Education & Training
Playing Dice with Steam
Sterilization Process Monitoring
by Martha Young, BS, MS, CSPDT
by David Jagrosse, CSPDT
Objectives
After completion of this self-study activity, the learner
will be able to:
1. Choose an internal chemical indicator that provides the
information you desire about the sterilization process.
2. Correctly use Class 5 integrating indicator process challenge devices to release non implant loads.
70
MANAGING INFECTION CONTROL
3.
4.
Develop a recall policy and procedure based on the
results of biological and chemical indicator process challenge devices.
Discuss the risks involved with using a chemical indicator process challenge device instead of a biological
indicator process challenge device for routine sterilizer
monitoring and release of implants.
December 2009
Education & Training
Test Questions
6.
2.
7.
1.
3.
4.
5.
Sterilizer qualification testing for dynamic-air-removal
sterilizers includes running a BI PCD in three consecutive
empty cycles followed by running a Bowie-Dick test pack
in three consecutive empty cycles.
A. True
B. False
Class 5 integrating indicators respond to all the critical
parameters of the sterilization process and their performance is designed to be equivalent to or exceed the
performance requirements of BIs under ideal steam
sterilization conditions
A. True
B. False
A Class 5 integrating indicator process challenge device
may be used to release implants.
A. True
B. False
Running a biological indicator in each load will reduce the
total number of items affected by a positive biological
indicator and, thereby, reduce overall patient risk.
A. True
B. False
Class 6 emulating indicators are cycle verification indicators
designed to react to all critical variables of specified
sterilization cycles.
A. True
B. False
Many thanks to the team at 3M Health Care for
working with Managing Infection Control to provide
the following accredited course. IAHCSMM has
awarded 1 contact point for completion of this
continuing education lesson toward IAHCSMM
recertification. The CBSPD has preapproved this
inservice for 1 contact hour for a period of five (5)
years from the date of publication, and to be used
only once in a recertification period. This inservice is
3M Health Care Provider approved by the California
Board of Registered Nurses, CEP 5770 for 1 contact
hour. This form is valid up to five (5) years from the
date of publication. Instructions for submitting
results are on page 86.
Managing Infection Control and 3M Health
Care will be working collaboratively to provide
continuing education courses in monthly editions of
Managing Infection Control.
72
MANAGING INFECTION CONTROL
8.
9.
The usage of Class 6 emulating indicators is not
discussed in the Association for the Advancement of
Medical Instrumentation’s, Comprehensive guide to
steam sterilization and sterility assurance in health
care facilities, ANSI/AAMI ST79:2006, A1:2008,
and A2:2009.
A. True
B. False
The sterility assurance level (SAL) of a steam
sterilization process can be measured by a chemical
indicator.
A. True
B. False
The Association for the Advancement of Medical
Instrumentation’s, Comprehensive guide to steam
sterilization and sterility assurance in health care
facilities, ANSI/AAMI ST79:2006, A1:2008, and
A2:2009 recommends the use of biological indicators
for routine sterilizer efficacy testing, monitoring loads
containing implants, and sterilizer qualification testing.
A. True
B. False
If the Class 5 integrating indicator or Class 6 emulating
indicator in a process challenge device indicates a
sterilization process failure for a load and no operator
error is identified then you do not have to recall loads
back to the last negative biological indicator.
A. True
B. False
10. Use recommended practices and standards developed
by the Association for the Advancement of Medical
Instrumentation, the Association of periOperative
Registered Nurses, and the Centers for Disease
Control and Prevention to guide best practices and
protect patients.
A. True
B. False
Introduction
There is nothing worse than a recall. Okay, maybe
there is, such as a recall that does not collect 100 percent
of the contents of the affected products. A few years ago
I had a brand new steam sterilizer that was producing
random positive biological indicators. It was the
darnedest thing.
Each time a sterilization process failure occurred, we
would immediately re-verify the results of what I refer to
as the “holy trinity”: the physical, chemical (CI) and
biological indicator (BI) results. All were performing as
expected. There were no signs of a sterilization process
failure other than the occasional positive BI. It came to the
point that the staff did not “trust” the new $100,000 steam
sterilizer anymore.
