. 2013;309(22):2345-2352. (Prospective
cluster-randomized trial; 864 cases)
116. Talpaert MJ, Gopal Rao G, Cooper BS, et al. Impact of
guidelines and enhanced antibiotic stewardship on reducing
broad-spectrum antibiotic usage and its effect on incidence
77. Bouchillon S, Hoban DJ, Badal R, et al. Fluoroquinolone
resistance among gram-negative urinary tract pathogens:
global smart program results, 2009-2010. Open Microbiol J.
2012;6:74-78. (Laboratory research)
78. Omigie O, Okoror L, Umolu P, et al. Increasing resistance to
quinolones: A four-year prospective study of urinary tract
infection pathogens. Int J Gen Med. 2009;2:171-175. (Laboratory research)
79. Gupta K. Emerging antibiotic resistance in urinary tract
pathogens. Infect Dis Clin North Am. 2003;17(2):243-259.
(Review)
80. Mazzulli T. Resistance trends in urinary tract pathogens and
impact on management. J Urol. 2002;168(4 Pt 2):1720-1722.
(Review)
81. Catal F, Bavbek N, Bayrak O, et al. Antimicrobial resistance
patterns of urinary tract pathogens and rationale for empirical therapy in Turkish children for the years 2000-2006. Int
Urol Nephrol. 2009;41(4):953-957. (Retrospective case-control
767 cases; 698 patients)
82. Miller LG, Tang AW. Treatment of uncomplicated urinary
tract infections in an era of increasing antimicrobial resistance. Mayo Clin Proc. 2004;79(8):1048-1053. (Review)
83. Gupta K, Hooton TM, Stamm WE. Increasing antimicrobial
resistance and the management of uncomplicated community-acquired urinary tract infections. Ann Intern Med.
2001;135(1):41-50. (Review)
84. Hulbanni A. Guidelines for the management of cystitis and
pyelonephritis in the emergency department. EM Practice
Guidelines Update. 2012;4(8):1-10. (Review)
85. Jancel T, Dudas V. Management of uncomplicated urinary
tract infections. West J Med. 2002;176(1):51-55. (Review)
86. Dielubanza EJ, Mazur DJ, Schaeffer AJ. Management of noncatheter-associated complicated urinary tract infection. Infect
Dis Clin North Am. 2014;28(1):121-134. (Review)
87. Foo LY, Lu Y, Howell AB, et al. A-Type proanthocyanidin
trimers from cranberry that inhibit adherence of uropathogenic P-fimbriated Escherichia coli. J Nat Prod. 2000;63(9):12251228. (Laboratory research)
88. Jones AE, Puskarich MA. The Surviving Sepsis Campaign
guidelines 2012: update for emergency physicians. Ann
Emerg Med. 2014;63(1):35-47. (Guideline)
89. Gold NA, Bithoney WG. Methemoglobinemia due to ingestion of, at most, three pills of Pyridium in a 2-year-old: case
report and review. J Emerg Med. 2003;25(2):143-148. (Case
report)
90. Fincher ME, Campbell HT. Methemoglobinemia and hemolytic anemia after phenazopyridine hydrochloride (Pyridium) administration in end-stage renal disease. South Med
J. 1989;82(3):372-374. (Case report)
91. Hummers-Pradier E, Ohse AM, Koch M, et al. Urinary tract
infection in men. Int J Clin Pharmacol Ther. 2004;42(7):360-366.
(Prospective cross-sectional survey; 90 patients)
92. Trautner BW. New perspectives on urinary tract infection in
men. JAMA Intern Med. 2013;173(1):68-70. (Review)
93. Ulleryd P, Zackrisson B, Aus G, et al. Prostatic involvement
in men with febrile urinary tract infection as measured by
serum prostate-specific antigen and transrectal ultrasonography. BJU Int. 1999;84(4):470-474. (Prospective case-control;
70 patients)
94. Brede CM, Shoskes DA. The etiology and management of
acute prostatitis. Nat Rev Urol. 2011;8(4):207-212. (Review)
95. Singh K, Kumar S, Villareal R, et al. Urinary Tract Infection.
In: Lerma EV, Berns JS, Nissenson AR, eds. Current Diagnosis & Treatment: Nephrology & Hypertension. New York: The
McGraw-Hill Companies, Inc. 2009:329-336. (Textbook)
96. Wing DA, Hendershott CM, Debuque L, et al. Outpatient
treatment of acute pyelonephritis in pregnancy after 24
weeks. Obstet Gynecol. 1999;94(5 Pt 1):683-688. (Prospective,
randomized trial; 92 patients)
97. Beckford-Ball J. Management of suspected bacterial urinary
Copyright © 2014 EB Medicine. All rights reserved.
