Aviation Public Health Manual
advertisement

CIVIL AVIATION AUTHORITY, BANGLADESH
AVIATION PUBLIC HEALTH MANUAL
FIRST EDITION
NOVEMBER 2015
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
RECORD OF AMENDMENTS
Amendment
Number
19 Nov 2015
Date
Pages Affected
Date Entered
Initials
i
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
LIST OF EFFECTIVE PAGES
Topic/Chapter
Page No
Edition
Date of Issue
Cover
-
1
19 Nov 2015
Record of Amendments
I
1
19 Nov 2015
List of effective pages
ii-vi
1
19 Nov 2015
Table of contents
vii-xi
1
19 Nov 2015
Appendices
Xii
1
19 Nov 2015
Distribution List
Xiii
1
19 Nov 2015
Foreword
Xv
1
19 Nov 2015
Chapter 1
1-1
1
19 Nov 2015
1.1
1-1-6
1
19 Nov 2015
1.2
1-7
1
19 Nov 2015
Chapter 2
2-1
1
19 Nov 2015
2.1
2-1
1
19 Nov 2015
2.2
2-1
1
19 Nov 2015
2.3
2-2
1
19 Nov 2015
2.4
2-3
1
19 Nov 2015
2.5
2-4
1
19 Nov 2015
2.6
2-4
1
19 Nov 2015
2.7
2-4-6
1
19 Nov 2015
2.8
2-6
1
19 Nov 2015
Figure 2.1
2-7
1
19 Nov 2015
Chapter 3
3-1
1
219Nov 2015
3.1
3-1
1
19 Nov 2015
3.2
3-2-5
1
19 Nov 2015
3.3
3-6
1
19 Nov 2015
3.4
3-6
1
19 Nov 2015
3.5
3-7
1
19 Nov 2015
19 Nov 2015
ii
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
3.6
3-7-9
1
19 Nov 2015
3.7
3-10
1
19 Nov 2015
3.8
3-10
1
19 Nov 2015
3.9
3-11
1
19 Nov 2015
3.10
3-11
1
19 Nov 2015
3.11
3-11
1
19 Nov 2015
3.12
3-12
1
19 Nov 2015
3.13
3-12
1
19 Nov 2015
3.14
3-13
1
19 Nov 2015
3.15
3-13
1
19 Nov 2015
3.16
3-14
1
19 Nov 2015
3.17
3-14
1
19 Nov 2015
3.18
3-15
1
19 Nov 2015
3.19
3-15
1
19 Nov 2015
Chapter 4
4-1
1
19 Nov 2015
4.1
4-1
1
19 Nov 2015
4.2
4-1
1
19 Nov 2015
Figure 4.1
4-2
1
19 Nov 2015
4.3
4-2
1
19 Nov 2015
4.4
4-3
1
19 Nov 2015
4.5
4-3-4
1
19 Nov 2015
Figure 4.2
4-5
1
19 Nov 2015
4.6
4-6
1
19 Nov 2015
4.7
4-6
1
19 Nov 2015
4.8
4-7
1
19 Nov 2015
4.9
4-7
1
19 Nov 2015
Chapter 5
5-1
1
19 Nov 2015
5.1
5-1
1
19 Nov 2015
19 Nov 2015
iii
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
5.2
5-1
1
19 Nov 2015
5.3
5-2
1
19 Nov 2015
5.4
5-2-3
1
19 Nov 2015
5.5
5-4
1
19 Nov 2015
5.6
5-4
1
19 Nov 2015
5.7
5-4-5
1
19 Nov 2015
5.8
5-6
1
19 Nov 2015
5.9
5-6
1
19 Nov 2015
5.10
5-7-8
1
19 Nov 2015
5.11
5-9
1
19 Nov 2015
Figure 5.1
5-10
1
19 Nov 2015
Figure 5.2
5-11
1
19 Nov 2015
Chapter 6
6-1
1
19 Nov 2015
6.1
6-1
1
19 Nov 2015
6.2
6-1
1
19 Nov 2015
6.3
6-1
1
19 Nov 2015
6.4
6-2
1
19 Nov 2015
6.5
6-3
1
19 Nov 2015
6.6
6-3
1
19 Nov 2015
6.7
6-3-7
1
19 Nov 2015
6.8
6-8
1
19 Nov 2015
6.9
6-9
1
19 Nov 2015
6.10
6-10-11
1
19 Nov 2015
6.11
6-12
1
19 Nov 2015
6.12
6-15
1
19 Nov 2015
6.13
6-15
1
19 Nov 2015
6.14
6-17
1
19 Nov 2015
6.15
6-17
1
19 Nov 2015
19 Nov 2015
iv
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
6.16
6-18
1
19 Nov 2015
6.17
6-21
1
19 Nov 2015
6.18
6-21
1
19 Nov 2015
Chapter 7
7-1
1
19 Nov 2015
7.1
7-1
1
19 Nov 2015
7.2
7-1
1
19 Nov 2015
7.3
7-2
1
19 Nov 2015
7.4
7-2
1
19 Nov 2015
7.5
7-3
1
19 Nov 2015
7.6
7-4
1
19 Nov 2015
Chapter 8
8-1
1
19 Nov 2015
8.1
8-1
1
19 Nov 2015
8.2
8-1
1
19 Nov 2015
8.3
8-2
1
19 Nov 2015
8.4
8-2
1
19 Nov 2015
8.5
8-2
1
19 Nov 2015
8.6
8-3
1
19 Nov 2015
Chapter 9
9-1
1
19 Nov 2015
9.1
9-1
1
19 Nov 2015
9.2
9-1
1
19 Nov 2015
9.3
9-2
1
19 Nov 2015
Figure 9.1
9-3
1
19 Nov 2015
Figure 9.2
9-4
1
19 Nov 2015
9.4
9-5
1
19 Nov 2015
9.5
9-6-7
1
19 Nov 2015
Chapter 10
10-1
1
19 Nov 2015
Chapter 11
11-1
1
19 Nov 2015
1
19 Nov 2015
Chapter 12
19 Nov 2015
v
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
12.1
12-1-3
1
19 Nov 2015
12.2
12-3-4
1
19 Nov 2015
12.3
12-4-5
1
19 Nov 2015
1
19 Nov 2015
Appendices
Appendix 1
App 1-1
1
19 Nov 2015
Appendix 2
App 2-1
1
19 Nov 2015
Appendix 3
App 3-1
1
19 Nov 2015
Appendix 3A
App 3A-1
1
19 Nov 2015
Appendix 4
App 4-1
1
19 Nov 2015
Appendix 5
App 5-1-4
1
19 Nov 2015
Appendix 6
App 6-1-2
1
19 Nov 2015
Appendix 7
App7-1-2
1
19 Nov 2015
Appendix 8
App 8- 1-3
1
19 Nov 2015
Appendix 9
App 9- 1-3
1
19 Nov 2015
Appendix 10
App 10- 1-3
1
19 Nov 2015
Appendix 11
App 11-1-13
1
19 Nov 2015
Appendix 12
App 12-1-14
1
19 Nov 2015
References
Ref 1-1
1
19 Nov 2015
19 Nov 2015
vi
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
TABLE OF CONTENTS
CHAPTER 1
PAGE
NO
1-1
1-7
1.1
1.2
Definitions
Abbreviation
2.1
2.2
2.3
2.4
2-1
2-1
2-2
2-3
Fig
2.1
Introduction
Responsibility of airport operator
Screening during outbreak
Inbound aircraft carrying a suspected case of a communicable disease which
may pose a serious public health risk
Exercises
General guidelines for cabin crew when facing a suspected case of
communicable disease on board
Responsibilities of Cabin Crew
Notification of Suspected Communicable disease, or other Public Health Risk,
on board an aircraft
Notification of Suspected Communicable disease, or other Public Health Risk,
on board an aircraft
3.1
3.2
3.3
3.4
3.5
3.6
3.7
3.8
3.9
3.10
3.11
Disinsection of aircraft
Procedure of disinsection
Disinfection of aircraft
Procedure of disinfection
Disposal of used air sickness containers
Aircraft Interior Cleaning
Special Needs
Precautions against animals transportation in the aircraft
Foodstuffs carriage in aircraft
International certificate of vaccination and prophylaxis
Importation of Radioactive Material
3-1
3-2
3-6
3-6
3-7
3-7
3-10
3-10
3-11
3-11
3-11
2.5
2.6
2.7
2.8
CHAPTER 2
In the event of a communicable disease outbreak
19 Nov 2015
CHAPTER 3
Facilitation of Public Health Provisions
2-4
2-4
2-4
2-6
2-7
vii
Civil Aviation Authority, Bangladesh
3.12
3.13
3.14
3.15
3.16
3.17
3.18
3.19
4.1
4.2
4.3
4.4
4.5
4.6
4.7
4.8
4.9
5.1
5.2
5.3
5.4
5.5
Aviation Public Health Manual
Facilities required for implementation of public health,
Emergency , Medical relief, animal and plant quarantine measures
Passenger amenities in the airport
Relief flights following natural and man-made disasters which seriously
endanger human health when, United Nations (UN) assistance is required
Implementation of International Health Regulations and Related Provisions
Communicable Disease Outbreak National Aviation Plan
Facilitation of the transport of persons with disabilities
Access to airports of disabled persons
Access to air services of disabled persons
CHAPTER 4
Water supply in the airport and in the aircraft
3-12
3-12
3-13
3-13
3-14
3-14
3-15
3-15
Background
Water supply and transfer chain
Figure 4.1: Aircraft potable water supply and Transfer chain
Complying with International Health Regulations (2005)
General Roles and Responsibilities of each component of water supply
Hazards in the water supply chain
Figure 4.2: Sources of water contamination in the transfer chain
Monitoring of potable water supply
Indicators of monitoring water
Frequency of monitoring
Surveillance ( Inspection procedures of the establishment)
4-1
4-1
4-2
4-2
4-3
4-4
4-5
4-6
4-6
4-7
4-7
Background
Requirements for sanitary condition of airports
Design and construction of airports
Airport toilet sanitation
Toilet cleaning
5-1
5-1
5-2
5-2
5-4
19 Nov 2015
CHAPTER 5
Cleaning and disinfection of airport facilities
viii
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
5.6
Toilet cleaning Schedule
5-4
5.7
Vector control in airport
5-4
5.8
Rodent (Rats) control in airport
5-6
5.9
Inspection of airport facilities
5-6
5.10
Cleaning of Public areas in airport
5-7
5.11
Core capacity requirements for designated airports
5-9
Figure 5.1:
PoE core capacity requirements at all times (Routine)
5-10
Figure 5.2:
PoE core capacity requirements (PHEIC)
5-11
CHAPTER 6
Food Safety in aviation
6.1
General
6-1
6.2
Safe food supplies
6-1
6.3
Quality control of food
6-1
6.4
Airport catering establishments
6-2
6.5
Flight catering kitchens
6-3
6.6
Airports Hotel/Restaurants
6-3
6.7
Flight catering premises
6-3
6.8
Food handlers
6-8
Food preparation
6-9
6.10
Prevention of contamination
6-10
6.11
Cleansing and sanitization of dishes and utensils
6-12
6.12
Cleaning of catering premises
6-15
6.13
Food storage in the catering centre
6-15
6.14
Laboratory facilities at flight catering establishment
6-17
6.15
Transportation of food to the aircraft
6-17
6.16
Preservation of food in the aircraft
6-18
6.17
Inspection of flight catering centre
6-21
6.18
Solid waste disposal
6-21
6.9
19 Nov 2015
ix
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
CHAPTER 7
Medical supplies in the aircraft
7.1
Introduction
7-1
7.2
First aid kits and Universal precaution kits
7-1
7.3
Emergency medical kit- Aeroplanes
7-2
7.4
Oxygen storage and dispensing apparatus
7-2
7.5
Contents of first aid kit and universal precaution kit
7-3
7.6
Contents of Emergency medical kit- Aeroplane
7-4
CHAPTER 8
Medical support during aircraft accident
8.1
Actions by medical services during aircraft accident on the airport
8-1
8.2
Actions by designated hospitals
8-1
8.3
Actions by medical services during aircraft accident off the airport
8-2
8.4
Actions by designated hospitals
8-2
8.5
Provisions of medical services during aircraft emergency
8-2
8.6
Hospitals
8-3
CHAPTER 9
Triage and Medical care
9.1
Immediate need for care of injured in aircraft accidents
9-1
9.2
Triage Principles (all emergencies)
9-1
9.3
Standardized casualty identification tags and their use
9-2
9.1 Figure :Casualty Identification Tag
9-3
9.2 Figure :Casualty Identification Tag
9-4
9.4
Care Principles
9-5
9.5
Control of flow of the injured
9-6
19 Nov 2015
x
Civil Aviation Authority, Bangladesh
12.1
12.2
12.3
Aviation Public Health Manual
CHAPTER 10: Care of ambulatory survivors
10-1
CHAPTER 11: Care of Fatalities
11-1
CHAPTER 12
Airport Medical Services
General
Airport Medical Care Facilities/First aid room
Airport without a medical care
19 Nov 2015
12-1
12-3
12-4
xi
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
APPENDICES
Appendices
SUBJECT
PAGE
NO
Appendix 1
Aircraft General declaration
App 1-1
Appendix 2
Certificate of Residual disinfection
App 2-1
Appendix 3
Public Health Passenger Locator Card
App 3-1
Appendix 3A
Public Health Passenger Locator Card (CAAB Approved)
Appendix 4
Appendix 5
Model International certificate of vaccination or prophylaxis
Inspection checklist for evaluating the sanitation status and
implementation of international health regulations (IHR) to airports
Appendix 6
Medical (Cabin) Inspection Checklist
Appendix 7
Inspection of airline service area or Transfer point
Appendix8
On-site Inspection to assess the cleaning status of the aircraft
Appendix 9
Inspection checklist of flight catering service center
Appendix 10
Inspection checklist for flight catering food preparation, Storage
and transportation
State and Airport assistance visit checklist from ICAO-CAPSCA
Appendix 11
Appendix 12
Standard operating procedure (SoP) for HSIA when infectious
disease threat is reported on arriving aircraft
References
Serial no 1 to 13
19 Nov 2015
App 3A-1
App 4-1
App 5-1
to 5-4
App 6-1
to 6-2
App 7-1
to 7-2
App 8-1
to 8-3
App 9-1
to 9-3
App 10-1
to 10-3
App 11-1
to 11-13
App 12-1
to 12-14
Ref 1-1
xii
Civil Aviation Authority, Bangladesh
SL NO
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
Aviation Public Health Manual
DISTRIBUTION LIST
INTERNAL
Chairman, CAAB
Member (Operations and Planning), CAAB
Chief Engineer, CAAB
Director, Flight Safety and Regulations, CAAB
Director, Hazrat Shahjalal International Airport, Dhaka
Superintending Engineer (Civil), CAAB
Superintending Engineer ( (E/M), CAAB
Airport Manager, Shah Amanat International Airport, Chittagong
Airport Manager, Osmani International Airport, Sylhet
Airport Managers - Cox’s Bazar Airport, Jessore Airport, Saidpur
Airport, Barisal Airport, Shah Makhdum Airport,Rajshahi
Medical Assessor, CAAB
Civil Aviation Training Centre (CATC)
Master Copy, CAAB
Technical Library, CAAB
EXTERNAL
Chairman AOC, HSIA
Managing Director, Biman Bangladesh Airlines
Managing Director, Regent Airways
Managing Director, United Airways (BD) Ltd
Managing Director, NovoAir
Managing Director ,US-Bangla Airlines
Bangladesh Airlines Training Centre(BATC)
Airport Health Officer, Airport Health Department, HSIA
Director, IEDCR, Director General of Health Services
Director(Disease Control), Director General of Health Services
Deputy Director, Plant Quarantine Station, HSIA
Project Director, Livestock Quarantine Station, HSIA
Biman Flight Catering Centre (BFCC), HSIA
Flight Catering Centre- Regent Airways, United Airways (BD) Ltd, ,
NovoAir, US-Bangla Airlines
19 Nov 2015
COPY NO
01
02
03
04
05
06
07
08
09
10-14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32-35
xiii
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
THIS PAGE INTENTIONALLY LEFT BLANK
19 Nov 2015
xiv
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
FOREWORD
With the increased growth in international travel and trade and the emergence and reemergence
of international disease threats and other public health risks, International Civil Aviation
Organization (ICAO) published ICAO Health Related SARPs and Documents (Annexes 6, 9, 11,
14, Procedures for Air Navigation Services- Air Traffic Management (PANS-ATM, Doc 4444).
Airports Council International (ACI) and International Air Transport Association (IATA)
provided necessary guidelines for the protection of health of passengers, crews and the personnel
working at the airports. WHO had also published a guide in 2009, “Hygiene and Sanitation in
aviation” for use by the health professionals in each member state with a view to clarify the
ultimate responsibility for the safety of food, water and proper handling of wastes in
international airports. Keeping all these in view, Civil Aviation Authority, Bangladesh has
extended its all out efforts to meet these challenges and keep the airports safe- “ to prevent,
protect against , control and provide a public health response to the international spread of
communicable diseases in ways that are commensurate with and restricted to public health risks,
and which avoid unnecessary interference with international traffic and trade”.
In pursuance of the powers conferred upon the Chairman, CAA, Bangladesh vide Rule 214 of
CAR 84, the Chairman is pleased to approve this Aviation Public Health Manual - Ist Edition
2015 which is a guidance material for the stakeholders involved in airports and airlines activities.
The Manual will be beneficial to the airports and airlines operators and other stakeholders in
aviation to ensure a safe environment for travelers using points of entry facilities.
This Manual is also a guidance material for the airport medical authority to deal with routine
medical emergencies which normally occur at the airport and also in possible aircraft accidents.
It shall have immediate effect.
19 Nov 2015
xv
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
- BLANK PAGE -
19 Nov 2015
xvi
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
-BLANK PAGE-
19 Nov 2015
i
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
-BLANK PAGE-
19 Nov 2015
xiv
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
CHAPTER 1
1.1
Definitions
The following definitions are required to know when you go through the different chapters of
this Aviation Public Health Manual.
Admission: The permission granted to a person to enter a State by the public authorities of that
State in accordance with international laws.
Advance Passenger Information (API) System: An electronic communications system
whereby required data elements are collected and transmitted to border control agencies prior to
flight departure or arrival and made available on the primary line at the airport of entry.
Affected area: Means a geographical location specifically for which health measures have been
recommended by WHO under IHR.
Affected: Means a person, baggage, cargo, containers, conveyances, goods, postal parcel, or
human remains that are infected or contaminated, or carry sources of infection, so as to constitute
a public health risk.
Aircraft equipment: Articles, including first-aid and survival equipment and commissary
supplies, but not spare parts or stores, for use on board an aircraft during flight.
Aircraft operator: A person, organization or enterprise engaged in or offering to engage in an
aircraft operation.
Airline: As provided in Article 96 of the Convention, any air transport enterprise offering or
operating a scheduled international air service.
Authorized agent: A person who represents an aircraft operator and who is authorized by or on
behalf of such operator to act on formalities connected with the entry and clearance of the
operator’s aircraft, crew, passengers, cargo, mail, baggage or stores and includes, where national
law permits, a third party authorized to handle cargo on the aircraft.
Backflow: Flow of water or other liquids, mixtures or substances into the distribution pipes of a
potable supply of water from any source or sources other than the potable water supply. Backsiphonage is one form of backflow.
Backflow preventer: Approved backflow prevention plumbing device that would typically be
used on potable water distribution lines where there is a direct connection or mixtures or
substances from any source other than the potable water supply. Some devices are designed for
use under continuous water pressure, whereas others are non-pressure types.
Back-siphonage: Backward flow of used contaminated or polluted water from a plumbing
fixture or vessel or other source into a water supply pipe as a result of negative pressure in the
pipe.
Baggage: Personal property of passengers or crew carried on an aircraft by agreement with the
operator.
19 Nov 2015
Page 1-1
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
Biohazard bag: Bag used to secure biohazard waste that requires microbiological inactivation in
an approved manner for final disposal. Such bags must be disposable and impervious to moisture
and have sufficient strength to preclude tearing or bursting under normal conditions of usage and
handling.
Cleaning: Removal of visible dirt or particles through mechanical action, normally undertaken
on a routine and frequent basis. The cleaning process and some products used for cleaning also
result in disinfection.
Competent authority: Authority responsible for the implementation and application of health
measures under International Health Regulations (2005).
Control measures: Those steps in the drinking-water supply that directly affect drinking-water
quality and that collectively ensure that drinking-water consistently meets health-based targets.
They are activities and processes applied to prevent hazard occurrence.
Cross-connection: Any unprotected actual or potential connection or structural arrangement
between a potable water plumbing system and any other source or system through which it is
possible to introduce into any part of the potable system any used water, industrial fluid, gas or
substance other than the intended potable water with which the system is supplied. Bypass
arrangements, jumper connections, removable sections, swivel or change-over devices and other
temporary or permanent devices through which backflow can occur are considered to be crossconnections.
Cargo: Any property carried on an aircraft other than mail, stores and accompanied or
mishandled baggage, other safety-related aspects, and security-related aspects, of air transport
operations. Provision of services during flights, in particular for catering, and for the comfort of
passengers.
Communicable disease: It is taken to include those diseases resulting from infections by
transmissible agents such as viruses and bacteria, and that have the potential to cause a serious
public health risk or emergency of international concern.
Crew member: A person assigned by an operator to duty on an aircraft during a flight duty
period.
Contamination: Presence of an infectious or toxic agent or matter on a human or animal body
surface, in or on a product prepared for consumption or on other inanimate objects, including
conveyances that may constitute a public health risk.
Conveyance: An aircraft, ship, train, road vehicle or other means of transport on an international
voyage.
Core capacity: Capacities listed at Annex 1 of IHR (2005).
Decontamination: Means a procedure whereby health measures are taken to eliminate an
infectious or toxic agent or matter on a human or animal body surface, in or on a product
prepared for consumption or on other inanimate objects, including conveyances, that may
constitute a public health risk;
19 Nov 2015
Page 1-2
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
Deratting: Means the procedure whereby health measures are taken to control or kill rodent
vectors of human disease present in baggage, cargo, containers, conveyances, facilities, goods
and postal parcels at the point of entry
Diseases: Means an illness or medical condition, irrespective of origin or source, that presents or
could present significant harm to humans;
Disembarkation: The leaving of an aircraft after landing, except by crew or passengers
continuing on the next stage of the same through-flight.
Disinfection: The procedure whereby health measures are taken to control or kill infectious
agents on a human or animal body, in or on affected parts of aircraft, baggage, cargo, goods or
containers, as required, by direct exposure to chemical or physical agents.
Disinsection; The procedure whereby health measures are taken to control or kill insects present
in aircraft, baggage, cargo, containers, goods and mail.
Embarkation: The boarding of an aircraft for the purpose of commencing a flight, except by
such crew or passengers as have embarked on a previous stage of the same through-flight.
Emergency preparedness: Programme of long term activities whose goal is to strengthen the
overall capacity and capability of a country or a community to manage efficiently all types of
emergencies and bring about an orderly transition from relief through to recovery.
Flight crew member: A licensed crew member charged with duties essential to the operation of
an aircraft during a flight duty period.
Free pratique: Permission of an aircraft after landing, to embark or disembark, discharge or
load cargo or stores.
Food handling area: Any area where food is stored, processed, prepared or served.
Food preparation area: Any area where food is processed, cooked or prepared for service.
Food service area: Any area where food is presented to passengers or crew members (excluding
individual cabin service).
Food storage area: Any area where food or food products are stored.
Food transport area: Any area through which unprepared or prepared food is transported
during food preparation, storage and service operations (excluding individual cabin service).
Health Measure: Means procedures applied to prevent the spread of diseases of contamination;
a health measure does not include law enforcement or security measure.
Ill person: Means an individual suffering from or affected with a physical ailment that may pose
a public health risk;
Infection: Means the entry and development or multiplication of an infectious agent in the body
of humans and animals that may constitute a public health risk;
19 Nov 2015
Page 1-3
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
International traffic: Means the movement of persons, baggage, cargo, containers,
conveyances, goods or postal parcels across an international border, including international trade.
Inspection: The examination, by competent authority or under its supervision, of areas,
baggage, containers, conveyances, facilities, goods or postal parcels, including relevant data and
documentation, to determine if a public health risk exists.
Narcotics control: Measures to control the illicit movement of narcotics and psychotropic
substances by air.
Personal protective equipment: Equipment and materials used to create a protective barrier
between a worker and the hazards in the workplace.
Potable water: Fresh water that is intended for drinking, washing or showering; for handling,
preparing or cooking food; and for cleaning food storage and preparation areas, utensils and
equipment. Potable water, as defined by the WHO Guidelines for drinking-water Quality, does
not represent any significant risk to health over a lifetime of consumption, including different
sensitivities that may occur between life stages.
Potable water tanks: All tanks in which potable water is stored for distribution and use as
potable water.
Public health authority: Government agency or designee responsible for the protection and
improvement of the health of entire populations through community-wide action.
Public health surveillance: The ongoing, systematic collection, analysis and interpretation of
data about specific environmental hazards, exposure to environmental hazards and health effects
potentially related to exposure to environmental hazards, for use in the planning, implementation
and evaluation of public health programmes.
Passenger amenities: Facilities provided for passengers which are not essential for passenger
processing.
Person with disabilities: Any person whose mobility is reduced due to a physical incapacity
(sensory or locomotors), an intellectual deficiency, age, illness or any other cause of disability
when using transport and whose situation needs special attention and the adaptation to the
person’s needs of the services made available to all passengers.
Pilot-in-command: The pilot responsible for the operation and safety of the aircraft during
flight time.
Point of entry: Means a passage for international entry and exit of travelers, baggage, cargo,
containers, conveyances, goods and postal parcels as well as agencies and areas providing
services to them on entry or exit.
19 Nov 2015
Page 1-4
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
Public health emergency of international concern: An extraordinary event which is
determined, as provided in the International Health Regulations (2005) of the World Health
Organization: (i) to constitute a public health risk to other States through the international spread
of disease and (ii) to potentially require a coordinated international response
Public health risk: A likelihood of an event that may affect adversely the health of human
populations, with an emphasis on one which may spread internationally or may present a serious
and direct danger.
Quarantine: Means the restriction of activities and/or separation from others of suspect persons
who are not ill or of suspect baggage, containers, conveyances or goods in such a manner as to
prevent the possible spread of infection or contamination;
Relief flights: Flights operated for humanitarian purposes which carry relief personnel and
relief supplies such as food, clothing, shelter, medical and other items during or after an
emergency and/or disaster and/or are used to evacuate persons from a place where their life or
health is threatened by such emergency and/or disaster to a safe haven in the same State or
another State willing to receive such persons.
Reservoir: Means an animal, plant or substance in which an infectious agent normally lives and
whose presence may constitute a public health risk;
Rodent: Any of the relatively small placental mammals that constitute the order Rodentia,
having constantly growing incisor teeth specialized for gnawing. The group includes rats, mice,
squirrels, marmots, etc
Surveillance: Means the systematic ongoing collection, collation and analysis of data for public
health purposes and the timely dissemination of public health information for assessment and
public health response as necessary;
Suspect: Means those persons, baggage, cargo, containers, conveyances, goods or postal parcels
considered by a State Party as having been exposed, or possibly exposed, to a public health risk
and that could be a possible source of spread of disease;
Sewage: Any liquid waste that contains animal or vegetable matter in suspension or solution,
including liquids that contain chemicals in solution.
Transfer point: Site of intermittent connection for water transfer between the hard-plumbed
airport water distribution system and the aircraft water system. Sometimes referred to as
Watering point.
Traveller: Means a natural person undertaking an international voyage;
Turbidity: Light-scattering cloudiness or lack of transparency of a solution due to the presence
of suspended particles. Turbidity is not necessarily visible to the eye.
Vector: Means an insect or other animal which normally transports an infectious agent that
constitutes a public health risk;
19 Nov 2015
Page 1-5
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
Visitor: Any person who disembarks and enters the territory of a Contracting State other than
that in which that person normally resides; remains there lawfully as prescribed by that
Contracting State for legitimate non-immigrant purposes, such as touring, recreation, sports,
health, family reasons, religious pilgrimages, or business; and does not take up any gainful
occupation.
Water supply surveillance: Continuous and vigilant public health assessment and review of the
safety and acceptability of drinking-water supplies. There are two types of approaches: auditbased approaches and approaches relying on direct assessment. In the audit approach, assessment
activities, including verification testing, are undertaken largely by the supplier, with third-party
auditing to verify compliance. In direct assessment, the drinking-water supply surveillance
agency carries out independent testing of water supplies.
WHO IHR Contact Point: The unit within WHO that is accessible at all times for
communication with the national IHR Focal Points.
19 Nov 2015
Page 1-6
Civil Aviation Authority, Bangladesh
1.2
Aviation Public Health Manual
Abbreviation
AFTN -Aeronautical Fixed Telecommunication Network
AHO -Airport Health Officer
ACI -Airports Council International
ANO -Air Navigation Order
App -Appendix
ATM -Air Transport Management
ATS -Air Traffic Services
CAAB -Civil Aviation Authority, Bangladesh
CARs -Civil Aviation Rules
CMH -Combined Military Hospital
CAPSCA-Collaborative Arrangement for the Prevention and Management of Public Health
Events in Civil Aviation
CMT -Crisis Management Team
Doc -Document
DGHS -Director General of Health Services
DMCH- Dhaka Medical College Hospital
ECR -Environmental Conservation Rules
HERT -Health Emergency Response Team
HSIA -Hazrat Shahjalal International Airport
ICAO -International Civil Aviation Organization
IHR -International Health Regulations
IATA -International Air Transport Association
IEDCR-Institute of Epidemiology, Disease control and Research
OIA -Osmani International Airport
PANS -Procedures of Air Navigation Services
PHEIC -Public Health Emergency of International Concern
PIC -Pilot- in- Command
PLC -Passenger Locator Card
PoE -Point of Entry
PPE -Personal Protective Equipment
Ref - Reference
SAIA -Shah Amanat International Airport
SoP -Standard Operating Procedures
SARPS-Standards and Recommended Practices
WHO -World Health Organization
19 Nov 2015
Page 1-7
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
THIS PAGE INTENTIONALLY LEFT BLANK
19 Nov 2015
Page 1-8
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
CHAPTER 2
In the event of a communicable disease outbreak
2.1
Introduction
2.1.1
In the event of an outbreak of communicable disease on an international level, air travel
will be the focus of much attention due to the potential for aviation to increase the rate at
which a disease spreads, thereby decreasing the time available for preparing
interventions. Advance preparation should make it possible to reduce the consequences.
2.1.2
Airport operators are to protect the health and look into the welfare of travellers, staff and
the public and to take necessary steps to reduce the opportunities for dissemination of
communicable diseases by air.
2.2
Responsibility of airport operator
The following measures are to be taken by airport operators and health authorities against
communicable diseases that might pose a serious risk to public health:
2.2.1
The responsibility for management of the risk of communicable diseases at airports rests
with the public health authority and the relevant airport operator.
2.2.2
The airport authority is to make available adequate supplies of appropriate personal
protective equipment (including hand-washing facilities or sanitizing gels) for airport
staff.
2.2.3
Travelers and health professionals should have access to consistent information about
postponing travel and screening measures that may be in place at an airport, should a
potential traveler have an illness prior to commencing air travel. Such information will
usually be taken from a public health information site or developed in close collaboration
with the public health authority.
2.2.4
Before arrival at the airport terminal building, information can be provided to travellers
by means of an airport/ airline web site or by electronic link to a public health web site by
recorded telephone message or by printed media. A telephone message may give health
information directly and possibly refer the listener to further sources of information.
2.2.5
The media can play a useful role in informing travellers of the situation at an airport and
links with the media should be established so that journalists can obtain information at
short notice. Notices on radio and television stations and public information delivered
through other forms of mass media e.g. internet, can be very effective.
2.2.6
Travelers who have medical conditions that may affect their fitness for travelling should
have their attending physician complete the International Air Transport Association
Medical Information Form (“MEDIF”, or the equivalent form in use by the airline) or
discuss the situation with the airline ticketing/reservations staff who will forward the
enquiry to appropriate medical staff.
19 Nov 2015
Page 2-1
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
2.2.7 The information shall be given by signage, stands, posters or electronic displays in the
airport. The text would be adjusted according to the information to be conveyed. The
WHO or national public health authority will provide the information on symptoms
2.2.8
Public announcements, and other forms of communication, should be provided in the
languages used by persons most frequently travelling through the airport, including
English, as well as the State’s own language(s).
2.2.9
To ensure public confidence, airport operators should explain to passengers, as fully as
possible, the reasons for any necessary health-related measures.
2.3
Screening during outbreak
2.3.1
According to WHO, screening for communicable diseases can potentially reduce
opportunities for transmission and forestall or delay international spread. Depending on
the epidemiology, extent of transmission and severity of the disease (attack and mortality
rates), screening of arriving and departing travellers at international airports may be
considered.
2.3.2
Screening measures that match the behavior of the communicable disease in question
have the greatest chance of reducing the number of cases and limiting or preventing
international spread.
2.3.3
Screening methods include visual inspection, questionnaire and temperature
measurement using thermal scanners, infra-red-thermometer etc or any other method
recommended by WHO.
2.3.4
If the National public health authority determines that screening is to be employed, it
should discuss the issues with the airport operator in order to develop acceptable plans.
