Guideline
[Optional heading here. Change font size to suit]
Document Number # QH-GDL-406:2013
Routine Visual Evoked Potentials
Clinical Neurophysiology
1. Purpose
This guideline provides recommendations regarding best practice to support high quality
visual evoked potentials (VEP) practice throughout Queensland public health facilities.
2. Scope
This guideline provides information for all clinical measurement practitioners who perform
routine VEP.
This guideline relates to the performance of pattern reversal (PR) (checkerboard) and flash
VEP’s in clinical practice for children and adults who have the ability to concentrate and
comply with the test requirements.
This guideline provides minimum requirements for recording a routine VEP.
3. Related documents
Authorising Policy and Standard/s:
•
This Guideline is primarily based on the International Society for the Clinical
Electrophysiology of Vision (ISCEV) standard for Clinical Visual Evoked Potentials
(2010). References from alternate sources of information have been identified in
this document.
Procedures, Guidelines and Protocols:
•
Queensland Health Guide to Informed Decision-making in Healthcare 1
•
Australian Guidelines for the prevention and control of infection in healthcare
(CD33:2010) 2
•
International Organisation of Societies for Electrophysiological Technology (OSET)
Guidelines for Infection Control in the Clinical Neurophysiology Department 1999 3
Forms and templates:
•
Consent to clinical digital images 4
Version No.: <no>
Version No.: <no>
; Effective From: <date>
; Effective From: <date>
Effective From: 07/12/2013
Page 1 of 16
Page 1 of 16
Page 1 of 16
Department of Health: Routine Visual Evoked Potentials
4. Guidelines for performing routine visual evoked potentials (VEP)
4.1.
•
4.2.
Emergency Protocol
Follow Hospital and Health Service (HHS) protocols in the event of an emergency.
Infection Control Procedures
•
International Organisation of Societies for Electrophysiological Technology (OSET)
Guidelines for Infection Control in the Clinical Neurophysiology Department 1999 3
•
Australian Guidelines for the prevention and control of infection in healthcare 2
(2010) http://www.nhmrc.gov.au/node/30290
•
Local Hospital and Health Service guidelines.
4.3.
•
4.4.
Gaining Consent
Gain the patient’s consent using the Queensland Health Guide to Informed
Decision-making in Healthcare document 1.
Identifying Indications/Contraindications
The indication for performing a VEP is for investigation of function of the visual sensory
pathway. This can include but is not limited to:
•
clinically silent central nervous system lesions in multiple sclerosis
•
visual field defects such as hemianopia
•
central scotoma.
Contraindications for performing a PRVEP include:
•
marked visual impairment
•
acute optic neuritis
•
inability to co-operate with the testing procedure.
Note: If clinically indicated a flash VEP may be appropriate in these instances.
4.5.
Facilities and equipment
•
Perform the routine VEP within a quiet, temperate room with controllable light
levels.
•
Ensure the patient can sit comfortably for the duration of the set up and recording.
•
Ensure the patient is able to view and concentrate on the stimulus pattern
comfortably and with minimal disruption for the duration of the recording.
Effective From: 07/12/2013
Page 2 of 3
Department of Health: Routine Visual Evoked Potentials
4.6.
Personnel and training requirements
Relevant training includes:
•
Undergraduate course(s) offered at Central Queensland University and Charles
Sturt University
•
Graduate Certificate in Clinical Neurophysiology offered at Charles Sturt University
•
American Society of Electroneurodiagnostic Technology www.aset.org.
4.7.
Test Procedure
4.7.1. Electrodes
Electrode Placement
This guideline will refer to the 10/20 system of electrode placement as the
internationally recognised standard 5.
For the performance of routine visual evoked potentials, place the electrodes in
accordance to the International 10/20 System of Electrode Placement 6.
Place the recording electrodes at O1, Oz, O2. T5 and T6 can be placed if there are
available recording channels. Place a reference electrode at Fz and a ground
electrode at Cz 7.