22
www.ebmedicine.net • July 2014
1. What is the most common causative organism
for uncomplicated UTI?
a. Klebsiella marcesens
b. Enterobacter faecalis
c. Proteus mirabilis
d. Escherichia coli
of Clostridium difficile infection. J Antimicrob Chemother.
2011;66(9):2168-2174. (Retrospective case-control; 349 cases)
117. Danaher PJ, Milazzo NA, Kerr KJ, et al. The antibiotic support team--a successful educational approach to antibiotic
stewardship. Mil Med. 2009;174(2):201-205. (Prospective
cohort; 52 patients)
118. Hecker MT, Fox CJ, Son AH, et al. Effect of a stewardship
intervention on adherence to uncomplicated cystitis and
pyelonephritis guidelines in an emergency department setting. PLoS One. 2014;9(2):e87899. (Retrospective cohort; 52
patients)
119. Reddick B, Howe K. The impact of pneumonia guidelines
and core measures on patient-oriented outcomes. N C Med J.
2013;74(5):434-437. (Editorial)
120. Tipler PS, Pamplin J, Mysliwiec V, et al. Use of a protocolized approach to the management of sepsis can improve
time to first dose of antibiotics. J Crit Care. 2013;28(2):148-151.
(Retrospective cohort; 209 patients)
121. Doganis D, Siafas K, Mavrikou M, et al. Does early treatment
of urinary tract infection prevent renal damage? Pediatrics.
2007;120(4):e922-e928. (Prospective cohort; 278 patients)
122. Elkharrat D, Chastang C, Boudiaf M, et al. Relevance in the
emergency department of a decisional algorithm for outpatient care of women with acute pyelonephritis. Eur J Emerg
Med. 1999;6(1):15-20. (Prospective cohort; 83 patients)
123. Israel RS, Lowenstein SR, Marx JA, et al. Management of
acute pyelonephritis in an emergency department observation unit. Ann Emerg Med. 1991;20(3):253-257. (Retrospective
case control; 87 patients)
124. Safrin S, Siegel D, Black D. Pyelonephritis in adult
women: inpatient versus outpatient therapy. Am J Med.
1988;85(6):793-798. (Retrospective case control)
125. Pinson AG, Philbrick JT, Lindbeck GH, et al. ED management of acute pyelonephritis in women: a cohort study. Am
J Emerg Med. 1994;12(3):271-278. (Retrospective cohort; 194
patients)
126. Sanchez M, Collvinent B, Miro O, et al. Short-term effectiveness of ceftriaxone single dose in the initial treatment of acute uncomplicated pyelonephritis in women. A
randomised controlled trial. Emerg Med J. 2002;19(1):19-22.
(Prospective randomized trial; 144 patients)
2. An 18-year-old male presents with anorexia,
lower abdominal pain, and trace leukocytes on
urine dipstick. What is your next step?
a. Nothing further needs to be done. Treat and street for cystitis.
b. Order a WBC count to establish whether appendicitis is present.
c. Consider appendicitis, and more history and physical examination is indicated.
d. Proceed straight to CT abdomen and pelvis.
3. A diabetic female patient who is chronically
noncompliant with her medications is diagnosed with a lower UTI. Which of the following
is the next best step?
a. Discharge home on the broadest spectrum antibiotic available.
b. Discharge home with antibiotic and no further consideration.
c. Consider that the diabetes may be severe or
poorly controlled and, therefore, this may be a complicated UTI and cultures may be indicated.
d. Prescribe a fluoroquinolone, as they are best class in all communities.
4. Change the sex of the patient in question 1 to
male. Which of the following now applies?
a. Cultures are indicated only because of diabetes.
b. Cultures are not indicated, because men recover quickly from UTI
c. Prescribe a fluoroquinolone, as they are best class in all communities.
d. Cultures are indicated because of the patient’s sex.
CME Questions
Take This Test Online!