Costs associated with providing screening equipment shall normally be met by the
national public health authority
2.3.5
Travellers determined at screening to be at increased risk of having a communicable
disease posing a potentially serious public health risk should undergo secondary
screening by a medical practitioner. If the assessment is positive i.e. the traveller is
thought to be suffering from a communicable disease which poses a serious public health
risk, consideration should be given to prevent his/her departure. Such a decision should
not be taken lightly and has legal implications that need to be adequately considered in
preparedness planning. (IHR (2005) Articles 23.3, 23.5, 31 and 32 cover health measures
for arriving and departing travellers, including requirements for minimizing discomfort
and distress for passengers that are at risk of a communicable disease). appropriate
diagnosis, and management, in accordance with the IHR (2005) with a view to protecting
the public from potential infection i.e. by isolation or quarantine. Appropriate isolation or
quarantine facilities should be identified by the public health authority and to be sited
away from the airport site. Travellers arriving or departing from an ‘at risk’ area should
be provided with the available information about risks, risk avoidance, symptoms
associated with the disease and when and where to report should these symptoms
develop.
19 Nov 2015
Page 2-2
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
2.4
Inbound aircraft carrying a suspected case of a communicable disease
which may pose a serious public health risk
2.4.1
A number of considerations should be taken into account when an aircraft arrives
carrying a suspected case of a communicable disease which may pose a serious public
health risk. These include the following points.
2.4.2 The pilot in command (PIC) needs to be advised of where to park the aircraft, such
information will normally be communicated to the PIC by air traffic control. This may be
on a remote stand, or, depending on the situation, on the apron with or without a
passenger boarding bridge attached. Such aircraft should be parked at stands which have
all the relevant facilities, enable continued ventilation of the aircraft and allow easy
accessibility to public health personnel to assess any suspect case(s) and permit efficient
clearance of passengers.
2.4.3
Action should be taken to disembark the travellers as soon as possible after the situation
has been evaluated and a public health response has been instituted, if needed.
2.4.4
Personal protective equipment (PPE) appropriate to the suspected communicable disease,
the mode of transmission and the nature of duties being performed by aviation personnel,
should be worn. For many communicable diseases, disposable gloves and good hand
hygiene (at times in combination with surgical masks) are sufficient. The national public
health authority may provide detailed recommendations.
2.4.5
A traveller having a communicable respiratory disease should wear a surgical mask
unless the traveller is unable to tolerate it.
2.4.6
All surfaces that may have been in contact with a sick traveller need to be appropriately
treated. Removable materials should be handled with biohazard precautions.
2.4.7
A sick traveller should be appropriately escorted from the aircraft to an area for further
assessment/treatment. Appropriate infection control measures should be applied. The
IHR (2005), Annex 1B outlines the core capacity requirements regarding transport
facilities needed to manage public health emergencies, including the designation of
ambulances for the transport of cases of infectious disease from a flight.
2.4.8
Before disembarkation, travellers and crew on the same aircraft as the sick traveller
should be segregated from other travellers until traveller seating details, contact details
and destination have been obtained and they have been advised by public health authority
staff of any necessary precautionary measures.
2.4.9
Procedures need to be in place for obtaining baggage, customs and security clearance of a
sick traveller, and other travellers. There is currently no evidence to support the cleaning
and/or disinfection of baggage belonging to a suspected case or his/her contacts.
2.4.10 Consideration should be given to the comfort of all passengers, particularly if placed in
isolation, or detained on board the aircraft. Provision should be made for food, water and
other essentials.
19s Nov 2015
Page 2-3
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
2.4.1.11A procedure for transporting a sick traveller to hospital needs to be in place.
2.5
Exercises:
Airport operators should establish a method of testing their preparedness by means of
drills/exercises involving all relevant stakeholders, especially public health authorities,
airport operators and airlines.
(Ref: Airport preparedness guidelines for outbreaks of communicable disease issued by
ACI and ICAO in April 2009).
2.6
General guidelines for cabin crew when facing a suspected case of
communicable disease on board:
2.6.1
The following are general guidelines for cabin crew when facing a suspected case of
communicable disease on board.
2.6.2
A communicable disease is suspected when a traveller (passenger or a crewmember) has
a fever (temperature 38°C/100°F or greater) associated with one or more of the following
signs or symptoms:
Appearing obviously unwell
Persistent coughing
Impaired breathing
Persistent diarrhea
Persistent vomiting
Skin rash
Bruising or bleeding without previous injury
Confusion of recent onset
Note 1:This list of signs and symptoms is identical to that listed in the Health part of the
ICAO Aircraft General Declaration (Appendix1) and in the World Health Organization
nd
International Health Regulations (2005) 2 Edition.
Note 2: If food poisoning from in-flight catering is suspected, proceed as per companyestablished protocol. The captain still has to follow the ICAO procedure mentioned in
chapter 2.7.15 below.
Note 3: If temperature of the affected person is normal but several travellers have similar
symptoms, think of other possible public health issues such as chemical exposure.
2.7
Responsibilities of Cabin Crew
2.7.1
If medical support from the ground is available, contact that ground support immediately
and/or page for medical assistance on board (as per company policy).
2.7.2
If medical ground support and/or on board health professional is available, crew should
follow their medical advice accordingly.
19 Nov 2015
Page 2-4
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
2.7.3
If no medical support is available, relocate the ill traveller to a more isolated area but
only if two rows can be cleared immediately in front of a solid bulkhead. If the ill
traveller is relocated, do not reuse the vacated seat and make sure that the cleaning crew
at destination is advised to clean and disinfect both locations.
2.7.4
Designate one cabin crew member to look after the ill traveller, preferably the crew
member that has already been dealing with this traveller. More than one cabin crew
member may be necessary if more care is required.
2.7.5
When possible, designate a specific lavatory for the exclusive use of the ill traveler. If not
possible, clean and disinfect the commonly touched surfaces of the lavatories ( Faucet,
door handles, waste bin cover, counter top) after each use by the ill traveller.
2.7.6
If the ill traveller is coughing, ask him/her to follow respiratory etiquette:
2.7.7
Provide tissues and advice to use the tissues to cover the mouth and nose when speaking,
sneezing or coughing.
2.7.8
Advise the ill traveller to practice proper hand hygiene∗. If the hands become visibly
soiled, they must be washed with soap and water.
2.7.9
Provide an airsickness bag to be used for the safe disposal of the tissues.
2.7.10 If a face mask is available, the ill traveller should be asked to wear it. As soon as it
becomes damp/humid, it should be replaced by a new one. These masks should not be
reused and must be disposed safely after use. After touching the used mask (e.g., for
disposal), proper hand hygiene must be practiced immediately.
2.7.11 If the ill traveller cannot tolerate a mask or refuses it, the designated cabin crew
member(s) or any person in close contact (less than 1 metre) with the ill person should
wear a mask. The airline should ensure that their cabin crewmembers have adequate
training in its use to ensure they do not increase the risk (for example by more frequent
hand-face contact or by mask adjustment, or by repeatedly putting it on and off.)
2.7.12 If there is a risk of direct contact with body fluids, the designated cabin crew member
should wear disposable gloves. Gloves are not intended to replace proper hand hygiene
and hands should be washed with soap and water. An alcohol-based hand rub can be used
if the hands are not visibly soiled. 8.10 Store soiled items (used tissues, face masks,
oxygen mask and tubing, linen, pillows, blankets, seat pocket items, etc.) in a biohazard
bag if one is available. If not, use a sealed plastic bag and label it “biohazard”.
2.7.1
Any similar symptoms.
2.7.14 Ensure hand carried cabin baggage follows the ill traveller.
19 Nov 2015
Page 2-5
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
2.7.15
As soon as possible, advise the captain of the situation because he/she is required by the
International Civil Aviation Organization regulations (ICAO Annex 9, Chapter 8, and
paragraph 8.15) and the World Health Organization International Health Regulations
(WHO IHR 2005, Article 28(4)) to report the suspected case(s) to air traffic control.
Also remind the captain to advise the destination station that cleaning and disinfection
will be required.
2.7.16
Ask all travellers seated in the same row, 2 rows in front and 2 rows behind the sick
traveller to complete a passenger locator card. Cards are to be made available in the
aircraft or in the airport by the public health authority when there is declaration of
public health emergency of international concern (PHEIC) by WHO.
2.7.17
It is advisable of washing one’s hands with soap and water for at least 15 seconds.
Touching the face with hands should be avoided. Hands should be washed frequently.
(Ref: IATA General Guidelines for cabin crew on suspected communicable disease, Oct
2011).
2.8
Notification of Suspected Communicable diseases or other Public
Health Risk, on board an aircraft
2.8.1
The flight crew of an aircraft shall, upon identifying a suspected case(s) of
communicable disease, or other public health risk, on board the aircraft, promptly notify
the ATS unit with which the pilot is communicating, the information listed below:
aircraft identification;
departure aerodrome;
destination aerodrome;
estimated time of arrival;
number of persons on board;
number of suspected case(s) on board; and
nature of the public health risk, if known.
2.8.2
The ATS unit, upon receipt of information from a pilot regarding suspected case(s) of
communicable disease, or other public health risk, on board the aircraft, shall forward a
message as soon as possible to the ATS unit serving the destination/departure, unless
procedures exist to notify the appropriate authority designated by the State, and the
aircraft operator or its designated representative.
2.8.3
When a report of a suspected case(s) of communicable disease, or other public health
risk, on board an aircraft is received by an ATS unit serving the destination/departure,
from another ATS unit or from an aircraft or an aircraft operator, the unit concerned
shall forward a message as soon as possible to the public health authority (PHA)/airport
authority/aircraft operator and the aerodrome authority
Note 1:
The information to be provided to the departure aerodrome will prevent
the potential spread of communicable disease, or other public health risk, through other
aircraft departing from the same aerodrome.
19 Nov 2015
Page 2-6
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
Note 2:AFTN (urgency message), telephone, facsimile or other means of transmission may be
used .
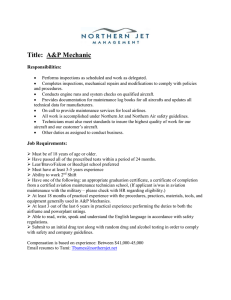
Figure 2.1:
Notification of suspected communicable disease, or other public health risk, on
board an aircraft.
(Ref:
Procedures for Air Navigation Services-Air Traffic Management,
Doc 4444, Chapter 16.6)
19 Nov 2015
Page 2-7
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
THIS PAGE INTENTIONALLY LEFT BLANK
19 Nov 2015
Page 2-8
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
CHAPTER 3
Facilitation of Public Health Provisions
3.1
Disinsection of aircraft
3.1.1
All the Bangladeshi registered airlines shall limit any routine requirement for the
disinsection of aircraft cabins and flight decks with insecticide aerosol while passengers
and crews are on board, to same-aircraft operations originating in, or operating via,
territories that they consider to pose a threat to their public health, agriculture or
environment.
3.1.2
Air operator shall periodically review its requirement for disinsection of aircraft and
modify them, as appropriate, in the light of all available evidence relating to the
transmission of insects to their respective territories via aircraft.
3.1.3
When disinsection is required it shall authorize or accept only those methods, whether
chemical or non-chemical, and/or insecticides, which are recommended by the World
Health Organization and are considered efficacious by the State.
Note: — This provision does not preclude the trial and testing of other methods for
ultimate approval by the World Health Organization.
3.1.4
Airlines shall ensure that their procedures for disinsection are not injurious to
of passengers and crew and cause the minimum discomfort to them.
the health
3.1.5
State shall, upon request, provide to aircraft operators appropriate information, in plain
language, for air crew and passengers, explaining the pertinent national regulation, the
reasons for the requirement, and the safety of properly performed aircraft disinsection.
3.1.6
When disinsection has been performed in accordance with procedures recommended by
the World Health Organization, concerned authority shall accept a pertinent certification
on the General Declaration as provided for in Appendix 1or, in the case of residual
disinsection, the Certificate of Residual Disinsection set forth in Appendix 2 in this
Manual.
3.1.7
When disinsection has been properly performed and a certificate is presented or made
available to the public authorities in the country of arrival, the authorities shall normally
accept that certificate and permit passengers and crew to disembark immediately from the
aircraft.
3.1.8
Air operator is to ensure that insecticide used for disinsection of the aircraft shall not
have a deleterious effect on the structure of the aircraft or its operating equipment.
Flammable chemical compounds or solutions likely to damage aircraft structure, such as
by corrosion, shall not be employed.
(Ref:
19 Nov 2015
Annex 9, Chapter 2, article 2.23-2.30)
Page 3-1
Civil Aviation Authority, Bangladesh
3.2
Procedure of Disinsection:
3.2.1
Introduction:
Aviation Public Health Manual
Disinsection of the aircraft is to be carried out in such a manner that passengers do not
undergo any discomfort or suffer any injury to health that no damage is done to the
structure or operating equipment of the aircraft. As far as possible, the aircraft should be
disinfected using methods approved by WHO. As Bangladesh is malaria and other
mosquito borne disease prone area disinsection to be done as per International Health
Regulations when the aircraft leave our international airports for an area where these
vectors have been eradicated. The same requirement applies to aircraft leaving an airport
in an area where the transmission of malaria or other mosquito borne diseases is
occurring. Disinsection is also permitted at the airport of arrival if it is not carried out
satisfactorily.
3.2.2 WHO recommended insecticides
Natural pyrethrins
d-Phenothrin
permethrine
3.2.3 Procedure of spraying
Following three points must be observed during disinsection of the aircraft:
Disinsection must only take place when all crew and passengers have disembarked.
There must be an assurance from the authorities using the insecticide that it will have no
harmful residual effects on the aircraft structure.
After disinsecting, an adequate amount of time must be allowed to ventilate the aircraft
before boarding begins.
3.2.4 WHO Recommended Disinsection Procedures
3.2.4.1 “Blocks away” Disinsection
This procedure takes place prior to take off, when disinsection is required, after
passengers have boarded and the doors have been closed.
The aircraft is treated by crew members walking through the cabins and discharging
Approved single shot aerosols containing quick-acting ―knock-down‖ insecticides based
on either 2% d-Phenothrin or permethrine.
Spraying is to be carried out at a rate of 35 g of formulation per 100 m3 (10 g per 1000
ft3).
Prior to disinsection the procedure should be announced and the passengers should be
advised to close their eyes and/or cover their faces for a few seconds whilst the procedure
is carried out if they feel that it may cause them inconvenience.
For disinsection to be effective, the aircraft air conditioning system must be turned off
whilst spraying is carried out, and the crew must treat all possible insect harborages
19 Nov 2015
Page 3-2
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
including toilets, galleys and wardrobes unless these areas have been sprayed together
with the flight-deck prior to the boarding. Foodstuffs and galley utensils should be
protected from contamination.
The flight deck is sprayed prior to boarding by the crew.
Cargo holds, wheel wells and all other parts of the aircraft accessible from the outside
only, in which insects can find shelter are to be disinsected by ground staff as near as
possible to the time the aircraft leaves the apron.
Stations requiring “Blocks-away” disinsecting should have four aerosol dispensers, two
for use and two spares in case of malfunction. The dispensers are marked with a serial
number. Only the numbers of the used dispensers are entered on the Health Part of the
Aircraft General Declaration.
The empty aerosol dispensers must be retained and upon the aircraft’s arrival at its
destination, must be produced along with the General Declaration to the Port Health
Authority as evidence of disinsecting. If after the disinsecting procedure has been
completed, the flight is aborted and the doors are opened when the aircraft returns to the
ramp, the procedure must be repeated before the next take-off.
Although not regarded as a preferred method, the on-arrival-method may be retained as
an acceptable back-up method if an aircraft, coming from areas of threat, has not been
adequately disinsected by any of the recommended methods.
3.2.4.2 Pre-flight and Top-of-descent Spraying
This two-step method is similar to the blocks-away except that the aircraft is first sprayed
on the ground with an aerosol containing a residual insecticide before passengers and
crew board the aircraft.
3.2.4.2.1 Pre-flight spraying
The pre-flight spray containing 2% permethrine must be applied to the flight deck, all
toilet areas, lockers, wardrobes and crew rest areas, except where approval has been
granted for the residual treatment (see below) of these areas. Pre-flight spraying of the
residual insecticide shall equate to a rate of 35 g of the formulation per 100 m3 (10 g per
1000 ft3).
3.2.4.2.2 Top-of-descent (In-flight) spraying
The second step of this method is carried out at top-of-descent ( in-flight spraying) as the
aircraft starts its descent to the airport of arrival.
A quick-acting knock-down‖ insecticide is sprayed into the passenger cabin by crew
members walking along each aisle holding 2(two) 100 g cans at a slow walking pace of
one row per second starting at the rear of the aircraft.
An announcement shall be made before in-flight spraying is started and passengers who
feel that it may cause them inconvenience should be advised to close their eyes and cover
their faces while the procedure is carried out.
19 Nov 2015
Page 3-3
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
The active ingredient of the aerosol used for in-flight spraying must be 2% dPhenothrin. The spraying is to be applied as near as possible to the ceiling at a
rate of 35 g of the formulation per 100 m3 (10 g per 1000 ft3).
An entry confirming the treatment should be made in the aircraft declaration of
health and the empty spray cans of pre-flight and in-flight spraying must be
retained in the aircraft and delivered to the appropriate authority on arrival.
3.2.4.3
Residual Treatment
3.2.4.3.1
This method has been included in WHO recommendations on the disinsecting of
aircraft in 1985.
3.2.4.3.2
The procedure aims at producing an even film of the residual insecticide
permethrine on all interior surfaces of the aircraft to ensure that if an insect gains
access to the aircraft and land on a surface it will receive an effective dose of
insecticide.
3.2.4.3.3
The formulation used for residual treatment is a 2% emulsion or an aerosol.
Spraying of the interior surfaces shall produce an even deposit of 0.5 g
Permethrine per m2 on carpets and 0.2 g per m2 on other interior surfaces
including ceilings, walls, lockers, curtains and wall areas behind them, toilets and
galleys excluding surfaces used for food preparations. Subsequent applications
shall be done at the rate of 0.2 g per m2 on carpets and 0.1 g per m2 on other
surfaces.
3.2.4.3.4
After spraying is completed, air conditioning packs should be run for at least one
hour to clear the air of the volatile components of the spray.
3.2.4.3.5
Treatment must be at intervals not greater than two months to ensure efficacy of
the insecticidal film. Replacement carpets or seat covers which are exchanged
within the 2 months period shall be retreated. The same applies to surfaces
receiving substantial cleaning.
3.2.4.3.6
A Certificate of Residual Disinsection shall be issued by the appropriate authority
and signed by the person who supervised the treatment (As per Appendix 2).
3.2.4.3.7
A WHO consultation 1995 states that, insofar as efficacy inconveniences to, and
safety of passengers with possible predisposition to adverse health reaction is
concerned, the residual disinsection method provides the most assurance. It does
not require passengers and crew to be exposed to aerosol sprays and has the added
benefit of lessening the workload of aircraft cabin crew.
3.2.4.4
Pre-embarkation method
3.2.4.4.1
This disinsection procedure consists of spraying all interior spaces of the aircraft
with an aerosol containing a mixture of a fast-acting (2% Phenothrin) and a
residual (2% permethrine) insecticide before embarkation.
19 Nov 2015
Page 3-4
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
3.2.4.4.2
Trials have proven the efficacy of this method killing all flying insects and others
which gained access to the aircraft.
3.2.4.4.3
The strong repellant effect of this aerosol also prevents a substantial number of
insects from entering the aircraft.
3.2.4.4.4
Spraying of the aerosol mixture is carried out after cleaning and catering is
finished, and no longer than one hour before boarding begins.
3.2.4.4.5
All interior spaces shall be sprayed including flight deck, crew rest, lockers,
wardrobes, and toilets.
3.2.4.4.6
Air conditioning packs have to be turned off during treatment.
The obvious advantages of this method are:
3.2.4.5
no inconvenience to passengers and crew; no departure delays;
application possible by trained airline staff;
use of relatively safe, WHO-recommended insecticides;
simple and inexpensive method, easy to audit by authorities.
Two-step-method
The objectives in the development of this method were: to achieve reliable
insecticidal activity against a broad spectrum of flying and non-flying vectors; to
avoid the application of insecticides in the presence of passengers and crew; to
avoid the cumulative contamination of all the interior surfaces of the aircraft with
a residual insecticide taking the long lasting effects of absorption and release of
permethrine on the aircraft interior materials into account.
3.2.4.5.1
First step:
A film of residual pyrethroid is applied in regular intervals to the floor and side
walls of the aircraft cabin and other interior spaces as a spot or barrier treatment
to control and eliminate non-flying vectors such as lice, ticks, mites and fleas as
well as other insect pests such as cockroaches and ants. Cargo holds are treated
with a residual film according to the residual treatment method.
The treatment can easily be done together with routine maintenance by trained
staff. In addition regular pest monitoring with diagnostic measures should be
established. Depending on the results of monitoring further treatment with
suitable baits may be necessary.
3.2.4.5.2
Second step:
At destinations where disinsection is needed the interior of the aircraft is sprayed
with an aerosol containing 2% d-Phenothrin not more than one hour before crew
and passengers board the aircraft. After cleaning and catering are finished, trained
members of the ground staff walk along each aisle twice at a slow walking pace
of one row per second and discharge the fast-acting aerosol
19 Nov 2015
Page 3-5
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
above the seats on the first turn and under the seats on the second. The spraying should be
done at a rate of 35 g of the formulation per 100 m3 (10 g per 1000 ft3) with spray cans
of 100- 250 g size and a specified discharge rate.
The doors of the aircraft must be closed, all overhead and sidewall lockers, cupboards
and toilets have to be opened and the air condition must be turned off during treatment
and for at least another 10-15 minutes.
Besides the fast acting kill effect d-Phenothrin has a relatively short residual-effect which
ensures that flying insects entering the aircraft during passenger boarding will receive an
effective dose of insecticide when they land on cabin surfaces during the flight.
The repellant effect of -Phenothrin additionally reduces the number of flying vectors
entering the aircraft during boarding.
(Ref: IATA Medical Manual, section 5 and WHO guide to hygiene and sanitation in
aviation, chapter 10.3)
3.3
Disinfection of aircraft
3.3.2
When aircraft disinfection is required, the following provisions shall apply:
3.3.1
the application shall be limited solely to the container or to the compartment of the
aircraft in which the traffic was carried;
the disinfection shall be undertaken by procedures that are in accordance with the aircraft
manufacturer and any advice from WHO;
the contaminated areas shall be disinfected with compounds possessing suitable
germicidal properties appropriate to the suspected infectious agent;
the disinfection shall be carried out expeditiously by cleaners wearing suitable personal
protective equipment; and
flammable chemical compounds, solutions or their residues likely to damage aircraft
structure, or its systems, such as by corrosion, or chemicals likely to damage the health of
passengers or crew, shall not be employed.
The airlines shall ensure that where there is contamination of surfaces or equipment of
the aircraft by any bodily fluids including excreta, the contaminated areas and used
equipment or tools shall be disinfected on during his stay in the territory visited.
(Ref: Annex 9, Chapter 2 to 2.31-2.32)
3.4
3.4.1
Procedure of disinfection:
Introduction
Disinfection of aircraft is very much important following transport of a suspected case of
communicable disease on board an aircraft. Under such circumstances the airport health
authority should be consulted as not all effective disinfectants are suitable for use on
board. WHO, IATA, aircraft manufacturers and ICAO are the main organizations
23 Nov 2015
Page 3-6
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
involved in determining a suitable disinfection process at the international level. Should
an infectious disease be diagnosed either during the flight or immediately on arrival and
before the aircraft departs again, disinfection may be of value.
3.4.2
The Procedures
3.4.2.1 The disinfectants most commonly employed are sodium hypochlorite diluted to strength
of 100mg/L and a 5% solution of formalin.
3.4.2.2 Sodium hypochlorite is also used when disinfecting aircraft after the carriage of a person
infected with a food or waterborne disease.
3.4.2.3 Personnel wearing water proof gloves should swab the following areas with the sodium
hypochlorite solution, which should remain in contact with these surfaces for 30 minutes
before they are rinsed with warm water and dried to remove any residual chlorine:
All surfaces of the toilet compartment.
All surfaces and food containers in the galley.
All meal tables, seat armrests and ashtrays in the cabin.
3.4.2.4 The toilet system should be drained and flushed in the normal way but the chemical fluid
containing a bactericide should be allowed to stand at least for 2 hours.
3.4.2.5 The fabric covers of the seat in which the infected person sat, and those of the seats in
row in the front and the row behind should be removed, soaked in the disinfectant
solution for 1 hour and, sent for dry cleaning suitably marked.
3.4.2.6 The remaining seats and carpets should be vacuum cleaned and the dust incinerated.
3.4.2.7 All hard surfaces should be swabbed with formalin solution which, after 30 minutes
contact, should then be rinsed away with warm water.
3.4.2.8 The personnel engaged in disinfecting work should wear waterproof gloves as well as
face masks in addition.
3.5
Disposal of used air sickness containers
Used air-sickness containers should be stored in the toilet compartment. They should not
be put down the toilet, and a notice to this effect should be placed in the toilet
compartment. They should be removed from the aircraft by the toilet servicing team and
disposed of along with the toilet wastes. If any receptacle is used on the aircraft for
storage of used sickness containers, it should be thoroughly cleaned, washed and
disinfected after each use.
3.6
Aircraft Interior Cleaning
When an aircraft commences a flight, boarding passengers always look for an attractive
cabin interior. During flight conditions gradually deteriorate, and therefore at each transit
stop rapid tidying is necessary.
19 Nov 201
Page 3-7
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
Though complete cleaning is not possible when passengers remain on board but all
efforts to be made to provide comforts to the passengers. The extend of cleaning will
depend on the amount of time available, at all events priority must be given to the
removal of litter and dry waste and the cleaning of toilet compartments and galleys.
Regulatory Authority shall conduct inspection to assess the aircraft interior cleaning
status (Appendix 6) for necessary corrective action.
3.6.1
Cleaning Schedules
The following are the suggested minimum procedures:
3.6.1.1 Cleaning during transit stops,
Galley:
Empty waste bin clean
Clean sinks
Clean worktop
Remove any debris, wipe up spillages and clean floor.
Toilet compartments:
Remove debris and waste bins.
Wipe wash hand basin.
Wipe and dry top and back of the toilet seat and cover
Empty and clean ashtray.
Wipe mirrors, surrounds and fittings as necessary
Replenish toilet soap and toiletries.
Clean floor.
Passenger cabins:
Clear debris from seats, seat-back pockets and hat racks.
Wipe clean all tables.
Empty ashtrays.
Sweep floor.
Brush seats.
Flight deck:
Clear debris, Empty waste containers and ashtrays.
Clean exterior of windscreen.
If time does not permit completion of the above tasks, priority should be given to
the removal of waste and the cleaning of galleys and toilets.. To expedite cleaning
procedures and to reduce the amount of equipment required, disposable swabs
impregnated with this product can be prepared in advance, stored in polyethylene bags,
and used for all wiping operations.
3.6.1.2 Intensive cleaning
A more thorough cleaning should be carried out once every 24 hours, either during a
night stop (this will apply mostly to short-haul aircraft) or at any other operationally
convenient time. Intensive cleaning, which will usually take four times as many
man-hours as the transit clean, consists of the following operations:
19 Nov 2015
Page 3-8
Civil Aviation Authority, Bangladesh
3.6.2
Aviation Public Health Manual
Galley:
Clear debris, wipe up spillages, clean floor
Empty, wash and disinfect waste bins.
Clean all work surfaces, sinks, fittings and galley structures.
Clean all cabin crew seats.
Clean all container and trolley stowages, including the framework.
Clean control panel, telephones, doors, panels, etc.
Toilet compartments:
Clean wash-hand-basin, mirrors, surrounds and fittings.
Clean and dry hinged panel below wash-hand-basin.
Wash and dry toilet surrounds.
Wash and dry top and back of toilet seat.
Passenger cabins:
Clean all ashtrays and seat-back pockets.
Brush seat backs, cushions and armrests.
Clean chair frames under seat cushion.
Clean all tables and hat racks.
Vacuum-clean all carpets.
Clean interior of cabin windows, surrounds and blinds.
Clean all cabin fittings, service panels, bulkheads and head linings.
Vacuum-clean all ventilation grilles.
Change all soiled headrest covers.
Sweep steps and clean handrails of air stairs where applicable.
Replace all used blankets with freshly laundered ones.
Flight deck:
Clean all ashtrays and empty waste bins.
Clean crew seats and harnesses.
Vacuum-clean floor.
Wipe clean sides of consoles, ledges, etc.
Clean interior and exterior of windows.
About Galleys
Aircraft galleys or pantries vary in size, shape and construction according to the type
of aircraft. Some parts of the galley are semi permanent fixtures and only normally
removed during an aircraft maintenance check. Other parts are mobile i.e., modules,
food containers, trolleys, some types of oven, and beverage containers.
Galleys are extremely difficult to clean satisfactorily at times other than during
maintenance checks, since they have many almost inaccessible areas in which foods and
beverages particularly the latter can penetrate. The introduction of modules in widebodied aircraft is an improvement, but much more could be done to design a galley that
would be easier to clean than the present type.
3.6.3
Problem areas
Aircraft cleaners need to pay particular attention to the following dirt traps and make sure
that they are thoroughly cleaned out:
Catering equipment runners.
Bar box recesses.
19 Nov 2015
Page 3-9
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
Floor of catering container compartments.
Sink drain pipes (frequently blocked).
Drinking-fountain wastes and bottle top remover recesses.
Toilet compartment cupboards.
First-aid stowage holds.
Special Needs
3.7
There are occasions when special action is needed during flight especially when carpets
or seats are soiled by a sick passenger. This sickness may be the result of an infection
causing nuisance to other passengers. There might be a health hazard, since a major
replacement of soiled seat covers cannot be undertaken until arrival to the next airport,
the cabin crew is to be supplied with cleaning materials for use in such an emergency
condition.
Aerosol dispensers containing a detergent/bactericide/odour counteragent may solve the
immediate problem before action can be taken on the ground.
Following aerosol dispensers may be used under such circumstances as per the WHO
guide to hygiene and sanitation in aviation (2009):
Carboxide- A mixture of 10% ethylene oxide and 90% carbon dioxide.
A mixture of ethylene oxide and Freon II
Betapropiolactone in vapour form
Note: When any of the above three ingredients is used, disinfecting should be carried
out only by trained personnel.
(Ref: Who guide to hygiene and sanitation in aviation 2009, Chapter 8, 8.1, 8,2, 8.3, 8.4).
3.8
Precautions against animals transportation in the aircraft:
3.8.1
Animals, both wild and domestic, tropical fish, birds and different types of domestic pets
are transported in a large number by air, regularly and frequently.
3.8.2
As domestic pets can transmit a lot many zoonotic diseases, all animal should be
transported in the freight holds under most aseptic condition. Before any animal is
accepted for transport, it must be ascertained that no discomfort will be caused to
passengers or crew from odours, noise or the animal’s escape from restrain during
voyage.
Only healthy animals in a suitable condition should be accepted. Those that are unfit,
infirm, diseased or injured, or likely to give birth during the journey should be rejected.
All animals should be carried in containers suitable to their species and size.
Animals should not be placed near foodstuffs.
Animals for laboratory use must be separated from other animals to reduce the risk of
cross infection.
Different species of animals should not be mixed, and care should be taken not to place in
close proximity cages containing animals naturally hostile to each other.
To minimize odour during flight, and cages are being handled, solid deodorant sachets
3.8.3
3.8.4
3.8.5
3.8.6
3.8.7
3.8.8
19 Nov 2015
Page 3-10
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
should be attached to each container, but out of the animal’s reach. They must never be
sprayed with disinfectant.
3.8.9 The consignor should be given full information about import permit, veterinary health
certificate, veterinary examination, quarantine and trans-shipment to the country of
destination.
3.8.10 All airports from which animals are exported, imported or held in transit should be
provided with animal holding rooms and to be suitably constructed as per “WHO guide to
hygiene and sanitation in aviation” Under all the conditions Veterinary advice must be
readily available in the airports.
3.9
Foodstuffs carriage in aircraft
3.9.1
Foodstuffs containers carried in the aircraft should always be kept in a clean condition.
3.9.2
Containers should be washed out thoroughly before loading commences and after load
has been discharged.
3.9.3
A solution of detergent/germicide is recommended. After being washed, the container
should be allowed to dry thoroughly before reuse.
3.9.4
Precautions should be taken to prevent any contamination of foodstuffs by other cargo.
(Ref: Who guide to hygiene and sanitation in aviation 2009, Chapter 9.2& 9.3)
3.10
International certificates of vaccination or prophylaxis
3.10.1 In cases where proof of vaccination or prophylaxis is required by national authorities
under the International Health Regulations (2005), State shall accept the International
Certificate of Vaccination or Prophylaxis prescribed by the World Health Organization
in the IHR (2005) (Appendix 4 ).
3.10.2 In emergency situations resulting from force majeure, aircraft operators and airport
operators should give priority assistance to those passengers with medical needs,
unaccompanied minors and persons with disabilities who have already commenced their
journey
(Ref: ICAO Annex 9 Chapter 3. H)
3.11 Importation of radioactive material
3.11.1 The concerned authority shall facilitate the prompt release of radioactive material being
imported by air, particularly material used in medical applications, provided that
applicable laws and regulations governing the importation of such material are complied
with.
Note- The advance notification, either in paper form or electronically, of the transport of
radioactive materials would likely facilitate the entry of such material.
19 Nov 2015
Page 3-11
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
3.12 Facilities required for implementation of public health, emergency
medical relief, and animal and plant quarantine measures (Annex 9
chapter 6C)
3.12.1 The concerned authorities in cognigence to Chairman, CAA, Bangladesh shall ensure the
maintenance of public health, including human, animal and plant quarantine at state
designated international airport (HSIA).
Medical authorities should ensure that all the international airports are having facilities
and services for vaccination or revaccination, and for the delivery of the corresponding
certificates.
International airports should have available access to appropriate facilities for
administration of public health and animal and plant quarantine measures applicable to
aircraft, crew, passengers, baggage cargo, mail and stores.
Airports authority should ensure that passengers and crew in transit can remain in
premises free from any danger of infection and insect vectors of diseases and, when
necessary, facilities should be provided for the transfer of passengers and crew to another
terminal or airport nearby without exposure to any health hazard. Similar arrangements
and facilities should also be made available in respect of animals.