The Queen Square electrode placement can be utilised as an alternative method
and has been shown to be useful when investigating hemi field defects 5, 8.
Electrode Choice
For electrodes used to record a VEP, ensure undistorted recordings of no less than
a frequency range of 10 –100Hz 6.
Ensure the electrodes used are of the same material - preferably silver/silver
chloride (Ag/AgCl) or gold cup 9.
Electrode Impedance
Measure electrode impedance prior to each recording. Electrode impedance should
also be measured at any time during the VEP where an electrode needs to be
altered or adjusted. Electrode impedance should be 5Kohms or below and be of a
similar value, i.e. within 3kohm range of each other 5.
4.7.2. Machine parameters
Common Mode Rejection Ratio
For common mode rejection to work effectively, ensure the active and reference
electrodes are of equal impedance and all input electrode impedances maintained
below 5Kohms 10.
For VEP’s, set the common mode rejection ratio to 120dB or greater 6.
Effective From: 07/12/2013
Page 3 of 3
Department of Health: Routine Visual Evoked Potentials
Input impedance of pre-amplifiers
Set the pre-amplifiers for the performance of VEP’s to at least 100MΩ 6.
Analogue to digital signal conversion
Ensure the sample rate is a minimum of 500 samples per second per channel with a
minimum resolution of 8bits 5.
Automatic artefact rejection
Ensure automatic artefact rejection excludes signals that exceed +/- 50-100uV in
amplitude and return to baseline rapidly following a high amplitude artefact 5.
Filters
For the purpose of VEP’s filters shall be set to the following levels:
•
low Pass/High Frequency Filter ≥ 100Hz
•
high Pass/Low Frequency Filter ≤ 1Hz 6.
The use of the 50Hz ‘notch filter’ is strongly discouraged. Any applicable artefact
can be rectified by addressing the source of the interference, such as nearby
electrical equipment or the recording electrodes 6.
Sweep duration
Generally 250ms post stimulus for adults is sufficient however if major response
components are significantly prolonged or delayed, a longer analysis time may be
required to obtain reproducible results (up to 500ms) 11.
In children an analysis time of up to 400ms post stimulus may be required, or
enough to adequately visualise a response 6.
Averaging
At least 100 individual trials to be averaged – more may be required (up to 400) to
ensure reproducibility in low amplitude responses and to ensure that a stable
waveform is recorded with minimal noise 5.
The quality of the recorded data shall be monitored while averaging the signal to
ensure integrity and patient compliance/alertness. If compliance or fixation wanes
during the recording, more trials may need to be averaged 7.
At least two total runs should be obtained and superimposed to verify reproducibility
of waveform morphology, latency and amplitude 11.
4.7.3. Recording
Patient Information
Document the following details as minimum, with any VEP recording:
•
patient name
•
hospital reference number or unit record (UR) number
•
date of birth
Effective From: 07/12/2013
Page 4 of 3
Department of Health: Routine Visual Evoked Potentials
•
recording date
•
referring doctor
•
recording practitioner initials
•
recording time
•
relevant clinical details
•
clinical question to be answered
•
current medications
•
visual acuity.
Determine the visual acuity of the patient prior to performing any VEP procedure.
Allow the patient to wear their prescription glasses or contact lenses 6.
Note: It is important to make a note of any extreme pupil sizes or any anisocoria.
For pattern reversal stimuli the patient must not have had any mydriatic or miotic
drugs.
Confirm the pupils are not dilated prior to the VEP using flash stimuli 6.
Patient Attention
Monitor the patient’s attention throughout the recording to ensure alertness and
compliance with the requirements of the test.
If the patient becomes drowsy and loses the ability to readily fixate on a point, use
encouragement and interaction to ensure that the latency of responses is accurate
11
.
4.7.4. Pattern reversal full field
An alternating, high contrast black and white checkerboard is the standard pattern
stimulus used 6.