After an exhaustive step-by-step process involving
facility engineering, the sterilizer manufacturer, and
December 2009
Education & Training
the BI manufacturer it was determined that the culprit was
a manufacturing defect involving a steam trap. It wasn’t up to
specifications which caused inconsistencies in pulling or
achieving the required deep vacuums needed to effectively
remove air. The part was replaced (not only on ours but on the
entire line of the manufacturer’s steam sterilizers) and the intermittent process failures ceased. As a side note, 100 percent of
my recalled goods were captured during these events due to my
awesome staff following our recall policy. We also re-qualified
the steam sterilizer each time it failed following the guidance
of the Association for the Advancement of Medical
Instrumentation’s Comprehensive guide to steam sterilization
and sterility assurance in health care facilities, ANSI/AAMI
ST79:2006.1
In our dynamic-air-removal steam sterilizer we ran a BI
PCD in three consecutive empty cycles followed by a BowieDick test pack in three consecutive empty cycles. The sterilizer
was put back into use if the BIs were negative and the BowieDick test sheets showed a uniform color change. (ANSI/AAMI
ST79 section 10.7.5.1) 2
We turned this negative experience into a positive
chance to review the entire steam sterilization process and
identify areas of opportunity for improvement. The important
takeaways were that we needed to set up a more challenging
and frequent monitoring regimen thereby increasing our
chances of not only detecting sterilization process failures
but doing so as soon as possible. The review identified the
following improvements.
Upgrade Internal Chemical Indicators
We were using a Class 4 multi-variable indicator for
internal pack monitoring. For biological indicator monitoring
our frequency of testing was once daily and with every
implant load. The exception being during the time we had
problems with the “bad” steam sterilizer, when BIs were
used on every cycle. We chose to upgrade to Class 5
integrating indicators because they provide more information about the performance of the steam sterilization process
than Class 4 CIs by monitoring all the critical parameters
of the steam sterilization process. In addition their performance is designed to be equivalent to or exceed the
performance requirements of BIs under ideal steam sterilization conditions.
The ANSI/AAMI ST79 guidance for choosing the
class of CI is:
“An internal CI should be used with each
package, tray, or rigid sterilization container system
to be sterilized. This internal CI may be a singlevariable indicator (Class 3 CI), multi-variable
indicator (Class 4 CI), or integrating indicator
(Class 5 CI). The class of CI chosen will depend
upon how many critical process variables are to be
monitored and how much information is desired
about the sterilization process.” (ANSI/AAMI ST79
section 10.5.2.2.2) 2
Today, we use a Class 5 CI inside each package and
do not use that package if it has not reached its endpoint.
The Class 5 CI has the 3 stated values required to
meet the Association for the Advancement of Medical
Instrumentation Sterilization of health care products-Chemical
indicators-Part 1: General requirements, ANSI/AAMI/ISO
11140-1:2005 CI standard. This standard upgraded the
performance requirements of Class 5 CIs by requiring their
performance correlate with a BI at three time/temperature
relationships (e.g., 121°C/250°F, 132°C/270°F and at least
one temperature in between such as 128°C /263°F). The
standard also requires that for the stated value at 121ºC/
250ºF be greater than 16.5 minutes to ensure that chemical
indicators labeled for use in a 132°C/270°F cycle do not
change too quickly or inappropriately at lower temperatures.3
74
MANAGING INFECTION CONTROL
December 2009
Education & Training
In our facility a BI/Class 5 CI PCD is used in every load and implants
are quarantined until the BI is negative.