3.12.2 Civil aviation authority and respective airline shall ensure that handling and distribution
procedures for consumable products (i.e. food, drink and water supplies) on board aircraft
or in the airport are in compliance with the International Health Regulations (2005) and
relevant guidelines of the World Health Organization, the Food and Agriculture
Organization and national airport regulations.
3.12.3 The airport and the aircraft operators, shall ensure that a safe, sanitary and efficient
system is instituted, at international airports, for the removal and disposal of all waste,
waste water and other matters dangerous to the health of persons, animals or plants, in
compliance with the International Health Regulations (2005) and relevant guidelines of
the World Health Organization, the Food and Agriculture Organization and national
airport regulations.
3.12.4 Director General of Health Services in coordination to Chairman shall ensure that
international airports maintain facilities and services for first-aid attendance on site, and
that appropriate arrangements are available for expeditious referral of the occasional
more serious case to prearranged competent medical attention.
3.13 Passenger amenities in the airport
3.13.1 Airport operators should provide suitable childcare facilities in passenger terminals, and
that they are clearly indicated by signage and are easily accessible.
(Ref: ICAO Annex 9, Chapter 6.35-6.41, 6.46)
19 Nov 2015
Page 3-12
Civil Aviation Authority, Bangladesh
3.14
Aviation Public Health Manual
Relief flights following natural and man-made disasters which seriously endanger
human health or the environment, and similar emergency situations where United
Nations (UN) assistance is required
3.14.1Bangladesh shall facilitate the entry into, departure from and transit through their
territories of aircraft engaged in relief flights performed by or on behalf of international
organizations recognized by the UN or by or on behalf of States and shall take all
possible measures to ensure their safe operation. Such relief flights are those undertaken
in response to natural and man-made disasters which seriously endanger human health or
the environment, as well as similar emergency situations where UN assistance is
required. Such flights shall be commenced as quickly as possible after obtaining
agreement with the recipient country.
Note 1-According to its Internationally Agreed Glossary of Basic Terms, the United
Nations Department of Humanitarian Affairs considers an emergency to be “a sudden and
usually unforeseen event that calls for immediate measures to minimize its adverse
consequences”, and a disaster to be “a serious disruption of the functioning of society
,causing widespread human, material or environmental losses which exceed the ability of
the affected society to cope using only its own resources”.
Note 2-With respect to the application of measures to ensure the safe operation of relief
flights, attention is drawn to Annex 11 — Air Traffic Services, the Manual Concerning
Safety Measures Relating to Military Activities Potentially Hazardous to Civil Aircraft
Operations (Doc 9554) and the Manual concerning Interception of Civil Aircraft (Doc
9433).
3.14.2 Civil Aviation Authority, Bangladesh shall ensure that personnel and articles arriving on
relief flights are cleared without delay.
(Ref: ICAO Annex 9.Chapter 8.C)
3.15
Implementation of International Health Regulations and Related Provisions
3.15.1 Bangladesh shall comply with the pertinent provisions of the International Health
Regulations (2005) of the World Health Organization.
3.15.2 Health Authority shall take all possible measures to have vaccinators use the Model
International Certificate of Vaccination or Prophylaxis, in accordance with Article 36 and
Annex 6 of the International Health Regulations (2005), in order to assure uniform
acceptance.
3.15.3 Concerned Health Authority shall make arrangements to enable all aircraft operators and
agencies concerned to make available to passengers, sufficiently in advance of departure,
information concerning the vaccination requirements of the countries of destination, as
well as the Model International Certificate of Vaccination or Prophylaxis conforming to
Article36 and Annex 6 of the International Health Regulations (2005) ( Appendix 4 ).
19 Nov 2015
Page 3-13
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
3.15.4 The pilot-in-command of an aircraft shall ensure that a suspected communicable disease
is reported promptly to air traffic control, in order to facilitate provision for the presence
of any special medical personnel and equipment necessary for the management of public
health risks on arrival.
Note 1-A communicable disease could be suspected and require further evaluation if a
person has a fever (temperature 38°C/100°F or greater) that is associated with certain
signs or symptoms: e.g. appearing obviously unwell ;persistent coughing; impaired
breathing; persistent diarrhoea; persistent vomiting; skin rash; bruising or bleeding
without previous injury; or, confusion of recent onset.
Note 2-In the event of a case of suspected communicable disease on board an aircraft, the
pilot-in-command may need to follow his operator’s protocols and procedures, in
addition to health-related legal requirements of the countries of departure and/or
destination. The latter would normally be found in the Aeronautical Information
Publications (AIPs) of the States concerned.
Note 3-Annex 6 — Operation of Aircraft describes the “on board” medical supplies that
are required to be carried on aircraft. The Procedures for Air Navigation Services — Air
Traffic Management (PANS-ATM, Doc 4444) describes the procedures to be followed
by the pilot-in-command in communication with air traffic control.
3.15.5. When a public health threat has been identified, and when the public health authorities
require information concerning passengers’ and/or crews’ travel itineraries or contact
information for the purposes of tracing persons who may have been exposed to a
communicable disease, “Public Health Passenger Locator Card” reproduced in Appendix
13 of ICAO Annex 9 need to be used. (Appendix 3, 3A)
Note -It is suggested that Public Health Authority of Director General of Health Services
makes available adequate stocks of the Passenger Locator Card, for use at their
international airports and for distribution to air operators, for completion by passengers
and crew.
(Ref:
ICAO Annex 9 Chapter 8.12-8.15.1)
3.16 Communicable Disease Outbreak National Aviation Plan
3.16.1 Public Health Authority of Director General of Health Services, Ministry of Health and
Family Welfare in cognizance to Chairman shall establish a national aviation plan for an
outbreak of a communicable disease posing a public health risk or public health
emergency of international concern.
(Ref: ICAO Annex 9, Chapter 8.16)
3.17 Facilitation of the Transport of Persons with disabilities
3.17.1 When travelling, persons with disabilities should be provided with special assistance in
order to ensure that they receive services customarily available to the general public.
23 Nov 2015
Page 3-14
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
3.17.2 Authority should take the necessary measures to make accessible to persons with
disabilities all the elements of the chain of the person’s journey, from arrival at the airport
of departure to leaving the airport of destination.
3.17.3 Air operators, airports and ground handling operators are to provide necessary
transportation services for persons with disabilities, from arrival at the airport of
departure to leaving the airport of destination.
(Ref: Annex 9 Chapter 8.22-8.26)
3.18 Access to airports of disabled persons
3.18.1 Airport Authority shall take the necessary steps to ensure that airport facilities and
services are adapted to the needs of persons with disabilities.
3.18.2 The Authority should ensure that lifting systems or any other appropriate devices are
made available in order to facilitate the movement of elderly and disabled passengers
between the aircraft and the terminal on both arrival and departure as required where
telescopic passageways are not used.
3.18.3 Measures should be taken to ensure that the hearing- and vision-impaired are able to
obtain flight information.
3.18.4 For elderly and disabled persons being set down or picked up at a terminal building,
reserved points should be located as close as possible to main entrances. To facilitate
movement to the various areas of the airport, access routes should be free of obstacles.
3.18.5 Where access to public services is limited, every effort should be made to provide
accessible and reasonably priced ground transportation services by adapting current and
planned public transit systems or by providing special transport services for people with
mobility needs.
3.18.6 Adequate parking facilities should be provided for people with mobility needs and
appropriate measures taken to facilitate their movement between parking areas and the
terminal buildings.
3.18.7 Direct transfer from one aircraft to another of passengers, particularly elderly and
disabled passengers, should be authorized, where necessary and possible, whenever this
is warranted by deadlines in making connecting flights or by other circumstances.
(Ref:
Annex 9 Chapter 8.27-8.33)
3.19 Access to air services of disabled persons
3.19.1 Air operator shall take the necessary steps to ensure that persons with disabilities have
adequate access to air services.
3.19.2 Air operator should introduce provisions by which aircraft coming newly into service or
after major refurbishment should conform to minimum uniform standards of accessibility
with respect to equipment on board aircraft which would include movable armrests, onboard wheelchairs, lavatories and suitable lighting and signs.
19 Nov 2015
Page 3-15
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
3.19.3 Wheelchairs, special apparatus and equipment required by persons with disabilities
should be carried free of charge in the cabin where, in the view of the aircraft operator,
space and safety requirements permit or should be designated as priority baggage.
3.19.3 Service animals accompanying passengers with disabilities should also be carried free of
charge in the cabin, subject to the application of any relevant national or aircraft operator
regulations.
3.19.4 In principle, persons with disabilities should be permitted to determine whether or not
they need an escort and to travel without the requirement for a medical clearance.
However, advance notice should be mandatory where assistance or lifting is required.
Aircraft operators should only be permitted to require passengers with disabilities to
obtain a medical clearance in cases of medical condition where it is clear that their safety
or well-being or that of other passengers cannot be guaranteed. Furthermore, aircraft
operators should only be permitted to require an escort when it is clear that a person with
disabilities is not self-reliant and, as such, the safety or well-being of that person or that
of another passenger cannot be guaranteed.
3.19.5 If the presence of an escort is required, air operators are to offer discounts for the carriage
of that accompanying person.
(Ref: Annex 9 Chapter 8.34-8.38)
19 Nov 2015
Page 3-16
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
CHAPTER 4
Water supply in the airport and in the aircraft
4.1
Background
Travel can facilitate the transfer of communicable disease. The volume and rapidity of
travel can have an international impact on disease. This is particularly true for aircraft, as
the global span of the aviation industry requires the loading and rapid transport of people
and supplies from many locations all over the world.
One risk is posed by the potential for microbial contamination of aircraft water by animal
or human excreta. This contamination may originate from source waters or may occur
during transfer operations or while water is stored on board the aircraft. Waterborne
disease burdens in many parts of the world include cholera, enteric fevers (Salmonella),
bacillary and amoebic dysentery and other enteric infections. These diseases are not
unique to water; food may actually be the dominant risk vector in some environments,
and, in fact, most airlines have a good record with respect to known contamination
incidents. However, any location is at risk if proper procedures and sanitation practices
are not continuously followed to ensure the safety of water that is used for drinking and
food processing and preparation.
4.2
Water supply and transfer chain
Even if the water at the airport is safe, that does not ensure that it will remain safe during
the transfer to the aircraft and storage activities that follow. An understanding of the
aircraft drinking-water supply and transfer chain will help to illustrate the points at which
the water can become contaminated en route to the tap on board the aircraft. Generally,
the aircraft drinking-water supply and transfer chain consists of four major Components:
4.2.1
The source of water coming into the airport;
4.2.2
The airport water system, which includes the on-site distribution system. It may also
include treatment facilities if the airport produces its own potable water;
4.2.3
The transfer point (sometimes referred to as the watering point), including the water
transfer and delivery system. It is typically a temporary interconnection between the hard
plumbed distribution system of the airport (e.g. at a hydrant) and the aircraft water
system, by means of potable water vehicles and carts, refillable containers or hoses. This
water transfer process provides multiple opportunities for the introduction of
Contaminants into the drinking-water;
4.2.4
The aircraft water system, which includes the water service panel, the filler neck of the
aircraft finished water storage tank and all finished water storage tanks, including
refillable containers, piping, treatment equipment and plumbing fixtures within the
aircraft that supply water to passengers or crew.
19 Nov 2015
Page 4-1
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
Figure 4.1 is a flow diagram of a typical aircraft potable water supply and transfer chain.
It depicts the water path from potable water source to the aircraft’s galley and lavatory
taps serving passengers and crew.
4.3
Complying with International Health Regulations (2005)
4.3.2
In accordance with Article 24 (c) of the IHR (2005), Medical authority in cognizance to
Chairman CAAB is required to take all practicable measures to ensure that international
conveyance operators keep their conveyances free of sources of contamination and
infection, which should include drinking water.
However, it is the responsibility of each aircraft operator to ensure that no sources of
infection and contamination are found on board, including in the water system. For this
purpose, it is important that these standards are being upheld on the aircraft, in terms of
both the quality of the water taken on board from the source of supply on the ground and
maintenance of water quality on board.
Regulatory authorities are required to ensure, as far as practicable, that the facilities at
international airports are in sanitary condition and are kept free of sources of infection
and contamination, as per Article 22 (b).
4.3.1
4.3.3
4.3.4
Annex 1 B 1 (d) of the IHR (2005) requires every airport specifically designated by a
State to have or develop within a limited period the capacity to provide safe potable water
supplies for travellers using airport facilities.
19 Nov 2015
Page 4-2
Civil Aviation Authority, Bangladesh
4.4
Aviation Public Health Manual
General Roles and Responsibilities of each Component of water supply:
The authority is to develop an effective means of achieving consistency in ensuring the
safety of drinking water supply. The entity responsible for each component of the
drinking-water supply chain is water source, airport, transfer point and aircraft. General
roles and responsibilities for each such component are as follows:
4.4.1
Water Source: Role is to provide to the airport a safe water supply of sufficient quantity
and quality. Responsibilities are to monitor the water system by sampling water and
providing sampling results to the airport competent authority on request, advising the
airport authority of any adverse results and action to be taken, and advising the airport
authority when the water supply has or may become contaminated and of action taken.
4.4.2
Airport authority: Role is to maintain the integrity of the water supplied and to provide
safe water to the occupants, travellers, visitors, workers, water haulers and transfer points
to the aircraft within the airport grounds. Responsibilities are to monitor the water system
by sampling water and sharing sampling results with authorities and also stakeholders on
request and to advise not only the water supplier but all concerned parties who use their
water of any adverse results and corrective actions. In some circumstances, the airport
may be both the source water supplier and provider of treated drinking-water.
4.4.3
Transfer Point (Water haulers): Role is to provide water to the aircraft.
Responsibilities are to maintain a safe water supply from the transfer point to the aircraft,
to maintain the equipment in good working order, to monitor the water system by
sampling water and sharing sampling results with stakeholders on request and to report
adverse results and action to be taken to the aircraft operator and airport authority.
4.4.4
Aircraft operator: Role is to provide a safe water supply to the passengers and crew for
drinking, culinary purposes and personal hygiene. Responsibilities are to maintain their
onboard water tank(s) clean and free of harmful microbial contamination, to monitor the
water system by sampling water, to share sampling results with stakeholders, to report
adverse results to the competent authority and take corrective actions, and, when and
where required, to advise the crew and passengers of the adverse results. The WSP (water
safety plans) for an airport source water supplier and drinking-water provider may be
fairly detailed owing to the size and complexity of the facilities, whereas WSPs may be
relatively basic for transfers and on board aircraft.
4.4.5
Overview of water safety plans (WSPs)
Water safety plans (WSPs) are the most effective management approach for consistently
ensuring the safety of a drinking-water supply. A potable water source at the airport is not
a guarantee of safe water on board the aircraft, as the water may be contaminated during
transfer to or storage or distribution in the aircraft. A WSP covering water management
within airports from receipt of the water through to its transfer to the aircraft,
complemented by measures (e.g. safe materials and good practices in design,
construction, operation and maintenance of aircraft water systems) to ensure that water
quality is maintained on the aircraft, provides a framework for water safety in aviation.
19 Nov 2015
Page 4-3
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
The WSP should be reviewed and agreed upon with the authority responsible for
protection of public health to ensure that it will deliver water of a quality consistent with
the health-based targets.
4.5
Hazards in the water supply chain
4.5.1
The water transfer points between the airport source and the aircraft onboard storage and
distribution system present significant opportunities for contamination. Common
equipment used to transfer water includes piping, hoses, potable water cabinets, bowsers,
tanks, filling stations, refillable containers, and hydrants (including taps/faucets).
Equipment should be constructed of appropriate materials (e.g. corrosion-resistant
materials) certified for this application, properly designed, operated, labelled and
maintained, and used for no other purpose that might adversely affect the quality of the
water. Assumptions and manufacturer specifications for each piece of equipment need to
be validated to ensure that the equipment is effective.
4.5.2
Potable water should be obtained from those transfer points approved by the competent
authority. The lines’ capacity should be such as to maintain positive pressure at all times
to reduce the risk of backflow. There should be no connections between the potable water
system and other piping systems. Backflow of contaminated water into the potable water
system needs to be prevented by proper installation of piping, backflow prevention
devices and plumbing. Water for drinking and culinary use on aircraft should not be
taken from water closets, washrooms or other places where danger of contamination
exists or may develop.
4.5.3
The tanks should be so designed that they can be disinfected and flushed and should be
provided with a drain that permits complete drainage of the tank. They should be labelled
“DRINKING WATER ONLY”. The inlet and outlet to the tank should terminate in a
downward direction or gooseneck and should be provided with caps or closures with
keeper chains for protection against contamination. The inlet and outlet should be
equipped with couplings of a type that permits quick, easy attachment and removal of the
hose. When hoses are transported on the water cart, storage facilities should be provided
on the cart to protect the hoses from contamination.
19 Nov 2015
Page 4-4
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
Figure 4.2: Sources of water contamination in the transfer chain
19 Nov 2015
Page 4-5
Civil Aviation Authority, Bangladesh
4.6
Aviation Public Health Manual
Monitoring of potable water supply
All water on the aircraft intended for drinking, food preparation or human contact
should be potable and meet the GDWQ (WHO Guideline for drinking water quality) or
specifications of national standards (ECR 97), whichever are more stringent. If the water
provided at the airport, at the transfer point or on the aircraft does not meet the GDWQ or
national standard, the appropriate responsible entity must take measures to ensure that
water on board will be safe. These may include, for example, providing water treatment,
deciding not to board water at that location and/or obtaining water from an alternative
source: Specific requirements applicable to water on aircraft are provided in the
following guideline:
Sl no
Parameters
1.
2.
3.
4.
5.
6.
7.
8.
9.
4.6.1
pH
Turbidity (NTU)
Total hardness(mg/L)
Chloride (mg/L)
TDS (mg/L)
Iron Fe (mg/L)
Arsenic As (mg/L)
Nitrate-N (mg/L)
Total coliform (N/100
ml )
Remarks
Bangladesh Standard
(ECR- 97)
6.5-8.5
10
10
600
1000
0.3-1.0
0.05
10
0
WHO Standard
6.5-8.5
05
200
1000
0.3
0.01
50
0
E.coli or thermo tolerant (faecal) coli forms: No E. Coli (Fecal) coliforms should be
detected in any 100 ml sample of water. A positive test may be an indication of potential
pathogenic (primarily bacterial) microorganisms associated with human excreta.
Turbidity: Turbidity that increases in the airport water indicates that dirth has entered the
system during the transfer.
Detection of odour/colour/taste may indicate cross-connection with the liquid waste
system.
Chemicals contamination of water with nitrate/nitrite at the airport indicates cross
connections with the liquid waste system and copper leaching.
Metal such as iron can be leached from some materials into the water and contribute
adverse taste or in some cases, health concerns.
4.7
Indicators of monitoring water
4.7.1
Monitoring at airport water taps is carried out at locations to ensure that persons served
by the airport are provided safe water. Recommended parameters that should be
monitored at the entrance to the transfer point are E. coli or thermotolerant (faecal)
coliforms, disinfectant residual, chemicals of acute significance, corrosion-related
contaminants, and turbidity and aesthetic parameters.
4.7.2
Monitoring at the transfer point takes place to ensure that water boarded on aircraft is
safe. Recommended parameters that should be monitored at the transfer point to the
19 Nov 2015
Page 4-6
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
aircraft (includes bowsers, trucks, carts, hoses, refillables) are E. coli or thermotolerant
(faecal) coliforms, disinfectant residual and, if required, turbidity.
4.7.3
Monitoring on aircraft is carried out at locations to ensure that persons on board the
aircraft are provided safe water. It is recommended that E. coli or thermotolerant (faecal)
coliforms be monitored at representative taps (e.g. galley, lavatory, drinking fountains).
The monitoring should take place at each major servicing, in addition to regular E. coli
spot checks while in service. Complaints about aesthetic parameters (odour/colour/taste)
will trigger further investigations into the water quality and may indicate the need to
monitor for turbidity. Additional parameters to be monitored include chemicals of acute
significance and corrosion-related contaminants. Disinfectant residuals are also measured
after the aircraft has been disinfected and flushed.
4.7.4
All critical parameters are monitored at a sufficient frequency to ensure safe water.
4.8
Frequency of monitoring
4.8.1
Regular monitoring of each parameter is necessary to ensure that safe water quality is
maintained, as each step in the water transfer chain provides an opportunity for
contamination. Documentation (recordkeeping) of monitoring should be kept for
assurance and analysis in the event of an incident.
4.8.2
In certain situations, the frequency of monitoring should be increased for a period
necessary to determine appropriate corrective action and/or assurance that measured
parameters have returned to safe levels. Examples of situations warranting increased
monitoring are positive E. coli or thermotolerant (faecal) coliform results, excessively
humid conditions, during or after natural disasters affecting source water quality and
immediately after maintenance activities that have the potential to affect water quality.
4.8.3
Aesthetic parameters such as odour, colour or taste are typically “measured” through
customer complaints, although the crew may also wish to do an independent periodic
check. This is a subjective parameter, as individuals have different sensitivities.
4.9
Surveillance (Inspection Procedures of the Establishment)
4.9.1
In most cases, surveillance consists primarily of sanitary inspections of airports, transfer
points or airlines (Appendix 5-11). Sanitary inspection is a tool for determining the state
of the water supply, infrastructure and the identification of actual or potential faults and
should be carried out on a regular basis. Any deficiency identified during inspection must
be corrected within a reasonable time period specified by the regulatory authority.
4.9.2
Surveillance should be accomplished by authorized and trained officers from public
health authorities, or the services of qualified independent inspectors may be utilized.
4.9.3
Specifications for qualifications of the inspectors should be established, and inspectors
should undergo adequate training, including periodic updates and recertification.
Independent inspectors should meet the same requirements as those from the public
health authorities.
(Ref: WHO Guide to hygiene and sanitation in aviation 2009
Chapter 2 & ECR 97- Schedule 3.B).
219Nov 2015
Page 4-7
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
THIS PAGE INTENTIONALLY LEFT BLANK
19 Nov 2015
Page 4-8
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
CHAPTER 5
Cleaning and disinfection of airport facilities
5.1
Background
Cleaning refers primarily to the removal of visible dirt or particles. It is to be kept in
mind that the cleaning process and some products used for cleaning purpose also need
disinfection, which is undertaken on a routine and frequent basis.
Disinfection refers to specific measures taken to control, deactivate or kill infectious
agents, such as viruses and bacteria. Disinfection is normally undertaken during periodic
maintenance checks or after a public health event, such as the suspected carriage of an
infectious passenger. The commercial air transportation is an efficient means for
spreading communicable disease widely by surface contact and proximity to infected
persons.
Competent authorities have responsibilities to ensure that international airports and
aircraft are kept free of sources of infection and contamination (Article 22.1(a, b, c, d, e,
g)) of IHR 2005. The competent authority needs to exercise oversight over cleaning and
disinfection programmes so that its obligations under the IHR (2005) are fulfilled. Under
the IHR, the competent authorities are responsible for supervising service providers
relating to travellers, baggage, cargo, containers, conveyances and goods at points of
entry, including with inspections and medical examinations, as necessary. They are also
responsible for supervision of disinfection, disinsection and decontamination of
conveyances, as well as baggage, cargo, containers and goods under the IHR (2005).
Finally, they are responsible for the supervision of the removal and safe disposal of any
contaminated water or food, human or animal deject, wastewater and any other
contaminated matter from a conveyance (Article 22.1(c ,e–f)). In the context of
conveyances (as well as baggage, cargo and goods) arriving from affected areas, the
competent authorities are responsible for monitoring them so that they are free of sources
of infection or contamination (Article 22.1(a)).
5.2
Requirements for Sanitary condition of airports
To keep airports in a sanitary condition following requirements are to be fulfilled:
5.2.1
That a documented, tested and updated routine cleaning programme exists, and ensure
that premises are regularly and hygienically cleaned. An appropriate number of trained
personnel are available, in relation to the volume and complexity of the airport facilities
and cleaning procedures.
5.2.3
Personal protective techniques and equipment are used by personnel: related equipment
and information (operational procedures for its use) are available.
5.2.4
Cleaning equipment and supplies are available in relation to the volume and complexity
of the airport facilities and cleaning procedures.
5.2.5
Cleaning equipment is properly identified and satisfactorily maintained and stored in a
designated storage area.
19 Nov 2015
Page 5-1
Civil Aviation Authority, Bangladesh
5.3
Aviation Public Health Manual
Design and construction of airports
Airports are to be designed and constructed in a manner that facilitates proper cleaning
and disinfection.
5.3.1
Facilities are designed and constructed of suitable materials (e.g. impervious, smooth and
without seams) to facilitate cleaning and to reduce the risk of harbouring insects, rodents
and other vectors.
5.3.2
Proper design will minimize the amount of accumulated debris and waste and reduce
opportunities for survival of vectors and reservoirs of disease, such as rodents and
insects.
5.3.3 Washrooms designed without doors and with automatic faucets (taps) using “electronic
eyes” (which automatically control the flow of the water to the faucet) are preferable, as
they will reduce contact with hands/fingers.
5.3.4
Providing paper wipes for hand drying will reduce the risk of cross-contamination,
especially when dispensed using “electronic eyes” (hand dryers can promote spread of
pathogens).
(Ref:
5.4
WHO guide to hygiene and sanitation in aviation 2009, Chapter 3.1, 3.2, 3.2.1.2)
Airport toilet sanitation
Passengers, ground staff and members of the public visiting airports may be carriers of
intestinal disease. Meticulous cleanliness of toilets at airports together with the sanitary
treatment, h a n d l i n g and disposal of toilet wastes, is therefore of the utmost
importance
Toilet facilities provided at airports should therefore be of the highest standard and
maintained at the maximum level of cleanliness.
The following minimum r e q u i r e m e n t s are suggested for passenger toilet blocks at
airports.
5.4.1
General features
Screening-When the entrance door is open the interior of the toilet block should not
be visible.
Floors -These should b e of ceramic tiles with coved skirting to walls
Drainage -Floor drainage should discharge into the drainage system through a properly
trapped gully. Floor gully grids should be flush with the floor surface, of suitable
design to allow easy access, and capable of preventing blockage of the gully by waste
material. All fittings should be individually trapped.
Walls-These should be covered from floor to ceiling with tiles or other approved
materials and finishes."Hygiene notices” ("You a r e invited in the interest of hygiene
19 Nov 2015
Page 5-2
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
to wash your hands after using this toilet"), inscribed in glazed tile or on a hard
plastic material, should be fitted in toilet compartments and above urinals.
Ceilings-Ceilings should b e finished with washable material and should not be
perforated.
Lighting-Toilets, cleaner’s compartment and urinals should be adequately lighted,
Supplementary lighting for mirrors and above wash-hand washings should be
provided.
Windows-Where there are windows in toilet accommodation they should be fitted with
translucent laminated glazing frames.
Ventilation-W here natural ventilation is not available, an adequate and efficient
mechanical means of ventilation must be provided.
5.4.2
Toilets related facilities
5.4.2.1 Compartments:
In general, compartment walls should not reach the ceiling, and there should be a
space of 15 cm (6 in) between the lower edge and the floor. The end of the
compartment wall should abut tightly against the main wall to eliminate the
possibility of a dirt trap. Compartment wall surfaces should be nonabsorbent, scratchproof and easy to clean.
Toilet doors should be of durable material with a smooth surface and easy to clean.
They should not reach the ceiling, and there should be a space of 15 cm (6 in)
between the lower edge and the floor. The inner side should be fitted with a
combined doorstop and with rubber buffer.
5.4.2.2 Fittings:
Toilets shoul d be low-level, pedestals al l o wi n g easy cleaning of the floor beneath.
They should be white or pastel colored. Seats should be made of an i m p e r v i o u s
material to facilitate cleaning. Toilet-roll holders should be of a thief-proof type.
Urinals may be the "open-slab" or individual bowl type, according to requirements.
Urinals should be equipped with an adequate automatic flushing mechanism.
Wash-hand-basins should be of the cantilevered type allowing easy access beneath for
floor cleaning. If cantilevered, the basin should either be recessed or be
fitted to allow a space of not less than 10 cm (4 in) between the back of the basin
and the wall. Wash-hand-basins may be in a continuous row, but where separated the
intervening space should be not less than 15 cm (6 in). Hot and cold running water
must be supplied to each basin.
Wall mirrors should generally be provided, but should not be placed above wash-handbasins. They should be adequately lit.
In women's toilets handbag shelves should be sited below wall mirrors.
Hand-drying facilities should generally consist of disposable paper towels or hot-air
dispensers. Where paper towels are made available, free-standing metal receptacles
should be provided for their disposal after use.
19 Nov2015
Page 5-3
Civil Aviation Authority, Bangladesh
5.5
Aviation Public Health Manual
Soap may be in either liquid or powder form, and the dispenser should usually be
sited within the width of the wash-hand-basin, but towards the right-hand side of it.
All women's toilets should have the facilities for the disposal and supply of sanitary
towels:
Drinking-water fountains should preferably be situated outside but adjacent to toilet
suites.
In or adjoining large toilet blocks provision should be made for a cleaners' locker
room complete with sluice. In all other toilet blocks, a cleaners' storeroom should be
provided.
The number of toilets required will, of course, depend u p o n t h e number of persons
using the airport, account being taken of increased demand at anticipated peak periods.
Facilities must be provided in the arrivals, departure and transit areas, restaurants and
all other sections open to the public. Provision s h o u l d be made for toilets specially
equipped for handicapped and infirm passengers.
Toilet cleaning
Toilets that are in constant use should have a permanent attendant whose main
function is to service the unit. He or she should replenish soap, towels, toilet paper,
etc., as required, and generally keep the place tidy; cleaning any fitting t h a t
b e c o m e s soiled. A cleaning schedule should be prepared for all toilet units,
whether the work is done by airport employees or by contractual labour. The person
responsible for maintaining the toilets should appraise the efficiency of the cleaning
materials used and make sure that they do not damage surfaces. The toilets should
be kept in a good state of repair and decoration.
5.6
Toilet cleaning schedule: A cleaning schedule should include the following tasks:
Remove all soiled towels and other rubbish to refuse store.
Clean wash-hand-basins, taps, shelves, mirrors, pipe work, metal work and all fittings.
Clean and disinfect all toilet pans, urinals and drain gullies.
Wash floors, splash backs, pedestals and seats, including under-sides.
Replenish towels, soap, toilet paper and sanitary towels.
Wash walls, doors, windows and light fittings
Cleaning materials should include an efficient detergent/ germicide/odour-counteragent.
The frequency of cleaning should be flexible, and extra cleaning-i.e., over and above the
requirements specified earlier should be carried out on demand if an inspection reveals
the need.
(Ref: Chapter 6.1, WHO guide to hygiene and sanitation by James BAILEY, 1977)
5.7
Vector Control in Airport
Passengers and crews must be protected against diseases spread by insects. Given the
speed of present day aircraft, it would be possible to fly several times round the world
within the incubation period of these diseases. This emphasizes the need for the rapid
detection and destruction of the responsible vectors. The control of mosquitoes, flies,
other insects of health significance and rodents is of particular importance at the airports.
19 Nov 2015
Page 5-4
Civil Aviation Authority, Bangladesh
5.7.1
5.7.2
5.7.3
Aviation Public Health Manual
Mosquito control
Rooms used by the passengers and crews in transit at international airports should be
effectively mosquito proofed as there is prevalence of mosquitoes and flies in
Bangladesh. Care should be taken to screen all openings, including doors, windows, air
ducts, floor drainage holes at the base of the walls and any other apertures. Measures
should be taken daily to destroy any mosquitoes that might have gained entrance.
Residual sprays containing an insecticide to which the local mosquitoes are susceptible
should be used on walls and ceilings, particularly in sleeping areas. Spraying should be
done at regular intervals.
Protection against mosquitoes is often attained more completely and satisfactorily by
destroying their breeding places or killing the insects in their larval stages by Mineral
oils, Paris green or synthetic insecticide etc. To accomplish this, the entire area within the
mosquito flight range of buildings used by crews and passengers should be brought under
control by ditching, drainage, filling, and elimination of water containers, or by the
application of larvicides.
Mosquitoes are to be controlled by fogging spray of DDT, Linden, Malathion or OMS-33
outside the terminal building. Inside terminal building ULV spray is to be carried out
without causing discomfort to passengers.
Aedes aegypti mosquito is the vector of Dengue and yellow fever, present either inside
the airport perimeter or within a zone of 400 meters outside the perimeter. To keep the
area within the perimeter of an airport free from Aedes aegypti and other vectors in their
larval and adult stages, it is necessary to maintain active antimosquito measures within a
protective area extending for a distance of at least 400m outside the perimeter.
Malaria is transmitted by Anopheles mosquitoes which is also prevalent in our country,
need to be cared of. From a practical standpoint, airports and transit areas should be
mosquito-proofed in the interest of the comfort, convenience and safety of air crews and
passengers. So the periodic spraying of buildings particularly the interior of the sleeping
quarters is highly desirable.
Flies Control
Flies that may carry the germs of filth borne diseases are frequently responsible for the
contamination of food supplies. They often breed in filth, manure, offal and decaying
organic matter and on prepared food, in which the germs may multiply greatly
particularly if food stands at room temperature for several hours.
In addition to flies, insects such as ants, cockroaches etc thrive on organic matter; they
may contaminate and cause considerable damage to food supplies. The measures needed
to keep these insects under control are the observation of scrupulous cleanliness and the
storage of food in proper containers, supplemented by the application of chemicals.
Control Measures
The best method of controlling flies is to eliminate the natural breeding places combined
with a scrupulous cleanliness of the airports.
Spraying airport buildings by pyrethrins combined with other toxic agents
Spraying inside airport buildings with residuals sprays containing DDT, HCH or other
suitable insecticide recommended by WHO.
19 No2015
Page 5-5
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
In case of resistant strain of flies, good control may be obtained by using suspended cords
treated with organ phosphorus compounds.