If an abnormal VEP is obtained in a patient with visual symptoms, perform a pattern
electroretinogram (pERG) if available 6. See section 4.7.8 and Appendix 1 for
further information relating to pERG.
Example of Full Field Recording Montage (5 channel and 3 channel, respectively) 5:
Channel 1: T5 to Fz
Channel 1: O1 to Fz
Channel 2: O1 to Fz
Channel 2: Oz to Fz
Channel 3: Oz to Fz
Channel 3: O2 to Fz
Channel 4: O2 to Fz
Ground: Cz
Channel 5: T6 to Fz
Ground: Cz
Effective From: 07/12/2013
Page 5 of 3
Department of Health: Routine Visual Evoked Potentials
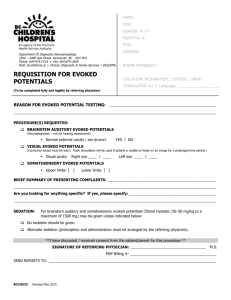
Pattern Reversal Full Field Markers:
N75 – 1st negative peak (1st upward deflection)
P100 – 1st positive peak (1st downward deflection)
N145 – 2nd negative peak (2nd upward deflection) 11
Figure 1: Taken from Liveson (1992): Example of pattern reversal VEP waveforms
12
.
Note: Please note, this image is provided as an example of waveform morphology only; not
amplitude and latency.
Settings
Stimulus Type
•
alternating high contrast (black and white) checkerboard 13
Stimulus rate
•
1-3 reversals per second or 200ms on and 400ms off 6, 13
Phases
•
responses to phases are averaged with the opposite phase 13
Brightness contrast:
•
contrast between black and white shall be greater than 80% 5, 6
Intensity:
•
Ensure the mean luminance of the stimulus is greater than 50 cdm-2 and there
is no change in mean luminance during the reversal of the pattern 5.
•
Ensure the luminance is uniform and varies no less than 30% between the
centre and periphery of the visual field 6.
Effective From: 07/12/2013
Page 6 of 3
Department of Health: Routine Visual Evoked Potentials
•
Lighting within the recording room should be homogenous with an average
room luminance equal to the average stimulus luminance; however the
luminance of the background beyond the checkerboard stimulus is not critical to
the results 6.
Stimulation
•
Monocular stimulation is used to ensure that there is no masking of a unilateral
conduction abnormality 14.
Check width
•
Different check sizes can be used separately; large or small 5.
•
Large checks should measure 60’ of arc (1˚ ± 20%); small checks should
measure 15’ (0.25˚ ± 20%)6.
Field Size
•
While it is not necessary to use a square field (for example computer monitor
displaying the stimulus pattern does not need to be square) ensure the aspect
ratio between width and height does not exceed 4:3 and the field size is at least
15˚ (of visual angle) at the smallest point6.
Check colour
•
Use an equal number of black and white checks6.
Fixation point
•
The fixation point shall be located in the centre of the screen positioned at the
corner of four checks 11.
Distance of stimulus from patient
•
4.7.4.1.
The distance between the patient and the stimulus can range from 50 -150 cm,
dependent on the visual arc required6. Measure the distance from the nasion to
the fixation point on the screen.
Pattern reversal hemi field
Each eye is tested separately to both left and right hemi-field stimulation;
whereby the pattern is presented to one half of the visual field on one side of
the fixation point 11.
Example of Hemi Field Recording Montage, Queen Square method (5 channel
and 3 channel, respectively) 5:
Channel 1: L10 to Fz
Channel 1: L5 to Fz
Channel 2: L5 to Fz
Channel 2: M0 to Fz
Channel 3: M0 to Fz
Channel 3: R5 to Fz
Channel 4: R5 to Fz
Ground: Cz
Effective From: 07/12/2013
Page 7 of 3
Department of Health: Routine Visual Evoked Potentials
Channel 5: R10 to Fz
Ground: Cz
Pattern Reversal Hemi Field Markers:
N75 – 1st negative peak, 1st upward deflection
P100 – 1st positive peak, 1st downward deflection
N145 – 2nd negative peak, 2nd upward deflection11
Settings:
As for full field stimulation settings, except for the following:
Stimulus rate
•
maximum of 4 reversals per second 11
Brightness contrast
•
Ensure the contrast between black and white checks is at least 50% 11.