When the internal chemical indicator detects a problem we
follow the guidance of ANSI/AAMI ST79:
“If the interpretation of the CI suggests
inadequate steam processing, the contents of the
package should not be used. The department head or
designee in the sterilizing department should then
decide whether to recall that sterilized load. The decision should be based on the results of physical
monitoring (time and temperature recordings), the
results of internal CIs elsewhere in the load, and, if
applicable, the results of any PCDs in the load (a PCD
containing a BI, a PCD containing a BI and a Class 5
integrating indicator, or a PCD containing a Class 5
integrating indicator). If the results of a PCD
containing a BI are not yet available, the remaining
packages from the same load should be quarantined and
not used until the BI results are obtained.” (ANSI/AAMI
ST79 section 10.5.2.2.2) 2
We felt it was important to have the most accurate internal
chemical indicator on the market. Since the Class 5 integrating
indicator mimics the BI, we have greater assurance that if it
passes then the BI will be negative. We have detected mechanical
issues by using the Class 5 integrating indicator. Typically we
have needed a steam trap replaced because air was not being
completely removed from the chamber on all cycles.
ANSI/AAMI ST79 guidance says a “PCD containing a
Class 5 integrating CI may be used to routinely release loads
containing nonimplantable items to assure the adequacy of the
sterilization cycle.” (ANSI/AAMI ST79 section 10.5.4) 2 A Class
5 CI PCD cannot be used to release implants. (ANSI/AAMI
section 10.5.4) 2
We adopted the use of Class 5 Integrating Indicator PCDs
when AAMI provided guidance for use. We decided to run these
Class 5 CI PCDs in every load and a BI daily plus implants
because we thought it would be more cost effective. When we
realized that we would have to recall back to the last negative BI
when the Class 5 PCD showed a failure, the savings was not
there so we went to every load monitoring with a BI PCD (see
Policy and procedure update).
Policy and Procedure Update
The staff realized that it only made sense to run BIs on every
load to reduce the total number of items affected by a positive BI
76
MANAGING INFECTION CONTROL
and thereby reduce overall patient risk. The cost was measured
against the possibility of one potential lawsuit with our risk
management department and it was determined that the
every load BI testing was potentially less expensive than
one law suit. We also wanted to deliver the same standard
of care for our patients. Wouldn’t you want the instrument
sets for your surgery procedure tested with a BI?
We hold BIs to be the gold standard of testing as they
contain living microorganisms. To bridge the gap between
the 3-hour rapid readout BI result we would also use a
standalone Class 5 CI PCD on every load. Shortly after the
rapid readout BI manufacturer introduced the rapid readout
BI PCD containing a Class 5 integrating indicator, we had
the best of both worlds. We reduced cost and storage space
with the new bundled BI/ Class 5 CI PCD.
In addition the new ANSI/AAMI ST79:2006 guidance
stated that a Class 5 integrating CI should be included in the
BI PCD which should be used to monitor every sterilization
load containing implants.
“A Class 5 CI should be included with the BI
in the PCD so that if an implant must be released on
an emergency basis, additional information about
the critical parameters of the sterilization process
will be available and documented.” (ANSI/ AAMI
ST79 section 10.6.1) 2
The implant should be quarantined until the BI result
is available. (ANSI/AAMI ST79 section 10.6.3) 2 In cases
of documented medical exceptions (see ANSI/AAMI
Annex L for examples of an implant log and exception
form) the implant could be released based on the Class 5
CI result. This event needs to be documented and the
information fully traceable to the patient. (ANSI/AAMI
ST79 10.6.3) 2
In our facility a BI/Class 5 CI PCD is used in every load
and implants are quarantined until the BI is negative. Loads
are not released on the results of a Class 5 CI except in
defined emergency situations. Nonimplant loads are released
based on the Class 5 CI result.
This also meets the ANSI/AAMI guidance which
states a BI should be used with PCDs for routine sterilizer
efficacy monitoring at least weekly, but preferably ever
day that the sterilizer is in use. (ANSI/AAMI ST79 section
10.5.3.2) 2
December 2009
Education & Training
That was then. This is now.
Today Class 6 emulating indicators are available from at least
three manufacturers in the U.S. market. Currently there are no
ANSI/AAMI recommended practices covering the use of these
devices. The new A2:2009 amendments in ANSI/AAMI ST79
only include a definition or acknowledgement of their existence.