It is important to dispose of organic wastes, including liquid waste containing organic
matter, in such a way as to eliminate any possibility of fly breeding.
Other breeding places like kitchen slops, decaying fruits, open septic tanks, human and
animal excrement, or even lawn clippings to be given due importance.
5.8
5.8.1
Rodent (Rats) Control in Airport
History shows that the rats follow the arteries of commerce, and as more and more goods
are moved by air they are increasingly likely to become internal air travelers. They do
much damage, particularly in food storage premises. Rats often carry fleas as a Plague
vector. To keep the airport free from filthy activities of rats, following preventive
measures need to be taken:
5.8.2
Preventive Measures
Rats harbourage, the places where rats can establish nests or find concealment to be
eliminated.
Proper storage of foodstuffs to be done so that they are denied access to any sort of
nourishment.
Rat proofing structures can keep them out of buildings altogether.
Use of poisons can reduce rat populations.
Improvement of general cleanliness and good housekeeping can successfully control rats.
All refuses, debris and similar wastes should be removed frequently.
All materials-food or otherwise should be stored above ground or floor level, stacked in
orderly piles or in bins.
DDT or some other suitable insecticide powder should be used to dust all suspected areas
so as to destroy all rat fleas if available.
Night personnel on duty in airports should close doors tightly so that the rats cannot
passing through.
A strong light shining down on the threshold may discourage rats from running through
an open door.
Outdoor accumulations of refuse should be removed as promptly as possible.
Food or garbage stored out of doors should be kept in closed containers made of rat proof
materials.
(Ref: WHO guide to hygiene and sanitation in aviation 2009 Chapter 10.2)
5.9 Inspection of airport facilities
Regular inspections by health authorities at intervals not exceeding one month are
advisable, but the frequency may be varied according to the conditions found on
inspection.
19 Nov 2015
Page 5-6
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
5.10
Cleaning of Public areas in airport.
5.10.1
Public areas and room
3.10.1.1
Post hand-washing signs to encourage good hand-washing practices
staff and guests.
5.10.1.2
5.10.1.7
5.10.1.8
Use disposable paper wipes for cleaning to avoid the possibility of crosscontamination.
Use the proper chemical sanitizing agent, following the manufacturer’s
instructions concerning contact time.
Frequently clean and sanitize handrails, handles, telephones and any other hand
contact areas, elevators and landings in all passenger corridors.
Frequently clean and sanitize all public rooms.
Clean carpets using a steam cleaner that achieve a minimum temperature of 71°C
unless the floor coverings are not heat tolerant (some carpets can be steamed only
to 40 °C; otherwise shrinkage and colour runs may occur).
Frequently clean and sanitize garbage cans.
Clean and sanitize soft furnishings; steam clean if the items are heat tolerant.
5.10.2
Public restrooms
5.10.2.1
Post hand-washing signs to encourage good hand-washing practices among all
staff and guests.
Frequently clean and sanitize door handles, toilet flushers, faucets, dryers,
counters and any other hand contact areas.
Provide either an air dryer or disposable paper towels for hand-drying (only
single-use cotton towels should be utilized).
Check levels of soap and paper towels.
Use disposable paper wipes for cleaning to avoid the possibility of crosscontamination.
Use the proper chemical sanitizing agent following the manufacturer’s
instructions concerning contact time.
Restaurants and lounges
5.10.1.3
5.10.1.4
5.10.1.5
5.10.1.6
5.10.2.2
5.10.2.3
5.10.2.4
5.10.2.5
5.10.2.6
5.10.3
5.10.3.1
5.10.3.2
5.10.3.3
5.10.3.4
5.10.3.5
5.10.3.6
5.10.3.7
19 Nov 2015
among all
Post hand-washing signs at each hand sink to encourage good hand-washing
practices among all staff and guests.
Require staff to wash hands frequently.
Provide hand sanitizers to staff to complement good hand-washing practices.
Self-serve unpackaged items (e.g. peanuts, water) should not be available to
guests.
Provide snacks on request, in small individual containers.
Frequently clean condiment containers that are served by staff (recommended to
clean between each customer use).
Use disposable paper wipes for cleaning to avoid the possibility of cross
contamination.
Page 5-7
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
5.10.3.8
Clean and sanitize all tables and chairs with a detergent solution and sanitizer
(with correct contact time) after each shift and after closin
5.10.4
Spas and salons
5.10.4.1
Post hand-washing signs to encourage good hand-washing practices among all
staff and guests.
Require staff to wash hands frequently.
Use disposable paper wipes for cleaning to avoid the possibility of crosscontamination.
Use the proper chemical sanitizing agent following the manufacturer’s
instructions concerning contact time.
As per routine practices, ensure that common-use tools and materials are cleaned
with detergent and sanitized after each use (e.g. combs should be kept in
sanitizing solution that is regularly refreshed).
Fitness centre
5.10.4.2
5.10.4.3
5.10.4.4
5.10.4.5
5.10.5
5.10.5.1
5.10.5.7
Post hand-washing signs to encourage good hand-washing practices among all
staff and guests.
Require staff to wash hands frequently.
Use disposable paper wipes for cleaning to avoid the possibility of crosscontamination.
Use the proper chemical sanitizing agent following the manufacturer’s contact
time.
Frequently clean and sanitize all surfaces.
Post signs to remind users to wipe down equipment with provided sanitizing spray
after use.
Clean and sanitize equipment at least once during each shift.
5.10.6
Games rooms
5.10.6.1
Post hand-washing signs to encourage good hand-washing practices among all
staff and guests.
Require staff to wash hands frequently.
Use disposable paper wipes for cleaning to avoid the possibility of crosscontamination.
Use the proper chemical sanitizing agent following the manufacturer’s
instructions concerning contact time.
Frequently clean and sanitize all surfaces.
Clean and sanitize equipment at least once during each shift, paying special
attention to control sticks, handles, knobs and buttons.
It is the responsibility of airport authority to provide a hygienic environment for
passengers. Areas where food is prepared, stored and served, any surfaces
commonly touched by people and washroom facilities, among others, should be
kept free from contaminants that might compromise human health, even when
there is no identified outbreak of disease.
5.10.5.2
5.10.5.3
5.10.5.4
5.10.5.5
5.10.5.6
5.10,6,2
5.10.6.3
5.10.6.4
5.10.6.5
5.10.6.6
19 Nov 2015
Page 5-8
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
Prevention or mitigation of disease transmission is the goal. Hygienic conditions
also minimize the likelihood of infestation by rodents, as vectors of disease.
(WHO guide to hygiene and sanitation in aviation 2009, Annex-E)
5.11
Core capacity requirements for designated Airports
As WHO member state the designated Hazrat Shahjalal International Airport is to
develop core capacities as per Annex 1B of international Health Regulations
(2005) within the stipulated timeframe given by WHO.
5.11.1
The capacities: At all times
5.11.1.1
To provide access to:
an appropriate medical service including diagnostic facilities located so as to
allow the prompt assessment and care of ill travellers, and
adequate staff, equipment and premises;
5.11.1.2
To provide access to equipment and personnel for the transport of ill travellers to
an appropriate medical facility;
5.11.1.3
To provide trained personnel for the inspection of conveyances;
5.11.1.4
To ensure a safe environment for travellers using point of entry facilities,
including potable water supplies, eating establishments, flight catering facilities,
public washrooms, appropriate solid and liquid waste disposal services and other
potential risk areas, by conducting inspection programmes, as appropriate; and
5.11.1.5
To provide as far as practicable a programme and trained personnel for the control
of vectors and reservoirs in and near points of entry.
19 Nov 2015
Page 5-9
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
Figure: 5.1: PoE core capacity – At all times (routine)
5.11.2 : The capacities: During Public Health Emergency of International Concern
(PHEIC)
The followings requirements are to be developed responding to events that may constitute
a public health emergency of international concern
to provide appropriate public health emergency response by establishing and maintaining
a public health emergency contingency plan, including the nomination of a coordinator
and contact points for relevant point of entry, public health and other agencies and
services;
to provide assessment of and care for affected travellers or animals by establishing
arrangements with local medical and veterinary facilities for their isolation, treatment and
other support services that may be required;
to provide appropriate space, separate from other travellers, to interview suspect or
affected persons;
to provide for the assessment and, if required, quarantine of suspect travellers, preferably
in facilities away from the point of entry;
19 Nov 2015
Page 5-10
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
to apply recommended measures to disinsect, derat, disinfect, decontaminate or otherwise
treat baggage, cargo, containers, conveyances, goods or postal parcels including, when
appropriate, at locations specially designated and equipped for this purpose;
to apply entry or exit controls for arriving and departing travellers; and
to provide access to specially designated equipment, and to trained personnel with
appropriate personal protection, for the transfer of travellers who may carry infection or
contamination.
Figure 5.2: PoE core capacity during Public Health Emergency of International Concern.
(Ref: International Health Regulations-2005, Annex 1B)
19 Nov 2015
Page 5-11
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
THIS PAGE INTENTIONALLY LEFT BLANK
19 Nov 2015
Page5-12
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
CHAPTER 6
Food Safety in Aviation
6.1
General
Food hygiene has been defined as t a k i n g all the measures necessary for ensuring the
safety, wholesomeness and soundness of food at all stages-from its growth,
production or manufacture to its final consumption. The objective of food hygiene
practice consists in the production and serving of food as free as possible from
contaminants, including toxic substances, thus ensuring that its consumption will not
cause illness. Passengers often assess an airline by the quality of the meals served on
board. Commercially, therefore, it is important to provide food that is safe, of high
quality, palatable, and attractively served. Food is responsible for the transmission of
a large number of illnesses which should be kept into consideration during serving to
the passengers and crews.
6.2
Safe food supplies
6.1.1
Raw m a t e r i a l s must be of the highest quality obtainable. It should always be stored
separately and prepared in separate areas from cooked foods to prevent the risk of
cross-infection.
6.1.2
Certain foods present special risks, since they provide good media for the growth of
bacteria that cause food poisoning. These include any perishable food that consists
in whole or inert of milk or milk products, eggs, meat, poultry, fish, shellfish, or
other ingredients capable of supporting the rapid and progressive growth of infectious
or toxigenic microorganisms. The danger of environmental contamination and crosscontamination from raw meat, poultry and seafood to cooked foods cannot be
overemphasized. Mussels, crabs, oysters, prawns and other shellfish should not be
used unless it is certain that they are fresh and have been obtained from uninfected
sources.
6.1.3 Quality control o f food
The bacteriological control of meals served in flight presents a practical difficulty.
With the exception of frozen meals, kept till after a laboratory examination h a s
b e e n completed, meals generally will have been consumed before the results of
such examinations. Foods from all catering premises at airports serving passengers
and the public at large, as well as those from premises at airports or elsewhere that
p rovide in-flight meals for both crews and passengers, should be subject to
surveillance and regular sampling. At the minimum, the foods most likely to be
contaminated with pathogenic organisms should be sampled on a routine
monthly basis.
Foodstuffs less likely to be infected need not be sampled so
frequently.
This routine sampling should reveal any unsatisfactory conditions, which, if present,
would necessitate extra sampling to determine their cause. In cases of suspected food
borne infections, emergency sampling will be necessary.
19 Nov 2015
Page 6-1
Civil Aviation Authority, Bangladesh
6.4
Aviation Public Health Manual
Airport catering establishments
The Airlines or the catering contractors in some cases prepare foods to serve either in
airport restaurants, cafeterias and snack bars for consumption by passengers, air crew,
members of the public and airport personnel, and
T h e standards of hygiene, specifications, and handling techniques wil l be t he sa me
bot h for flight catering kitchen as well as ground catering.
The principal difference between the two categories of catering is that generally food
for consumption on the ground is prepared more or less on demand, or only a short
time before it is served. It is usually prepared and cooked in a part of the premises
where it is to be consumed. On the other hand, food for aircraft meals is prepared in
premises other than those in which it will be consumed often thousands of miles
away; many hours or, in the case of frozen meals, many weeks will elapse before
it is eaten. However, with the increasing use of frozen meals, or, as the method is
described, "cook freeze catering", the two types of catering technique are drawing
closer together.
Certain precautions must be followed to ensure that the control and high standard is
maintained in the catering establishment during preparation of food:
6.4.1 These precautions are:
6.4.1.1
6.4.1.2
6.4.1.3
6.4.1.4
6.4.1.5
6.4.1.6
6.4.1.7
6.4.1.8
6.4.1.9
6.4.1.10
6.4.1.11
19 Nov 2015
Containers in which food is delivered should be stored in a clean dry area;
they should not be used for any other purpose and should be returned at the
time of the next delivery.
Caterers should be careful not to overstock, so that all food can be u sed
within its shelf life.
Meals should be planned well in advance, which will assist in correct stock
rotation.
All food must be used in strict rotation: packs should therefore be properly
date marked or coded with the date of p roduction.
Meals that are to be frozen should be transferred to a deep freeze without
delay.
Any foods whose temperature has risen to -10 ºC or above during
storage should not be used until bacteriological and physical examination
shows them to b e satisfactory. Discs indicating temperature change can be
helpful in this respect.
For storage of up to 3 months, food should be kept at temperatures ranging
between 8 °c (0 °F) and -23 °C (-9 °F).
When food is to be regenerated, frozen packs should be put straight into a
convection oven or steamer after removal from the deep freeze.
The number of meals placed in ovens should not cover an entire meal period but
should be staggered to meet anticipated demand.
Meals should be served as quickly as possible after the reheating cycle is
completed.
It must be realized that, once regenerated, frozen foods will deteriorate at the
same rate freshly cooked foods (or sometimes at an even faster rate).
Page 6-2
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
6.4.1.12 Any food prepared in excess of consumer requirements must not be reheated more than
once.
Flight catering kitchens
6.5
6.6
Flight catering should always be carried out quite separately and in a different building
from ground catering, unless by structural arrangements effective separation can be
achieved in one building. Aircraft meals need to be supplied from kitchens that are:
Under the direct control of the airline; or
Staffed and controlled by a catering concessionaire but permanently supervised by the
airline. Airlines should not uplift foods from a caterer that holds a monopoly business and
prepares food in poor hygienic standards.
Airlines, in addition to health administrations, have a duty to inspect and collect food
samples for bacteriological and other examinations.
Airports Hotel / restaurants
Hotels in which crews and passengers are accommodated are another important source
of food supplies, which should not be overlooked. It is pointless to demand high
standards of food hygiene at airports and in flight catering, if contaminated food is
eaten at hotels. In fact, a difficulty in investigating alleged food borne illness occurring
in flight or after arrival is to decide from which source the food was supplied. The
standards of hygiene therefore apply equally to airport, flight and hotel catering.
(Ref: Who guide to hygiene and sanitation in aviation, Chapter 4.1-4.3)
6.7
Flight catering premises
Premises where food or beverages are stored, prepared or served should be roomy
enough to avoid congestion and allow for possible expansion of operations; they
should be constructed in such a manner and of such materials that they can be kept
scrupulously clean and provide protection against the ingress and harbourage of rodents
and insects.
Provision should b e made for adequate lighting and ventilation, b o t h natural and
artificial, an adequate supply of potable water and drainage facilities.
Flight catering premises should be sited at airports or in their vicinity and as near as
possible to the aircraft departure parking area.
6.7.1
Construction
The structure should be of brick, concrete, or some other substantial material. The
building should be designed to permit easy and adequate cleaning, and kept in good
repair. Partitions within the structure should be kept to a minimum in order to
facilitate the use of mechanical cleaning equipment.
6.7.2
Floors
Floors must be even impervious, without cracks or open joints, smooth (but not
slippery), hard wearing and easy to clean.
19 Nov 2015
Page 6-3
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
Floors should slope evenly towards drainage outlets, a sufficient gradient being 2.5 cm
in 3m (1 inch in 10 feet).All drainage outlets should be trapped. Suitable materials
for floors are terrazzo, quarry tiles or granolithic chips bedded in concrete. Light
colours are recommended. They look attractive, reflect light and show up dirt.
5.7.3 Walls
Walls should be light coloured and made of a substantial, durable, smooth, impervious
and washable material. They should be free from ledges or projections, which
collect dust, and be tiled, preferably from floor to ceiling, but if this is not possible
then to a minimum height of 1.5 m (5 ft) from the ground and coved at the top.
Surfaces that are not tiled must be finished in plaster and painted (preferably in a
washable mat finish). Gloss paint may be used in dry goods storerooms. The parts
of walls surrounding sinks should be tiled.
6.7.4 Ceilings
The ceiling must not harbour dirt; it should be easy to clean and-most
important-should absorb moisture. The most suitable ceiling is an under drawn,
plastered ceiling with a smooth continuous lower surface unbroken
by beams.
Junctions
with
walls should
be coved. The ceilings of kitchens should be
insulated. They can then be finished with a hard gloss paint. Paint must not be
used on a ceiling that is not insulated. In this case an absorbent colour wash is
recommended.
6.7.5 Joints
All internal joinery should be of simple design. Joints should as far as possible be
tight and flush-fitting. The woodwork surrounding doors, windows and other
openings should be fixed to the internal wall surfaces so as to avoid open joints.
All internal joinery work- which should be kept to a minimum-should be
finished with a hard gloss surface.
6.7.6 Doors
Doors should be flush-fitting without panels or ledges. They should open outwards
and be self-closing. The bottoms of doors should be protected on both sides with
metal kicking-plates.
6.7.7 Windows
Windows should be so sited as to facilitate cleaning on both sides, and panels
should be large rather than small. Internal window sills should be splayed at an
angle to prevent their use as shelves.
6.7.8 Ventilation
Adequate ventilation is essential. A current of air sufficient to keep the room cool
and remove the fumes and steam is required.
Complete air conditioning is
recommended wherever possible. Natural ventilation may be sufficient only in certain
kinds of weather, and artificial ventilation should therefore be available to
supplement or replace it when necessary.
19 Nov 2015
Page 6-4
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
All cooking apparatus (e.g., steamers, fryers, grills, and ovens) should be fitted with
hoods and extraction units to draw off fumes, steam and heat. These hoods should
be constructed in such a way that they are easy to clean. however possible,
ventilation ducts should be fitted flush with walls or ceiling; if this requirement
cannot be met sufficient space should be left between the ducts and the wall to
allow for all round cleaning. Duct inlets should be insect proof. Inlet screens
should be removable for cleaning.
6.7.9
Lighting
All parts of the premises must be adequately lit so that there are no dark passages and
corners.
The window area should equal at least one- fifth of the floor area.
Artificial lights should be so placed that both glare and shadow are avoided. A
number of small points produce less glare than one large point. There should be
lights over food preparation tables, sinks, and all other kitchen working areas.
Fluorescent lighting is recommended.
6.7.10 Protection against insects and rodents
All windows, doors and other openings should be insect-proofed with material having
at least 6 meshes per cm (16 meshes per inch). Plastic insect-proof screening is
recommended.
Kitchen entrances should have self-closing double doors opening
outwards. All buildings should be rodent-proof.
Regular inspection and disinsecting should be practiced to prevent the
contamination of foodstuffs by flies, cockroaches, ants and other in- sects.
Disinsecting may be carried out by spraying, fumigation, the treatment of walls with
insecticidal paint, the use of repellent dispensers, or the use of electrically operated
equipment that emits ultraviolet rays, thereby attracting insects, which are then killed
by contact with an electrified grille.
All rodenticides, fumigants, insecticides or other toxic substances should be stored
in locked cabinets and handled only by authorized persons to prevent the possibility
of food contamination.
6.7.11 Exclusion of’ domestic a n i m a l s
Dogs, cats and other domestic animals should be excluded from all parts of the
food premises.
6.7.12 Water s u p p l y
Adequate supplies of both hot and cold running water are essential. All water used in
food preparation premises should be potable. As it is inadvisable to provide hot water
for general purposes throughout the premises at temperatures above 60ºC, provision
must be made for the temperature to be raised to 82ºC for the sanitization of dishes
and utensils.
6.7.13 Dish washing
Mechanical dish washing is recommended to enable the correct temperature of 82º C
(180 °F) to be achieved.
19 Nov 2015
Page 6-5
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
Where dish washing is carried out by hand, two sinks, or preferably three, should be
provided. Sinks and draining boards should have a smooth, hard, even surface and be
constructed of porcelain finished fire clay, stainless steel or plastic. Wooden sinks and
draining boards should not be used.
6.7.14 Pan washing
When pan washing is done manually, at least two, or preferably three, sinks of
large capacity are required. The size of each should be at least 75cm x 60 cm x 60 cm
(30 in x 24 in x 24 in). Grease traps should be fitted to the drain taking the waste
from the sinks. Alternatively, completely automatic washing machines may be used for
the cleansing and sanitization of pots, pans, large baking utensils, etc. Several
designs are available, but each type should provide for washing with a detergent
solution at 60-70º C (140-160 ºF) and a rinse with clean hot water at 82º C (180 ºF).
6.7.15 working surfaces
Surfaces should be impervious to liquids, smooth and easily cleaned. Those with which
food comes into contact should be made of a material that is nontoxic and is not itself
affected by such contact. Stainless steel, marble or laminated plastics are suitable
materials. The bottom shelves of tables must be at least 15 cm (6 in) above the floor, to
permit easy cleaning. These furnishings should be of simple design and free from
crevices, cracks and corners in which dust can collect. They should be mobile for easy
cleaning and capable of withstanding repeated cleaning by nor- mal methods.
6.7.16 Cupboards
Cupboards should be metal and simple in design. If the sides fit tight to the wall there
should be no back. Otherwise they must be mobile so that the backs can be easily
cleaned. The whole interior must be accessible for cleaning. Shelves should be
removable for regular cleaning
6.7.17 Cooking apparatus
Cooking apparatus should be located in the centre of the kitchen, with access all
round. Supply and waste pipes, etc., must be so placed as to facilitate cleaning. The
lagging of hot-water pipes should only be coated with substances that set hard and are not
affected by temperature changes.
6.7.18 Refrigerators, cold rooms, etc.
Refrigerators and cold rooms should be as far away as practicable from sources of
heat. The internal surface should be smooth, impervious and easy to clean. Each
cold room must have a readily visible means of reading the internal temperature and
a warning device to pre- vent the door from being left open. A sealed trapped gulley
should be provided to drain away liquid during defrosting. All racks should be
removable and easy to clean. Internal surfaces and racks should be made of metal.
19 Nov 2015
Page 6-6
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
The temperature of refrigerators and cold rooms should not exceed 4° C.
Thermometers should be sited in the warmest zone of the refrigerated area. The
temperature of deep freezes should not be above -18 ºC. For long-term storage
(i.e., for periods of more than 3 months) the temperature should be between 26 ºC and -29 ºC.
6.7.19 Food storage
All food stores should be dry, well lit, well ventilated, vermin-proof and clean, and
situated away from sources of heat, both natural and artificial. All racks and shelves
should be easily removable for cleaning operations. The bottom shelf must b e at
least 15 cm (6 in) from the floor to allow air circulation. If the shelf is fixed and
wider than 30 cm (12 in), it may need to be higher to permit cleaning. Foodstuffs must
not be stored directly on the floor, even if they are in boxes or cartons.
6.7.20 Drainage
Drainage should be sufficient to remove all waste water without the use of floor
channeling.
If channeling is unavoidable, it should be uncovered, constructed in
glazed earthenware and self-cleaning. All drains must be large enough to carry peak
loads. They should be adequately trapped and ventilated. The drainage system
should be so constructed as to allow no risk of the contamination of potable water
supplies by liquid wastes. Drainage and disposal must conform to local and national
bylaws and building regulations.
6.7.21 Garbage Storage
Waste should be kept in covered bins or disposable paper or plastic sacks p r ovided
with a foot operated hinged lid. Full bins or sacks should be removed from the
kitchen promptly and their contents suitably disposed of. Bins must be covered at
all times. If waste food is to be used for animal feed, it should be stored separately
from garbage. Provision must be made for the washing and disinfection of used
garbage bins.
Garbage bins should never be washed or stored in the vicinity of
aircraft containers used for human excreta, since, when in use, they are placed near or
inside food preparation areas and may be handled by catering staff.
6.7.22 Staff cloakrooms
Staff cloakrooms should provide, separately for each sex, toilets and wash-handbasins, i n d i v i d u a l lockers for clothes and changi ng rooms with showers. The
toilet areas should be well lit and ventilated and not open directly on to a food area.
Kitchen staff should only be able to enter the food premises after passing through
t h e changing rooms and wash rooms.
There should be 1 wash-hand-basin for every 10 persons, each basin being provided
with hot and cold water, soap, nail brush and disposable towels. There should be 1
toilet for every 20 persons if the number of staff does not exceed 100, and 1 for
every 25 persons if more than 100 are employed. For male workers the proportion of
toilets may be slightly reduced if an adequate number of urinals are also available.
19 Nov 2015
Page 6-7
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
Toilets for women staff should be provided with a satisfactory means for the disposal
of sanitary towels. Notices must be fixed in conspicuous positions in all
cloakrooms requesting persons to wash their hands after using the toilet. There
should be at least 1 shower for every 75 persons, but in hot countries the proportion
of showers should be increased.
In addition to facilities in cloakrooms, there must be an adequate number of
wash-hand-basins conveniently located throughout the premises. At least one
should be available in each section-e.g., in the bakery, cold kitchen, and meat
preparation area. They should also be provided with hot and cold water, soap, nail
brushes, and towels (preferably of the single-use disposable type). Liquid soap should
be supplied from a metal or polyvinyl chloride dispenser. conveniently sited, vandalproof, easy to clean, and delivering the correct quantity for adequate washing. Pedaloperated spray taps are an added precaution to prevent cross-contamination. Sinks in
kitchen areas should not be used for washing hands.
(Ref: Annex 9, Chapter 4.4)
6.8
Food handlers
Persons who are suffering e i t h e r from a disease capable of being transmitted by
food or water or are carriers of such a disease should not be employed in food
preparation or food handling.
Food handlers should be kept under regular surveillance. Staff who have infected
wounds or sores or are suffering from gastrointestinal illness or any other condition
likely to cause the c ontamination of food or food contact surfaces, or who have been
in contact with a person suffering from a food or waterborne disease, should report
immediately to the management; they should be excluded from food handling until
given medical clearance to return to work.
All persons applying for jobs as food handlers should undergo a pre- recruitment
medical examination and a professional assessment should be made of their clinical
history. Only those who are free from infec tion and are proved not to be carriers
should be engaged. While this will ensure that at the time of recruitment the food
handler is healthy, it is important to impress on employees their obligation to report
any of the above-mentioned conditions should they occur during employment.
6.8.1 Training
All food handlers should receive training in food hygiene. Such training should
be given by specialist officers employed by airlines, or by officers of the health
authority, or by both. Lectures, supplemented by films and visual aids, should be
arranged to suit the various grades and duties of the personnel.
All food handlers should receive basic instruction in hygiene in its application to the
work they do, company regulations and procedures, health requirements, use of
equipment, use of protective clothing, code of practice in handling food, reporting of
sickness, personal hygiene, and general hygiene standards in working areas.
19 Nov 2015
Page 6-8
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
Those staff responsible for particular duties should receive additional instruction. For
example, storekeepers must be taught about the practice and value of stock rotation
and temperature control; cleaners should be taught correct practices for storing
cleaning materials, techniques of using equipment and materials, the reasons for strict
adherence to cleaning schedules, and the correct way to report faults in addition to
basic training, should learn the rudiments of bacteriology and how to prevent
contamination.
6.9
Food preparation
Raw materials should be washed to remove soil or other contaminants.
Green
salads should be soaked for 5 minutes in a 50 mg/1 solution of sodium hypochlorite,
and then thoroughly rinsed in running potable water.
This is of Particular
importance when the produce concerned has been grown in countries where human
excreta is used as a fertilizer.
The vegetables may be washed in an ordinary
vegetable sink if the more sophisticated equipment is not available.
Meals should be prepared as near as possible to the time of consumption, unless they
are to be deep frozen. However, except in very small units preparing food for one
service at a time, flight meals have to be ready several hours before departure time.
Special precautions must therefore be taken. In order to prevent the introduction of
pathogenic organisms, or the proliferation of those already present, temperature control is vital. After foodstuffs are removed from storage, they should be prepared
and cooked as soon as possible. It is important that frozen raw foods-particularly
poultry and seafood-must be completely thawed before cooking to ensure adequate
heat penetration and the destruction of any pathogenic organisms present.
Immediately after cooking, the food should be placed in the meal trays. For hot
meals on short-haul operations, the trays should be put into hot ovens so that the
temperature of the food never falls below 63ºc (145 ºF). It would be preferable if a
temperature of 74 º c (165º F) could be attained. This applies when the aircraft
departure is not more than, say 1 hour later. For later departures the meals, after
having been cooled quickly should be placed in a cold-room in which the
temperature is not more than 4 ºC (40 °F). Here the food should remain until it
is time to load the aircraft. It should then be placed in electric aircraft ovens
already heated to above 85ºC (185 °F) .
For long-haul operations both hot and cold meals must be placed in a cold-room at
4º C (40 ºF) and remain there until required. Food is constantly being moved into
and are frequently opened. To counteract this, entrances should be protected by the
installation of a cold-air curtain, or double-door entrance, the former being preferable.
Food should not be held longer than 24 hours in cold- rooms.
Meals should be transported at 4ºC (40 ºF) to the aircraft. This temperature can be
maintained by placing the trays in modules and surrounding them with dry ice.
Meals that are to be served hot are transferred into ovens on the aircraft for rapid
reheating. Aboard aircraft, cold meals should be held at temperatures below 10ºC
(50ºF) and hot meals at temperatures above 63 ºC (145 ºF).
19 Nov 2015
Page 6-9
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
If meals that are to be served hot are not to be heated shortly after takeoff, they
must be kept at a temperature below 10ºC (50 °F) until they are placed in ovens.
Meals that are to be supplied in a frozen state either to the aircraft or in bulk to
outstations should, as soon as possible after cooking and dishing, be stored in a
deep freeze at a temperature not exceeding -18ºc (0 °F). Food for long-term storage
should be kept at temperatures ranging between -26 ºC and -29ºC (-15 ºF and -20
°F).
6.9.1
Cross-infection
A potential hazard is the possible transference of bacteria from raw foods to cooked
foods either by human contact or by contact with equipment.
Raw foods should preferably be handled by different personnel in a separate section
and with different equipment from that used for cooked foods. If this is not possible,
after raw food has been handled, the operative's hands, and all knives, cutting boards,
slicing machines, work surfaces and utensils and equipment must be washed and
sterilized before contact is made with cooked foods.
6.10
Prevention of contamination
6.10.1 Hands Care
Hands are the most common medium by which pathogenic organisms are transferred
to food from the skin, nose, bowel, etc., as well as from other foods. They should
therefore be kept scrupulously clean, and be thoroughly washed not only every time
after the toilet is used and after raw food (especially meat and poultry) is handled, but
frequently throughout the day. It has been shown that the use of an efficient and
approved bactericidal soap· helps to reduce the number of pathogenic organisms on the
hands . Fingernails should be kept short and clean.
The handling of food, particularly cooked food, must be kept to a minimum and
whenever possible tongs, spoons or forks should be used , or the hands t o b e
covered by disposable gloves. Some handling of food is, however, inevitable, which
again emphasizes the need for frequent hand washing. It is a worthwhile practice
to swab food handlers' fingers to check for organisms causing food poisoning in order
to assess whether the hand-washing routine or other procedures can be improved.
Any cuts, septic conditions or abrasions on the hands should be appropriately treated
and protected with a waterproof dressing. First-aid facilities should be provided to
meet these contingencies. Food handlers should be forbidden to spit and to use tobacco
in any form while in. food premises. They should endeavour not to cough or sneeze
in the vicinity of uncovered food.
No personal outer clothing and articles should be taken into food areas; they
should be stored in the locker rooms provided. Food storage, preparation, and
handling areas should not be used as changing rooms or sleeping quarters.
Protective clothing, including suitable head gear (e.g., hair net or cap), must always be
worn in food premises, and the clothing kept clean.
19 Nov 2015
Page 6-10
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
6.10.2 Steps of hand wash:
WHO recommended following steps of hand wash to clean soiled hands:
Wash hands when visibly soiled for a duration of 20-30 seconds. Apply a palmful of
liquid soap in a cupped hand/Soap with water , covering all surfaces. Rub hands palm to
palm; Right palm over left dorsum with interlaced fingers and vice versa; Palm to palm
with fingers interlaced; Backs of fingers to opposing palms with fingers interlocked.
Rotational rubbing of left thumb clasped in right palm and vice versa; Rotational rubbing,
backwards and forwards with clasped fingers of right hand in left palm and vice versa.
Once
dry,
your
hands
are
safe.
19 Nov 2015
Page 6-11
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
6.10.3 Equipment
All working surfaces should be kept clean. This includes not only tables, but articles
such as slicing machines, cutting boards, pastry mixers, utensils of all kinds,
crockery and cutlery, in fact anything with which food comes into contact.
Equipment and utensils should be so designed as to prevent the accumulation of dirt
and to permit easy and thorough cleaning. Wherever possible, equipment should be
mobile so that it can be moved during cleaning operations). Any equipment used for
the storage of inedible or contaminating materials should be suitably identified so that
it will not be used for storing edible products.
The use of disposable piping bags, gloves and head covers is recommended. Cutting
boards and butchers' blocks made from a synthetic rubber compound are
preferable to those made from wood, which often splits, thus providing an excellent
bacterial breeding ground or causing splinters to penetrate the food.
Fixed equipment and fittings should be positioned in such a way that either there re
no gaps which could harbor dirt or insects or every part is accessible for leaning
purposes. Service pipes to equipment should either be enclosed in accessible columns
or voids or be at least 15 cm (6 in) a b o v e ground level to enable the floor to be
cleaned. Most flight catering premises operate 24 hours a day 7 days a week.
Equipment is often in continual use, and cleaning becomes a practical problem,
particularly in the case of such items as ovens and grills. An other problem is
created by congestion, because demand has in many instances outstripped production
capacity. In such cases either a rota system must be introduced whereby equipment
can be taken out of operation for cleaning, or duplicate equipment must be installed.