Stimulation
•
Monocular stimulation is used to ensure there is no masking of a unilateral
conduction abnormality 14.
•
Each eye is tested to both left and right hemi-fields separately 11.
Check width
•
Different check sizes can be used separately; large or small 5.
•
Large checks should measure 60’ of arc (1˚ ± 20%); small checks should
measure 15’ (0.25˚ ± 20%) 6.
Field size
•
While it is not necessary to use a square field (for example computer monitor
displaying the stimulus pattern does not need to be square) ensure the
aspect ratio between width and height does not exceed 4:3 and the field
size is at least 15˚ (of visual angle) at the smallest point 6.
Fixation point:
•
The fixation point is still to be located at the centre of the stimulus screen,
however it will only be located in the corner of 2 checks for hemi-field
stimulation 11.
Effective From: 07/12/2013
Page 8 of 3
Department of Health: Routine Visual Evoked Potentials
4.7.5. Flash stimulus
Flash stimulus VEP’s are used infrequently and are reserved primarily for infants and other
patients that cannot maintain fixation and when reduced visual acuity cannot be
rectified 7.
Example of Full Field Flash Recording Montage (5 channel and 3 channel) 5:
Channel 1: T5 to Fz
Channel 1: O1 to Fz
Channel 2: O1 to Fz
Channel 2: Oz to Fz
Channel 3: Oz to Fz
Channel 3: O2 to Fz
Channel 4: O2 to Fz
Ground: Cz
Channel 5: T6 to Fz
Ground: Cz
Flash Recording Markers
6 peaks appear in the first 250ms and are labelled as:
I or N1 (negative peak 1)
II or P1 (positive peak 1)
III or N2 (negative peak 2)
IV or P2 (positive peak 2)
V or N3 (negative peak 3)
VI or P3 (positive peak 3) 6, 11.
Figure 2: 1 Taken from Smith (2006) pg 131 15
Note: This image is provided as an example of waveform morphology only;
not amplitude and latency, also the polarity is reversed on this example.
Effective From: 07/12/2013
Page 9 of 3
Department of Health: Routine Visual Evoked Potentials
4.7.6. Stimulus Type/Pattern generator:
A white flashing light is the stimulus utilised in flash VEP’s. This can be delivered to
the patient via a stroboscope lamp (similar to that used in photic stimulation in EEG)
or via a ganzfeld stimulator 5.
Stimulus rate
•
Ensure the stimulus of flashes of while light occurs at 1-2Hz 5.
Intensity
•
Ensure the luminance of the flash is at least 3cd/sm-2, 6 .
Stimulation
•
Monocular stimulation is used to ensure that there is no masking of a
unilateral conduction abnormality 14.
Field Size
•
Ensure the flash stimulus subtends a visual field of at least 20˚ 6.
Distance of stimulus from patient
•
The distance between the patient and the flash stimulus is 30 cm 7.
4.7.8 Pattern Electro Retino-gram (pERG)
Use the PERG (if available) in a patient with an abnormal visual evoked potential to
establish whether a retinal (macular) disorder is present, and thus differentiate
between macular and optic nerve dysfunction as a cause for the VEP abnormality
16
.
For the purpose of incorporating the pERG in the VEP test set up, the VEP
stimulating visual arc, luminance, contrast and reversal rate parameters are used.
Example montages for full field pattern reversal or flash stimulation incorporating an
ERG channel
10:20 System
Queens Square
Channel 1:
iERG - iOC
Channel 1:
iERG - iOC
Channel 2:
O2 to Fz
Channel 2:
R5 to Fz
Channel 3:
Oz to Fz
Channel 3:
MO to Fz
Channel 4:
O1 to Fz
Channel 4:
L5 to Fz
Ground:
Cz
Ground:
Cz
Effective From: 07/12/2013
Page 10 of 3
Department of Health: Routine Visual Evoked Potentials
Electrodes
4.8.