Current subscribers receive CME credit absolutely free by completing the following test. Each
issue includes 4 AMA PRA Category 1 CreditsTM, 4
ACEP Category 1 credits, 4 AAFP Prescribed
Take This Test Online!
credits, and 4 AOA Category 2A or 2B credits.
Monthly online testing is now available for
current and archived issues. To receive your free
CME credits for this issue, scan the QR code
below with your smartphone or visit
www.ebmedicine.net/E0714.
July 2014 • www.ebmedicine.net
5. A patient with flank pain and an obstructing
stone has 1+ leukocytes on dip. Which of the
following is TRUE?
a. No further diagnostic maneuvers are indicated.
b. Further consideration is warranted. This may represent a UTI concurrent with an obstructing stone and possibility of failure, and development of sepsis is increased.
c. Blood has leukocytes, and when there is hematuria there is also pyuria. Even 3+ leukocytes is not worrisome.
d. Antibiotics and cultures are indicated; otherwise no further considerations or management is necessary.
23
Reprints: www.ebmedicine.net/empissues
6. Nitrofurantoin is:
a. A tertiary amine
b. Indicated for pyelonephritis
c. A good choice in lower UTI
d. An old, out-of-date drug with no indications
7. You diagnose a patient with a UTI. You
pull out your pink antibiotic pocketbook
from residency, and it gives you a
recommendation. Which of the following is
most true?
a. The recommendations in this book accurately reflect local resistance patterns and the best antibiotics to use.
b. This is best practice only when no local antibiograms or antibiotic stewardship programs for the local community exist.
c. A nationally famous person wrote it. It must be true and accurate.
d. It doesn’t matter if it is 5 years old. Susceptibility patterns don’t change that fast.
8. Your local antibiotic stewardship program
recommends nitrofurantoin as a first-line
agent for cystitis. What is the best way to
view this recommendation?
a. Antibiotic stewardship programs have been shown to be of little value.
b. It is always better to use a pocketbook with national guidelines.
c. Antibiotic stewardship programs are useful, and their recommendations bear careful consideration.
d. Only when antibiotic stewardship programs are composed by national experts do their recommendations carry weight.
Physician CME Information
Date of Original Release: July 1, 2014. Date of most recent review: June 10, 2014. Termination
date: July 1, 2017.
Accreditation: EB Medicine is accredited by the Accreditation Council for Continuing Medical
Education (ACCME) to provide continuing medical education for physicians. This activity has
been planned and implemented in accordance with the Essential Areas and Policies of the
ACCME.
Credit Designation: EB Medicine designates this enduring material for a maximum of 4 AMA PRA
Category 1 Credits™. Physicians should claim only the credit commensurate with the extent of their
participation in the activity.
ACEP Accreditation: Emergency Medicine Practice is approved by the American College of
Emergency Physicians for 48 hours of ACEP Category I credit per annual subscription.
AAFP Accreditation: This Medical Journal activity, Emergency Medicine Practice, has been
reviewed and is acceptable for up to 48 Prescribed credits by the American Academy of Family
Physicians per year. AAFP accreditation begins July 31, 2013. Term of approval is for one year
from this date. Each issue is approved for 4 Prescribed credits. Credit may be claimed for one
year from the date of each issue. Physicians should claim only the credit commensurate with the
extent of their participation in the activity.
AOA Accreditation: Emergency Medicine Practice is eligible for up to 48 American Osteopathic
Association Category 2A or 2B credit hours per year.
Needs Assessment: The need for this educational activity was determined by a survey of medical
staff, including the editorial board of this publication; review of morbidity and mortality data from
the CDC, AHA, NCHS, and ACEP; and evaluation of prior activities for emergency physicians.
Target Audience: This enduring material is designed for emergency medicine physicians,
physician assistants, nurse practitioners, and residents.
Goals: Upon completion of this article, you should be able to: (1) demonstrate medical decisionmaking based on the strongest clinical evidence; (2) cost-effectively diagnose and treat the most
critical ED presentations; and (3) describe the most common medicolegal pitfalls for each topic
covered.
Objectives: Upon completion of this article, you should be able to: (1) differentiate the
classification of UTI as upper and lower, and complicated versus uncomplicated; (2)
describe the causative organisms for UTI and the best antibiotics to use for upper and
lower UTI, given local antibiogram data; and (3) recognize the value of local antibiograms
and antibiotic stewardship programs.
