Testing the Immunity of Active Implantable Medical Devices to CW
advertisement

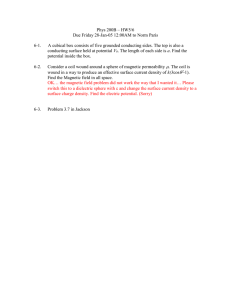
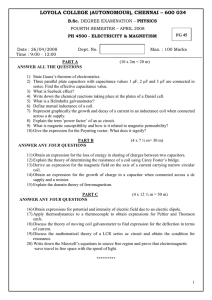
IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 54, NO. 9, SEPTEMBER 2007 1679 Testing the Immunity of Active Implantable Medical Devices to CW Magnetic Fields up to 1 MHz by an Immersion Method Valentin Buzduga3 , Member, IEEE, Donald M. Witters, Senior Member, IEEE, Jon P. Casamento, Member, IEEE, and Wolfgang Kainz, Member, IEEE Abstract—This paper presents a magnetic-field system and the method developed for testing the immunity of the active implantable medical devices to continuous-wave magnetic fields in the frequency range up to 1 MHz. The system is able to produce magnetic fields of 150 A/m for frequencies up to 100 kHz and strengths decreasing as 1/f between 100 kHz and 1 MHz, with uniformity of the field within 2.5% in the volume for tests. To simulate human tissue, the medical device, together with its leads, is placed on a plastic grid in a saline tank that is introduced in the magnetic field of the induction coil. This paper offers an alternative for the injection voltage methods provided in the actual standards for assessing the protection of the implantable medical devices from the effects of the magnetic fields up to 1 MHz. This paper presents the equipment and signals used, the test procedure, and results from the preliminary tests performed at the Food and Drug Administration–Center for Devices and Radiological Health on implantable pacemakers and neurostimulators. The new system and test method are useful for the EMC research on the implantable medical devices. Index Terms—Electromagnetic compatibility (EMC), electromagnetic interference (EMI), implantable biomedical devices, magnetic fields, pacemakers. I. INTRODUCTION BRIEF survey on the applicable standards shows that the active implantable medical devices (AIMDs) have to comply with certain requirements for protection from the effects of the continuous-wave (CW) magnetic fields. For example, the following requirements are listed from the AIMD standards PC69 [1], EN45502-2-1 [2], and ISO14708-1 [3]: 1) protection from persisting malfunction due to CW sources (PC69, clause 4.3.1). A Manuscript received August 28, 2006; revised January 5, 2007. This paper was supported in part by an appointment to the Research Fellowship Program for the Center for Devices and Radiological Health administered by the Oak Ridge Associated Universities through a contract with the U.S. Food and Drug Administration. The opinions and conclusions stated in this paper are those of the author(s) and do not represent the official position of the Department of Health and Human Services. The mention of commercial products, their sources, or their use in connection with material reported herein is not to be construed as either an actual or implied endorsement of such products by the Department of Health and Human Services. Asterisk indicates corresponding author. V. Buzduga is with Scantek, Inc., Columbia, MD 21046 USA. He is also with Capitol College, Laurel, MD 20708 USA (e-mail: buzdugav@yahoo.com). D. M. Witters, J. P. Casamento, and W. Kainz are with the Food and Drug Administration, Center for Devices and Radiological Health, Rockville, MD 20852 USA (e-mail: donald.witters@fda.hhs.gov; jon.casamento@fda.hhs.gov; wolfgang.kainz@fda.hhs.gov). Digital Object Identifier 10.1109/TBME.2007.893502 2) temporary response to CW sources (PC69 clause 4.4.1). 3) protection from sensing modulated electromagnetic fields as cardiac signals (PC69, clauses 4.5.1.1 and 4.5.2.1). 4) protection from ac magnetic field exposure in the range 1 to 140 kHz (PC69, clause 4.8.1). 5) protection from electromagnetic nonionizing radiation (ISO14708-1, clause 27). Compliance with requirements 1) and 4) is confirmed if after application of the test signal, the AIMD functions prior to the test without further adjustment. For protection 2), the AIMD should operate during the test in its set mode or in the interference mode as described by the manufacturer. The compliance with requirement 3) is confirmed if the AIMD functions in its set mode at all times irrespective of the application of the test signal, while the test method for protection 5) is under development. An important issue for standard methodology is the electromagnetic stress applied to AIMD during these tests. The test signal is not always the magnetic field, though the goal of the tests is assessing the behavior of the medical device in the case of exposure to magnetic fields. For protections 1), 2), and 3), the test signal is the voltage which is applied to the AIMD leads in order to simulate the effect of time-varying magnetic fields on device