“Emulating indicators (Class 6) are cycle verification indicators designed to react to all critical variables
of specified sterilization cycles, with the stated values
having been generated from the critical variables of
the specific sterilization process.
NOTE 1-This edition of ANSI/AAMI ST79 does
not cover the use and application of Class 6 emulating
indicators.
NOTE 2-See ANSI/AAMI/ISO 15882:2008 for
information on the selection, use, and interpretation
of chemical indicators.” (ANSI/AAMI ST79 section
10.5.2.1) 2
The Class 6 emulating indicator products have caused a
good deal of debate since their introduction, in my opinion
primarily due to poor and confusing marketing and a lack of data
and education. I have always had a philosophy that I describe
as the “Rainbow.” In nature why would we ever want to remove
a color from the rainbow? We would much rather add one. The
same philosophy holds for monitoring the sterilization process.
When there is a sterilization process failure, I want a plethora
of products to accurately represent what was occurring in
that cycle.
Class 6 CIs were marketed as replacements for all other CIs
and BIs. The new Holy Grail had been found. I am among many
who have not quite determined where these products will play
a role (if any) in my arsenal of monitoring the effectiveness of
the sterilization process. I am currently doing my own product
evaluations and testing.
In the testing performed at my facility, my dynamicair-removal sterilizers were capable of killing BIs in a PCD
at a one minute exposure at 135ºC with a three phase vacuum
cycle. In the same cycle, the Class 5 CIs in a PCD did not reach
their end point until three minutes. The current Class 5 CIs
and PCDs are correlated to mimic a BI death kill under defined
ideal steam sterilization conditions while Class 6 CIs are not.
Class 6 CIs in a PCD changed at four minutes. Even though
it is a small window of time, the Class 6 CIs took longer to
reach their endpoint but is that important since we are not
inactivating chemicals on our surgical instruments, we are
killing living microorganisms.
The ANSI/AAMI definition of an SAL is:
“sterility assurance level (SAL):probability of a
single viable microorganism occurring on an item after
sterilization.” (ANSI/AAMI section 2, definition 2.121) 2
78
MANAGING INFECTION CONTROL
ANSI/AAMI ST79 defines sterilization as:
“Validated process used to render a product
free from viable microorganisms.” (ANSI/AAMI
section 2, definition 2.122) 2
ANSI/AAMI ST79 also states:
“Biological indicators are the only sterilization
process monitoring device that provides a direct
measure of the lethality of the process.” (ANSI/
AAMI section 10.5.3.1) 2
Chemical indicators cannot determine or confirm the
SAL achieved for a sterilization load. The SAL can only be
estimated for completely validated processes. Biological
indicators provide the only direct confirmation that a
process killed microorganisms.
You have to ask yourself how much further do we want
to go beyond dead spores. Aren’t dead spores dead already?
ANSI/AAMI ST79 has very clear guidance on the
usage of BIs. A BI PCD should be used for:
Routine sterilizer efficacy testing weekly, preferably
each day the sterilizer is in use (section 10.5.3.2);
Every implant load, which should be quarantined until
the BI testing is available (section 10.5.3.2 and
10.6.3); and
Sterilizer qualification testing after the sterilizer installation, relocation, malfunctions, and major repairs and
after sterilization process failures, in each type of cycle
used on a sterilizer (section 10.5.3.2).2
“Rationale: The use of BIs provides evidence of
efficacy by challenging the sterilizer with a large
number of highly resistant bacterial spores.
Biological monitoring provides the only direct
measure of the lethality of a sterilization cycle.”
(ANSI/AAMI ST79 section 10.7.1) 2
ANSI/AAMI is very clear that CIs do not replace the
use of BIs but are used as external and internal CIs. In addition Class 5 CI PCDs may not be used to monitor implant
loads. The Association of periOperative Room Nurses
(AORN) have clear recommendations for both the use of
chemical and biological indicators in Recommendation
XVI of the Recommended Practices for Sterilization in the
Perioperative Practice Setting as do the Centers for Disease
Control and Prevention (CDC) in Recommendation 16 in
the 2008 Guideline for Disinfection and Sterilization in
Healthcare Facilities.4,5
Dr. Sheila Murphey of the FDA also is clear about the
fact that CIs do not replace the use of BIs. This is stated in
an email from her that is posted on the CBSPD Web site on
April 11, 2009.
