Nasal Pressure Airflow Measurement
advertisement

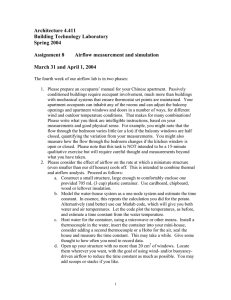
Nasal Pressure Airflow Measurement An Introduction Dr. David Rapoport, M.D. Robert Norman, M.S., R.R.T. Michael Nielson, R.R.T., R.PSG.T. Copyright © 2001 by Pro-Tech Services, Inc. All rights reserved Pro-Tech Services, Inc. 4338 Harbour Pointe Blvd. S.W. Mukilteo, WA 98275 (425) 322-0300 (800) 919-3900 Fax: (425) 322-0301 www.pro-tech.com Printed in the USA Preface The Polysomnogram, the “Gold Standard” test in the field of Sleep Medicine, has remained largely unchanged since the 1950’s. With the recognition of sleep disordered breathing as a common disease the focus has shifted beyond what was the original exclusive use of the EEG to characterize sleep, with an incidental interest in respiration, to a greater emphasis on respiratory monitoring. The tools to detect respiration, however, have only recently begun to evolve. Consequently, many laboratories still rely almost exclusively on nasal and oral thermistors (or thermocouples) to detect the presence and nature of breathing. Newer technologies for the measurement of airflow and detection of elevated upper airway resistance include the nasal cannula/pressure transducer system. The intensified interest in nasal cannula monitoring and the fact that many technologists are unfamiliar with its use have led us to conclude that a “primer” on this technique would be beneficial to provide information on the proper use and interpretation of the nasal pressure waveform. Dr. David Rapoport, M.D. Robert Norman, M.S., R.R.T. Michael Nielson, R.R.T., R.PSG.T. Contents Preface............................................................................................ iii Chapter 1: A Brief History of Respiratory Monitoring on NPSG .....................1 Chapter 2: Introducing Nasal Pressure Airflow Measurement..........................3 Chapter 3: How to Record the Nasal Pressure Signal .......................................5 Chapter 4: Extraction of the Snoring Signal from the Pressure Waveform ......9 Chapter 5: Common Problems.........................................................................11 Chapter 6: Nasal Pressure Airflow and NCPAP..............................................15 Chapter 7: Scoring Atlas..................................................................................21 Chapter 8: Frequently Asked Questions ..........................................................33 Bibliography and Acknowledgements...........................................43 Chapter 1 A Brief History of Respiratory Monitoring on NPSG Prior to the recognition of the syndrome of Obstructive Sleep Apnea (OSA), the main purpose of measuring respiration was to detect the timing of breaths. As the need to detect apnea increased during the 1970’s, the thermistor/thermocouple came into their own because they were ideal tools to identify the total absence of airflow. Their ease of use and comfort on patients has led to their being accepted as an integral tool in polysomnography. However, it is important to understand what is being detected and the limitations of this type of technology. By definition, thermistors and thermocouples are not airflow sensors but are simply detecting the temperature oscillation (between inhaled room air temperature and warmer exhaled air) as a qualitative indicator of airflow. Total cessation of airflow (apnea) is well detected because of the complete lack of temperature variation. In the mid 1980’s it became clear that it was clinically necessary to detect and count partial airway obstruction events, and the term hypopnea was introduced. Although the original description of hypopnea emphasized significant reductions in airflow it was natural to try to extract this information from thermistors and thermocouples that were in extensive use in most laboratories. However, in the case of incomplete airway obstruction, the relationship between temperature change and true flow is not straightforward. Thus the amplitude of the signal resulting from a partially obstructed breath may be reduced not at all (if the full effect of exhaled warm air is detected) or to a variable extent (depending on characteristics of the sensor and the way in which the signal is processed, e.g., filtered). An example of the lack of relationship between true flow amplitude of breaths and the signal obtained from a thermistor is shown on the left graph of Figure 1.1. PEAK INSPIRATORY FLOW 80 60 40 20 0 80 60 40 20 0 0 20 40 60 80 100 Pneumotach Flow (% full scale) Figure 1.1 100 (% full scale) Nasal Cannula Flow 100 (% full scale) Thermister Amplitude (SIMULTANEOUS COLLECTION) 0 20 40 60 80 100 Pneumotach Flow (% full scale) Despite the limitations of the thermistor/thermocouple, their use has persisted until recently as the usual clinical practice in most laboratories, and scoring of hypopnea has evolved to the following practice: events of reduced airflow are first identified from the respiratory (thermistor) signal; they are then validated as true hypopneas by their coincidence with desaturation or arousal on EEG. Typical definitions in use today required a decrease in the thermistor signal (50 – 75%) associated with oxyhemoglobin desaturation of 2% – 4% or EEG microarousal. However, if the thermal sensor does not