•
A fibre electrode can be placed on the lower eyelid and tethered at the nasal
canthus and lower outer canthus of the eye 16.
•
Place a reference electrode at the ipsilateral outer canthus (iOC) of each eye 16.
•
Impedances of the reference and ground electrodes should be less than 5KΩ
and equal. It is recommended not to measure impedance when the recording
electrode is on the eye unless explicitly specified by the particular equipment
manufacturer 16. This applies current to the eye which is contraindicated.
Quality Control Procedures
Refer to the International Organisation of Societies for Electrophysiological Technology
(OSET) Guidelines for Digital EEG 17.
Normal Values
•
Establish normative data using standard stimuli and recording parameters for each
neurophysiology laboratory 6.
•
Recording parameters such as ambient light, pattern luminance and contrast shall
be the same for all patients tested and for all subjects from which normative data is
obtained 11.
•
Normative values from other institutions or sources may only be utilised if
equivalent stimulation and recording parameters are employed and only after
testing the validity of the adopted normal values on at least 10 locally gathered
subjects under normal recording conditions 18.
•
Note that normative values may be influenced by age, gender and differences in
visual acuity; and that acquired normative data for adults must be in a given age
range. Additional normative data may need to be acquired for elderly (>60) or
paediatric (<5) populations 6, 7.
External checks of stimuli and recording parameters 10
For further information please refer to: Brigell, M., et al. (2003). "Guidelines for calibration
of stimulus and recording parameters used in clinical electrophysiology of vision."
Documenta Ophthalmologica 107(2): 185-193.
5. Review
This Guideline is due for review on: 07/12/2016
Date of Last Review: New Document
Supersedes: Nil
Effective From: 07/12/2013
Page 11 of 3
Department of Health: Routine Visual Evoked Potentials
6. Business Area Contact
Dane Enkera – Statewide clinical measurements network (Chair)
7. Definitions of terms
Term
Impedance
Definition / Explanation / Details
The apparent resistance of a circuit to the flow of
an alternating electric current.
Common mode
rejection ratio
The tendency of a differential amplifier to reject
input signals common to both input leads
Source
Blakiston’s Gould Medical
Dictionary, 4th ed.1979.
McGraw Hill, Inc.
Fundamentals of EEG
Technology, Tyner, et al 1983
Filters
Separate a range of frequencies to allow only
specific frequencies to be examined.
Spehlmann’s Evoked Potential
Primer, 2001 4.
Luminance
The brightness of a light-emitting source (e.g., a
view box or computer monitor). Measured in
cd·s·m‾² (candela-seconds per meter squared)
Mosby's Medical Dictionary, 8th
edition. © 2009, Elsevier.
Minute
A unit of angular measurement equal to one
sixtieth of a degree, or 60 seconds. Also called
minute of arc
Anisocoria
Inequality of the size of the pupils of the eye.
Mydriatic
Relating to dilated pupils of the eyes
Miotic
Relating to constricted pupils of the eyes
Collins English Dictionary –
Complete and Unabridged ©
HarperCollins Publishers 1991,
1994, 1998, 2000, 2003
The American Heritage®
Medical Dictionary Copyright ©
2007, 2004 by Houghton Mifflin
Company. Published by
Houghton Mifflin Company. All
rights reserved.
The American Heritage®
Dictionary of the English
Language, Fourth Edition
copyright ©2000 by Houghton
Mifflin Company. Updated in
2009.
The American Heritage®
Dictionary of the English
Language, Fourth Edition
copyright ©2000 by Houghton
Mifflin Company. Updated in
2009.