circuitry. Annex M in PC 69 gives the correlation between the voltage levels used in the standard tests and the radiated field strengths. For protections 4) and 5), the standards recommend tests with magnetic fields. The test level for protection 4) is 150 A/m (rms) up to 100 kHz and strengths decreasing from 100 kHz to 140 kHz. The recommended test equipas ment is formed from a generator and a radiating coil with a dicm and exceeding the largest linear dimension ameter of of the AIMD by 50%. The calculations show nonuniformity in this case up to 30% for the testing field in the volume corresponding to the AIMD can. For protection 5), ISO14708-1 does not give the test equipment but recommends as a first guide, test levels of 150 A/m (rms) up to 100 kHz and test levels decreasing between 100 kHz and 30 MHz. as In connection with the standards listed before, this paper presents a system that is capable of producing magnetic fields of 150 A/m up to 100 kHz and strengths decreasing as between 100 kHz and 1 MHz, with uniformity of % in adequate volume for testing AIMD together with their leads. This paper describes the system prototyped at FDA–CDRH and the methods used for testing the immunity of the implantable pacemakers and neurostimulators to CW magnetic fields. The new test method offers the possibility to characterize the protection 0018-9294/$25.00 © 2007 IEEE 1680 IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 54, NO. 9, SEPTEMBER 2007 Fig. 1. Block diagram of the magnetic-field test system. of these medical devices from the effects of the magnetic fields by means of immunity diagrams in the frequency domain. This paper presents interference signals caused by CW magnetic fields, AIMD immunity characteristics obtained with the new test method, and points out the usefulness of the new test system and method for AIMD research and standard development. Fig. 2. Induction coil C28. II. MAGNETIC-FIELD TEST SYSTEM Fig. 1 shows the block diagram of the magnetic-field test system prototyped at FDA–CDRH. The system was designed to produce the magnetic-field test levels recommended in clause 27 of ISO14708-1 for the frequency range up to 1 MHz, namely between 150 A/m up to 100 kHz and levels decreasing as 100 kHz and 1 MHz [4]. The system is formed of: • the CW signal generator model HP 33120A; • the power-amplifier model 1000A (DC to 1 MHz) manufactured by Industrial Test Equipment Co. Inc. (ITE); • the induction coil model C28 prototyped at FDA-CDRH (nonstandard Helmholtz coil). For producing the magnetic fields for tests, the CW signal generator drives the power amplifier whose load is the induction coil. The magnetic field for tests can be adjusted for frequency and strength in the specified limits by means of the frequency and amplitude controls of the signal generator. The specifications of the signal generator and power amplifier used in this system can be found on the manufacturers’ websites and in user manuals. Next, we present the characteristics of the induction coil prototyped for this application, brief feasibility calculations for the test system, and the methods used for measuring the magnetic field in the induction coil during tests. • inductance: 1.26 H. . • resistance: . • impedance at 100 kHz: • coil constant: . In the cylindrical volume for tests located at the center of the induction coil C28, the uniformity of the magnetic field is within %. Fig. 3 presents the uniformity of the axial component of the magnetic field H in the midplane (0 cm) and in the two planes cm). The which limit the cylindrical volume for tests (at reference for these diagrams is the magnetic field at the center of the coil C28. The magnetic-field vector magnitude differs from the axial component by less than 0.1% in the cylindrical volume for tests. In a sphere of 9-cm diameter, concentrically placed in coil C28, the magnetic-field uniformity is within % with respect to the center value. A. Induction Coil Model C28 B. Feasibility Calculations PC69 shows that, at implantation, the AIMD leads form effective loop areas between 191 cm and 232 cm (average values). Therefore, the induction coil was conceived to produce the magnetic field of 150 A/m at 100 kHz in a cylinder of diameter 17 cm (circular area 227 cm ) and height 3 cm when the coil is supplied by the ITE amplifier model 1000 A. The coil was also designed to produce a uniform magnetic field in a sphere of 9-cm diameter for testing the implantable insulin infusion pumps whose largest linear dimension is about 8 cm. These desiderata were achieved with the nonstandard Helmholtz coil model C 28 shown in Fig. 2, which has the following specifications: • two single-turn circular loops, series connection; • material: copper pipe, diameter 1.6 cm; • diameter of