December 2009
Education & Training
“The Steris Verify SixCess CI is a Chemical
Indicator. It may be used as you would use any other
Chemical Indicator. However, it is NOT a Biological
Indicator and should not be used in place of a BI.”6
What about recalls? If the Class 6 CI PCD shows a
failure do you recall back to the last Class 6 CI PCD that
showed a pass? The answer is “No” based on the A2:2009
amendments for ANSI/AAMI ST79. All recalls are back to the
last negative BI. An updated section addresses what actions
to take when a BI PCD or CI PCD (Class 5 CI, Class 6
not included) indicates a sterilization process failure.
(ANSI/AAMI ST79 section 10.7.5) 2 This section now includes
a decision tree for conducting investigations of steam sterilization
continued on page 82
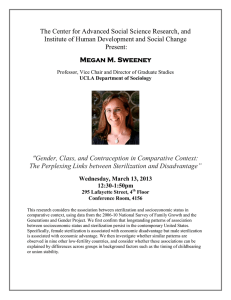
Figure 12. Decision tree for conducting investigations of steam sterilization process failures.
Reprinted from ANSI/AAMI ST79:2006 and A1 & A2 with permission of Association for the Advancement of Medical
Instrumentation, Inc.© 2009 AAMI www.aami.org. All rights reserved. Further reproduction or distribution prohibited.
December 2009
MANAGING INFECTION CONTROL
79
Education & Training
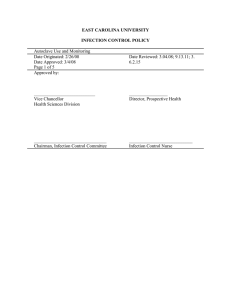
Table 8
Checklist for identifying reasons for steam sterilization process failures
OPERATOR ERRORS
Incorrect use and interpretation of monitoring tools
•
Incorrect physical monitors for the load
•
Incorrect use of BI or BI PCD
Incorrect selection of BI or BI PCD for the load
Incorrect placement of BI PCD in the load
(e.g., another pack was placed on top of the PCD)
Incorrect incubation of BI
Misinterpretation of BI result
Incorrect documentation of BI result
•
Incorrect use of Class 5 integrating CI PCD
Incorrect selection of CI PCD for the load
Incorrect placement of CI PCD in the load
(e.g., another pack was placed on top of the PCD)
Misinterpretation of Class 5 integrating CI result
Incorrect documentation of Class 5 integrating
CI result
•
Incorrect use of internal CI
Incorrect selection of internal CI for the load
Misinterpretation of internal CI result
Incorrect documentation of internal CI results
•
Incorrect storage of any CIs or BIs
•
Failure to check physical monitors for functionality
before running cycle
•
Use of broken media ampoule or ampoule with missing
spore strip
•
Use of BI PCD or CI PCD that is missing the BI or CI
•
Use of defective CI (e.g., a CI that is expired, faded, shows
a partial color change because of incorrect storage, or has
been previously exposed to the sterilant)
Selection of incorrect cycle for load contents
(containment device or medical device manufacturer’s
instructions for use not followed)
Use of inappropriate packaging materials or
packaging technique
•
Incorrect packaging or containment device for
the cycle parameters
•
Incorrect preparation of containment device for use (e.g.,
incorrect filters, valves, or bottom tray)
•
Use of a paper–plastic pouch, woven or nonwoven
•
•
•
•
•
•
•
•
wrapper, or towel in a 270ºF to 275ºF (132ºC to
135ºC) gravity-displacement cycle
Use of a tray that does not allow air removal and
steam penetration
Use of a wrapper that is too large for the application
Placement of a folded paper–plastic pouch inside
another paper–plastic pouch
Placement of a paper–plastic pouch inside
a wrapped set or containment device without
verification of adequate air removal and steam
penetration by product testing