In countries where flies present a problem, all openings from catering premises to the
external air should be screened with gauze, p referably nylon, with 6 meshes per
cm (16 per in). Doors should be screened and self-closing. Cold air curtains c a n
b e u s e d a t e n t r a n c e s instead of screens. However, insects may still get into
buildings, so regular inspection and treatment is necessary. For flying insects electric
exterminators, are very effective and have the advantage of retaining the dead
insects in a tray. They do, however, attract flying insects and should be positioned
near entrances.
Another piece of automatic equipment, which dispenses an approved insecticide
at regular intervals, has the advantage of repelling rather than attracting insects and
can therefore be located inside the premises.
6.11
Cleansing and sanitization of dishes and utensils
The cleansing and sanitization of non disposable dishes and utensils in flight
kitchens and airport restaurant and snack bar kitchens should be carried out, whether
manually or mechanically, on a routine basis. If the water is naturally hard, it is both
economical and advisable to install a water softener, particularly for mechanical dish
washing, to prevent the furring of jet nozzles.
Nov 2015
Page 6-12
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
6.11.1 Washing by hand
For manual cleansing and sanitization of dishes and utensils preferably three large
stainless steel or galvanized sinks, large enough to hold the biggest item, should be
used. Only in very small establishments are all utensils and dishes washed by hand.
In larger establishments manual cleansing and sanitization are usually confined to
cooking pots and pans, while items such as crockery, glasses, trays, and containers
are cleansed and sanitized by machine
The hot water supply should be abundant and delivered at temperature of 60 ºc
(140º F), so that a temperature of approximately 50 ºc (120 ºF) is available for the
cleansing of dishes and utensils by hand.
Prior to cleansing, waste food from dishes and utensils should be scraped into
covered waste receptacles. The dishes and utensils should then be soaked, scraped
and pre-rinsed in the first sink, in order to re-move remaining scraps of food,
grease and other deposits. Soaking should be carried out at a temperature
of approximately 45 ºC (115 º F). A recommended concentration of an efficient
detergent should be added to the water to emulsify fats.
Dishes and utensils should then be thoroughly cleansed in the second sink in
water maintained at a temperature of approximately 50ºc (120 ºF) (higher water
temperatures may scald the operators hands). The water, which should be
changed frequently, should contain an efficient detergent added at a concentration
that should be suited to the mineral content of the water. Dishes and utensils
should then be placed in long-handled wire baskets (required to prevent the scalding
of the operative's hands) for immersion, in the third sink, in clean hot water at a
temperature of 82ºC (180 ºF) for at least 2 minutes to ensure sanitization and to remove
detergent residues. The dishes and utensils should then be removed and left to dry
in the wire baskets. Drying towels are not necessary and should not be used, since
when they become soiled they may spread contaminating materials to other dishes
and utensils.
An alternative method is to use an efficient combined detergent/germicide for washing
and partial disinfection, followed by rinsing and hot- water sanitization. The product
is usually in such a concentrated form that it should be added by an automatic
dispenser to ensure correct dilution.
Use of excessive quantities of detergent is not only wasteful but may also irritate the
operative's skin. An efficient detergent/ germicide should:
be safe to use;
be immediately and completely soluble in hard or soft water;
be unaffected by alkalinity, acidity or organic matter;
be chemically neutral;
prevent deposits of mineral matter in hard water; and
leave no residue after rinsing and draining.
19 Nov 2015
Page 6-13
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
6.11.2 Mechanical washing
With the exception of the pan wash in larger establishments all items should be
washed by machine.
Utensils are fed through the machine on a moving belt. The first section is the wash
tank, in which the temperature of the water should be 60ºC (140 °F). At a higher
temperature food debris will tend to adhere to the utensil. Only a detergent of low
spumescence should be added to this tank usually by an automatic dispenser. The
next tank is the rinse tank, in which water at a temperature of 82 ºC (180 °F) is
sprayed through fine nozzle jets. The addition of chlorine to remove stains-except in
a concentration of less than 40 mg/1-is not recommended. It is unnecessary and
may damage metal components and cutlery. Machines should preferably have a
third section-a hot-air drying chamber, operating at approximately 100 ºC (212 °F).
Utensils are dry on exit from the machine or within a few seconds. To help the
drying process and to prevent water spots, a spirit-based rinse aid is added usually
by automatic means to the rinsing water. The machine should be provided
with temperature-indicating dials in all sections.
Water for dish washing machines should, if necessary, be softened, since hard water
will leave a deposit that causes a blockage of the jets. Dish-washing machines require
regular maintenance by skilled personnel. Jet arms should be dismantled and
cleaned daily. All dishes, glasses and other articles should be inspected after washing.
Any item that has not been satisfactorily cleaned should be rejected. (The proportion
of rejects may be as high as 25% .) These items should be placed in a special
soaking tank containing hot water and a detergent with chlorine added at a
concentration of approximately 40 mg/1. After soaking, the utensils should pass
once again through the dish washing machine.
Unsatisfactory washing may result if the machines used are faulty or badly maintained,
if the type of material of which the dishes or utensils are made is unsuitable, or if
their shape encourages the retention of debris in corners, etc. Food containers and
waste containers should also be washed by machine but at different times.
6.11.2.1 Cleansing of equipment
Fixed equipment, food preparation tables, shelves, etc., are washed by hand. The
same detergent/germicide can be used, mixed with hot water and applied either by
brush, where soiling is excessive, or by swabbing. For the latter procedure, strongtextured paper is recommended, which can be discarded after each piece of
equipment is cleaned. Fresh paper can then be used to dry and polish the cleaned
surface .All pieces of equipment that come into direct contact with food must be
cleaned at least at the end of each working period, and also when the opportunity
arises during break periods.
All food-slicing machines should be thoroughly
degreased and cleaned at the end of each working period with the use o f a
detergent/germicide. It may be necessary to degrease and clean cutting blades
during working periods. All other surfaces should be cleaned at least once daily,
and more frequently if necessary.
19 Nov 2015
Page 6-14
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
Mobile items such as trolleys should be removed to a cleaning bay for washing
either by hand, or with mechanical equipment using steam or high-pressure hot
water containing detergent. Trolleys should be washed in this way at least once a
week, and at all other times kept clean by wiping. Heavy equipment such as
cooking stoves, fryers, grills, and griddles will need carbon removers and heavy duty
detergents.
They should be washed daily and deep cleaned once a week.
Machinery that can be dismantled should be taken apart and washed daily.
6.12
Cleaning of Catering Premises
To ensure effective cleaning, walls, floors, doors, windows, ceilings and all other
parts of the structure must be kept in a good state of re pair. One person
preferably someone who is not
involved in food production and can therefore be
objective about priorities-should be made responsible for the cleanliness of the
premises. Cleaning may be carried out by persons employed directly by the air port
authority, by contractual service or by a combination of the two types of worker.
This last arrangement is the most common: usually floors, the lower parts of walls,
and equipment are cleaned by airport employees, and all the high level surfaces,
windows, ventilation apparatus, trunking and extraction hoods, etc., by contractual
cleaners.
An elementary but often overlooked requirement in catering establishments is a
storeroom for cleaning equipment and materials.
The storeroom should be
conveniently sited and have a hot and cold water supply and a large sluice sink.
The cleaning of premises should be carefully planned so that every part is dealt with
according to a schedule.
The cleaners should be fully instructed in the use of cleaning tools and materials and
in the dismant ling of equipment; they should also be made aware of the hazards.
Too often cleaners receive little or no training· and therefore do their work in a
perfunctory manner. In a recent publication it is pointed out that cleaning standards
deteriorate if the cleaning apparatus and equipment themselves are not kept in a
hygienic condition. This is a factor that is often overlooked. Equipment (such as
mops and brushes) that is to be used repeatedly should be strong enough to
withstand constant cleaning after use. Apparatus used for wet cleaning is likely to
become heavily contaminated with bacteria unless it is disinfected by heat or
chemicals. Normal washing will not remove all bacteria, and the organisms that remain
may multiply. Next tirne the equipment is used, instead of removing bacteria from
soiled surfaces, it will increase the bacterial load. The most effective treatment for
wet-cleaning apparatus is heat disinfection combined with laundering.
As previously mentioned, food preparation premises at airports operate on the basis of
a 7-day week, so the cleaning schedule should be arranged accordingly. The
following schedule is given only as an example; it may need to be varied to suit
local circumstances.
6.13
Food storage in the catering centre
The proper storage of food at all stages from the arrival of raw materials to the
departure of completed meals is most important, calling for constant and systematic
care by management and staff.
19 Nov 2015
Page 6-15
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
A recommended rule for storing food is: keep the quantity to an acceptable minimum,
keep it clean, keep it cool, keep it covered.
Keeping stocks to a minimum reduces the length of storage time and the risk of
deterioration. In all cases, however, stocks should be regularly inspected and a proper
rotation system installed. Access to food store rooms must be restricted and subject
to control.
The only food kept in food preparation areas should be that needed during the day.
Everything else should remain in the storeroom.
6.13.1 Cold storage
Cold storage facilities can be either free-standing cabinets for small quantities of
food or walk-in rooms for larger amounts. In each case the temperature should be
such that the food is kept at or below 4 ºC (40 °F). This means that the
refrigeration plant must be capable of reducing. the temperature to approximately 1
ºC (34 °F). All refrigerators should be provided with a thermometer, which should be
sited in the warmiest zone of the refrigerated space: Separate refrigerators should be
provided for the various types of food. Thus there should be one each for (a)
dairy products, (b) meat, (c) fish, (d) fruit, (e) vegetables, and (f) confectionary. To
avoid the risk of cross-contamination, cooked foods should not be stored in the same
refrigerator as uncooked foods. Refrigerators should not be so crowded as to prevent
good air circulation. (This is particularly important
in the
storage of
vegetables.) They should always be kept clean and tidy, but should be cleared
out and thoroughly washed at least once a week. Disinfectants should not be used,
as they may taint the food. Cleaning should coincide with defrosting, although
most modern refrigerators defrost automatically. In flight catering, refrigerated transit
and holding rooms are necessary. The former room is for the purpose of holding
the food prior to placing it on meal trays, and the latter for holding the completed
meals (on trays placed in containers) while awaiting transport to the aircraft
6.13.2 Deep freeze storage
The temperature of the food in deep freezes should never rise above -18ºc (0ºF), and
it should be possible to decrease the temperature to as low as -40 ºC (-40 °F) for
much longer term storage. Again, thermo- meters are necessary. To prevent rises
in temperature when the door is opened, access to the deep freeze must be carefully
restricted. In addition, there should be an anteroom to provide an airlock, which, if
con- trolled at a temperature not exceeding 4º C, will provide an additional cold
room. Proper stock rotation is necessary in order to avoid leaving food in the deep
freeze for such long periods that its nutritional value is lowered or physical changes
occur (e.g., loss of color). The length of time that food should be kept in the deep
freeze varies with the composition of the food, but for stock rotation 3 months could
be a standard for all aircraft meals.
The complete defrosting and cleaning of a deep freeze are a major task, and an
alternative store will be required in which to place the food removed during this
procedure.
19 Nov 2015
Page 6-16
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
It should therefore coincide with a time when stocks are at their lowest, and once
a year is probably sufficient. Automatic defrosting is essential to keep the deep
freeze operating efficiently. Hot food should not be placed in refrigerators or deep
freezes till it has first been cooled to a temperature not exceeding 30 ºC
(85 °F). Otherwise the temperature of food already present might be raised and
condensation produced, which reduces the efficiency of the refrigerator.
The
time this cooling takes is critical, because at temperatures between 30ºC and 50ºC (86 ºF
and 120 °F) bacterial multiplication is very rapid.
The cooling period should not exceed 2 hours. As far as meat is concerned, the larger
the cut the longer it takes to cool; smaller cuts are therefore r e c o m m e n d e d .
Mobile cooling cupboards a r e available to speed up the cooling procedure. Hot
foods should be placed in these cupboards, cooled down to temperatures of 4 OC (40
°F) and then placed in refrigerators, if not immediately required for service.
Prepared food, including aircraft meals, that is to be deep frozen for later use, should
be cooled to the storage temperature of -18 ºC (0 ºF) as quickly as possible to
minimize the evaporation of its water content. This loss will be much reduced if
the meal trays are covered with vapor proof material. The internal temperature of
the food should drop to -18ºc (0 ºF) within 90 minutes of the completion of
cooking. To help to achieve this rapid cooling, blast freezers are usually installed. Air
at temperature as low as -35 ºC ( -30 °F) is blown over the food. On removal from
the blast freeze, the food should go straight into the deep freeze.
6.14
Laboratory facilities at flight catering establishment
In addition to any control by the health authorities, it is desirable that all large
food production concerns, especially flight catering establishments, should possess
their own laboratory. This will enable all meals supplied to aircraft to be subjected
Individual items and processes can be checked as
to bacteriological control.
necessary, and at the time of production. In spite of their most willing cooperation,
national laboratories often have only limited resources, and full control can only be
achieved if a laboratory is provided at a flight catering unit.
6.15
Transportation of food to the aircraft
Aircraft meals have to be transported from the preparation premises to the aircraft,
and special vehicles are necessary in order to service all types of aircraft.
For hygienic reasons, the walls, ceiling, floor and doors of all vehicles used for
transporting food should be lined with metal or of some other approved smooth
impervious material. In tropical countries where the flight catering premises are not
at or adjacent to the airport, vehicles should be refrigerated. All vehicles should be
kept in good re- pair and in a clean condition.
After clean
vehicles are
waste food
rubbish-for
19 Nov 2015
equipment and food have been loaded on to the aircraft, the same
frequently used to bring away offloaded equip- ment, surplus and
remaining in the containers. They should not be used to carry away
example, the contents of
Page 6-17
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
waste bins. The catering vehicle should be washed out each time used equipment is
offloaded and prior to servicing other aircraft. In addition, at the end of each day, the
interior of the vehicle should be washed with a detergent/germicide solution.
6.16
Preservation of Food in Aircraft
Food for service to passengers is stored in the galley or pantry areas. The number of
pantries s h o u l d vary with the size and type of a ircraft, there s h o u l d b e a
separate galley for first-class passengers.
6.16.1 Meals may consist of:
cold food served on the trays previously laid out in flight catering: on the
aircraft they should be kept either in refrigerated modules or in containers
holding a small slab of dry ice;
hot meals on short-haul aircraft, which should be kept in heat-retaining ovens and
served almost immediately after take-off; or
hot meals on long-haul aircraft, which should be either frozen or chilled and
reheated in a variety of ovens, quite rapidly, so that they can be served, if
necessary, shortly after take-off.
6.16.2 The following types of aircraft oven are to be used:
Mobile heat retaining ovens that will keep food hot to a maxi- mum temperature
of 85 ºC (185 °F). They should not be used to heat frozen or chilled meals, since
this process may take up to 3 hours, and such slow heating can be a potential
risk.
Conventional fixed ovens that will reheat chilled food to 85 ºC (185 º F) in 45
minutes. Another 15 minutes must be allowed for heating frozen food to the
same temperature.
Fixed convection ovens that will reheat chilled food to 85 ºC (185 °F) in 18-20
minutes. Another 5 minutes must be allowed for frozen food.
Microwave ovens that will thaw frozen food in 35 seconds and heat to 85 ºC
(185 °F) in a further 35 seconds.
Cabin crew should keep a careful watch for insects, especially cockroaches, and
examine each tray, including the underside, as it is taken from the container. The
presence of insects should be reported to the airline's medical service. If flying
insects are seen on board, cabin crew should spray with an approved insecticide
aerosol.
Each galley should have a small supply of detergent/germicide avail- able for use if
any odd item of equipment has to be washed in flight. Normally this will not be
necessary, as a sufficient supply of clean crockery, glasses and cutlery should be
provided to make re-use unnecessary. All galleys should have a sufficient number of
waste bins provided in which to deposit wastes produced during a flight. At each
airport from which food is uplifted, all used equipment, surplus meals and waste
should be offloaded and replaced with a complete set of clean equipment and fresh
meals.
19 Nov 2015
Page 6-18
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
6.16.3 Crew meals
Cabin crew are normally supplied with special meals, or receive an allowance to buy
food on arrival. When flight deck personnel eat during the flight, it is absolutely
essential that the captain should be given a completely different meal from that
served to the co-pilot, prepared from food obtained from different sources.
The same principle must apply if they eat in ground catering premises a few hours
before take off. This is an essential safety precaution to reduce the possibility of
their both eating food contaminated by a pathogen that causes a disease with a short
incubation period to which they might succumb during the next flight.
6.16.4 Passenger illness
In addition to the usual epidemiological precautions, if any passenger or crew member
becomes ill during the flight or on arrival at an airport, and it is alleged or suspected
that aircraft food might be the cause, the airline concerned should be notified
immediately and supplied with detailed information.
To assist cabin crew to obtain the correct information, a questionnaire should be
supplied with the aircraft documents. This should be completed by the chief
steward or purser. It is important that unconsumed portions of the suspected meal,
together with three of each of the other meals-or, if no spare meals are available,
then three partly eaten meals-should be returned under refrigeration to the airline
hygiene officer. If no such officer exists, these samples should be sent to the most
appropriate person at the airline's base station, as quickly as possible, together with
the completed questionnaire. SIf a passenger is found to have an infectious
disease or is suspected of being infected, the health authority should be notified
immediately.
6.16.5 Food wastes
After offloading from the aircraft, waste food, including left-over unserved whole
meals, which will be on trays and in meal containers, or in modules on wide-bodied
aircraft, should be brought back to flight catering without delay. Offloading should
commence as soon as possible after the aircraft lands, so that the galley can be
cleaned before fresh equipment and food is loaded. All used equipment and waste
food should be brought to an unload- ing bay, which should be separate from the
loading bay from which the clean equipment and aircraft meals are dispatched. This
is necessary to prevent any cross-contamination between waste and fresh food.
The waste food must not remain in flight catering. Disposal by whatever method
should be rapid, safe and hygienically executed. All meal trays should be removed
from the containers for stripping. Before re-use, the containers must be thoroughly
washed, which is most efficiently done in a container washing machine. This should
incorporate a wash tank operating at 60ºC (140 ºF) with added detergent, and a rinse
tank operating with clean water only at a temperature of 82ºC (180 °F). All reusable equipment and utensils should be separated and passed to the dish-washing
section for either manual or mechanical cleaning.
19 Nov 2015
Page 6-19
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
The stripping of meal trays can be done entirely by hand, all waste matter being
placed in metal or plastic containers of various kinds. As soon as these are full they
should be emptied into a larger container for removal and final disposal, in the same
way as other airport waste, which deals with solid wastes disposal.
If the small waste containers are not disposable, adequate washing facilities are
required, and the containers must be cleaned before being returned to flight catering.
Manual stripping can be assisted by a conveyor-belt system on to which the contents
of the meal trays are emptied, and as they travel along the belt, all re-usable items
of equipment such as cutlery, crockery and glassware are removed. This leaves the
waste, which can be removed in containers or by mechanical waste disposal units
that grind it into segments for discharge into sewers.
The stripping belt should be so designed and constructed that it can be effectively
cleaned without dismantling, otherwise it will quickly become a breeding ground for
bacteria. Regular maintenance is necessary to prevent breakdowns. If these occur,
alternative means of disposal must be readily available.
Garbage grinders also require regular maintenance. Metal objects, such as cutlery,
must not be allowed to enter the unit, since they damage the grinding blades, which
will quickly put the mechanism out of action. This can be prevented if operators
are vigilant and screens are provided.
If waste food is stored while awaiting collection, it should be compacted
mechanically in the bulk container so that its volume is reduced considerably. This
system is usually operated by contractors who supply the compacting unit and bulk
containers. The containers should be housed in a separate room, which-especially
in warm climates should be air conditioned. Provision must be made for washing
the walls and floor of tqe garbage room.
If waste chutes are used, they must be constructed in a smooth, non- absorbent
material, such as stainless steel, and their design must ensure that the waste passing
through meets no obstruction. Provision should be made for washing the chute at
least once daily.
Another method of disposal is the automatic reduction of all waste to a pulp by a
wet process system.
Waste is introduced into a steel tank housing a rotating
impeller plate studded with grinding teeth and filled with water. It is reduced to
pulp, suspended in water as slurry.
This is pumped through pipes to a water press. In the water press most of the
moisture is removed, converting the slurry to a moist pulp amounting to about
20% of its original volume. The water is recycled in a closed system.
The pulp is odourless and ready for removal and disposal by conventional methods. The
advantages of this system, as claimed by the manufacturers, are that it eliminates air
pollution and im- proves sanitation, and that the pulp is unattractive to insects,
rodents, and other vermin. Waste handling is reduced, and the installations are easy
to clean.
19 Nov 2015
Page 6-20
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
6.16.6 The principles of the system are illustrated below:
All waste food offloaded from aircraft must be destroyed by one of the approved
methods. A ll food scraps and unserved meals are taken from the unloading bay
direct to an incinerator within the airport perimeter or within easy access of the
airport. Other kinds of rubbish produced in food premises-boxes, cartons, bottles,
cans, jars, etc. should be stored in covered containers while awaiting collection, which
must be done at least once daily. No off loaded food wastes should be allowed
to be used for animal feed. This prohibition does not, however, apply to fresh food
waste produced during the preparation of meals. It should be kept separate from other
rubbish and stored in a special swill area, which should be sited well away from
food supplies and food utensils.
The waste should be stored in covered bins and collected at least once daily.
The b i n s should be clearly marked and kept for this use only. The swill storage
area should be kept clean and facilities for washing the area should be provided.
After being emptied, the bins should be washed and disinfected, preferably by heat.
A more satisfactory arrangement is to engage the services of a swill contractor to
take away the bins and replace them with clean ones
6.17 Inspection of flight catering centre
All food premises should be inspected regularly and frequently by health authority
officers and by airline hygiene officers (As per Appendix 7&8). The former shall
have enforcement authority. Where the health authority ·can devote more time to
airport food preparation premises, knowing that the airline officer will be monitoring
flight catering. The health authority and airline hygiene officers should work in
close liaison. The frequency of inspection will depend on the operating standards
found i.e. it will be increased when conditions are unsatisfactory and decreased
when they are good. Detailed inspections, in which note is made of all structural
defects and faulty methods of food preparation and handling techniques, should be
carried out on average at monthly intervals, with revisits as necessary to see that
recommendations have been implemented. In addition, frequent adhoc visits should
be made just to check handling practices. Any faults seen can often be rectified
immediately and a few minutes' conversation with food handlers in their working
environment.
(Ref: WHO (Geneva) guide to hygiene and sanitation in aviation Chapter 4 by James
BAILEY, 2nd edition 1977,)
6.18 Solid waste disposals
Garbage and other dry waste matter emanate from many sources at an airport,
including terminal restaurants, warehouses, offices, and work- shops, as well as from
the aircraft themselves.
The storage, transport, and final disposal of solid wastes
must be carried out with care to pre vent nuisance, health hazards and indirectly
danger to aircraft..
19 Nov 2015
Page 6-21
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
6.18.1 Storage
6.18.1.1 On the ground
An adequate number of covered receptacles constructed in metal or some other
nonabsorbent material should be sited at strategic points in the airport-i.e., in
convenient locations for all buildings in which refuse is produced. The size of the
receptacles may vary from the conventional 0.l m3 (3.5-ft3) dustbin, where the
quantity of refuse is small, to purpose-built containers of a much larger capacity. Some
of these containers should be placed in convenient positions to receive the dry waste
taken from aircraft during transit. It is essential that the containers should be covered
at all times to prevent the scattering of litter and dust by the wind, the breeding of
flies and the attraction of rodents, scavenging dogs, and birds. For this reason
refuse awaiting disposal should never be stored in an open compound.
Where it is absolutely impossible to obtain covered containers, any compound that has
to be used for the retention of solid wastes must be roofed and screened. The floor
of such a compound must be of concrete and kept in good repair. Facilities for
washing down the floor should be provided. The floor should slope towards a
trapped drain gully connected to the foul-drainage system of the airport.
6.18.1.2 On the aircraft
Dry waste accumulating on aircraft should be stored in containers made of lightweight impervious material-e.g., polyethylene. Polyvinyl chloride should not be
used, owing to the toxic fumes produced when it is burnt. Some of these containers
will be purpose-made and fit into galley units as an integral part.
The waste containers should be emptied at each transit stop and washed with a
detergent/disinfectant
solution before being re- turned.
The recommended
practice is for each airport to stock a spare set of interchangeable galley waste
containers, washed and disinfected, which can immediately replace the full ones
offloaded. After being emptied, these soiled containers should be taken to a unit
for washing either by hand or by machine.
The use of disposable polyethylene liners will help to prevent undue soilage of
waste containers, but must never be a substitute for washing, as the liners get torn
and spillage results. Ideally, containers should be disposable, waterproof and resistant
to tearing. Waste containers may either be washed with hot water and detergent
solution supplied at high pressure from a mobile machine, cleaned by steam, also
under pressure, or passed through a container washing machine.
6.18.1.3 Collection and transportation
In transporting dry wastes from aircraft or airport buildings to the covered storage
containers, care must be taken to avoid spillage and other nuisances. The wastes
should therefore be transported in covered vehicles or containers.
19 Nov 2015
Page 6-22
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
The same principle applies when waste is taken from the storage area for final
disposal. Special purpose-built vehicles with dustless loading facilities should always
be employed, and open vehicles strictly prohibited. Strong winds are prevalent at
some airports and the scattering of litter during collection and transport causes not
only a nuisance but, in some circumstances, a health risk and a safety hazard.
6.18.1.4 Waste disposal
The disposal of wastes calls for careful planning.
WHO Scientific Group, which stated:
This has been emphasized by a
"The disposal of wastes must take place within a closed environment comprising
only earth, air, and water. When the liquid, solid, or gaseous residues from waste
treatment are disposed of, they must be discharged into one or more of these phases
of the environment. Any or all of the phases may be polluted, and any solution to the
general problem of the disposal of wastes therefore involves a decision as to which
part of the environment can accept residues with least damage to the whole. In other
words, in deciding on a site for the disposal of residues, their total effect on the
environment must be studied. Wastes must no longer be transferred from one
environmental phase to another without adequate study.
This is particularly
important in view of the fact that some residues persist permanently. In connection
with the disposal of waste from airports, apart from the possible spread of disease by
flies and rodents, which are attracted to disposal areas, there is the additional risk to
aircraft from bird strikes during take-off.
Birds are attracted by organic wastes, and it is vital that the disposal site should be
carefully planned well away from runways and flight paths, in order to prevent a
bird hazard problem. The land around airports is increasingly being used as a site for
garbage dumps and sanitary landfills because of the readily available property at a
relatively low cost. The United States Federal Aviation Administration has recently
issued guidelines aimed at banning the location of garbage dumps or sanitary
landfills within 3000 m (10 000 ft) of airport runways used by turbo-jet aircraft and
within 1500 m (5000 feet) of those used by piston- engine aircraft.
The action is intended to minimize the hazards to airport flight operations posed by
large numbers of birds attracted to the dumps or landfills. Birds striking aircraft can
damage critical control surfaces, and if they are drawn into turbine engines a loss of
power results. Damage can also be caused by large items of litter being sucked into
aircraft engines. In deciding on the location of the disposal site, the direction of
the prevailing wind should therefore be taken into account.
The site must be well away from food preparation premises to prevent
the
migration of flies and rodents, which breed on organic wastes. In selecting a
site it must be remembered that flies can travel up to distances of approximately 10
km (6 miles) or maybe even further when assisted by the wind. However, regardless
of distance from the airport, disposal must be efficiently controlled to prevent
nuisance and health hazards. If waste matter is indiscriminately deposited on the
ground or in bodies of water, breeding places for rodents and insects will be created.
19 Nov 2015
Page 6-23
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
Uncontrolled or incomplete combustion of solid wastes will release undesirable
pollutants into the atmosphere. It may also produce large volumes of smoke, which
if close to a runway could be distracting to pilots.
Inefficient incineration may give rise not only to smoke but also to dust or grit
emission.
Acceptable disposal methods include:
Incineration in a mechanical plant designed, equipped and operated to prevent air
pollution.
Pulverization controlled as above.
Controlled tipping or, as it is also described, sanitary landfill.
The residue from methods 1and 2 may also be finally disposed of by controlled
tipping. This procedure basically consists in depositing the waste on low-lying
land from which the topsoil has been removed. The waste is placed in layers
not exceeding 2 m (6ft 6 in) in depth, compacted, and then at the end of each day
covered with the previously removed topsoil to a depth of not less than 15 cm (6 in).
The area must also be provided with screens to arrest litter scattered by the wind.
The sanitary landfill system of disposal reduces insect and rodent breeding but
does not eliminate it entirely, especially in tropical regions, where the high
temperature and humidity increase the rate of decomposition and accelerate
breeding, It is therefore vital that effective vector and rodent control measures at
airports should be extended to waste disposal sites.
6.18.1.5 Special wastes
At airports the need frequently arises to dispose of toxic, noxious or polluting wastes,
which may be either solid, semi-solid or liquid. The disposal of these hazardous
wastes must be strictly controlled. At no time should they be disposed of
indiscriminately. Airports should make special arrangements, in conjunction with
the health authority, for the collection and disposal of any material considered
hazardous. There may also be occasions when condemned food requires disposal.
This again should be done under the direction and supervision of the health
authority.
19 Nov 2015
Page 6-24
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
Distribution of responsibilities and suggested areas of concern, by authority
or agency:
a. Distribution of responsibilities
Authority or agency
Health administration
Health authority
Airport authority
Responsibility
Ensuring the provision of an efficient system at
airports for the storage, removal and safe
disposal of refuse, condemned food and other
matter dangerous to health ( Article 14.1of IHR)
Ensuring the provision of facilities for vector and
rodent control at waste disposal installations
Carrying out regular and frequent hygiene
inspections of airports and installations.
Providing for the storage, removal and safe
disposal of solid wastes (Article 14.3 of IHR)
b. Suggested areas of concern
Airlines
Airport authority
Aircraft manufacturers
Removal of waste from the aircraft and transport
to waste storage
Ensuring the provision of an adequate number of
litter containers, ashtrays, etc. throughout the
airport and the frequent removal of the contents.
Designing suitable and acceptable waste disposal
receptacles for aircraft
(Ref: WHO guide to hygiene and sanitation in aviation, Chapter 7, 2nd edition, 1977)
19 Nov 2015
Page 6-25
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
THIS PAGE INTENTIONALLY LEFT BLANK
19 Nov 2015
Page 6-26
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
CHAPTER 7
MEDICAL SUPPLIES IN THE AIRCRAFT
7.1
Introduction
All Bangladeshi registered aircrafts shall be equipped with accessible and adequate
medical supplies as follows while on operation:
7.2
First-aid kits and Universal precaution kits
7.2.1
First Aid Kits.
7.2.1.1 No person may operate the following aircraft unless it is equipped with an accessible,
approved first-aid kit(s):
7.2.1.2 Aero planes with a maximum certificated take-off weight of over 5700 kg;
7.2.1.3 All AOC holders.
7.2.2 The number of first-aid kits to be carried shall comply as following:
7.2.2.1 Each aircraft shall carry first aid kits in accordance with at least the following
schedule:
Number of passenger seats
0-100
101-200
201-300
301-400
401-500
More than 500
Number of first aid kits
1
2
3
4
5
6
7.2.2.2 The location of first aid kits should be distributed evenly throughout the aircraft
7.2.2.3 Readily accessible to cabin crew members, if cabin crew members are required
for flight, and
7.2.2.4 Located near the aircraft exits should their use be required outside the aircraft in
an emergency situation.
7.2.2.5 The contents of first aid kits to be carried shall comply with serial no 7.5.1 below.
7.2.3
Universal Precaution Kit.
7.2.3.1 No person shall operate an aircraft that requires a cabin crew member unless it is
equipped with at least one universal precaution kit.
7.2.3.2 The contents of universal precaution kits to be carried in the aircraft shall comply with
serial no 7.5.2 below.
19 Nov 2015
Page 7-1
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
7.2.3.3 Each aircraft shall carry universal precaution kits in accordance with the following:
Two kits; and
Additional kits, as determined by the Authority, at times of increased public
health risk, such as during an outbreak of a serious communicable disease having
pandemic potential.
Emergency medical kit – aeroplanes
7.3
7.3.1
No person may operate a passenger flight in an aeroplane with 30 seats or more unless
the aeroplane is equipped with an approved emergency medical kit for treatment of
injuries or medical emergencies that might occur during flight time or in minor accidents.
7.3.2
7.3.3
The contents of emergency medical kits to be carried shall comply with serial no 7.6
below.
The medical kit shall be stored in a secure location.
7.3.4
Oxygen storage and dispensing apparatus
7.4.1
All aircraft intended to be operated at altitudes requiring the use of supplemental oxygen
shall be equipped with adequate oxygen storage and dispensing apparatus.
The oxygen apparatus, the minimum rate of oxygen flow, and the supply of oxygen shall
meet applicable airworthiness standards for type certification in the transport category as
specified by the Authority.
No person may operate an aircraft at altitudes above 10,000 feet unless it is equipped
with oxygen masks, located so as to be within the immediate reach of flight crew
members while at their assigned duty station.
No person may operate a pressurized aeroplane at altitudes above 25,000 feet unless:
Flight crew members oxygen masks are available at the flight duty station and are of a
quick donning type;
Sufficient spare outlets and masks and/or sufficient portable oxygen units with masks are
distributed evenly throughout the cabin to ensure immediate availability of oxygen to
each cabin crew member regardless of his location at the time of cabin pressurization
failure.
7.4.2
7.4.3
7.4.4
7.4.5
An oxygen dispensing unit connected to oxygen supply terminals is installed so as to be
immediately available to each occupant, wherever seated. The total number of dispensing
units and outlets shall exceed the number of seats by at least 10%. The extra units are to
be evenly distributed throughout the cabin.