Discussion of Investigational Information: As part of the newsletter, faculty may be presenting
investigational information about pharmaceutical products that is outside Food and Drug
Administration-approved labeling. Information presented as part of this activity is intended
solely as continuing medical education and is not intended to promote off-label use of any
pharmaceutical product.
Faculty Disclosure: It is the policy of EB Medicine to ensure objectivity, balance, independence,
transparency, and scientific rigor in all CME-sponsored educational activities. All faculty
participating in the planning or implementation of a sponsored activity are expected to disclose
to the audience any relevant financial relationships and to assist in resolving any conflict
of interest that may arise from the relationship. In compliance with all ACCME Essentials,
Standards, and Guidelines, all faculty for this CME activity were asked to complete a full
disclosure statement. The information received is as follows: Dr. Best, Dr. Ou, Dr. Kitlowski,
Dr. Bedolla, Dr. Grossman, Dr. Lazarciuc, Dr. Jagoda, Dr. Damilini, and their related parties
report no significant financial interest or other relationship with the manufacturer(s) of any
commercial product(s) discussed in this educational presentation.
Commercial Support: This issue of Emergency Medicine Practice did not receive any commercial
support.
Method of Participation:
•Print Semester Program: Paid subscribers who read all CME articles during each Emergency
Medicine Practice 6-month testing period, complete the CME Answer and Evaluation Form
distributed with the June and December issues, and return it according to the published
instructions are eligible for up to 4 hours of CME credit for each issue.
•Online Single-Issue Program: Current, paid subscribers who read this Emergency Medicine
Practice CME article and complete the test and evaluation at www.ebmedicine.net/CME are
eligible for up to 4 hours of Category 1 credit toward the AMA Physician’s Recognition Award
(PRA). Hints will be provided for each missed question, and participants must score 100% to
receive credit.
Hardware/Software Requirements: You will need a Macintosh or PC to access the online archived
articles and CME testing.
Additional Policies: For additional policies, including our statement of conflict of interest, source
of funding, statement of informed consent, and statement of human and animal rights, visit http://
www.ebmedicine.net/policies.
CEO & Publisher: Stephanie Williford Director of Editorial: Dorothy Whisenhunt Content Editors: Erica Carver, Jenique Meekins Editorial Projects Manager: Kay LeGree
Director of Member Services: Liz Alvarez Office Manager: Kiana Collier Member Services Representative: Paige Banks
Director of Marketing: Robin Williford Marketing Communications Specialist: Aron Dunn Marketing Coordinator: Katherine Johnson
Subscription Information:
Direct all questions to:
EB Medicine
Phone: 1-800-249-5770 or 1-678-366-7933
Fax: 1-770-500-1316
5550 Triangle Parkway, Suite 150
Norcross, GA 30092
E-mail: ebm@ebmedicine.net
Website: www.ebmedicine.net
To write a letter to the editor, please email:
jagodamd@ebmedicine.net
12 monthly evidence-based print issues; 48 AMA PRA Category
1 CreditsTM, 48 ACEP Category 1 credits,
48 AAFP Prescribed credits, and 48 AOA Category 2A or 2B
CME credits; and full online access to searchable archives
and additional CME: $329 Individual issues,
including 4 CME credits: $30
(Call 1-800-249-5770 or go to
http://www.ebmedicine.net/EMP issues to order)
Emergency Medicine Practice (ISSN Print: 1524-1971, ISSN Online: 1559-3908, ACID-FREE) is published monthly (12 times per year) by EB Medicine (5550 Triangle Parkway, Suite 150,
Norcross, GA 30092). Opinions expressed are not necessarily those of this publication. Mention of products or services does not constitute endorsement. This publication is intended as
a general guide and is intended to supplement, rather than substitute, professional judgment. It covers a highly technical and complex subject and should not be used for making specific
medical decisions. The materials contained herein are not intended to establish policy, procedure, or standard of care. Emergency Medicine Practice is a trademark of EB Medicine. Copyright
© 2014 EB Medicine. All rights reserved. No part of this publication may be reproduced in any format without written consent of EB Medicine. This publication is intended for the use of the
individual subscriber only and may not be copied in whole or part or redistributed in any way without the publisher’s prior written permission — including reproduction for educational purposes
or for internal distribution within a hospital, library, group practice, or other entity.
Copyright © 2014 EB Medicine. All rights reserved.
24
www.ebmedicine.net • July 2014