Incorrect placement of basins in set
(i.e., basins are not aligned in the same direction)
Failure to use nonlinting absorbent material
between nested basins
Preparation of textile packs that are too dense
to sterilize with the cycle parameters chosen
Inadequate preconditioning of packaging
materials (i.e., not holding package materials
at 68ºF to 73ºF (20ºC to 23ºC) for 2 hours
before use)
Incorrect loading of sterilizer
•
Stacking of containment devices if not
recommended by manufacturer
•
Stacking of perforated instrument trays
•
Incorrect placement of instrument trays
(i.e., not laying instrument trays flat or parallel
to the shelf)
•
Incorrect placement of paper–plastic pouches
(e.g., placing pouches flat instead of on edge;
not allowing sufficient space between pouches;
not placing pouches with plastic sides facing
one direction)
•
Incorrect placement of basins (i.e., not placing
basins on their sides so that water can drain)
•
Incorrect placement of textile packs (i.e., not
placing them on edge)
•
Placement of packages too close together,
impeding air removal and sterilant penetration in
the load
(continued on page 82)
80
MANAGING INFECTION CONTROL
December 2009
Education & Training
(continued from page 80)
Table 8
Checklist for identifying reasons for steam sterilization process failures
STERILIZER OR UTILITIES MALFUNCTIONS
Poor steam quality or quantity
•
Wet steam
Improper insulation of steam lines
Malfunction of trap in steam line or no trap
in steam line
Malfunction of drain check valve or no
drain check valve
Steam contact with a cold load
Too much water in steam produced at
boiler
•
Superheated steam
Improper heatup of chamber
Desiccated packaging materials (e.g.,
towels)
Steam pressure too low for the temperature
Excessive reduction of steam pressure too
close to sterilizer
Faulty steam control valve or pressure
reducer control valve
•
Other steam problems
Variations in steam pressure because of
clogged filter, poorly engineered piping,
or excessive demands
Out-of-calibration pressure gauges
and controllers
Clogged steam lines
Clogged steam supply strainer
Clogged chamber drain line, strainer, or
chamber drain screen
Malfunction of valves
Incomplete air removal
•
Inadequate vacuum or vacuum depth or other air removal system
•
Clogged chamber drain line, strainer, or chamber drain screen
•
Clogged vent lines
•
Leak caused by faulty door gasket
•
Leak in other areas of chamber
•
Plugged, faulty or incorrectly adjusted control valves
•
Low steam pressure
•
High water temperature
•
Inadequate water supply pressure
•
Clogged water supply strainer
•
Trapping of air by the load
•
Incorrect cycle parameters for the load
Inadequate cycle temperature
•
Out-of-calibration temperature gauge
•
Long heatup time for large loads (i.e., heat lag)
•
Clogged chamber drain line, strainer, or chamber drain screen
•
Variations in steam pressure because of clogged filter, poorly
engineered piping, or excessive demands on steam supply
•
Presence of noncondensable gases in steam line and load
•
Inadequate steam supply pressure
•
Clogged steam supply strainer
Insufficient time at temperature
•
Out-of-calibration control timer
•
Inappropriate cycle parameters for the load being processed
•
Come-up time of less than 1.5 minutes in a 270ºF to 275ºF
(132ºC to 135ºC) gravity-displacement cycle
•
Oversized load
Reprinted from ANSI/AAMI ST79:2006 and A1 & A2 with permission of Association for the Advancement of Medical Instrumentation, Inc.©