7.4.6
The amount of supplemental oxygen for sustenance required for a particular operation
shall be determined on the basis of flight altitudes and flight duration, consistent with the
operating procedures established for each operation in the Operations Manual and with
the routes to be flown, and with the emergency procedures specified in the Operations
Manual. See Implementing to determine the amount of supplemental oxygen needed for
non pressurized and pressurized aircraft.
19 Nov 2015
Page 7-2
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
7.5
Contents of First- aid kits and Universal precaution kits
7.5.1
The first-aid kits shall include at least the following contents:
(1)
Antiseptic swabs (10/pack)
(2)
Bandage: adhesive strips
(3)
Bandage: gauze 7.5 cm × 4.5 m
(4)
Bandage: triangular; safety pins
(5)
Dressing: burn 10 cm × 10 cm
(6)
Dressing: compress, sterile 7.5 cm × 12 cm
(7)
Dressing: gauze, sterile 10.4 cm × 10.4 cm
(8)
Tape: adhesive 2.5 cm (roll)
(9)
Steri-strips (or equivalent adhesive strip)
(10)
Hand cleanser or cleansing towelettes
(11)
Pad with shield, or tape, for eye
(12)
Scissors: 10 cm [as allowed by national regulations]
(13)
Tape: Adhesive, surgical 1.2 cm × 4.6 m
(14)
Tweezers: splinter
(15)
Disposable gloves (multiple pairs)
(16)
Thermometers (non-mercury)
(17)
Mouth-to-mouth resuscitation mask with one-way valve
(18)
First-aid manual, current edition
(19)
Incident record form
(20)
Mild to moderate analgesic [as allowed by national regulations]
(21)
Antiemetic [as allowed by national regulations]
(22)
Nasal decongestant [as allowed by national regulations]
(23)
Antacid [as allowed by national regulations]
(24)
Antihistamine [as allowed by national regulations]
19 Nov 2015
Page 7-3
Civil Aviation Authority, Bangladesh
7.5.2
Aviation Public Health Manual
The required universal precaution kits shall include at least the following contents:
(1)
Dry powder that can convert small liquid spill into a sterile granulated gel
(2)
Germicidal disinfectant for surface cleaning
(3)
Skin wipes
(4)
Face/eye mask (separate or combined)
(5)
Gloves (disposable)
(6)
Protective apron
(7)
Large absorbent towel
(8)
Pick-up scoop with scraper
(9)
Bio-hazard disposal waste bag
(10)
Instructions.
Note: The carriage of automated external defibrillator (AED) should be determined by
operators or the Authority on the basis of a risk assessment taking into account the
particular needs of the operation.
7.6
Contents of Emergency Medical kit – aeroplanes
7.6.1
The required medical kit shall include the following equipment:
(1)
Stethoscope
(2)
Sphygmomanometer (electronic preferred)
(3)
Airways, Oropharyngeal (three sizes)
(4)
Syringes (appropriate range of sizes )
(5)
Needles (appropriate range of sizes)
(6)
Intravenous catheters (appropriate range of sizes)
(7)
Antiseptic wipes
(8)
Gloves (disposable)
(9)
Needle disposal box
(10)
Urinary catheter
(11)
System for delivering intravenous fluids
19 Nov 2015
Page 7-4
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
(12)
Venous Tourniquet
(13)
Sponge gauze
(14)
Tape adhesive
(15)
Surgical mask
(16)
Emergency tracheal catheter (or large gauge intravenous cannula)
(17)
Umbilical cord clamp
(18)
Thermometers (non-mercury)
(19)
Basic life support cards
(20)
Bag-valve mask
(21)
Flashlight and batteries
Note: If a cardiac monitor is available (with or without an AED) add to the above list.
7.6.2
The required medical kit shall include the following medication:
(1)
Epinephrine 1:1 000
(2)
Antihistamine – injectable
(3)
Dextrose 50% (or equivalent) – injectable: 50 ml
(4)
Nitroglycerin tablets, or spray
(5)
Major analgesic
(6)
Sedative anticonvulsant – injectable
(7)
Antiemetic – injectable
(8)
Bronchial dilator – inhaler
(9)
Atropine – injectable
(10)
Adrenocortical steroid – injectable
(11)
Diuretic – injectable
(12)
Medication for postpartum bleeding
(13)
Sodium chloride 0.9% (minimum 250 ml)
(14)
Acetyl salicylic acid (aspirin) for oral use
(15)
Oral beta blocker
19 Nov 2015
Page 7-5
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
Note 1:
Epinephrine 1:10 000 (can be a dilution of epinephrine 1:1 000)
Note 2:
The United Nations Conference for the Adoption of a Single Convention
on Narcotic Drugs in March 1961 adopted such a Convention, article 32 of
which contains special provisions concerning the carriage of drugs in
medical kits of aircraft engaged in international flight.
(Ref: ICAO Annex 6, Chapter 6.2 & Attachment B)
19 Nov 2015
Page 7-6
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
CHAPTER 8
MEDICAL SUPPORT DURING AIRCRAFT ACCIDENT
8.1
Actions by medical services during aircraft accident on the airport
It shall be the responsibility of designated medical coordinator to supervise the medical
services and to:
8.2
8.1.1
Verify the notification of mutual aid medical and ambulance services and
their subsequent arrival at the rendezvous point or staging area;
8.1.2
Organize the necessary actions for triage, treatment of the casualties, and
their eventual evacuation by appropriate means of transportation;
8.1.3
Control the flow of casualties and ensure, together with the transportation
officer, the dispatch of the casualties to the designated hospitals by all available
means of transportation.
8.1.4
Maintain an accurate list of the casualties including their names and their final
disposition;
8.1.5
co-ordinate the transportation of the uninjured to the designated holding
area with the aircraft operator concerned;
8.1.6
Provide medical evaluation of ambulatory and uninjured survivors;
8.1.7
Arrange for the replenishment of medical supplies, if necessary, and
8.1.8
Organize with the police, reception facilities for the dead.
Actions by designated hospitals
Each designated hospital is to appoint a coordinator responsible for the following:
8.2.1
Immediately provide and transport doctors and medical teams skilled in trauma
care to the accident site upon notification of the emergency;
8.2.2
Provide medical care to the casualties when they arrive at the treatment area; and
8.2.3
Ensure that adequate doctors and nurses, operating rooms, intensive care units,
surgical teams, blood and blood volume expanders are available for emergency
situations, including aircraft accidents.
(Ref: Doc 9137 Part 7, Chapter 4.1.6 & 4.1.7)
19 Nov 2015
Page 8-1
Civil Aviation Authority, Bangladesh
8.3
8.4
Aviation Public Health Manual
Actions by medical services during aircraft accident off the airport
8.3.1
Fire Service and Civil defense and Medical authorities normally will be
responsible for organizing the medical response. However, the medical
response from the on-airport medical service should also be applicable to
mass casualty accidents occurring off the airport.
8.3.2
According to the mutual aid emergency agreement with the surrounding
hospitals, the airport authority shall provide its medical equipment, supplies
(i.e. first aid equipment, stretchers, body bags, mobile shelters, etc.) and
assistance of first-aid personnel at the accident site.
Actions by designated hospitals
8.4.1
The designated hospitals are to ensure that adequate doctors, nurses, and
operating room, intensive care, and surgical teams are available for
emergency situations of aircraft accidents.
8.4.2
Provide medical care to the injured when they arrive.
(Ref: Doc 9137 Part 7, Chapter 4.2.7 & 4.2.8)
8.5
Provisions of medical services during airport emergency:
8.5.1
The purpose of medical services is to provide triage, first aid and medical care in
order to:
save as many lives as possible by locating and stabilizing the most seriously
injured, whose lives may be in danger without immediate treatment;
provide comfort to the less seriously injured and to administer first aid
transport casualties to the proper medical care facility.
8.5.2
It is essential that provision of medical services such as triage, stabilization, first
aid, medical care, and the transporting of the injured to hospital(s) be carried out
in the most expeditious manner possible. To this end, well organized medical
resources (personnel, equipment and medical supplies) should be available at the
accident site in the shortest possible time. The medical aspects of the
emergency plan should be integrated with local hospitals as agreed upon in
the Memorandum of understanding (MOU).
8.5.3
The medical coordinator of the airport crisis management team should assume
control of the emergency medical operations at the accident site. In some cases,
it may be necessary to appoint an interim medical coordinator, to be relieved
when the designated medical coordinator arrives on site. The interim medical
coordinator can be designated from the airport rescue and fire fighting personnel.
8.5.4
Medical and ambulance services may be an integral part of the airport services,
particularly whenever an ambulance service is a part of the airport rescue and
fire fighting service.
19 Nov 2015
Page 8-2
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
Whenever medical and ambulance services are not available at the airport,
prearrangements with local, private, public or military medical and ambulance
services should be made. The plan has to ensure the dispatch of a satisfactory
assignment of personnel, equipment and medical supplies. To ensure a rapid
response, the plan can include arrangements for land, sea and airborne
transportation of medical services to the scene, and subsequent transportation of
persons requiring immediate medical care. Prearrangements are necessary for the
availability of doctors and other medical personnel for all airport emergencies.
The plan should list a sufficient number of doctors to offset any absences at the
time an emergency occurs.
The responsibilities of designated medical transportation officer would include:
8.5.5
alerting hospitals and medical personnel of the emergency;
directing transportation of casualties to appropriate hospitals suitable for
treatment of the particular injury;
accounting for casualties by recording the route of transportation, destination
hospital, and casualty's name and extent of injuries.
advising hospitals when casualties are en route; and
maintaining contact with hospitals, medical transportation, the senior medical
officer of the hospital, on-scene commander and the command post.
8.6
Hospitals
8.6.1
Participating hospitals should have contingency emergency plans to provide for
mobilization if necessary of medical teams to the accident site in the shortest possible
time. Availability of qualified personnel and adequate facilities at the hospitals to deal
with airport emergency situations is vital. In this respect, it is mandatory to establish in
advance an accurate list of surrounding hospitals. They should be classified according to
their effective receiving capacity and specialized features, such as neurosurgical ability
or burn treatment. In most circumstances it is unwise to deplete the most proximate
hospital to the accident site of essential medical and nursing personnel.
8.6.2
The distance from the airport and the ability to receive helicopters should be
considered. Reliable two-way communication shall be provided between the hospitals,
ambulances and helicopters. The alert of an aircraft accident should be made to a single
medical facility which then alerts all other facilities according to a local medical
communications network.
(Ref: Doc 9137 Part 7, Chapter 3.6 & 3.7)
19 Nov 2015
Page 8-3
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
THIS PAGE INTENTIONALLY LEFT BLANK
19 Nov 2015
Page 8-4
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
CHAPTER 9
TRIAGE AND MEDICAL CARE
9.1
Immediate need for care of injured in aircraft accidents
In the aftermath of an aircraft accident, many lives may be lost and many injuries
aggravated if immediate medical attention is not provided by trained rescue personnel.
Survivors should be triaged, given available emergency medical aid as required, and
then promptly evacuated to appropriate medical facilities.
9.2
Triage principles (all emergencies)
9.2.1
Triage is the sorting and classification of casualties to determine the order of priority for
treatment and transportation.
9.2.2
Casualties should be classified into four categories as follows :
9.2.3
Priority I:
Immediate care
Priority II:
Delayed care
Priority III:
Minor care
Priority IV:
Deceased
The first qualified, medically trained First aid crew and RFF persons who arrive at the
site must immediately begin initial triage. This person(s) will continue performing
triage until relieved by a more qualified person or the designated airport triage officer.
Victims should be moved from the tr iage area to the appropriate care holding areas
before definitive treatment is rendered. Casualties should be stabilized at the care holding
areas and then transported to the hospital for further management.
9.2.4 Effort should be made to ensure that Priority I casualties are treated first and receive
ambulance transportation priority when stabilized. This is the responsibility of the triage
officer.
9.2.5 Triage is most efficiently accomplished in place. However, the conditions at an accident
scene may demand the immediate movement of casualties before triage can be safely
accomplished. In that case, the casualties should be moved the shortest distance
possible, well away from fire fighting operations, and upwind and uphill from the
scene.
9.2.6
Triage of casualties should include the use of casualty identification tags to aid in the
sorting of the injured and their transportation to a designated hospital.
19 Nov 2015
Page 9-1
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
9.3
Standardized casualty identification tags and their use
9.3.1
Need for standardized tags - Casualty identification tags should be standardized
through colour coding and symbols to make the tag as simple as possible.Tags help to
expedite the treatment of mass casualties in a triage situation and thus permit more rapid
evacuation of the injured to medical facilities.
9.3.2
Tag design - Standardized tags should be designed to require only minimal information
to be entered thereon, be usable under adverse weather conditions, and be water resistant.
In this tag, numerals and symbols indicate the medical priority classification of casualties
as follows:
Priority I
or immediate care:
RED tag;
Roman numeral I; rabbit symbol
Priority II
or delayed care:
YELLOW tag;
Roman numeral II; turtle symbol
Priority III
Priority IV
9.3.3
or minor care:
GREEN tag;
Roman numeral III;
Ambulance with X symbol
or deceased:
BLACK tag
Where tags are unavailable, casualties may be classified by using Roman numerals on
adhesive tape or by placing marks directly on the forehead or on other exposed skin
areas to indicate priority and/or treatment needs. Where marking pens are unavailable,
lipstick can be used.
19 Nov 2015
Page 9-2
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
Figure 9.1 Casualty identification tag
19 Nov 2015
Page 9-3
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
Figure 9.2 Casualty identification tag
19 Nov 2015
Page 9-4
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
9.4
Care principles
9.4.1
Stabilization of the seriously injured should be accomplished at the accident
site. The i m m e d i a t e transportation of the seriously injured before stabilization should
be avoided.
9.4.2
In accidents occurring on or adjacent to the airport, rescue and fire fighting personnel
are generally the first emergency personnel on the scene. These personnel must be aware
that it is imperative that seriously injured casualties be located and stabilized as quickly
as possible. In cases where fire control or prevention does not require the efforts of all
rescue and fire fighting personnel, available persons should immediately commence
casualty stabilization under the direction of the most qualified trauma-trained individual
on the scene. First response rescue vehicles should carry initial supplies of casualty-care
equipment, including artificial airways, compresses, bandages, oxygen and other related
equipment used for the stabilization of smoke inhalation casualties and severe trauma.
Sufficient oxygen should be available for use on rescue and fire fighting personnel.
However, oxygen should not be used in areas where fuel spills or fuel soaked clothing is
present due to the explosion hazard.
9.4.3
Actions taken during the first few minutes of medical treatment should stabilize the
casualties until more qualified medical care is available. When specialized trauma teams
arrive, more sophisticated medical care (i.e. cardiopulmonary resuscitation, etc.) will be
provided.
9.4.4
The triage procedure and subsequent medical care should be placed under the command
of one authority, the designated medical coordinator, upon this officer's arrival. Prior to
this, the command of triage should be assumed by the individual designated by the
commanding rescue and fire fighting chief and should continue until relieved by the
predesignated medical coordinator.
9.4.5
The medical coordinator has responsibility for all medical aspects of the incident and
should report directly to the on-scene commander. The medical coordinator's primary
function will be administrative, not as a participant of the medical team treating the
injured.
9.4.6
As a means to easily identify and distinguish the medical coordinator, a white hard hat
and highly visible white coat or vest should be worn, with “MEDICAL COORDINATOR” displayed front and back in reflecting red letter
9.4.7
Care of Priority I (Immediate care) casualties This type of casualty includes:
(1)
(2)
(3)
(4)
(5)
(6)
(7)
major haemorrhages;
severe smoke inhalation;
asphyxiating thoracic and cervico maxillofacial injuries;
cranial traumata with coma and rapidly progressive shock;
compound fractures;
extensive burns (more than 30 per cent);
crush injuries;
19 Nov 2015
Page 9-5
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
(8) any type of shock and
(9) spinal cord injuries
The following actions are recommended:
(1) first aid (clearing of the wind pipe, stopping of haemorrhages by means of
haemostatic pads, and positioning the casualty in the recovery position;
(2) resuscitation;
(3) oxygen administration, except in areas of fuel or fuel soaked clothing and
(4) placing the injured under shelter pending transportation.
9.4.8
Care of Priority II (Delayed care) casualties. This type of casualty includes:
(1) non-asphyxiating thoracic trauma;
(2) closed fractures of the extremities;
(3) limited burns (less than 30 per cent);
(4) cranial trauma without coma or shock; and
(5) injuries to soft parts.
Note: Care of casualties sustaining injuries which do not need immediate emergency
medical treatment to sustain life can be delayed until Priority I casualties have been
stabilized. Transportation of Priority II casualties will be performed following minimum
on-site care.
9.4.9
Care of Priority III (Minor care) casualties:
(1)This type of casualty includes minor injuries only. Certain accidents/incidents will
occur where passengers have either minor or no injuries, or appear not to be injured.
Because these casualties can interfere with other priorities and operations, it is important
that they be transported from the accident/incident site to the designated holding area
where they should be re-examined.
(2)It is important that provisions be made for the care, comfort, and identification of
Priority III casualties. This should be provided through airport operations, the aircraft
operator (where involved), or international relief organization (Red Cross, etc.). All such
minor injured casualties will be taken for treatment to holding area designated by
airport authority.
(9)The holding area is well equipped with cooling systems, electric light, water,
telephones and toilet facilities. This telephone may be used to contact the Emergency
Operation Centre and will be under the control of appropriate CAAB staff. Site of crash
and other information and instructions may be related via this telephone. All aircraft
operator personnel and airport tenants should know the location of such designated
facilities.
9.5
Control of flow of the injured
9.5.1 The injured should pass through four areas which should be carefully located and
easily identified.
Collection area — location where initial collection of the seriously injured from the
debris is accomplished. Need for the establishment of this area will be dependent upon
the type of accident and the circumstances surrounding the accident site. The casualties
a r e transferred from the rescue and fire fighting personnel to medical services
personnel at this point. In most cases, however, this transfer will occur at the triage area.
19 Nov 2015
Page 9-6
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
Care area — This area will be set at the scene of the crash. This area should be
subdivided into three subareas according to the three categories of injured, i.e.
Immediate care (Priority I), Delayed care (Priority II) and Minor care (Priority III).
Care areas can be colour coded for identification purposes (Red — Immediate,
Yellow — Delayed, and Green — Minor). The use of coloured traffic cones, flags, etc.,
may be used. From here Priority III casualties are to be transferred to designated holding
area for treatment.
Triage area — The triage area should be located at least 90 m upwind of the accident
site to avoid possible exposure to fire and smoke
Transportation area — A transportation area should be located between the care area (
site of accident) and the egress road. Here the first aid crew in cooperation with other
medical staff will do identification, registration and labeling injured passengers, who are
entered into a register. The Medical Officer will also control the flow of ambulance and
ensure that the ambulance drivers are given the correct destination. For HSIA all
personnel from a crashed aircraft are to be sent to the Dhaka Medical College Hospital
for final checkup and insurance formalities.
9.5.2
Mobile facilities for the stabilization and treatment of Priorities I and II casualties.
Airport health department should have such facilities which consist of:
Conventional or resuscitation ambulances. A resuscitation ambulance is an ideal shelter
for Priority I casualty. The casualty may be treated there and subsequently conveyed
directly to a hospital;
Red tents a r e d e s i g n a t e d to accommodate serious or extremely urgent cases. These
facilities, with provisions for integrated A/C and lighting, can be transported to the
scene together with all the necessary medical equipment mentioned under Airport
Medical Services.
Yellow tents are used to accommodate Priority II casualties. Transportable mobile
hospitals or ambulances can be used for stabilization treatment for all casualties.
(Ref: ICAO Annex 14, Doc 9137, Part 7 Chapter 9)
19 Nov 2015
Page 9-7
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
THIS PAGE INTENTIONALLY LEFT BLANK
19 Nov 2015
Page 9-8
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
CHAPTER 10
CARE OF AMBULATORY SURVIVORS
10.1
Responsibilities of airports/airlines /Other agencies:
10.1.1 Activate already selected holding area for the particular emergency o c c u r r i n g o n
the airport.
10.1.2 Arrange transportation from the accident site to the designated holding area of airport.
10.1.3 To have doctors and nurses at the holding area
10.1.4 Furnish a full passenger / crew manifest for accountability purposes;
10.1.5 Interview the uninjured and record their names, addresses, phone numbers, and where
they can be reached for the next 72 hours;
10.1.6 Notify relatives or next of kin, if necessary;
10.1.7 Prevent interference by unauthorized persons.
10.2
10.3
10.4
Airport authority will arrange buses, Microbuses for immediate transportation of the
“walking injured”/ambulatory passengers from the accident site to the designated holding
area. This plan should be implemented automatically following notification of the
emergency. A nurse or first aid crew should accompany these people to the holding area.
Each and every passenger and crew member should be examined for nervous traumatism
(shock) and smoke inhalation. Cold or inclement weather may require additional
provisions for their protection and comfort.
Where the aircraft accident occurred in water or a marshy area, these people may be wet
and uncomfortable. These problems should be anticipated by having supplies of clothing,
footwear, and blankets readily available. It may be necessary to establish a special
holding area which can supply warmth and clothing to prevent hypothermia, and be
used for examination purposes, before these persons are transported to the designated
ambulatory holding area.
International relief agencies and military establishments may be requested for many of
the aforementioned requisites.
(Ref: Doc 9137 Part 7, Chapter 10)
19 Nov 2015
Page 10-1
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
CHAPTER 11
CARE OF FATALITIES
11.1
Evidence must be preserved when caring for the fatalities at an aircraft accident
site. It is important to realize that an undisturbed site will produce the most reliable
evidence for determining cause and/or future corrective action that may help prevent a
similar accident.
11.2
Whenever possible, the wreckage should remain undisturbed until the arrival of the
appropriate accident investigation authority.
11.3
If bodies have to be removed identify the locations where they were.
11.4
The tag number to be noted on the signage left on site so that it will be possible to know
what body was at any location on the accident site.
11.5
Bags to gather passengers personal effects should be available.
11.6
Areas immediately surrounding the location of the fatality should be completely
secured. Areas in which a large number of fatalities or dismembered bodies are located
should be left undisturbed until the arrival of the forensic doctor and the aircraft accident
investigator or a designee.
11.7
An adequate supply of disposable plastic gloves and leather gloves should be
available for stretcher bearers removing the remains of the fatalities. All gloves should
be burned following use in gathering body parts.
11.8
If it becomes necessary to move bodies or parts of the wreckage, photographs should be
taken showing the relative position of bodies and parts within the wreckage and a sketch
of their respective positions should be made prior to removal.. Special precautions should
be taken to avoid disturbing anything in the cockpit area.
11.9
The fatalities should be extricated and personal effects removed from the wreckage prior
to the arrival of the forensic doctor or appropriate authority only to prevent their
destruction by fire or for other similar compelling reasons.
11.10 Body bags are normally available from major local suppliers of caskets and
funeral organization, equipment and supply firms, and from nearby military facilities.
Stocks of body bags at each airport are desirable.
11.11 Body identification and determination of cause of death is conducted with the
concurrence of the authority designated for this duty. This operation is generally
conducted with the cooperation of forensic teams and other specialists.
11.12 Accidents which result in a large number of fatalities will overload normal morgue
facilities. So it should be preplanned to cope up with large number of fatalities. It should
be sited in an area where relatives or the general public have access.
19 Nov 2015
Page 11-1
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
11.13 After identification has been made of the fatality, efforts to contact next of kin should
commence. Agencies such as aircraft operators, public service organizations (i.e.
international relief agencies and police), or clergy should be utilized.
11.14 The accident investigation team generally has the authority and the need to require
autopsies and toxicological analyses of flight crew members, and in special cases,
passengers. The need for these tests should be determined prior to the release of bodies.
11.15 As soon as possible all participants in the fire fighting and rescue effort should be
debriefed. Their observations a r e t o be recorded. Sketches, diagrams, photographs,
movie films, and tape and video recordings made on the accident site as well as
appropriate details on the tagging of bodies and body parts removed from their positions
are invaluable tools for investigators.
11.16 The Forensic officer in charge shall wear a dark brown hard hat and vest or other apparels
as approved by authority with “FORENSIC CHIEF”
displayed front and back in
distinctive lettering.
(Ref: Doc 9137 Part 7, Chapter 11)
19 Nov 2015
Page 11-2
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
CHAPTER 12
AIRPORT MEDICAL SERVICES
12.1
General
12.1.1 Adequate medical services and supplies are to be made available at the airport health
department. The medical coordinator ( Airport Health Officer ) is responsible for the
provision and checking of medical supplies.
12.1.2 Medical authority is to provide sufficient medical supplies to deal with routine medical
emergencies which normally occur at the airport (on-the-job injuries, heart attacks, etc.)
plus possible aircraft accidents.
12.1.3 Emergency medical training: All personnel assigned to rescue duties especially the
personnel of airport health department, listed personnel from airport
employees and First aid crew of Civil Aviation Authority, Bangladesh
should be given first aid and CPR (cardiopulmonary resuscitation) training.
12.1.4 Rescue and fire fighting personnel should have the ability to stabilize seriously injured
casualties. At least two full-time members per shift of the airport rescue and fire
fighting service or other on-airport personnel should be trained to an emergency
medical treatment level. It is recommended that as many rescue and fire fighting
personnel as is practicable receive training to meet minimum standards of medical
proficiency and preferably to the level of personnel highly qualified in first aid or the
equivalent. Accordingly, they should have sufficient medical equipment at their
immediate disposal to initiate stabilization until full medical services are available at the
site or until transportation of casualties to adequate medical facilities is provided.
12.1.5 Airport rescue and fire fighting personnel should be trained in CPR (cardio- pulmonary
resuscitation) by the appropriate medical authority. Periodic exercises and drills in CPR
techniques are mandatory to maintain proficiency.
12.1.6 Airports may enlist volunteers from airport employees other than rescue and fire
fighting personnel to provide an immediate response to assist casualties resulting from
emergencies. Volunteers should be trained by accredited agencies in first aid and rescue
response duties. In case of an emergency, they should initially be under the supervision
of the first commander at the scene, i.e. the station fire officer, until the arrival of
the medical coordinator.
12.1.7 Emergency medical supplies and equipment: The airport health authorities should
arrange to have sufficient medical supplies, available on or in the vicinity of the
airport, to treat the passenger and crew.
12.1.8 The airport should have available stretchers, blankets, backboards and/or immobilizing
mattresses, preferably stored on a suitable vehicle which can be transported to the
accident site. Blankets are needed to alleviate casualties' exposure to shock and possible
adverse weather conditions. Since trauma victims in an aircraft accident sometimes
sustain severe spinal injuries, backboards and cervical collars should be used
19 Nov 2015
Page 12-1
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
when removing such casualties from the aircraft in order to minimize the possibility of
further spinal injury. The backboards should be of a type designed to fit through access
ways and aisles of commercial and business aircraft. They should have restraining straps
available so that the patient can be secured to the board.
12.1.9 Sufficient emergency oxygen and respiratory equipment should be available to treat
smoke inhalation victims.
12.1.10 Since the majority of non-accident related medical emergencies at airports involve
coronary difficulties, advanced life support systems should be readily available.
12.1.11 Mobile emergency hospitals or inflatable tents can be used for on-site treatment of
immediate care (Priority I — Red) and delayed care (Priority II — Yellow) casualties.
These units should be readily available for rapid response. The casualties can be treated
at the scene, stabilized and be available for transportation to the appropriate hospital.
12.1.12 A resuscitation type ambulance can be used as an ideal shelter for an immediate
c a r e (Priority I — Red) casualty.
12.1.13 To cope up with an emergency involving a large aircraft, it is recommended that the
general emergency medical supplies and equipment described in the following list be
available at the airport. If operations for smaller aircraft are planned for the specified
medical supplies and equipment should be adjusted to comply with reasonable
requirements.
12.1.14 List of General emergency supplies and equipment
500
100
Quantity
10
50
50
20
2-3
2-3
2-3
10
300-500
19 Nov 2015
Description
Triage labels
Stretchers, adaptable to the most commonly used
ambulances
Immobilizing mattresses for backbone fractures
Splints, either conventional or inflatable, for the various
types of fractures
First-aid kits, each containing a set of 10 tags,
haemostatic pads, tourniquets , scissors, dressings, sterile
burn packs
Arrangement of oxygen for about 20 casualties.
Electrocardiographic apparatuses
Suction devices
Analgesic Injection
Intravenous infusion packs with giving sets
Plastic bags or coffins for the deceased
Remarks
Page 12-2
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
12.1.15Emergency medical transportation facilities: The dispatch of casualties to
hospitals from the accident site should take into consideration the hospital(s) medical
personnel on staff, medical specialties and beds readily available. Ambulance available
with Airport Health Department shall be utilized as on-call ambulance for routine
medical emergencies. Written agreements with off-airport based ambulances should be
prepared to provide for emergency transportation services.
12.1.16 Airborne transportation equipment: Helicopters and fixed wing aircraft, should be
considered for emergency evacuation or for transport of medical services and equipment
from hospitals to the accident site.
12.1.17 Since it may be necessary to transport many casualties to appropriate off airport medical
facilities, ambulances arriving at the scene should report to the rendezvous point ( In case
of HSIA, area between cargo complex and hanger gate) and then to the designated
transportation officer. This officer will be responsible for ascertaining the number of
casualties who will need transportation to the designated medical facilities.
12.2 Airport medical care facilities / first-aid room
There are many general factors which influence the need for an airport first-aid room
or an airport medical facility.
Generally, it may be recommended that an airport medical care facility be available
when the airport employee’s number 1000 or more and that a first-aid room be available
at every airport. The airport medical care or first-aid room personnel and facilities
should be integrated with the airport emergency plan.
Location of airport medical care facilities: The facilities should be readily accessible to
the airport terminal building, to the general public and to emergency transportation
equipment (i.e. ambulances, helicopters, etc.). Site selection should avoid the problem of
having to move injured persons through congested areas of the airport terminal building,
while providing access to the facility by emergency vehicles by a route that as far as is
feasible can bypass normal public access roadways to and from the airport. This suggests
that the medical care facility be located so that access can be gained from the air side of
the airport terminal building .It is justifiable to be located near the egress road for easy
transportation of sick person.
12.2.1 1t is recommended that during the principal hours of airport activity at least one
person trained to deal with the following be on duty:
cardiopulmonary resuscitation (CPR);
bleeding from a traumatic source;
Heimlich maneuver (choking);
fractures and splinting;
burns;
shock;
emergency childbirth and immediate care of newborn, including premature;
19 Nov 2015
Page 12-3
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
common medical conditions which may influence the outcome of injury
(allergies, high blood pressure, diabetes, pace-maker, etc.);
basic measures for treatment and protection subsequent to spills or leaks of
radioactive materials, toxic, or poisonous substances;
treatment of emotionally disturbed persons;
recognition and first aid for poisons, bites, and anaphylactic shock; and
transportation techniques for injured persons.
12.2.2 The airport medical care facility should be adequately equipped to handle cardiac
arrest and other types of injuries and illnesses.
12.2.3 Sufficient emergency oxygen and respiratory equipment should be available to treat
smoke inhalation victims.
12.2.4 Since the majority of non-accident related medical emergencies at airports involve
coronary problems, advance life support systems including oxygen, oxygen regulators,
and other elements for cardiopulmonary care should be readily available. In addition,
first-aid kits (containing drugs, a wide selection of bandages and splints, blood
transfusion equipment, and burn and maternity kits), should be available.
12.3 Airport without a medical care Facility
12.3.1 At airports without a medical care facility / first aid room, the airport authority should
make arrangements to have available sufficient personnel trained in advanced first aid to
cover all active hours of airport operation. Equipment for first aid work at these airports
should consist at least an emergency medical care bag. This bag should be readily
available to be carried on a designated airport emergency vehicle and should contain at
least:
one plastic sheet (1.80 m × 1.80 m);
seven hemostats (one package of three, one package of four);
two field dressings (one 45 cm × 56 cm, one 56 cm × 91 cm);
ten abdominal pads (five packages of two);
forty 10 cm × 10 cm gauze pads (four packages of ten);
two tourniquets;
one artificial airway;
three disposable airways (one each No. 2, No. 4, No. 5);
one bulb syringe with two catheters (No. 12, No. 14 FR);
two large bandage scissors (medical scissor);
twenty disposable syringes with No. 25 GA 1.6 cm needle;
twelve alcohol sponge packages;
four rolls of gauze bandage (two 7.5 cm, two 5 cm);
two rolls of adhesive tape;
four Vaseline gauze dressings (15 cm × 91 cm);
box of 100 band-aids;
19 Nov 2015
Page 12-4
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
one blood pressure cuff and gauge;
two clipboards (22 cm × 28 cm);
six pencils;
sufficient supply of casualty identification tags;
one set of inflatable splints;
one resuscitate tube
one short spine board;
one flashlight;
two cervical collars;
one disposable obstetric kit; and
one immobilizing mattress.
(Ref: Doc 9137 Part 7)
19 Nov 2015
Page 12-5
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
THIS PAGE INTENTIONALLY LEFT BLANK
19 Nov 2015
Page 12-6
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
APPENDIX 1
AIRCRAFT GENERAL DECLARATION
(Inward/Outward)
Owner or Operator……………………………………..…
Nationality and Registration………………………………
Departure from…………………………………………....
(Place and Country)
Flight No……… Date………..
Arrival at………………………
(Place and Country)
FLIGHT ROUTING
(Place column always to list origin, every en-route stop and destination )
Place
Total Number of Crews
Ref: Regulations 12(1),(2) and 109(1) (2) (3) (4)
Number of Passengers
Cargo
Departure Place:
Embarking……………..
Transit on same
flight………………….