the loops: 28 cm; • distance between loops: 12 cm. The frame of the coil system is made of plexiglass. The deviation of the two loops from cylindrical geometry is less than 1 mm. The induction coil model C28 has the following functional parameters. The equations used in this paper for calculating the magnetic fields produced by circular loops can be found in the IEEE Standard P1309 [5]. Extended equations for inductance calculations are given in [6]. The calculations presented next reveal the optimum match of the induction coil C28 with the ratings of the kHz. The ITE amplifier model power amplifier for 1000 A is compatible with the inductive loads and has output ratings 25 V/40 A (rms values) up to 1 MHz. For limiting the dc offset current of the amplifier on the low-impedance loads, the manufacturer recommends mounting a series resistor in the circuit of the load so that it drops 1 to 2 V (rms) at the full current. For a maximum current of 30 A in this test arrangement, W, type MP9000 (noninwe chose a film resistor of ductive), mounted on a heat sink. In these conditions, the load of the amplifier is formed of the induction coil C28 in series with resistor. The impedance the connecting leads and the of this load is given by the equation Fig. 3. Coil C28: the deviation of the magnetic-field strength with respect to the center value. (1) BUZDUGA et al.: TESTING THE IMMUNITY OF ACTIVE IMPLANTABLE MEDICAL DEVICES 1681 To keep the load impedance at low values, the connecting leads are made of close pairwires or just coaxial cables with the lowest possible length. For the induction coil C28, the load impedance . On this load, the ampli(1) at 100 kHz is fier delivers the maximum current given by the equation (2) Fig. 4. Available field in the test system with coil C28. The magnetic field at the center of the coil system is given by the following equation: (3) In (3), is the number of turns, is the current through the series loops, is the radius of the loops, and is the distance from the center of the coil system to the center of each loop. cm and cm, For A/m (rms), (3) produces the magnetic-field strength which shows a testing reserve of 6% above 150 A/m at 100 kHz. Below 100 kHz, the amplifier can deliver higher currents within the rating of 40 A, provided by the lower value of the load impedance expressed in (1). Consequently, the system presents higher reserve for the magnetic-field strength at low frequenkHz, the load impedance given in (1) is mostly cies. For reactive and the maximum current through the induction coil C28 may be calculated with (4) (4) The inductances and do not change significantly up to 1 MHz, so that the current given in (4) and implicitly the magbetween netic field for tests in coil C28 can be decreased as 100 kHz and 1 MHz, provided that the maximum output voltage of the amplifier is 25 V (rms) in this frequency range. Equation (3) can be rewritten in the form which defines the constant of the coil (5) For cm and the induction coil model C28 cm, (5) gives the constant of (6) In practice, the current through coil is measured and used to calculate the magnetic-field strength at the center of the coil C28 with the following equation: (7) The measurements confirmed the above feasibility calculations. Fig. 4 presents the magnetic-field strength measured at the center of the induction coil C28 in the frequency range 1 kHz to 1 MHz. With respect to the test levels recommended in clause 27 of ISO14708-1, the system prototyped at FDA–CDRH provides testing reserve greater than 10% up to 90 kHz and reserve within few percents for frequencies between 100 kHz and 1 MHz. C. Measuring the Magnetic Field in the Induction Coil The immunity tests require measuring the magnetic-field strength in the induction coil. The coil should be calibrated and geometrically stable. Standard P1309 gives a guide for calibrating Helmholtz coils and those methods can be extended for the nonstandard Helmholtz coils. The following methods give accurate data on the magneticfield strength in the induction coil. • Measuring the current through coil and computing the magnetic-field strength with (7) or other field calculators. • Measuring the field with magnetic-field probes. At FDA–CDRH, we used triaxial magnetic-field sensors manufactured by Electric Research and Management Co. Inc. (ERM). A method for monitoring the magnetic field during tests is to measure the current through the induction coil and computing the field strength in the volume for tests. Another method is to correlate the field in the volume for tests with the field value at another location and measuring the field strength at that location with magnetic sensors. For example, 139 A/m measured at the center of the top loop confirms 150 A/m at the