Effective From: 07/12/2013
Page 12 of 3
Department of Health: Routine Visual Evoked Potentials
8. Approval and Implementation
Policy Custodian:
Julie Hulcombe – Chief Allied Health Officer
Responsible Executive Team Member:
Dr Michael Cleary
Deputy Director General
Health Service and Clinical Innovation
Approving Officer:
Dane Enkera – Statewide Clinical Measurements Network (Chair)
Consulting stakeholders:
Key stakeholders (position and business area) who reviewed this version are:
•
Queensland Health Clinical Neurophysiology Working Party (Emma Fetherston,
Fred Tremayne, Jo Wex, Carolin Healion, Annett Koenig, Kane Curtis, Susan
Koklas)
•
Clinical Measurements Advisory Group (CMAG) for Clinical Education and Training
•
Association of Neurophysiological Technologists Australia (ANTA)
•
Dr Robert Henderson – Consultant Neurologist (RBWH)
•
Dr Kate Rinney - Consultant Paediatric Neurologist & Epileptologist (Mater)
•
Dr Stefan Blum – Consultant Neurologist (Redcliffe Hospital / RBWH)
•
Queensland Health Neurophysiology Laboratory Managers (as of 15/07/2011)
Approval date:
07/12/2013
Effective from:
07/12/2013
Effective From: 07/12/2013
Page 13 of 3
Department of Health: Routine Visual Evoked Potentials
9. Appendices
Appendix 1 – Pattern reversal electroretinogram (PERG)
The PERG (if available) shall be used in a patient with an abnormal visual evoked potential
to establish whether a retinal (macular) disorder is present, and thus differentiate between
macular and optic nerve dysfunction as a cause for the VEP abnormality 16.
Electrodes
A number of different types of electrodes can be used but the most practical and less
invasive type is a fibre electrode that can be placed on the lower eyelid and tethered at the
nasal canthus and lower outer canthus of the eye 16.
Reference electrodes are placed at the ipsilateral outer canthus of each eye 16.
A ground electrode can be placed anywhere on the head.
Impedances of the reference and ground electrodes should be less than 5KΩ and equal. It
is recommended not to measure impedance in situ of the actual recording electrode unless
explicitly specified by the particular equipment manufacturer 16.
Recording Parameters 16
Stimulus:
Use the following stimulus parameters:
•
reversing checkerboard pattern with check size of 8° and the mean of the width and
height of the stimulus field at 15°
•
luminance that does not vary during stimulation and is at a ‘phototopic’ luminance
level of 80 cd/m-2.
•
contrast of the black and white checks are at 100% and no less than 80%.
•
PERGs are performed in a dim room with no direct lights in the patient’s field of
view
•
the reversal rate is delivered at 2Hz.
Recording Equipment
Use the following parameters of the recording equipment:
•
minimum input impedance of 100MΩ
•
the bandwidth range from 1-100Hz
•
sweep time is 150ms or more
•
limits for artefact rejection are set no higher than ± 50 uV
•
a minimum sampling rate of 1000Hz
Effective From: 07/12/2013
Page 14 of 3
Department of Health: Routine Visual Evoked Potentials
Recording Procedure
Position
Position the patient in a comfortable chair with a head rest. Ensure the pupils are not
dilated.
Fixation
Locate a fixation point in the centre of the screen.
Acuity
Test the visual acuity and the patient’s vision, corrected with lenses if available.
Stimulation
Binocular recording is preferable over monocular stimulation.
Monocular stimulation can be used if the VEP and PERG and recorded simultaneously 16.
Averaging
Obtain at least 100 artefact free sweeps. More may be required to improve the signal to
noise ratio. Duplicate the test to ensure reproducibility.
Example Waveforms
Obtain normal values for each department.
10.
Suggested Readings and References
10.1. Suggested readings
•
American Clinical Neurophysiology Society Guidelines http://www.acns.org/
•
ISCEV standard for clinical visual evoked potentials (2009 update)
http://www.springerlink.com/content/53p616266t26n100/fulltext.pdf
•
Guidelines for calibration of stimulus and recording parameters used in clinical
electrophysiology of vision
http://www.springerlink.com/content/u5531g5268381707/fulltext.pdf
10.2. References
1.