Arrival Place:
Disembarking…………
Transit on same flight…
Declaration of health
Name and seat number or function of persons on board with illnesses other than airsickness or the effects
of accidents who may be suffering from a communicable disease ( a fever- temperature 38ºc/ 100°F or
greater- associated with one or more of the following signs or symptoms, e.g. appearinf obviously unwell,
persistent coughing, impaired breathing, persistent diarrhoea,persistent vomitting, skin rash, bruising,or
bleeding without previous injury or confusion of recent onset, increases the likelihood that the person is
suffering a communicable disease as well as such cases of illness disemberked during a previous stop…..
Details of each disinsecting or sanitary treatment (place, date, time, method) during the flight. If no
disinsecting has been carried out during the flight, give details of most recent
disinsecting………………………………………………………………………………………..
……………………………….
Sign. Crew member concerned
I declare that all statements and particulars contained in this General Declaration, and in any
supplementary forms required to be presented with this General Declaration are complete, exact and true
to the best of my knowledge and that all through passengers will continue/have continued in this flight.
_____________________
Signature
Authorised Agent or Pilot –in- Command
Ref: ICAO Annex 9 (Appendix 1)
19 Nov 2015
Page App 1-1
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
APPENDIX 2
CERTIFICATE OF RESIDUAL DISINFECTION
GOVERNMENT OF…………………………………………………………………………..
CERTIFICATE OF RESIDUAL DISINFECTION
Interior surfaces, including cargo space, of this aircraft………….were treated with an approved
residual disinfection product on (date)………………………in accordance with the world health
organization recommendations ( WHO weekly Epidemiological Record No 7, 1985.p. 47; No 12
1985, p. 90; No 45, 1985, pp. 345-346; and No 44,1987, pp. 335-336) and any amendments
thereto.
The treatment must be renewed if cleaning or other operations remove a significant amount of
the residual disinfection product and in any case within 8 weeks of the above date.
Expiry date………………………………………………………………………………………
Signed…………………………………………………………………………………………….
Designation………………………………………………………………………………………
Date………………………………………………………………………………………………
19 Nov 2015
Page App 2-1
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
APPENDIX 3
PUBLIC HEALTH PASSENGER LOCATOR CARD
PUBLIC HEALTH PASSENGER LOCATOR CARD: To protect your health, public health officers
need you to complete this form whenever they suspect a communicable disease on board a flight. Your
information will help public health officers to contact you if you were exposed to a communicable
disease. It is important to fill out this form completely and accurately. Your information is intended to be
held in accordance with applicable laws and used only for public health purposes. – Thank you for
helping us to protect your health.
FLIGHT INFORMATION: 1. Airline name……………………….….. 2. Flight No ……….…………..
3. Seat No…………….…………..4. Date of arrival………...……………...
PERSONAL INFORMATION: 4. Name……………………………… Family name
………..…….
Given Name…………………………..…..Street Name and Number……..……………………………..…
City………………………..…..State/province………….…………......Country……..……………….…….
ZIP/Postal code………………………….….. .Your contact phone number………….… ………………..
Country code……………………….…Area code…………...………E-Mail……………………….……..
Passport or Travel document……………………………………………………………….……………….
Number…………………………………..….Issuing country/Organization…………………………..……
CONTACT INFORMATIONS:5. Address and Phone Number where you may be contacted during your
stay………………….Street Name and Number………………………………………………………..…
City………………….……..………... State/Province………………………………………………….…
Country………………..…ZIP/Postal code…………..Telephone Number…………..……….…………..
6. Contact information for the person who will best know where you are for the next 31 days, in case of
emergency or to provide critical health information to you. Please provide the name of close personal
contact or a work contact, This must not be you.
a. Name………..Family Name………..Given Name………… b. Telephone Number……….………..,
country code………........Area code………….... Phone
Number…….…………………………………….E-Mail address…… …………………………………
c. Address: Street Name and Number…..………… …..……City…………….…………………...
State/Province…………………………………………………………………………………..…….…....
Country…………………………………ZIP/Postal code………………………………..…………….….
7. Are you travelling with anyone else………………………..…..YES/NO……………………………,
if so who? (Name of individual or group)…………………………………………………………………
Ref: ICAO Annex 9 (Appendix 13)
19 Nov 2015
Page App 3-1
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
APPENDIX 3A
PUBLIC HEALTH PASSENGER LOCATOR CARD
(To be completed by all the passengers arriving from affected area/country or Suspect of the
same row, 2 rows front and 2 rows behind in the same aircraft)
Flight Information :
a. Airline and flight no
________________________________________________________
b. Date of arrival_______________c. Seat
no______________________________________
Personal information :
a. Name_________________________ d. Father’s
Name____________________________
b. Country (coming from)___________ e. Phone
no________________________________
c. Passport No ____________________ f. E-mail (if
any)___________________________
Contact Information :
a. Address (of Stay in
Bangladesh)______________________________________________
_____________________________________________________________________
___
_______________________
Signature of the Cabin Crew
Ref: CAAB Approved on 18 Aug 2014
19 Nov 2015
Page App 3A-1
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
APPENDIX 4
MODEL INTERNATIONAL CERTIFICATE OF VACCINATION OR PROPHYLAXIS
This is to certify that (name)…………………….date of birth…………………sex……...……
Nationality…………………………, National identification document, if applicable…..……..
Whose signature follows…………………………………………………………………………
has on the date indicated been vaccinated or received prophylaxis against:
(name of disease or condition)……………………………………………………in accordance
with the International Health Regulations.
Vaccine or
Date Signature and
Manufacturer
Certificate
Official stamp
prophylaxis
professional status
and batch No
valid
of
of supervising
of vaccine or
from………… administering
clinician
prophylaxis
Until………… centre.
1.
2.
(Ref: International Health Regulations (2005), Annex 6)
19 Nov 2015
Page App 4-1
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
THIS PAGE INTENTIONALLY LEFT BLANK
19 Nov 2015
Page App 4-2
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
Appendix 5
INSPECTION CHECKLIST FOR EVALUATING THE SANITATION STATUS AND
IMPLEMENTATION OF INTERNATIONAL HEALTH REGULATIONS (IHR) TO AIRPORTS
Ref:
A.
B.
C.
D.
International Health Regulations (IHR-2005), Annex-1.B
ICAO Annex 9 chapter 8. E
ICAO Annex 14 Doc 9137
WHO guide to hygiene and sanitation in Aviation, 3rd edition, 2009)
Name of the Airport :
Inspection date:
Name of the Inspector:
Regulatory Authority :
Sl
DETAILS
NO
Required Core Capacities at Point of Entry (PoE) - at all times
1
2
3
4
5
6
7
8
9
Yes
No
NA
Remarks
Does designated airport provide appropriate medical services
including diagnostic facilities for prompt assessment
\and care of ill travelers?
Does it provide adequate staff, equipment and premise
for care of the affected passengers?
Does it provide access to equipment and personnel for the
transport of ill travelers to the designated hospital / medical
facilities?
Does it provide trained personnel for inspection of Aircraft?
Does it ensure a safe environment for travelers using PoE
facilities including ?
1. potable water supplies
2. Eating establishments
3. Flight catering facilities
4. Public wash rooms
5. Appropriate solid and liquid waste disposal services
6. Other potential risks areas by conducting inspection
programme.
Does it provide a programme and trained personnel for the
control of vectors and reservoirs in and around the PoE?
Has the State established a public health emergency
contingency plan and nominated a Focal Point for point
of entry, public health and other agencies?
Does it provide assessment and care for affected travelers or
animals by medical and veterinary facilities (for their isolation
and treatment)?
Does it provide appropriate space, separate from other travelers,
to interview suspect or affected persons?
19 Nov 2015
Page App 5-1
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
10
Does it provide for quarantine of suspect travelers, in facilities
away from the point of entry?
11
Are there measures for derating, disinsecting, disinfecting &
decontaminating baggage, cargo, containers, conveyances,
goods or postal parcel?
12
Does it apply entry or exit controls for arriving and departing
travelers?
13
Does it provide access of designated equipment and trained
personnel with appropriate personal protection for the transfer
of infected travelers?
Facilities at airport fire station
14
Are the resuscitation Ambulance facilities available to face
airport emergency?
15
Is casualty care equipment including compresses, bandages,
oxygen etc available for management of smoke inhalation
casualties and trauma patients?
16
Are the fire fighters trained on first aid treatment?
Is the airport health department have following facilities?
(1)
Canopies and their covers
(2)
Collapsible tables, bags with towels and blankets
(3)
Large ground sheets
(4)
Portable basins and stands
(5)
Stretchers having modifications for mini buses and buses
(6)
Trailer full of medical equipment (stretchers, boxes of medical
stores, cans for water etc)
17
Did the doctors of airport health department attend any medical
emergency during the reported period?
18
Was it timely and efficiently attended? What was the response
time to attend the emergency?
19
Does it have adequate equipment to handle cases of cardiac
arrest and other types of injuries and illnesses?
20
How many patients were attended by doctors during the
reported period and how they were handled?
21
Did any death of passenger/ airport employee occur during the
reported period and how it was handled?
22
Are there sufficient oxygen and cardio resuscitation (CPR)
facilities with trained personnel available?
19 Nov 2015
Yes
No
NA
Remarks
Page App 5-2
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
ICAO Annex -9 ( Facilitation )
23
Does the State (Airport health department) have
International Vaccination Certificates available for the
passengers?
24
Does the State have available adequate stocks of “public
health passengers locator card” for distribution to aircraft
operators, for completion by passengers and crew when
cases of suspected communicable diseases are on board
the aircraft?
Sanitary Condition of the Airport : As Per WHO guide to hygiene
and sanitation in aviation
Public Areas and Rooms
25
Is the hand washing sign displayed for good hand washing
practices by staff and guests?
26
Does the staff use disposable wipes for cleaning to avoid
cross contamination?
27
Does the staff use proper chemical sanitizing agent?
28
Are the handrails, handles, telephones, other hand contact
areas, elevators and landings in all passenger corridors
cleaned and sanitized frequently ?
29
Are all the public rooms cleaned/sanitized regularly?
30
Are the carpets cleaned by steam cleaner?
31
Are the garbage cans cleaned regularly?
32
Are the soft furnishings cleaned and sanitized?
Public Washrooms
33
Is hand washing sign displayed?
34
Are the door handles, toilet flushes, faucets (water taps),
dryers, counters and any other hand contact areas cleaned
and sanitized regularly?
35
Are the hand dryers or disposable paper towels provided
for hand drying?
Yes
36
Are disposable paper wipes provided for cleaning to avoid
cross contamination?
Bars and
Lounges
37
Is the hand washing sign displayed at each hand sink?
38
Does the staff wash hands frequently
39
Are hand sanitizers provided to staff for good hand
washing practices?
40
Are snacks provided in small individual containers?
41
Are condiments (salt and pepper) containers that served by
staff cleaned frequently (recommended to clean between
each customer use)?
19 Nov 2015
No
NA
Remarks
Page App 5-3
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
42
43
Are disposable paper wipes used for cleaning?
Are all tables and chairs cleaned and sanitized after each
shift and after closing?
GENERAL HYGIENE AND SANITATION OF THE AIRPORT
44
Is the exhaust supplied to the toilets area serviceable?
45
Is the drainage system all right?
46
Are the lighting facilities in the airport as well as
washroom sufficient?
47
Is the ceiling of toilets all right?
48
Are the mosquitoes and flies in the airport under control/?
49
Are the dryers serviceable?
50
Is adequate hand washing soap / liquid dispensers
available?
51
Are the waste bins cleaned?
52
Are the toilets for use by the disabled passengers
properly constructed?
53
Are adequate chemicals and equipment available for
cleaning the airport?
54
Are Proper storage facilities for cleaning itemsavailable?
55
Are sufficient toilet tissues available in the wash rooms?
56
Are automatic electric Faucets (water taps) with
electronic eyes provided in the washrooms?
FINDINGS:
RECOMMENDATIONS:
Date:_____________________________Inspector’s Signature:________________________
19 Nov 2015
Page App 5-4
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
APPENDIX 6
MEDICAL (CABIN) INSPECTION CHECK LIST
Ref:
A.
B.
ICAO Annex 6, Chapter 6, Attachment-B (Medical Supplies)
CAAB, ANO Part –E (Chapter E.1)
Place:
Operator:
Arriving from:
Departing to :
Aircraft type:
Pilot in Command:
Cabin Chief:
Inspector / s Name :
Date and Time:
Operator (Chartered/Commercial):
Flight No:
Flight No:
Aircraft Registration No :
First Officer:
Other Cabin Crew:
SL NO
A
1
DETAILS
FIRST AID KIT (FAK)
Are the First aid kit /s available?
2
Is the number of first aid kits proportionate to the
no of passengers? .
If there is one first aid kit, is its location as close
as practicable to an emergency exit?
Are the first aid kits constructed of non
flammable material and free of dust and moisture?
Is the red crescent sign displayed prominently and
permanently?
Are the words “first aid kit” displayed both in
Bengali and English on the kit container?
Are the first aid kits readily accessible to the
occupants of the aircraft?
In case of more than one kits, Are they placed in
dispersed locations?
Does the first aid kit contain a hand book written
both in English and Bengali?
3
4
5
6
7
8
9
10
11
12
13
Yes
No
NA
Remarks
Is there an inventory of contents affixed to the
inside of the lid?
Does the first aid kit container have positive seal?
Are the contents verified and certified by a
medical officer/authorized representative?
Are the locations of FAK appropriately and
conspicuously marked in Bengali and English
19 Nov 2015
Page App 6-1
Civil Aviation Authority, Bangladesh
14
B
15
16
17
18
19
20
21
22
23
24
25
C
26
27
28
29
Aviation Public Health Manual
Does the certificate affixed on the exterior of the
container, exhibit the following information?
a. Serial number
b. Date of certification
c. Expiry date and signature
d. Authorization of the person certifying
EMERGENCY MEDICAL KIT (EMK )
Does the aircraft have emergency medical kit?
Is it readily accessible to the crew member?
Is it provided with a positive seal?
Is it provided with a proper inventory of
contents?
Does it contain the basic instructions for the use
of drugs in the kit?
Is the red crescent mark displayed on the kit
container?
Are the words “Emergency Medical Kit”
displayed on the kit container both in English and
Bengali?
Is stowed securely in a clearly marked location?
Is it constructed of non-flammable material and
free from dust and moisture?
Are the contents and serviceability of the contents
verified and certified by a medical
officer/authorized representative?
Does the certificate affixed on the container have
the following information?
a. Serial number
b. Date of certification
c. Expiry date and signature
d. Authorization of the person certifying
UNIVERSAL PRECAUTION KIT(UPK)
Does the aircraft have universal precaution kit ?
Is the number of UPK on board adequate? .
Are the kits evenly distributed throughout the
passenger cabin?
Are the kits readily accessible to the cabin crew
members?
FINDINGS:
RECOMMENDATIONS:
Date : ___________________Inspector’s Signature: ______________________
19 Nov 2015
Page App 6-2
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
APPENDIX 7
INSPECTION OF AIRLINE SERVICE AREA OR TRANSFER POINT
Name of the Airlines:
Inspection date:
Name of the Inspector
Regulatory Authority:
Satisfactory =S Satisfactory with Comments= SC Unsatisfactory = U Not Checked =NC
Sl NO
DETAILS
S/SC/U/NC
REMARKS
WATER PIPING SYSTEM
1
No cross connections
2
No backflow connections
3
Adequate pressure
HYDRANTS
4
Location satisfactory
5
Good maintenance
6
Quick type coupling
7
Proper surface drainage
WATER HOSE
8
Satisfactory material, smooth, no cracks
9
Quick type coupling
10
Satisfactory nozzle guard
11
Hose properly protected and stored
12
Hose handled properly, flushed before use
13
Nozzle different size and shape from waste
connections
WATER TANKS OR TANKS CARTS
14
Separate from toilet waste tank
15
Complete drainage possible
16
Water tanks labeled
17
Proper transferral of water
18
Personnel who remove waste do not handle water or
food
19
Soil cans covered during transportation
20
Sewage removed without spillage
21
Construction and maintenance of toilet waste carts
22
Equipment available for flushing aircraft sewage
retention tanks ( not by direct connection to water
supply)
19 Nov 2015
Page App 7-1
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
DISPOSAL OF TOILET WASTE
23
Disposal facilities removed from food/ drink serving
areas
24
Sewage disposal satisfactory
25
Can or tank cleaning facilities completely fly proof
26
Room clean, good repair
27
Hot water or stream available
28
Soil cans emptied and cleaned after removal from
aircraft
29
Carts emptied and flushed frequently
30
Satisfactory storage of clean soil cans
HANDLING OF AIRCRAFT REFUSE
31
Refuse handled properly, no spillage
32
Storage containers satisfactory, covered
33
Storage containers emptied frequently
34
Receptacles cleaned
35
Receptacles stored properly, not with soil cans
36
Other refuse disposal satisfactory
37
Airsickness containers properly disposed of
SANITARY FACILITIES FOR EMPLOYEES
38
Adequate, convenient toilets, locker rooms and
washrooms
39
Clean, good repair
40
Hand washing facilities with soap, towels, adequate
water
41
Hand washing sign posted
42
Drinking water provided is safe, no common cups
FINDINGS:
RECOMMENDATIONS:
Date :___________________Inspector’s Signature:__________________
(Ref:
WHO guide to hygiene and sanitation in aviation 2009, Annex-D)
19 Nov 2015
Page App 7-2
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
APPENDIX 8
ON-SITE INSPECTION TO ASSESS THE CLEANING STATUS OF THE AIRCRAFT
Place:
Operator:
Arriving from:
Departing to :
Aircraft type:
Pilot in Command:
Cabin Chief:
Inspectors name:
Date and Time:
Operator(Chartered/Commercial):
Flight No:
Flight No:
Aircraft Registration No :
First Officer:
Other Cabin Crew:
Satisfactory = S
Unsatisfactory = U
Satisfactory with Comments= SC
Not Checked
= NC
Area
Flight deck
SERVICES
S/SC/U/NC Remarks
Empty waste boxes and ashtrays
Clean crew tables and glass holders
Clean stowage areas and racks
Wipe seats
Clean floor/Vacuum carpets
Clean flight deck windows inside
Clean door and walls
Dispose of waste from closets
Dispose of litters and newspapers
Dispose of waste in seat pockets
Collect and re-stow pillows and blankets
(first, business class)
Fold and re-stow blankets in overhead bins
Re-stow pillows in overhead bins
Empty ashtrays
Clean tray tables and armrests
Clean cabin crew seat tables
Clean interphone surfaces
Clean cabin windows inside
Vacuum passenger and cabin crew cloth
covered seats
Wipe passenger and cabin crew leather
covered seats
Dispose of waste in overhead bins
Clean overhead bins outside and latch
handle surfaces
Clean PVC floors
Vacuum carpet
Cabin
Sl No
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
14
15
16
17
19 Nov 2015
Page App 8-1
Civil Aviation Authority, Bangladesh
Cabin
18
19
20
21
22
23
24
25
Galleys
26
27
28
Lavatories
Crew
areas
29
30
31
32
33
34
35
36
37
38
39
40
41
rest 42
43
44
45
46
47
48
49
50
51
19 Nov 2015
Aviation Public Health Manual
Empty and clean ashtrays
Vacuum ashtray holders
Collect and replace blankets
Collect and replace pillows
Collect and replace headrest covers
Clean passenger seats
Remove passenger seat cushions and
vacuum
Remove stains from carpets
Clean seat rails, ceiling, sidewalls,
doors, magazine racks
Empty waste bins and insert waste bags
Clean doors, latches, ceiling and
ventilation grills
Clean sinks, faucets and working
surfaces
Clean retractable tables
Clean ovens inside and outside
Clean service trolleys
Clean PVC floors
Empty waste bins and insert waste bags
Clean toilet bowl and seat
Clean basin, faucets and surfaces
Clean mirror
Clean change table
Clean wall surfaces and interior and
exterior door handles and locks
Clean PVC floors
Replenish soap dispenser
Replenish toiletry items
Dispose of waste from closets
Dispose of litters and newspapers
Remove sheets, pillows and blankets
from each sleeping berth
Clean surfaces within each sleeping
berth
Place clean sheets on mattresses
Clean lights, ventilators and interphones
Empty ashtrays
Vacuum carpets
Clean cabin crew seat tables
Clean cabin windows inside
Page App 8-2
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
FINDINGS:
RECOMMENDATIONS:
Date:___________________Inspector’s Signature:___________________
(Ref:
WHO guide to hygiene and sanitation in aviation 2009, Annex F)
19 Nov 2015
Page App 8-3
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
THIS PAGE INTENTIONALLY LEFT BLANK
19 Nov 2015
Page App 8-4
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
APPENDIX 9
INSPECTION CHECKLIST OF FLIGHT CATERING SERVICE CENTRE
(Hygiene Officer’s Self-inspection Checklist)
Name of the flight Catering
service centre :
Inspection date:
Name of the Inspector
Regulatory Authority:
I
Personal Hygiene
Standard
Yes
Employees wear proper clothing
Food handlers wear hair restraints
Fingernails are short, unpolished and clean
Jewellery is limited only to watch and plain
ring
Gloves are changed at critical points
Open sores, cuts or bandages on hands are
completely covered while handling food
Adequate hand washing and drying facilities
are available
Wash hands routinely and thoroughly follow
proper hand washing procedures
No smoking in preparation, service, storage
and ware washing areas
Eat, drink, or chew gum only in designated
areas away from work areas
Disposable tissues are used and disposed of
after coughing/blowing nose
Employees take appropriate action when
coughing or sneezing
Personnel with infections restricted
Employee illnesses are documented
II.
No
N/A
No
N/A
Remarks
Utensils and Equipment
Standard
All small equipment and utensils, including
cutting boards and can openers, are
thoroughly cleaned between uses
Small equipment and utensils are air dried
19 Nov 2015
Yes
Remarks
Page App 9-1
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
Work surfaces are clean to sight and touch
Work surfaces are washed and sanitized
between uses
Thermometers are washed and sanitized
between each use
Drawers and racks are clean
Small equipment is inverted, covered, or
otherwise protected from dust or
contamination when stored
III.
Cleaning and Sanitizing
Standard
Yes
Three-compartment sink is properly set up
for Ware washing (wash, rinse and sanities)
Cleaning procedures are in place for utensils,
equipment and premises
Chlorine test kit or thermometer is used to
check sanitizing rinse
If heat sanitizing is used, utensils should be
immersed in boiling water
If using chemical sanitizer, proper dilution
should be ensured
Cleaning chemicals and equipment are
stored properly
The utensils are allowed to air dry
Adequate clean wiping cloths are provided
Cleaned tableware and utensils are properly
stored
IV.
No
N/A
Remarks
No
N/A
Remarks
Waste Disposal
Standard
Yes
Adequate waste disposal bins are provided
Waste disposal bins are washed and
Sanitized
Waste disposal bins are emptied as
Necessary
Cartons and waste are removed from food
preparation area
Waste storage area is insect- or
rodent-proved
Proper storage is available for brooms, mops
and other cleaning utensils outside food
preparation area
19 Nov 2015
Page App 9-2
Civil Aviation Authority, Bangladesh
V.
Aviation Public Health Manual
Pest Control
Standard
Yes
No
N/A
Remarks
Screens are put on open windows and doors
and properly maintained
A pest control program is in place
No evidence of pests is present
FINDINGS:
RECOMMENDATIONS:
Date:___________________Inspector’s Signature:___________________________
( Ref: Food Safety Plan, Risk communication Section, Food and Environmental Hygiene
Department 6/2002, Public Health Laboratory Centre, Shek Kip mei, Kowloon)
19 Nov 2015
Page App 9-3
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
THIS PAGE INTENTONALLY LEFT BLANK
23 Nov 2015
Page App 9-4
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
APPENDIX 10
INSPECTION CHECKLIST FOR FLIGHT CATERING FOOD PREPARATION,
STORAGR AND TRANSPORTATION:
Name of the flight catering
service centre:
Inspection date:
Name of the Inspector
Regulatory Authority:
Stage
Receiving
Dry
Storage
Control limits
Yes
Inspect incoming food and
supplies immediately upon
receipt
All foods and supplies are
promptly moved to proper
storage areas
No
N/A
Remarks
Receiving area is clean and free
of food debris, boxes or other
refuse
Chilled and frozen products are
arriving at correct temperature
Products are supplied by
approved suppliers
Storage area is dry and well
Ventilated
All foods are labeled with name
and (expiry / delivery) date
FIFO (First-in-first-out) is used
There are no bulging or leaking
canned goods in storage
Opened bulk-food supplies are
stored in containers with tightfitting lids
Food is protected from
Contamination
All surfaces and floors are clean
Chemicals
and
cleaning
supplies are stored away from
food and other food-related
supplies
19 Nov 2015
Page App 10-1
Civil Aviation Authority, Bangladesh
Food
Handling
Cold
Storage
Aviation Public Health Manual
Frozen foods are thawed under
refrigeration or in cold running
water
Food is kept under appropriate
temperature (i.e. cold foods at
4°C or below and hot foods at
63°C or above)
Food is tasted using proper
method
Food is prevented from
cross-contamination
Food is handled with clean
utensils or clean hands
Avoid touching parts of utensils
that directly contact food
Proper cooling procedures have
been practiced
Thermometers are conspicuous
and accurate
Proper
temperatures
are
maintained: 4°C or below for
chillers and –18°C or below for
freezers
All foods are stored off the
floor.
Food is arranged in a way to
allow air circulation
Cooked foods are stored above
or separately from raw foods
Proper chilling procedures have
been practiced
All foods are properly wrapped,
labeled and dated
FIFO (First-in-first-out) is used
Units are clean
Hot
Holding
Units are clean
Temperature of food being held
is 63°C or above
Food is heated to 75°C before
placing in hot holding
19 Nov 2015
Page App 10-2
Civil Aviation Authority, Bangladesh
Display
Transport
Aviation Public Health Manual
Display of ready-to-eat and non
ready-to-eat foods is separated
Different sets of utensils are
used to handle ready-to-eat and
non ready-to-eat foods
Hot foods are kept at 63°C or
Above
Cold foods (e.g. raw oysters,
sashimi and salad) are kept at
4°C or below
Transport containers and carts
are regularly cleaned and
sanitized
Proper
temperatures
are
maintained during transport: at
4°C or below for cold foods and
above 63°C for
hot foods
Transport carts and containers
for food are covered
Transport vehicles are clean
FINDINGS:
RECOMMENDATION:
Date:___________________Inspector’s Signature:______________________________
(Ref: Food Safety Plan, Risk communication Section, Food and Environmental Hygiene
Department 6/2002, Public Health Laboratory Centre, Shek Kip mei, Kowloon )
19 Nov 2015
Page App 10-3
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
THIS PAGE INTENTIONALLY LEFT BLANK
19 Nov 2015
Page App 10-4
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
APPENDIX 11
ICAO COOPERATIVE ARRANGEMENT FOR THE PREVENTION OF SPREAD OF
COMMUNICABLE DISEASE TROUGH AIR TRAVEL (CAPSCA)
STATE AND AIRPORT ASSISTANCE VISIT CHECKLIST
State
Airport/City
Dates
Civil Aviation Authority
National Coordinator
Airport Operator
Focal Point
Public Health Authority
Focal Point
CAPSCA Visit Team
Leader and Technical
Advisors
Areas
Reference
Yes
No
Remarks
A. ADMINISTRATIVE
1. Does an entity fulfil the
function of the “Competent
Authority” (as defined in the
WHO International Health
Regulations (2005) i.e. does an
entity have responsibility for
IHR Article 1, Definitions
implementation of, In particular,
IHR (2005) Articles: 24, 25, 27,
28, 30, 31, 32, 35, 36, 38, 40,
41, 43, 46 and Annex 1(B), 4, 5
and 9? Which entity?
2. Do the Civil Aviation
Regulations cover public health
emergency related provisions of National Documentation
ICAO Annexes and guidance
material?
-
Annex 6
19 Nov 2015
Page App 11-1
Civil Aviation Authority, Bangladesh
-
Annex 9
-
Annex 11
-
Annex 14
-
Annex 18
-
PANS ATM Doc 4444
3. Is a Contact point established
for policy formulation and
operational organization of
preparedness plan for aviation?
4. Does the Public Health
Authority have designated
personnel at the airport?
5. Has the State established a
national committee for Public
Health Emergency planning?
Aviation Public Health Manual
ICAO web-based Guidelines for
States, Section “General
Preparedness”
National Documentation
National documentation
IHR Annex 1, A, 3
6. Is this Committee involved in
airport/aerodrome Public Health ICAO Annex 14, 9.1.1-9.1.3
Emergency Planning?
7. Is the Civil Aviation Authority
ICAO Annex 14, 9.1.1-9.1.3
involved?
8. Is the Public Health Authority
ICAO Annex 14, 9.1.1-9.1.3
involved?
9. If so, under a formal
ICAO Annex 14, 9.1.1-9.1.3
contract/agreement?
10. Are aircraft operators
ICAO Annex 14, 9.1.1-9.1.3
involved?
11. Are the Rescue and Fire
ICAO Annex 14, 9.1.1-9.1.3
Fighting services involved?
12. Is the Air Navigation Services
ICAO Annex 14, 9.1.1-9.1.3
Provider involved?
13. Are the Immigration/Customs
ICAO Annex 14, 9.1.1-9.1.3
Services involved?
14. Are the security services
ICAO Annex 14, 9.1.1-9.1.3
involved?
15. Are private health services
ICAO Annex 14, 9.1.1-9.1.3
involved?
219Nov 2015
Page App 11-2
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
16. Are the service providers
involved? (Airlines, Ground
Handling Service (GHS), cargo, ICAO Annex 14, 9.1.1-9.1.3
etc.)
17. Are formal
contracts/agreements utilised
specifying the involvement of
stakeholders?
National documentation
B. DOCUMENTATION
1. Does the airport have in place
a Plan for Public Health
ICAO Annex 14, 9.1.1-9.1.3
Emergencies?
2. Is it part of the Aerodrome
Emergency Plan?
ICAO Annex 14, 9.1.1-9.1.3
3. Is it compatible with the
national Aviation Preparedness ICAO Annex 9, 8.16
Plan for Public Health
Emergencies?
4. Is it compatible with the
National Preparedness Plan for
Public Health Emergencies?
5. Has the Airport/Aerodrome
Emergency Plan (Public Health
Emergency component) been
tested by conducting full-scale
exercises and/or table-top
exercises? Specify what and
when
6.Preparedness planning
involves:
Template for a National Aviation
Public Health
Emergency Preparedness Plan
ICAO web-based Guidelines for
States….Section ”General
Preparedness”
ICAO Annex 9, 8.19
ICAO web-based Guidelines for
States….Section ”General
Preparedness”
National Documentation
a Public health?
b Regulatory aviation
authority?
c Airport operator?
19 Nov 2015
Page App 11-3
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
d Aircraft operator?
e Air traffic management?
f Other service providers?
Specify
__________________________
7. Are the stakeholders familiar
with Annex 6, in particular
Attachment B (Medical
ICAO Annex 6, Attachment B
Supplies)?
8. Are the stakeholders familiar
with Annex 9, Chap. 8,
Appendices 1 (General
ICAO Annex 9, Appendices 1, 13;
Declaration) and 13 (Public
WHO IHR (2005) Annex 9
Health Passenger Locator
Card)?
9. Specify (1) who collects the
General Declaration and
Passenger Location Cards and
(2) who processes the
information on arrival.
National documentation
10. Are the stakeholders familiar
with Annex 11, in particular
Attachment C (Material
ICAO Annex 11, Attachment C
Relating to Contingency
Planning)?
11. Are the stakeholders familiar
with Annex 14, Chapter 9
(Aerodrome operational
services, equipment and
ICAO Annex 14,
installations) in particular
Chapter 9
paragraph 9.1 (Aerodrome
Emergency Planning)?
12. Are the stakeholders familiar
with the WHO International
WHO IHR (2005)
Health Regulations (2005)?
19Nov 2015
Page App 11-4
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
13. Are the stakeholders familiar with
ICAO Procedures for Air Navigation
Services-Air Traffic Management, Doc.
4444, in particular paragraph 16.6:
“Notification of suspected communicable ICAO PANS-ATM, Doc 4444
diseases on board an aircraft, or other
public health risk”?
14. For travellers designated as suspect
cases and asymptomatic contacts are there
systems in place for?
- Handling of their baggage
ACI web-based Guidelines for airport operators,
Section 6
- Security Screening
- Customs clearance
- Immigration
15. Are stakeholders familiar with related
guidance material, available from:
ICAO
www.capsca.org
WHO
www.capsca.org
IATA
www.capsca.org
ACI
www.capsca.org
16. Is there a national Preparedness Plan
for a Public Health Emergency?
WHO IHR (2005) Article 13
17. Which stakeholders receive training
concerning the national Preparedness Plan
for a Public Health Emergency (airport
National documentation
personnel, public health authority, etc.)?
18. Is there a National Aviation
Preparedness Plan for a Public Health
Emergency of International Concern
(PHEIC)? Is this Plan part of a National
Public Health Emergency Plan?
19 Nov 2015
ICAO Annex 9, 8.16
Page App 11-5
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
19. Does the Preparedness Plan
include phases as defined by
WHO in “Pandemic Influenza
WHO Pandemic Influenza
Preparedness and Response
Preparedness & Response, 2009
2009”?
20. Does a mechanism exist for
deciding when to initiate the
pandemic contingency plan
- When to stop it?
- What kind of measures
need to be put in place
21. Are communication methods
in place to inform public on
travel risks/procedures?
22. Is there a National Business
Continuity Plan for Public
Health Emergencies?
23. Is the aviation sector
considered in whole of society
approach to pandemic
preparedness?
24. Is there an
Airport/Aerodrome Operator
Business Continuity Plan for
Public Health Emergencies?
Template for a National Aviation
Public Health
Emergency Preparedness Plan
www.capsca.org
ICAO web-based Guidelines for States,
Section “Communication”
National documentation
ICAO web-based Guidelines for
States….Section “General
Preparedness”
Airport/aerodrome operator
documentation
C. EMERGENCY OPERATION CENTRE (EOC)
1. Is there in place a flow chart
to initiate the aviation
emergency response plan
National documentation
process?