center of the induction coil C28. Alternatively, a small circular loop may be used as a probe for CW magnetic fields. From and , the following equation is deduced, which gives the strength of the magnetic field as a function of frequency and the maximum voltage induced in a loop of diameter : All quantities in SI base units (8) At FDA–CDRH, we used all of these methods for measuring the magnetic-field strength during tests. The close data from multiple measurements with different probes confirm the performance of the new system. For quick estimation of the test level, the magnetic-field strength measured with ERM sensors at the center of the induction coil can be correlated with the output voltage level of the CW signal generator. This correlation permits evaluating the field strength in the volume for tests by reading the output voltage of the signal generator. Though the amplifier used in this application is not a voltage-controlled cur- 1682 IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 54, NO. 9, SEPTEMBER 2007 rent source and any change in the load impedance could produce deviations in a voltage–magnetic-field relationship. Therefore, the magnetic-field data for the AIMD immunity characteristics were collected with magnetic-field sensors. III. TESTING AIMD IN CW MAGNETIC FIELDS UP TO 1 MHZ The system that was just presented offers the possibility to investigate the immunity of AIMD to magnetic fields by immersing the device together with its leads into the testing field. A tissue simulator containing the AIMD is placed in the induction coil so that the medical device and its leads are positioned in the volume for tests. The AIMD is exposed to magnetic fields of different strengths and frequencies, while an oscilloscope monitors the signals delivered by the device under test in a tissue simulator. We next describe the tissue simulator and AIMD preparation for tests, the electromagnetic-interference (EMI) criteria used in the preliminary tests on pacemakers and neurostimulators, and the procedure developed at FDA–CDRH for testing the immunity of these implantable medical devices to CW magnetic fields. Fig. 5. AIMD on plastic grid. A. Tissue Simulator and AIMD Preparation for Tests The tissue simulator developed for this test system consists of a cylindrical plastic tank filled with saline solution of 0.18% concentration. A tissue simulator with other geometry developed at FDA–CDRH is described in PC69. The saline tank has an outside diameter 25 cm and height of about 23 cm for fitting the dimensions of the induction coil C28. A horizontal line marked on the saline tank shows the midplane of the cylindrical volume for tests at a normal position of the tank in coil C28. Thus, the AIMD of about 1-cm thickness can be properly positioned by visual inspection in the volume for tests of 3-cm height. A plastic grid, which fits the inner diameter of the cylindrical tank, supports the AIMD together with its leads as shown in Fig. 5. Four plastic legs that have threaded nuts permit adjustment of the vertical position of the plastic grid in the saline tank. The leads of AIMD are positioned on a circular contour of 17-cm diameter, which delimits an area of about 227 cm . For repeatable results, this area should be kept constant during tests. Therefore, we grooved a circular channel for leads and a shape for the can of the device on the plastic grid. The AIMD and its leads are fixed on the grid with thread and plastic ties. The plastic grid also fixes the sensing cable (pairwire or coaxial) which picks up the signal delivered by AIMD from saline. The ends of the sensing wires have the insulation removed on about 1 mm and are positioned a few centimeters from the tip of the AIMD leads. For testing the AIMD with a simulated heart signal, a similar cable may be used to inject the electrocardiographic signal in saline. The induction coil and the saline tank should be placed on a wooden or plastic table to avoid distortion of the testing magnetic field. The AIMD is configured for the required operation mode, the grid is introduced in the saline tank, and the threaded legs are turned for adjusting the position of AIMD in the volume for tests. Fig. 6 shows the tissue simulator introduced in the induction coil C28. The effective area bounded by the leads of the AIMD may be increased in this test arrangement by extending the length of the Fig. 6. Tissue simulator in coil C28. leads and turning more than one loop on the circular contour of 227 cm . This technique may be used for testing neurostimulators whose leads form effective loop areas that are larger than 227 cm at implantation. In such cases, the exposure area on the circular contour is calculated as the sum of an integer of loops of 227 cm and the