2.
3.
Queensland Health. Informed decision making in health care 2012 Available from:
http://www.health.qld.gov.au/consent/default.asp.
National Health and Medical Research Council. Australian Guidelines for the Prevention
and Control of Infection in Healthcare. National Health and Medical Research Council;
2010 [cited 2012 12/09/12]; CD33:[Available from:
http://www.nhmrc.gov.au/node/30290.
Rimmington S. Guidelines for infection control in the clinical neurophysiology
department. American Journal of Electroneurodiagnostic Technology. [Review].
1999;39(4):289-300.
Effective From: 07/12/2013
Page 15 of 3
Department of Health: Routine Visual Evoked Potentials
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
Queensland Health. Clinical images / recordings consent form2012: Available from:
http://hi.bns.health.qld.gov.au/forms/patient_record/forms/mr_i_4910.pdf.
Holder GE, Celesia GG, Miyake Y, Tobimatsu S, Weleber RG, International Federation
of Clinical N. International Federation of Clinical Neurophysiology: recommendations
for visual system testing. Clin Neurophysiol. 2010 Sep;121(9):1393-409.
Odom JV, Bach M, Brigell M, Holder GE, McCulloch DL, Tormene AP, et al. ISCEV
standard for clinical visual evoked potentials (2009 update). Documenta
Ophthalmologica. 2010 Feb;120(1):111-9.
Misulis KEFT. Spehlmann's evoked potential primer. Boston; Oxford: ButterworthHeinemann; 2001.
Blumhardt LD, Barrett G, Halliday AM. The asymmetrical visual evoked potential to
pattern reversal in one half field and its significance for the analysis of visual field
defects. Br J Ophthalmol. 1977 Jul;61(7):454-61.
American Clinical Neurophysiology Society. Guideline 1: Minimum Technical
Requirements for Performing Clinical Electroencephalography2006: Available from:
http://www.acns.org/pdfs/Guideline%201.pdf.
Brigell M, Bach M, Barber C, Moskowitz A, Robson J. Guidelines for calibration of
stimulus and recording parameters used in clinical electrophysiology of vision.
Documenta Ophthalmologica. 2003 2003/09/01;107(2):185-93.
American Clinical Neurophysiology S. Guideline 9B: Guidelines on visual evoked
potentials.[Erratum appears in J Clin Neurophysiol. 2006 Aug;23(4):preceding 281],
[Reprint in Am J Electroneurodiagnostic Technol. 2006 Sep;46(3):254-74; PMID:
17042161]. J Clin Neurophysiol. [Guideline]. 2006 Apr;23(2):138-56.
Liveson JAMDMMDM. Laboratory reference for clinical neurophysiology. Philadelphia:
F.A. Davis; 1992.
Spehlmann R. Evoked potential primer : visual, auditory, and somatosensory evoked
potentials in clinical diagnosis. Boston: Butterworth; 1985.
Evans A, Boggs J. Clinical Utility of Evoked Potentials2010: Available from:
http://emedicine.medscape.com/article/1137451-overview#a1.
Smith NJGMvPP. Neurophysiological monitoring during intensive care and surgery.
Edinburgh: Elsevier; 2006.
Holder GE, Brigell MG, Hawlina M, Meigen T, Vaegan, Bach M, et al. ISCEV standard
for clinical pattern electroretinography--2007 update. Documenta Ophthalmologica.
[Practice Guideline]. 2007 May;114(3):111-6.
Gregory D. Guidelines for digital EEG. American Journal of Electroneurodiagnostic
Technology. [Review]. 1999 December;39(4):278-88.
Celesia Gg BMG. Recommended standards for pattern electroretinograms and visual
evoked potentials. The International Federation of Clinical Neurophysiology.
Electroencephalography and clinical neurophysiology Supplement. 1999;52:53-67.
Effective From: 07/12/2013
Page 16 of 3