2. Command and control system
is established for management
of public health event ‘on the
day’?
19 Nov 2015
ICAO Annex 14 para. 9.17 – 18
ICAO web-based Guidelines for
States….Section “General
Preparedness”.
National documentation
Page App 11-6
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
3. Do Public Health Authority ICAO web-based Guidelines for
personnel participate in
States….Section “General
developing the aviation
Preparedness”
preparedness plan?
D. RESCUE AND FIRE FIGHTING (RFF) SERVICES
1. Do the RFF Services
participate in the development
and testing of the Aerodrome
Emergency Plan for Public
Health emergencies?
2. Are personnel familiar with
related guidance material,
available on www.capsca.org
ICAO web-based Guidelines for
States….Section ”General
Preparedness”
www.capsca.org
E. IMMIGRATION
1. Does the immigration
service participate in
development and testing of the
Aerodrome Emergency Plan
for public health emergencies?
2. Are personnel familiar with
related guidance material,
available on www.capsca.org
ICAO web-based Guidelines for
States….Section “General
Preparedness”
www.capsca.org
Airports Council International web3. Are there procedures for
based Guidelines for airport operators,
handling passengers suspected
Section 6
of being affected by a
communicable disease?
4. Are personnel trained about
ACI web-based Guidelines for airport
protective measures for
operators, Section 6
handling from suspected
passengers?
5. Are cargo and baggage
IATA web-based Guidelines for aircraft
handlers trained to use
operators, Section “Air Transport and
appropriate protective measures
Communicable; Diseases”
for handling luggage from
suspected passengers?
19 Nov 2015
Page App 11-7
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
H. AIR NAVIGATION SERVICE PROVIDER (ANSP)
1. Does the ANSP participate in
ICAO web-based Guidelines for States,
development and testing of the
Section “General Preparedness”
aerodrome Emergency Plan for
public health emergencies?
2. Are personnel familiar with
related guidance material,
www.capsca.org
available on www.capsca.org
3. Does the ANSP provide
training with the PANS-ATM
(Doc 4444, paragraph 16.6)
procedure for notifying the
PANS-ATM (Doc 4444)
destination airport of a potential
on-board public health
emergency?
4. Is a procedure in place for
transfer of information from the
ANSP to the public health
authority, notifying that
National documentation
anticipated arrival of an affected
aircraft?
5. Does the ANSP have a
contingency plan for managing
ICAO Annex 11, Attachment C
Public Health Emergencies?
6. Does the ANSP have a
Business Continuity Plan for
managing Public Health
Emergencies?
National documentation
I. MEDICAL SERVICES
1. Is the airport medical service
provided by the State or a
National documentation
private enterprise?
2. Has the service provider
received training in managing
public health emergencies?
19 Nov 2015
WHO IHR (2005) Annex 1 B
Page App 11-8
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
3. Has it established a
communication process with the National documentation
Public Health Authority?
4. Has ease of access to the
affected aircraft by medical
ACI web-based Guidelines for airport
service providers been
operators, Section 6
considered in designating an
aircraft parking position?
5. Are medical service providers
aware of (1) Notification
1 - ICAO PANS-ATM
procedure of a suspected case by
2 -ICAO Annex 9, Appendix 1; WHO
the pilot in command (2) Health
IHR (2005) Annex 9
part of the aircraft general
declaration?
6. Is there a procedure enabling
WHO technical advice for case
the public health authority to
management of Influenza A (H1N1) in
communicate with the affected
Air Transport
aircraft before landing?
7. Have Port Health Officers
ICAO Annex 9, Appendix 1; WHO
been made aware of cabin crew IHR (2005) Annex 9
identification procedures for
suspect cases (Health part of
Aircraft General Declaration)?
8. Does the medical service
provider participate in the
ICAO web-based Guidelines for States,
development and testing of the
Section “General Preparedness”
airport emergency plan for
public health emergencies?
9. Does the medical service use
and process (1) the General
National documentation
Declaration and/or (2) the Public
Health Passenger Locator Card?
10. Are suitable designated
areas / facilities provided for:
- Review of suspect cases IHR (2005) Annex 1B
by medical staff?
IHR (2005) Annex 1B
- Transport of cases to
medical facility
designated for purpose?
11. Does the medical service
provider have access to the
suspect or affected traveller’s
National documentation
assessment area?
19 Nov 2015
Page App 11-9
Civil Aviation Authority, Bangladesh
12. Is the use of personal
protective equipment (PPE)
considered?
Types of PPE
____________________
_____
13. Which personnel are
required to use PPE
____________________
______
- Training provided to
personnel
14. Procedure is in place for
obtaining a timely diagnosis of a
suspect traveller?
15. Does the medical service
have procedures for transfer of
suspect or affected travellers to
specialized evaluation units?
Aviation Public Health Manual
National documentation
National documentation
National documentation
WHO IHR (2005) Annex 1 B
16. Are facilities available to
enable rapid testing of biological
National documentation
specimens? What are they?
17. Does the medical service
have procedures for aircraft
disinfection?
18. What disinfectant product(s)
is used to disinfect an affected
aircraft?
19. What procedure is used?
How long does it normally take?
20. Is the service providr aware
of relevant aspects of the IHR
(2005)?
21. In the case of an affected
aircraft carrying a suspected
case of a communicable disease,
are efforts made to minimize the
delay to other travellers and the
return to service of the aircraft?
19 Nov 2015
WHO Guide to Hygiene and Sanitation
in Aviation
WHO Guide to Hygiene and Sanitation
in Aviation
WHO Guide to Hygiene and Sanitation
in Aviation
IHR (2005)
ACI web-based Guidelines for airport
operators, Section 6
Page App 11-10
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
22. Are procedures in place for
safe removal, transport and
disposal of liquid and solid
WHO Guide to Hygiene and Sanitation
waste generated from the on
in Aviation
board management of a case of a
potential communicable
disease?
J: SECURITY
1. Does the aviation security
(AVSEC) provider participate in
the development and testing of
the airport emergency plan for
public health emergencies?
2. Are there procedures in place
for managing aviation security
in the designated passenger
assessment area for suspect or
affected travellers?
3. Are personnel trained in the
use of protective measures for
managing suspect or affected
travellers?
ICAO web-based Guidelines for States,
Section “General Preparedness”
National documentation
ACI web-based Guidelines for airport
operators, Section 6
K. INFRASTRUCTURE
1. Are the international
passenger flows mixed, on
arrival and departure?
2. Is there a designated parking
position for an affected aircraft?
3. If so, where is the designated
position?
4. Are there provisions for
maintaining electricity, water
supply, waste disposal, etc. at
the aircraft after parking?
5. Does the airport have a
designated holding or waiting
area for suspect or affected
travellers?
19 Nov 2015
National documentation
ACI web-based Guidelines for airport
operators….Section 6
National documentation
National documentation
WHO IHR (2005) Annex 1 B
Page App 11-11
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
ICAO web-based Guidelines for States,
6. Requirements considered for
Section “Screening”
screening equipment
-
Maintenance
-
Calibration
-
Personnel Training
L. AIRCRAFT OPERATORS:
1. Do the aircraft operators
participate in the development
ICAO web-based Guidelines for States,
and testing of the aerodrome
Section “General Preparedness”
emergency plan for public
health emergencies?
2. Are aircraft operators aware
of (1) Notification procedure of 1 - ICAO PANS ATM
a suspected case by the pilot in 2 -ICAO Annex 9, Appendix 1, WHO
command (2) Health part of the IHR (2005) Annex 9
aircraft general declaration?
3. Are aircraft operators aware
of IATA guidelines for: cabin
IATA web-based Air Transport and
crew; maintenance crew; birdCommunicable Diseases Guidelines
strike; cleaning crew; passenger
agents?
4. Do the aircraft operators have
procedures enabling cabin crew IATA web-based Air Transport and
to identify travellers suspected Communicable Diseases Guidelines –
of having a communicable
Cabin Crew
disease
5. Do the aircraft operators have
IATA web-based Air Transport and
procedures for managing a
Communicable Diseases Guidelines –
suspected case of communicable
Cabin Crew
disease on board a flight?
6. Are Ground Personnel
familiar with World Health
WHO Pandemic Influenza
Organization (WHO) global
Preparedness & Response, 2009
influenza preparedness plan?
7. Number of trained personnel
assigned for these d23 Nov 2015
Page App 9-3
National documentation
uties, in relation to volume and
frequency of travellers:
8. Are arrangements for
translation and interpreters
WHO IHR (2005) Article 32
considered?
19 Nov 2015
Page App 11-12
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
9. Have personnel undergone a
training programme, to
National Documentation
recognize disease symptoms?
10. Are personnel familiar with
procedures regarding prompt
National documentation
assessment, care and reporting
of ill travellers?
M. MEDIA:
1. Is there a communications
strategy and plan?
CAPSCA Global Meeting Conclusion
ADDITIONAL REMARKS AND RECOMMENDATIONS
REMARKS
19 Nov 2015
RECOMMENDATIONS
COMMENTS
Page App 11-13
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
THIS PAGE INTENTIONALLY LEFT BLANK
19 Nov 2015
Page App 11-14
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
APPENDIX 12
STANDARD OPERATING PROCEDURE FOR HSIA WHEN INFECTIOUS
DISEASE THREAT IS REPORTED ON ARRIVING AIRCRAFT
Aircraft (Pilotin- Command )
Air Port Health Officer
(Lead CMT)
01716088748
8914870-4 Ext: 3466
Control Tower
(ATC, SATO)
CAAB
Exchange
Duty Medical Officer
(DMO)
8914249/8914247
(8901844, hot line
01799430033)
Fire Station of HSIA
(8914870-4/3233, 3205)
Duty Security Officer
(DSO)
8901453, 89148704/3053)
DAPO,((01819143003)
FWO, CAAB
Flight operation of
respective Airline
Director HSIA
(01913503810) 8901449,
8914870-4/ 3377
CAAB (Director ATS,
Director FSR,
Member OPS & Planning,
Chairman)
Immigration
Department
(01711706148)
8914226,
01713373072-3
19 Nov 2015
Customs
Department
8901748, 8901758-9
Biman Cabin
Appearance
section
Ground Handling
(GSE & Airport
Service)
Ground
Support
Equipment
(GSE)
Facilitation
and Welfare,
Page App 12-1
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
INFECTIOUS DISEASE THREAT
REPORTED TO DMO BY TOWER
ON
ARRIVING
AIRCRAFT
Duty Medical
Officer (DMO)
8914249/8914247
Director (CDC)
(01715566084)
(IHR FP)
pointPoint)
Director, IEDCR
(01711595139)
Director, HSIA
Health Emergency
Response Team
(HERT)
Referral Hospital
(01769010200)
Crisis
Management
Team (CMT)
Lead Air Port
Health Officer
017160887481
19 Nov 2015
Page App 12-2
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
In accordance to the International Health Regulations (IHR 2005) and the protocol for the
entry point Hazrat Shah Jalal International Airport (HSIA) in public health emergency caused
by biological agent, the following steps shall be taken:
1. Air Traffic Control (ATC) upon notification,
a. Obtain the following information from Pilot of the affected flight:
Aircraft Identification
Nature of emergency
Estimated time of arrival
Number of Passenger affected
Number of Crew affected
Country of travel origin and transit of the pax
Special treatment/Ambulance requirement
b. Alert Duty Medical Officer (DMO 8901844, hot line 01799430033), Airport Fire
Station (8914870-4/3233, 3205), Ground handling, SATO (off – 8901870-4/3412),
Duty Security Officer (DSO 8901453,8914870-4/3053), Director HSIA with the
information
c. Initiate information through CAAB exchange
Airport Health Officer (01716088748),
Director HSIA (01913503810),
Duty Airport Officer (DAPO 01819143003,8914870-4/3466)
Customs (8901748, 8901758-9) ,
Flight Operation of respective Airline,
OC Immigration {01711706148, 8914226(O.C) 01713373072-3}
Airport Fire Service (DFL)
Ground Handling (GSE & Airport Service)
CAAB (Director ATS, Director Flight Safety, Member OPS & Planning,
Chairman)
d. Activate Emergency Operation Centre (EOC) by SATO, if required
e. Intimate affected airline operator
f. Adjust air traffic to facilitate the priority landing
g. Coordinate aircraft parking to a separate bay (Bay 14/F3).
h. Facilitate any special requirement.
2. Director HSIA (after consultation with Director IEDCR and CDC, DGHS) will activate
the Crisis Management Team (CMT).
3. DMO of HSIA
Activates Health Emergency Response Team (HERT) after consultation
with AHO
Informs referral hospital to prepare
Contacts Director IEDCR and CDC, DGHS for their directives
Asks ambulances of airport and fire services and ambulance from other
sources to be prepared with PPE and present near the aircraft after landing.
19 Nov 2015
Page App 12-3
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
4. The HERT (comprising of two airport medical officers, two Nurse/SIs and two security
personnel provided by DSO; depending upon requirement the number of members may
vary) engages in mutual coordination and heads towards the special bay area of the
airport with an ambulance from the airport Fire service. The team arrives in 30 minutes
and prepare themselves with full personal protective equipments (PPE). The ambulance
driver and support staff also wears PPE.
5. Right upon arrival, the HERT coordinates with the Crisis Management Team (CMT),as
Annex C of Multihazard Public Health Emergency Contingency Plan, HSIA) They
jointly reviews the received information from the captain, decides on the activities and
responsibilities of the members.
6. The HERT is in constant communication with AHO and Director IEDCR and Disease
Control of DGHS.
7. Stair/ambulift of Ground Support Equipment (GSE) is at the special bay (Bay 14/F3)
where the plane is destined to park.
8. A trained cleaning team of three members one each from Biman cabin cleaning section
(cabin appearance), Ground Support Equipment (GSE) section and Facilitation and
Welfare section of CAAB is in waiting with PPE in hand.
9. By this time several other vehicles, including ambulance from airport and fire service,
van/micro bus/bus detailed from CAAB is ready at the special bay area. The aircraft
lands at the HSIA. ATC send the aircraft to a separate area (Bay 14 or F3) of the airport
for further action.
SEQUENCE OF EVENTS (PROCEDURES) UPON AIRCRAFT LANDING:
No.
9.1
Time
From To
Activity
Upon landing, the aircraft is sent to one far away holding lounge, bay 14
or F3 which, in such situation, will be cordoned/separated by the security
people to divert other flight passengers and staffs from being in contact
with any of the personnel's of the affected flight. DSO in consultation
with AHO (CMT lead) will coordinate these. If a holding lounge is not
available a cordoned holding area for the suspects has to be prepared.
Pilot informs the passengers about the situation and instructs the
passengers to be calm and remain in their seats).
19 Nov 2015
Page App 12-4
Civil Aviation Authority, Bangladesh
9.2
Aviation Public Health Manual
Health Emergency Response Team (HERT), a six-member team (two
airport medical officer, two Nurse/SI and two securities (detailed by
DSO)) arrives at the parking area by one ambulance. The team including
driver and support staff wears PPE.
At the same time other ambulance (number will depend on the number of
probable cases and suspects, as decided by the HERT) arrives and
positions itself nearby.
Other vans/micro bus/bus is placed at a distance.
A trained cleaning team of three members with their logistics (one each
from Biman cabin cleaning section-cabin appearances, Ground Support
Equipment (GSE) section and Facilitation and Welfare section of CAAB)
is in waiting with PPE in hand.
The other drivers and cleaners before engagement with cases or contacts
from the aircraft will wear their personal protective equipment.
9.3
The HERT boards the aircraft through the door nearest to the suspect case
by ambulift/stairs. The two airport security agents in protective equipment
secure the aircraft at the air stairs.
9.4
The team on board directly approaches the suspected passenger informed
by the flight attendant. The medical officers observe the case, enquire
about the symptoms, travel history and previous contacts in line with
standard questionnaire ( as attached) and determine status of the case and
suspected close contacts. Then with consultation with Director IEDCR and
AHO, they may come to the following decisions;
The team feels that the case does not fulfill the case definition of
communicable disease of national/international concern. They will
ask DAPO and DSO to initiate the process for usual customs and
immigration procedures immediately for all the passengers (but, in
that scenario the case and the close contact’s whereabouts and
contact details have to be collected in “Passenger Locator Card”
and followed up).
If the suspected case fulfills case definition, suspected close
contacts (passengers/crews) are identified;
Team (HERT) will provide mask to the case and suspects, ask
them to wear those and remain in their seats.
The cabin crew will be asked to evacuate other passengers through
other door/s or the same door (if none other is available) for usual
immigration and customs clearance. After that,
The suspected case in mask will be assisted and escorted by the
one Nurse/SI's to the aircraft stairs/ambulift.
The
Nurse/SI will accompany the suspected case to the airport
ambulance that is already waiting outside. The ambulance
immediately runs for the referral hospital through a predefined
route avoiding any contact with other staffs/passengers.
19 Nov 2015
Page App 12-5
Civil Aviation Authority, Bangladesh
9.4
Aviation Public Health Manual
The cleaning team in PPE will disinfect the aircraft stairs/ambulift after
suspected patient is transferred as per SoP.
9.4.6 The passengers/crews that might have been in contact with the
suspected passengers ( of the same row and two rows in front and two
rows back )will be then taken through the same stairs/ambulift to outside
the aircraft and then directly into the van/microbus that heads for the
isolation/quarantine room/holding area for further evaluation. The
remaining team accompanies them. If the team is convinced,
The suspects may be quarantined for 14-21 days for
observation and follow up. Or,
They may be sent home after customs and immigration
formalities, but keeping whereabouts and contact details
fulfilling the“ Passenger Locator Card” for future follow
up.
The cleaning team in PPE, again will disinfect the aircraft
stairs/ambulift after suspected patient transfer
If the suspected case fulfills case definition, and all the
passengers may be exposed;
All the passengers may be sent for isolation/quarantine.
After total evacuation, the cleaning team in PPE, with
additional persons will disinfect the whole aircraft
following SoP.
(**MERS-CoV is air-borne disease. Although Ebola is not air – borne
disease, but there might be possible contact with fluids in the airplane
(e.g. neighboring seats and other surfaces in the airplane), due to
sneezing etc. For MERS-CoV quarantine period is 14 and Ebola 21
days).
The passengers/crews, particularly the suspected contacts will be
provided with detail information about whom and when to contact
(Emergency HOT Lines of IEDCR; 01937110011, 01937000011,
01927711784 and 01927711785) if one or more of the following
symptom appears; fever, breathing difficulties, weakness, muscle pain,
headache, sore throat, vomiting, diarrhoea, rash, or bleeding. Passengers
will also be asked to record their temperatures twice daily for 21 days
and report higher temperature deviations.
The waiting ambulance/van/microbus/bus (for the passengers to be put in
quarantine or for the passengers that have to face the immigration
formalities, in accordance to the direction of the onboard medical officers
will be used as required.
19 Nov 2015
Page App 12-6
Civil Aviation Authority, Bangladesh
9.4
Aviation Public Health Manual
The drivers and support staffs of the vehicles carrying the suspect or
isolated/quarantined passengers will always wear protective clothes.
The quarantine provides all necessary conditions (accommodation, food
and medical care. The passengers will be provided the means to contact
with and inform their families).
9.5
* Within the airport area three entitites are responsible for cleaning
services. Biman cabin cleaning section (inchrge cabin appearance
section) is responsible for cleaning the aircraft; the stair and ambulift
cleaning is under the Ground Support Equipment (GSE) section and
Facilitation and Welfare section of CAAB is responsible for the runway
and airport area.
* Within the aircraft the Universal Precaution Kit (UPK) contains along
with other logistics some disinfectant and biohazard bag, which may be
used to dispose of the contaminated materials.
* Generally the biohazard bag and PPE will be available for these
purposes through the Airport Health Office.
*Generally a three member cleaning team, each from different section
will be grouped together and trained to perform the cleaning and
decontamination activities during this type of emergency.
Cleaning team in PPE cleans and disinfects aircraft stairs/ambulift each
time the case or contacts use it.
After disembarkation of all the passengers, the aircraft will undergo
thorough cleaning and decontamination process following cleaning
SoP/WHO guidance. All the waste is collected in biohazard bag and
disposed off according to waste disposal SoP. Reusable logistics are
thoroughly decontaminated and cleaned. The used passenger vehicles
will also be treated likewise
A cleaner in PPE with pump sprayer disinfects the HERT members
before they appropriately remove and dispose off their personal
protective equipment in yellow biohazard plastic bags.
The cleaners wait for 10 minutes in order that the disinfectant to have the
effect, after which they take off the PPE according to the SoP. They
perform personal disinfection of hand with appropriate liquid hand
disinfectant. The PPEs that has been already used is placed in biohazard
plastic bags for disposal of infectious waste, and will be handled by the
airport common waste management system, with a special vehicle for
medical waste.
19 Nov 2015
Page App 12-7
Civil Aviation Authority, Bangladesh
9.6
Aviation Public Health Manual
At the hospital entrance the ambulance carrying the suspected case
arrives along with the nurses/SIs. The case is sent immediately to the
isolation room for proper medical care under strict infection control
measures following hospital infection control SoP.
Once the patient enters the isolation room, a cleaner in PPE disinfects
the transportation route.
The same cleaner will also disinfect the ambulance as per vehicle
cleaning SoP.
9.7
The van transporting close contacts (passengers/crews) arrives and they
are put in the quarantine room.
A cleaning team in PPE disinfects the transportation route and the
ambulance/vehicles.
*The passengers remain in quarantine for 21 days or until confirmed to
have negative Ebola/MERS-CoV/H7N9 test results.
9.8
The concerned flight operator will provide all the relevant
documents/information of the cases and contacts to the Customs and
Immigration authorities. The rules for such emergencies/disasters will
become effective in such situations.
Ground handling will retrieve the baggage of the case and close contacts
along with their accompanying person/s, ensure customs check up and
deliver the baggage to the referral hospital/quarantine area.
Immigration authority will ensure clearance of the sick passenger/close
contacts on a priority basis.
10. According to the provisions of the International Health Regulations (2005) and the
adopted Protocol for Handling and Reporting at the entry point HSIA in case of public
health emergency or URGENT circumstances of international significance caused by
biological agent, the national contact point for the International Health Regulations
(Director, communicable Disease Control) informs immediately (within 24 hours) the
WHO Regional Office in New Delhi and the WHO Office in Dhaka, Bangladesh.
11. upon informed by Director, CDC, the Ministry of Health and Family Welfare
immediately organizes a press conference so to present to the media the latest
circumstances in a timely and objective manner as well as to prevent the spreading of
panic and misinformation among the population.
12. In the upcoming days, the population is regularly updated on the course of events, on the
situation with the infected persons and those in quarantine. Information materials are
prepared and distributed, providing general facts about Ebola/MERS-CoV/H7N9 (clinical
overview, mode of transmission, preventive measures). In order to calm the population,
the competent authorities inform: “The cases of Ebola/MERS-CoV/H7N9 have been
imported.
19 Nov 2015
Page App 12-8
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
13. All necessary measures have been undertaken to prevent the spread of the disease. The
persons that were in contact with the infected persons are put in 21-days quarantine under
constant supervision. The health status of the remaining passengers who were sent home
is continuously monitored for a 21-days period by the epidemiologist of the IEDCR.
14. If the Ebola/MERS-CoV/H7N9 test results obtained in the reference laboratory in
(IEDCR/ designated laboratory at home and abroad) are negative, the quarantine will
terminate as well as the health monitoring of the remaining passengers. The patients
admitted at the KGH for infectious diseases and febrile conditions will be treated for the
primary disease as per the evidence-based medicine.
References:
(1) CMT composition (Annex C, Multihazard Public Health emergency Contingency
Plan of HSIA)
(2) Questionnaire : will include the followings:
When did the symptoms first appeared: fever, vomiting, diarrhoea, stomach pain,
fatigue, Cold, runny nose?
Was there any history of contact with someone infected with similar symptoms ?
Where did he travel in the recent past??
To the flight attendant and the flight crew: Which crew/s came in contact with the
suspected passenger? Did the suspected passenger use the toilets or move around
or were in any contact with any of the other passengers? Whether any symptoms
among the close contacts?)
19 Nov 2015
Page App 12-9
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
INFECTIOUS DISEASE THREAT IDENTIFIED AT HEALTH DESK
Health Desk
IEDCR Hot lines
01937110011,
01937000011,
01927711784 and
01927711785
Duty Medical
Officer (DMO)
8914249/8914247
Director HSIA
(01913503810)
8901449, 8914870-4/ 3377
(Director CDC and IEDCR)
Referral Hospital
(01769010200)
Health Emergency
Response Team
Airport Fire Station
(8914870-4/3233,
3205),
(HERT)
Duty Security Officer
(DSO), HSIA
DAPO, HSIA
CMT (Lead Air Port
Health Officer)
017160887481
19 ov 2015
Page App 12-10
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
1. After disembarkation, on their way to immigration, the passengers will be passing
through the thermal scanner at health desk, and it beeps (there is a WHO/Public Health
Authority declared emergency in place).
2. In accordance to the International Health Regulations (IHR 2005) and the protocol for the
entry point Hazrat Shah Jalal International Airport (HSIA) in public health emergency
caused by biological agent, the following sequence of events shall be taken:
No
Time
From
Activity
To
2.1
2.2
19 Nov 2015
The Nurse/SI in mask and gloves (minimum infection control
measure) at the health desk identifies the passenger as a suspect
with communicable disease and a potential public health Threat.
They stop the passenger and accompanying personnel and inform
on Duty Medical Officer (DMO) for his advice and presence,
mentioning the suspected infectious case at the desk.
They request the passenger to come to the examination room
designated for and the accompanying passengers to wait in the
chairs placed outside.
After doing that, they will remove the mask and gloves, put them
in the biohazard bag and wear another set of mask and gloves to
welcome new case/s (if any). The Health desk staffs with those
minimal infection control measures will not go for any close
encounter with the suspects.
DMO arrives;
Before entering the examination room DMO will change into full
gear. Personal Protective Equipment in the designated donning
area.
DMO will move to the patient examination room a. Take history of the patient including symptoms,
demographic and contact information
b. Take history of his/her origin of travel including transit
places.
c. Take travel history e.g. visit history of West African
countries ( Sierra Leon, Liberia, Nigeria, Guinea) for
EBOLA within last 21 days and Middle-eastern countries
and South Korea for MERS-CoV within last 14 days ( at
the present context).
d. DMO will also check the travel documents of the
passengers.
e. DMO will take temperature by Infrared thermometer and
record it and will examine for other signs
Page App 12-11
Civil Aviation Authority, Bangladesh
2.2
Aviation Public Health Manual
f. DMO will ask for any other accompanying persons of
the suspected passenger and their physical status.
g. DMO will provide immediate medication if required.
h. After check up at the examination room of health desk,
if there is no signs and symptoms associated with
communicable diseases of concern or there is no
epidemiological link proven by checking the travel
documents and travel history, DMO will inform all
concerned about that.
The passenger/crew will fill in the “Passenger Locator Card” and
allowed to go to the immigration desk to finalize the immigration
procedures as usual.
2.3
DMO, if confirmed of suspicion,
If required will activate HERT after consultation with AHO
Will inform immediately the
i Airport ambulance of Airport Fire Station
ii CSO
iii Flight operator
iv Referral hospital
v Director HSIA, IEDCR and CDC of DGHS
vi Immigration
To be vigilant for other similar suspects in line
To take appropriate measure for infection control by wearing
mask and gloves and follow safe hygienic practices
To request passengers to fill in the “Passenger Locator Card”
and collect those from the passengers Will have relevant
information of the suspects travel and baggage documents
Will ask the Nurse at the health desk to wear PPE to
accompany the case/s when the ambulance arrives
2.4
Director HSIA (after consultation with Director IEDCR and CDC,
DGHS) will declare health emergency and activate the Crisis
Management Team (CMT).
23 Nov 2015
Page App 12-12
Civil Aviation Authority, Bangladesh
2.5
2.6
2.7
2.8
19 Nov 2015
Aviation Public Health Manual
Ambulance will arrive immediately, the driver and auxiliary
staff will wear PPE.
The suspect patient will be shifted to the ambulance through a
separate door with no/minimum chance of contact with other
passengers and airport staffs.
The Nurse in PPE will accompany the patient.
After the probable case is transferred,
DMO will doff PPE at the designated doffing station
The whole examination room, doffing area including exit way
upto the ambulance parking area has to be decontaminated with
0.5% chlorine solution
Desk, table, chair and other used logistics will be
decontaminated.
All the waste including the used mask, gloves, PPEs will be put
in a biohazard bag and disposed off accordingly.
The process will be performed by the trained cleaning team in
PPE. Health Team will supervise the decontamination process.
Ambulance driver and accompanying Nurse and support staff
will wear PPE just before receiving the patient.
Ambulance will transfer the patient/s to the referral hospital
through a specified route (shortest possible way towards Gate
8) with adequate precaution of infection control measures.
After transfer of the patient to the referral hospital, they will
doff their PPE, put them in biohazard bag and complete hand
hygiene practices. The ambulance will be thoroughly
decontaminated with 0.5% chlorine solution spray/fog by
trained cleaners in PPE in the referred hospital. After that the
ambulance will be again washed with soap water to wash off
the residual chlorine and dried for new assignments.
The waste including the PPEs used will be put in a biohazard
bag and dispose off accordingly.
The “Passenger Locator Card” available at health desk and
immigration area will be collected at the Immigration. For
these passengers a Leaflet will be provided with detail
information about whom and when to contact (Emergency
HOT Lines of IEDCR; 01937110011, 01937000011,
01927711784 and 01927711785) if one or more of the
following symptom appears; fever, weakness, muscle pain,
headache, sore throat, vomiting, diarrhoea, rash, difficulty in
breathing or bleeding. Passengers will be asked to record their
temperatures twice daily for 21 days and report any symptom
of illness on a daily basis.
Page App 12-13
Civil Aviation Authority, Bangladesh
2.8
Aviation Public Health Manual
“Passenger Locator Card ” will be available in the Aircraft, health
desk and in the immigration area
AHO will update Director DC and IEDCR of DGHS and HSIA, on the
details of travelers detected by the thermal scanners, total number of
travelers examined, details of the cases sent to the referral hospital
including their current updates, status of the close contacts etc.
After being informed by DMO, assisted by the flight operator,
A .Ground handling agents will retrieve the baggage of the passenger
and/or accompanying person/s, conduct surface cleaning, and ensure
customs check up. The patient need not stay back for baggage, but
authority will ensure that the baggage reaches to the passenger.
Immigration authority will ensure clearance of all immigration
formalities for an arriving sick traveler and any accompanying person/s
on a priority basis in accordance to the plan in emergency and
disasters.
2.9
3.
4.
5.
6.
Just after being informed of the situation AOC, PRO and SATO
together or individually within their capacities will handle the next of
kin’s of the affected flight passengers and the media. They need to
update time to time the status of the affected flight and the passengers,
prepare and deliver press release when seen appropriate.
According to the provisions of the International Health Regulations (2005) and the
adopted Protocol for Handling and Reporting at the entry point HSIA in case of public
health emergency of national/international concern caused by biological agent, the
national contact point for the International Health Regulations (Director, Disease
Control) informs immediately to the Ministry of Health and Family Welfare and within
24 hours, the WHO Regional Office in New Delhi and the WHO Office in Dhaka,
Bangladesh.
Upon informed by Director, DC, DGHS, the Ministry of Health and Family Welfare
immediately activates the IHR committees at different level. At the same time initiates
the Risk Communication activities to provide the latest updates to the media and general
population in a timely and objective manner as well as to prevent the spreading of panic
and misinformation among the population.
In the upcoming days, the population is regularly updated on the course of events, on the
situation with the infected persons, those in quarantine and the measures taken to contain
the situation. Information materials are prepared and distributed, providing general facts
about Ebola/MERS-CoV/H7N9 (clinical overview, mode of transmission, preventive
measures etc.).
If the Ebola/MERS-CoV/H7N9 test results obtained in the reference laboratory are
negative, the quarantine will terminate as well as the health monitoring of the remaining
passengers. The patients admitted at the KGH for infectious diseases and febrile
conditions will be treated for the primary disease as per the evidence-based medicine. All
these will be coordinated and decided by the National Rapid Response Team of IEDCR.
19 Nov 2015
Page App 12-14
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual
References
(1)
(2)
(3)
(4)
(5)
(6)
(7)
(8)
(9)
(10)
(11)
(12)
(13)
Suspected communicable disease: General Guidelines for cabin crew, IATA, October
2011
Airport preparedness guidelines for outbreaks of communicable diseases, issued by ACI
and ICAO: Revised April 2009.
WHO International Health Regulations (2005), 2nd edition, Reprinted 2008
ICAO Health Related Documents- Annex 6, Attachment B (Medical supplies), Amended
in 2009 & M CARs
ICAO Annex 14, Doc 9137, Part 7, Airport Services Manual
Procedures for Air Navigation Services- Air Traffic Management (PANS-ATM, Doc
4444)
IATA Medical Manual, 7th Edition, 2015
World Health Organization (WHO), Guide to Hygiene and Sanitation in Aviation, third
edition, Geneva 2009
Guide to Hygiene and Sanitation in aviation by James BAILEY, World Health
Organization Geneva 1977
ICAO Annex 9 to the convention on International Civil Aviation (Facilitation), Thirteen
edition, July 2011
Food Safety Plan, Food and Environmental Hygiene Department, Public Health
Laboratory Centre, Shek Kip Mei, Kowloon
ICAO: An Aviation Public Health Emergency Preparedness Plan: Cooperative
Arrangement for the Prevention of Spread of Communicable disease through air travel
(CAPSCA).
Environmental Conservation Rules, 1997 Ministry of Environment and Forest,
Government of the People’s Republic of Bangladesh.
----- END -----
19 Nov 2015
Page Ref 1-1
Civil Aviation Authority, Bangladesh
Aviation Public Health Manual