area of a circular number segment defined by the tip of the lead and the can of AIMD (9) The area of the circular segment results from (10), wherein is the radius of the circular contour in centimeters and is the length of the arc in centimeters (the length of the lead wrapped up in excess over the integer number of turns) (10) B. EMI Criteria for Medical Devices The tests performed at FDA–CDRH revealed the degradation of the signals delivered by AIMD in saline at different frequencies and strengths of the magnetic field. For assessing the immunity level of the AIMD, it is necessary to adopt reference signals for normal operation of devices and to define EMI criteria for correlating the AIMD signal degradation with the parameters of the magnetic field. The reference signal for normal operation of an AIMD is the signal delivered by the device in a tissue simulator at zero testing level. The EMI is the degradation of the AIMD signal over certain limits due to the testing field, for example: For pacemakers: • Criterion 1: deviations greater than 20% for the AV (atrioventricular) interval. BUZDUGA et al.: TESTING THE IMMUNITY OF ACTIVE IMPLANTABLE MEDICAL DEVICES • Criterion 2: deviations greater than 10% for the pulse interval. • Criterion 3: decrease of the atrial (A) or ventricular (V) pulse amplitude below 50%. For neurostimulators: • decrease of the pulse amplitude below 50%. The EMI criteria just shown were drawn from typical signal degradations exhibited by AIMD samples during the preliminary tests. These criteria were chosen as a convenient means to describe the immunity tests for AIMD by using the new system and do not suggest performance levels to be adopted for pacemakers or neurostimulators although the EMI criterion 2 for pacemakers is derived from the performance criteria given in PC69 for the tests between 450 and 3000 MHz. C. Test Procedure The preliminary tests on AIMD in the new magnetic-field system were performed at FDA–CDRH in laboratory conditions by using the procedure described next. The test equipment should be connected as shown in Fig. 1, the induction coil being seated on a wooden table. The medical device is prepared for tests, the tissue simulator is introduced in the induction coil, and the height of the plastic grid is adjusted for positioning the AIMD in the volume for tests as described before. A multichannel memory oscilloscope displays the AIMD reference signal on a memory channel while the signal picked up from saline is continuously displayed on a measuring channel. For signal analysis, it is useful to display a sequence of six to ten pulses delivered by AIMD in saline. The same oscilloscope may be used for measuring the field strength with magnetic-field sensors during tests. For accurate results, the relative position of the coil, saline tank, and plastic grid arrangement should be kept unchanged during tests after setting the reference signal. The power amplifier feeds the induction coil and the testing magnetic field is adjusted for frequency and strength from the controls of the signal generator. The noise of test frequency, which is superposed to the AIMD signal in the tissue simulator, can be attenuated by using filtering techniques on the measuring channel. For the tests described in this paper, we used continuous sinusoidal signals at fixed frequencies between 1 kHz and 1 MHz, at least four distinct frequencies per decade. For finding the immunity level of an AIMD to CW magnetic fields at a given frequency, the strength of the testing field at that frequency is increased from zero and the signal picked up from saline is continuously compared with the reference signal on the oscilloscope. As long as the AIMD signals picked up from saline do not deviate over the limits assumed in the EMI criteria, we count the immunity of the device to the applied test level. The highest magnetic-field strength at which the interference does not yet occur gives the immunity level of the AIMD to CW magnetic fields at that frequency. Generally, we increased the field strength with coarse steps of up to 20 A/m and refined the magnetic-field steps when investigating the interference phenomena. If the AIMD did not exhibit interference, we tested the immunity up to the maximum available field strength in the test system. For each testing frequency, we noted the immunity level found 1683 in measurements (A/m, rms values) and recorded for database the reference signal and the signal picked up from saline when the AIMD was exposed to the magnetic field at the immunity level. At certain frequencies and test levels, the AIMD pulses picked up from saline may deviate over the limits chosen in the EMI criteria. In such cases, the relation between the AIMD signal degradation and the