detect a candidate respiratory event and there is no desaturation, arousals are left “unexplained.” As this pattern has been recognized in more symptomatic patients, this has led to the recognition of the Upper Airway Resistance Syndrome (UARS) - defined as the presence of repetitive arousals following periods of increased respiratory effort (detected by esophageal manometry) but undetected by thermal sensors. The degree to which thermistors under-detect respiratory events has recently been investigated. Up to 70% of respiratory events may be missed in patients with symptoms consistent with OSA but without frank apnea/hypopnea. In some cases, the number of events missed with simple thermal technology may be sufficient to alter the ultimate patient diagnosis.4, 12 A recent position paper from the American Academy of Sleep Medicine (AASM) reemphasized that the detection of reduced airflow (the entry into defining a hypopnea) could not be performed with thermistors or thermocouples and that these devices should be reserved for the detection of apnea only.1 Chapter 2 Introducing Nasal Pressure Airflow Measurement. What is Measuring Nasal Pressure and How is this Different from Thermistors and Thermocouples Data coming from direct measurement of respiratory airflow (using masks and pneumotachographs) began to accumulate in the 1980’s. These data showed that transient elevations in “resistance” in the upper airway could be detected as a plateau or flattening of the inspiratory waveform. Initially, though, the only technique available to accomplish this was full facial pneumotachography, which was not suited to general clinical practice. Others and we began to use a more non-invasive alternative to measure airflow during diagnostic studies: this consisted of a nasal cannula (standard for oxygen administration) connected to a sensitive pressure transducer. In a number of papers,2, 12 it was shown that the relative amplitude of breaths and morphology of the respiratory waveform obtained from this pressure signal reproduces that obtained from full facial pneumotach in most situations. Nasal cannula pressure systems generate this respiratory waveform signal by detecting the fluctuations in pressure caused by inspiration and expiration. Unlike the inspiratory and expiratory fluctuations recorded via temperature from a thermocouple or thermistor, these signals are truly proportional to flow. There is a theoretical need to apply a linearization to the pressure signal by taking its square root, but this does little to affect the shape of the signal in most cases. Consequently, nasal pressure (NP) airflow appears to be far more sensitive and accurate in the capture of hypopnea and “Respiratory Effort Related Arousals” (RERA) events. This increased sensitivity should clearly enhance the diagnostic yield obtainable in the Polysomnographic evaluation of sleep patients. As published in the AASM guidelines, the only “validated,” and thus recommended, technique for the identification of RERAs was the use of an esophageal balloon manometer to measure intrathoracic pressure in order to identify a pattern suggesting increasing respiratory efforts ending in arousal. This technique, however, has not gained wide acceptance because of patient comfort issues (perceived or otherwise). Consequently, in many clinical laboratories, the diagnosis of UARS is made by inference. It is assumed that subtle changes in respiratory pattern (building respiratory effort and/or cascading snoring) terminated by EEG arousal represent a respiratory event (RERA). An alternative used by some clinical laboratories is to demonstrate that the repetitive arousals (or movements) are reduced in a patient when nasal CPAP is applied. The availability of a simple direct measure of nasal airflow (the nasal cannula/pressure system) provides an alternative to the thermal based flow devices and affords a more direct method to detect RERAs. Recent data shows that the nasal cannula technique contains information about respiratory airflow not found in the thermistor, and can be used to detect the subtle flow/resistance changes characteristic of UARS (now called RERA) with results similar to those obtained with an esophageal manometer. The use of the nasal cannula technique is also in accord with the AASM recommendations that state that thermistors/thermocouples are NOT appropriate to the detection of hypopnea and RERAs.2, 6, 9, 12 In summary, recent published data have shown that the use of the nasal cannula pressure based technique for assessing airflow and upper airway resistance changes, unlike temperature based probes, reliably detect apnea, hypopnea, and the subtle flow limitation observed in the “Upper Airway Resistance Syndrome”.2, 3, 4, 5, 6, 8, 11, 12, 13 Chapter 3 How to Record the Nasal Pressure Signal In our experience, the most frequent problem that laboratories have with implementing a recording of NP airflow relates to amplifier choice and filter settings. Attention to these issues is critical in recording a hi-fidelity representation of respiratory airflow. This section deals with appropriate use of AC and DC amplifiers and filter settings. Filter Settings There are three types of filters provided by most recorders. These are: Low frequency filter (LFF) (often referred to somewhat