2009 AAMI www.aami.org. All rights reserved. Further reproduction or distribution prohibited.
continued from page 79
process failures (see Figure 12) and a trouble shooting
checklist for identifying reasons for steam sterilization
process failures (see Table 8).2
Figure 12 says that if the CI PCD fails (see CI failures
on first line of decision tree), “Quarantine load, remove
sterilizer from service, and investigate cause of failure.”2
Figure 12 goes on to say:
“If cause of failure is immediately identified
(usually operator error) and confined to one load or
one item within the load (internal CI), correct the
cause and reprocess the load. If cause of the failure
82
MANAGING INFECTION CONTROL
is not immediately identified, quarantine the load and
recall all loads back to the last negative BI.”2
This means that if the Class 5 or any other CI PCD (i.e.,
Class 6 emulating indicator) in the load indicates a failure and
the reason for the failure is not immediately identified (usually
operator error) then all loads processed since the last negative BI
should be recalled. A recall back to the last passed CI PCD is not
a recall. Recalls are based on the BI results.2 A CI PCD may
assist in identifying a sterilization process failure for a specific
load but:
December 2009
Education & Training
“While the performance of Class 5 integrating CIs
has been correlated to the performance of BIs, these
sterilization monitoring devices do not contain spores
and thus do not directly measure the lethality of a
sterilization cycle; however, they provide additional
information about the attainment of the critical
parameters of the sterilization process.” (ANSI/AAMI
ST79 10.5.2.1) 2
This recall requirement would hold true for Class 6 CIs
because they also do not contain spores and their performance
is not required to correlate to a BI. Do we ignore these guidelines if we are using a Class 6 CI and not recall back to the last
negative BI if this CI PCD shows a failure?
Class 6 CIs are cycle specific. This is good and bad for
Class 6. It is good for monitoring extended cycles if FDA
ever chooses to clear those products for use but it is a concern
for end users. My staff is very intelligent and very capable
It is a slippery legal path
to deviate from established
practice and guidelines by
cherry picking which ones
to follow and which ones
to ignore. It is a legal
homerun for the plaintiff.
at Middlesex hospital, the best of the best, but they are
apprehensive about having to select specific monitoring
products for specific cycles with the large variety of specific
cycles we run these days in the department.
Although ANSI/AAMI ST79 states “As technology
progresses, new sterilization process monitoring devices may
be cleared by FDA and become available for use in health
care facilities. Health care facilities should rely on the knowledge and expertise of their infection prevention and control,
central service and surgical services professionals in the
selection and use of process monitoring devices.” (ANSI
/AAMI ST79 section 10.4) 2 AAMI cannot simultaneously
provide guidelines for every product as soon as it comes to
market. They are giving us latitude but that does not mean
you can ignore recommended practices such as using a BI to
release implants which should be quarantined until the BI
result is known. These recommendations are developed to
improve patient care and should not be ignored.
Don’t ever make decisions in a vacuum or be the lone
wolf within what The Joint Commission considers to be
your local standard of practice (i.e., facilities within your
geographic area). Healthcare facilities must consider the legal
ramifications of being a lone wolf when these decisions could
potentially be part of a jury trial. The question is “Why are
you the only one doing this outside the standard of practice.
Who made this decision and why? I can hear the plaintiff
asking you why you decided to follow some of the current
practices and guidelines but then ignored other portions of it.
It is a slippery legal path to deviate from established practice
and guidelines by cherry picking which ones to follow and
which ones to ignore. It is a legal homerun for the plaintiff.
Summary
Albert Einstein once said “God does not play dice with
the universe” meaning there was a purpose and order for
things we see in it. I believe this applies to our field of work.
As a myriad of new monitoring products along with their
stated uses enter the market they will find a place, a meaning,
and a purpose. Recommended practices and standards will be
developed by AAMI, AORN, and the CDC to guide us to best
practice thereby protecting the people for whom we are all
doing our best every day, our patients.
References
1.
2.
3.
84
MANAGING INFECTION CONTROL
Association for the Advancement of Medical Instrumentation.
Comprehensive guide to steam sterilization and sterility assurance
in health care facilities. ANSI/AAMI ST79:2006.
Association for the Advancement of Medical Instrumentation.
Comprehensive guide to steam sterilization and sterility assurance
in health care facilities. ANSI/AAMI ST79:2006, A1:2008 and
A2:2009.
Association for the Advancement of Medical Instrumentation.