magnetic-field strength is investigated through multiple measurements by increasing and decreasing the field strength with refined steps. The susceptibility is the lack of immunity, and the susceptibility level of the AIMD at a given frequency may be defined as the lowest test level at which the interference occurs. In the tests which revealed interference, we noted details on EMI at test levels within 5% to 20% above the immunity level of AIMD. Between the immunity level and the test level, which produced persistent EMI, an interval of uncertain operation (intermittent interference) was generally found for AIMD. For each testing frequency, we noted the susceptibility level found in measurements and recorded for database the reference signal and the signal picked up from saline when the AIMD was exposed to the magnetic field at the susceptibility level. When EMI at a given frequency was found, we examined the behavior of the AIMD up to the test level recommended in ISO14708-1. Two devices returned to normal operation at field strengths above the susceptibility level, as shown in the diagram in Fig. 9. PC69 and other standards recommend measurements with continuous sinusoidal signals either swept over the frequency range, or applied at four distinct frequencies per decade. As known from the measurements practice, the swept signals are suitable for conformity tests, when the device which does not comply with requirements is rejected. Obviously, if one finds EMI with swept signals and wants to investigate the phenomena, they have to stop the frequency sweeping and continue the tests at fixed frequencies to obtain details about that interference. Therefore, we only used signals at fixed frequencies in the immunity tests described in this paper. IV. EXPERIMENTAL RESULTS The experiments performed at FDA–CDRH have two goals: verifying the capability of the new system to produce the test levels recommended in clause 27 of ISO14708-1 for frequencies up to 1 MHz and developing the procedure for testing the immunity of implantable pacemakers and neurostimulators to CW magnetic fields in this system. We tested four pacemakers and two neurostimulators at two distinct frequencies: 58 kHz (corresponding to an electronic article surveillance system) and 100 kHz (the highest frequency where the system is required to produce 150 A/m). Each AIMD was affected at a different test level. For one pacemaker and two neurostimulators, we extended the tests for finding the immunity characteristics in the frequency range from 1 kHz to 1 MHz. The pacemakers were tested without simulated heart signals. From the numerous data recorded in the FDA–CDRH database from the preliminary tests on AIMD, we next present signal diagrams which show EMI at different test frequencies and immunity diagrams in the frequency range of 1 kHz to 1 MHz for implantable pacemakers 1684 IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 54, NO. 9, SEPTEMBER 2007 Fig. 7. Change of the AV interval in magnetic fields at 5 kHz. Fig. 10. EMI diagram for the pulse interval. Fig. 8. EMI diagram for the AV interval. Fig. 11. EMI diagram for a neurostimulator H = 31 A/m; f = 15 kHz. Fig. 9. Change of the pulse interval in magnetic fields at 58 kHz. and neurostimulators. When interference was found, the phenomena occurred either abruptly or progressively with respect to the test level. Fig. 7 presents the abrupt change of the atrioventricular (AV) interval of a pacemaker tested in magnetic fields at 5 kHz while Fig. 8 shows the signal diagram for this interference. The acceptable domain for this parameter was assumed to be 150 ms % (from 120 ms to 180 ms). Fig. 9 presents the progressive degradation of the pulse interval of a pacemaker in CW magnetic fields at 58 kHz, while a diagram for this interference is given in Fig. 10. The accept%. For magable pulse interval was assumed within 0.85 s netic fields between 50 A/m and 120 A/m, this pacemaker delivered pulses at intervals from 0.5 s to 1.7 s. Fig. 9 illustrates a window effect, and the pacemaker returned to normal pacing for test levels that were greater than 120 A/m. In other words, the interference occurred for magnetic-field strengths between 50 and 120 A/m. Similar diagrams illustrate the degradation of the pulse amplitude. For example, Fig. 11 shows the signal from an old model neurostimulator which was exposed to magnetic fields at 15 kHz. The data from tests at different frequencies allow drawing immunity characteristics for AIMD in the frequency domain. Fig. 12. Immunity diagrams for a pacemaker tested in CW magnetic fields. Fig. 12 shows immunity diagrams for a pacemaker and Fig. 13 shows immunity diagrams for two neurostimulators in the frequency range from 1 kHz to 1 MHz. In both figures, curve 1 corresponds to the maximum available field in the test system. In Fig. 12 (for pacemakers), curve 2 shows the immunity levels corresponding to EMI criterion 1 (AV interval degradation), while curve 3 shows the immunity levels corresponding to EMI criterion 2 (the pulse interval alteration). The immunity diagram corresponding to EMI criterion 1 is shown only up to 100 kHz, but the interference occurred at all test frequencies between 100 kHz and 1 MHz at test levels below 2 A/m. During the tests for finding the immunity levels guided by EMI criterion 2 for this pacemaker, we ignored the parameter deviations counted for EMI criterion 1. The pacemaker characterized in Fig. 12 had the settings: DDD mode, unipolar pace/unipolar sense, atrial amplitude BUZDUGA et al.: TESTING THE IMMUNITY OF ACTIVE IMPLANTABLE MEDICAL DEVICES 1685 • Prototyping extended-length leads for obtaining effective loop areas larger than 300 cm in the induction coil C28. • Extending the testing frequency up to 30 MHz as recommended in clause 27 of ISO14708-1. • Increasing the volume for tests by using larger coils and higher ratings amplifiers. ACKNOWLEDGMENT Results of the previous research performed at FDA-CDRH in the domain of the AIMD testing with magnetic fields can be found in [7] and [8]. REFERENCES Fig. 13. Immunity diagrams for neurostimulator samples tested in CW magnetic fields. 5 V, ventricular amplitude 5 V, atrial sensitivity 0.5 mV, and ventricular sensitivity 1 mV. In Fig. 13, curve 2 shows the immunity levels of an old neurostimulator model, while curve 3 reveals the improved performance of a new neurostimulator model. The tests with neurostimulators were performed with leads of about 75-cm length. According to (9) and (10), these leads provide an effective loop area of about 300 cm on the contour of 17-cm diameter. Higher exposure areas could reveal lower immunity levels for these devices. The immunity characteristics presented in Figs. 12 and 13 indicate targets for further electromagnetic-compatibility (EMC) design of the AIMD in the frequency range from 1 kHz to 1 MHz. V. CONCLUSION The system presented in this paper offers the possibility to test the immunity of AIMD to CW magnetic fields up to 1 MHz by the immersion method. The test procedure developed in conjunction with this system provides an alternative to the voltage-injection methods recommended in the actual standards for implantable pacemakers. The new system is able to produce amplitude-modulated magnetic fields and can be used for validating the standard test methods with modulated voltages. The system can also be used for checking the performance of the history function of medical devices. The experiments show that the CW magnetic fields may cause various pacing events which should be accurately recorded by the devices with history function included. The new test system is feasible, the test procedure is suitable for pacemakers and neurostimulators of different makes, and the preliminary tests provided repeatable results. This paper offers a useful tool for the engineers involved in the research, EMC design, and quality assurance of the active implantable medical devices. The test system presented in this paper can be further developed in the following directions. [1] American Nationals Standards Institute/Association for the Advancement of Medical Instrumentation, ANSI/AAMI PC69, Jan. 2006, Active implantable medical devices—EMC test protocols for implantable cardiac pacemakers and implantable cardioverter defibrillators, 2nd ed., Committee Draft. [2] European Committee for Standardization/European Committee for Electrotechnical Standardization - CEN/CENELEC, EN45502-21:2003, Dec. 2003, Active Implantable Medical Devices, Part 2–1: Particular requirement for active implantable medical devices intended to treat bradyarrhythmia (cardiac pacemakers). [3] Implants for surgery—Active implantable medical devices—Part 1: General requirements for safety, marking and for information to be provided by the manufacturer, ISO 14708-1:2000(E), 2000, International Organization for Standardization (ISO), Geneva, Switzerland. [4] V. Buzduga, Magnetic field test system 1 kHz to 1 MHz (CW), H = 150 A/m at f = 100 kHz Rockville, MD, Tech. Rep. #DP-900-05, Nov. 2005, FDA-CDRH. [5] Draft IEEE Standard for Calibration of Electromagnetic Field Sensors and Probes, Excluding Antennas, from 9 kHz to 40 GHz., IEEE P1309, May 4, 2004. [6] F. W. Grover, Inductance Calculations. New York: Dover , 2004. [7] M. Misakian, J. Casamento, and O. Laug, “Development of emulator for walk-through metal detectors,” IEEE Trans. Electromagn. Compat., vol. 44, no. 3, pp. 486–489, Aug. 2002. [8] W. Kainz, J. Casamento, P. Ruggera, D. Chan, and D. Witters, “Implantable cardiac pacemaker