Sterilization of health care products-Chemical indicators-Part 1:
General requirements, ANSI/AAMI/ISO 11140-1:2005.
December 2009
Education & Training
Sterile Process and Distribution CEU Information
CEU Applicant Name _________________________________________________
Address___________________________________________________________
City____________________________ State________ Zip Code ______________
4.
5.
6.
Association of periOperative Registered
Nurses. Recommended Practices for
Sterilization in the Perioperative Practice
Setting. AORN:2009.
Centers for Disease Control. Guideline for
Disinfection and Sterilization in Healthcare
Facilities, 2008.
FDA clarification of Class 6 emulating
indicators clearance from April 11, 2009.
CBSPD website: http://www.sterileprocessing.
org/ info.htm#ci
David Jagrosse, CSPDT, is the current
manager of central sterile service at
Middlesex hospital in Middletown, Conn.
He has more than 20 years of CSS/SPD
experience in the capacities of technician,
supervisor and manager. Mr. Jagrosse has
served as both a member (06) and chair
(07) of the former ASHCSP’s recognition
committee and is now an active member of
IAHCSMM. He has served IAHCSMM’s
Connecticut Central Service Association
chapter (www.ctsterile.org) as communications officer (98-00), vice president
(06-08) and current president. He is also
currently an active voting member of the
AAMI standards workgroup that publishes
AAMI ST79 (STWG40) that develops
guidelines within the CSS/SPD field. Mr.
Jagrosse is president of David Jagrosse
Consulting LLC, 203.465.8502, which
offers public speakers, educational seminars, and CSS/SPD audits. Mr. Jagrosse is
a consultant for 3M.
ANSWERS
1.
2.
3.
4.
5.
A
A
B
A
A
6.
7.
8.
9.
10.
A
B
A
B
A
Reprint with permission from Workhorse Publishing L.L.C.
86
MANAGING INFECTION CONTROL
The CBSPD (Certification Board for Sterile Processing and Distribution) has preapproved this inservice for 1 contact hour for a period of five (5) years from
the date of publication. Successful completion of the lesson and post test must be
documented by facility management and those records maintained by the individuals
until recertification is required. DO NOT SEND LESSON OR TEST TO CBSPD.
For additional information regarding Certification contact: CBSPD, 148 Main St.,
Lebanon, NJ, 08833 or call 908-236-0530 or 800-555-9765 or visit the Web site at
www.sterileprocessing.org.
IAHCSMM has awarded 1 Contact Point for completion of this continuing education
lesson toward IAHCSMM recertification.
Nursing CE Application Form
This inservice is approved by the California Board of Registered Nurses, CEP
5770 for one (1) contact hour. This form is valid up to five (5) years from the date
of publication.
1. Make a photocopy of this form.
2. Print your name, address and daytime phone number and position/title.
3. Add the last 4 digits of your social security number or your nursing license number.
4. Date the application and sign.
5. Answer the true/false CE questions. KEEP A COPY FOR YOUR RECORDS.
6. Submit this form and the answer sheet to:
3M Sterilization Assurance, Attn HC4160
RR Donnelly Fulfillment Services
585 Hale Ave N., Oakdale, MN 55128-9935
7. For questions, contact craig@manageinfection.com.
8. Participants who score at least 70% will receive a certificate of completion
within 30 days of Managing Infection Control’s receipt of the application.
Application
Please print or type.
Name______________________________________________________________
Mailing Address______________________________________________________
City, State, Country, Zip _______________________________________________
Daytime phone (
)__________________________________________
Position/Title_______________________________________________________
Social Security or Nursing License Number ________________________________
Date application submitted _____________________________________________
Signature __________________________________________________________
Offer expires November 2014
On a scale of 1-5, 5 being Excellent and 1 being Poor, please rate this program
for the following:
1)
Overall content ___________________
3)
Usability of content ________________
2)
Met written objectives ______________
<12/09>
Copyright©2009-2010/Workhorse Publishing L.L.C./All Rights Reseved.
December 2009