EMC testing in a novel security system simulator,” IEEE Trans. Biomed. Eng., vol. 52, no. 3, pp. 520–530, Mar. 2005. Valentin Buzduga (M’06) received the M.S. degree in electronics from the Technical University “Gh. Asachi” Iasi, Romania, in 1977, and the Ph.D. degree in electronics and telecommunications from the Politehnica University, Bucharest, Romania, in 2000. Currently, he is with Scantek, Inc., Columbia, MD, and an Adjunct Professor with Capitol College, Laurel, MD. He was a Design and Compliance Engineer with Tehnoton, Isai, and taught courses on electronics engineering and electromagnetic compatibility (EMC) at Technical University “Gh. Asachi” and performed research in EMC and acoustics. He developed new models for the electromagentic-interference (EMI) analysis in terms of circuits’ theory and published a number of papers on these topics, including the three-port characterization of the transmission line. In acoustics, he developed test methods based on the constant divergence of the sound pressure level which were published in the Noise Control Engineering Journal. From 2004 to 2006, he participated in a research fellowship program coordinated by ORISE at FDA–CDRH, where he performed emission tests with metal detectors, immunity tests with medical devices, and developed a magnetic-field test system and test methods for implantable medical devices. His research interest includes the EMC design, modeling of the electromagnetic interactions for biomedical applications, and development of acoustical test methods immune to environmental noise. 1686 IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 54, NO. 9, SEPTEMBER 2007 Donald M. Witters (M’80–SM’93) received the B.S. degree from the University of Maryland, College Park, and the M.S. degree in biomedical engineering from Georgetown University, Washington, D.C. He has more than 30 years of experience working at the U.S. Food and Drug Administration’s Center for Devices and Radiological Health (CDRH), and chairs the CDRH Electromagnetic Compatibility (EMC) and Wireless Working Group. This group is charged with assessing EMC and radio-frequency wireless technology issues for medical devices and systems and developing strategy and tools for public health and medical device safety and effectiveness. He has performed laboratory research on medical device EMC, RF wireless technology, and precision microwave calibrations, and helped develop and write several national and international consensus standards. He was instrumental in the development of the wireless medical telemetry service (WMTS) that remains the first radio spectrum created to protect wireless medical telemetry from electromagnetic interference. Jon P. Casamento (M’79) received the B.S.E.E. degree from the University of Maryland, College Park, in 1979. Currently, he is the Deputy Director of the Division of Solid and Fluid Mechanics at the FDA’s Center for Devices and Radiological Health, Office of Science and Engineering Laboratories, Rockville, MD. He was with the Food and Drug Administration since 1980 and has been testing medical devices for electromagnetic compatibility with radio-frequency emitters since 1991. He has made measurements of electromagnetic emissions from antitheft systems and electromagnetic surveillance systems. He is interested in broadband magnetic-field sources for testing medical device immunity to these emissions. Wolfgang Kainz (M’02) received the M.S. degree in electrical engineering from the Technical University of Austria, Vienna, Austria, in 1997 and the Ph.D. degree in technical science from the Technical University Vienna, Austria, in 2000. After working for the Austrian Research Centers Seibersdorf (ARCS) on electromagnetic compatibility of electronic implants and exposure setups for bio-experiments, he joined The Foundation for Research on Information Technologies in Society—IT’IS (Zurich, Switzerland) as Associate Director. He was a Manager for IT’IS together and worked on the development of in-vivo and in-vitro exposure setups for bio-experiments. In 2002, he joined the U.S. Food and Drug Administration in the Center for Devices and Radiological Health. He is Chairman of the IEEE Standard Coordination Committee 34, Subcommittee 2 which develops compliance techniques for wireless devices. His research interest is focused on the safety and effectiveness of medical devices and safety in electromagnetic fields. This includes computational electrodynamics (FDTD simulations) for safety and effectiveness evaluations; magnetic resonance imaging (MRI) safety; performance and safety of wireless technology used in medical devices; electromagnetic compatibility of medical devices, especially electronic implants; and dosimetric exposure assessments.