confusingly as the “high pass filter”) High frequency filter (HFF) and 60 cycle filter (often referred to as the “notch” filter). On some polygraphic recorders the low frequency filter may be referred to as the “Time Constant.” This concept relates specifically to AC amplifiers. Low frequency filters are used to prevent the “wandering baseline” which occurs in some signals. The behavior of these amplifiers can be seen dramatically during the typical calibration that is done with a DC voltage (usually 50µV). When this voltage (a constant signal) is passed through the amplifier, a calibration signal, such as is shown in Figure 3.1 is generated. While the peak of the rise provides a value for “calibration” i.e., the size of a 50µV wave, the AC amplifier characteristic is to force any constant value back to baseline (even though the input value from the calibration source does not change). The time required for the pen deflection to fall back to 37% of its full amplitude is known as the “fall time constant”. There is an inverse relationship between the time constant and the low filter setting. Increasing the low frequency filter will decrease the time constant and vice versa. In general, a low frequency filter will attenuate or suppress any signal which changes at a frequency below the assigned frequency. If the “time constant” is relatively short, say 1 or 2 seconds, a respiratory airflow signal will begin to decay prematurely during a sustained breath, thus significantly affecting the morphology of the waveform. In the case of the NP airflow waveform, a short time constant can cause the plateau associated with inspiratory flow reduction to decay prematurely and become undetectable. In fact, with a short enough time constant (such as that used in thermistor recordings) ALL respiratory waveforms are changed to a near perfect sine wave appearance. The high frequency filter attenuates or suppresses all signals whose frequency is above the set value. This is extremely crucial when the user is attempting to isolate information generated from a specific frequency range, and gets rid of high frequency signals like muscle artifact in the EEG. This is also illustrated in the case of the snoring signal captured from the nasal airflow signal. When the high frequency filter is set to 70Hz, all information up to 70Hz is captured; this includes the snoring information. When the high frequency filter is set to 5Hz, only the slow information below 5 Hz is captured which would in this case be respiration. Notch or 60 cycle filters are used to attenuate or suppress a single narrow range of frequencies (typically 60 cycle “noise”). If chosen to eliminate a frequency which is not in the range of the desired signals, they do little to affect the physiological signal. Amplification: AC or DC In order to properly record the NP airflow signal, it is necessary to pay close attention to the decisions regarding the amplification (or system input type) of the airflow signal. This is true whether the airflow signal will be recorded on a polygraph or with a digital recording system. The first decision is whether you wish to record the data via AC or DC inputs. The main difference between AC and DC amplification is whether constant-voltage input will result in a constant-voltage output (this happens when you chose DC), or whether constant, or near-constant, voltage signals will be filtered out of the signal (this happens when you chose AC, and is described in the section on filtering, above). In the following descriptions, polygraph refers to either the classic analog polygraph or a computerized data acquisition system. Use of AC Input for the Nasal Cannula Pressure Signal During flow limitation, the inspiratory airflow can be nearly constant for over 2 seconds. A nasal pressure airflow transducer will output a nearly constant voltage throughout inspiration under this condition. In order for these events to be properly visualized in an AC configuration, the polygraph or other recording device must NOT be set to suppress such “nearly constant” signals. Thus it must have the capability of establishing a low frequency cutoff filter setting of 0.05Hz or less (or a time constant approximately 3 seconds). The optimal setting would be 0.01Hz (time constant approximately 5 seconds). This setting will allow the respiratory waveforms to appear essentially identical to a DC signal. An example of the effect of different recordings of the identical flow signal obtained from a nasal cannula pressure transducer output is shown in Figure 3.2. The bottom trace shows a flow limitation event recorded using a DC amplifier. During the flow limitation event, only a slight decrease in flow occurs during each inspiration. The top tracing shows the same event recorded through an AC amplifier with a low frequency filter that is set too high. During each inspiration flow falls back to zero flow (center line) well before inspiration ends. The middle tracing shows the same signal recorded with an AC amplifier with an appropriate low frequency filter set and is virtually identical to the DC recorded signal. The greatest disadvantage of using the AC recording settings is that many older systems, designed to record EEG type signals, do not have appropriate low frequency filters for respiration signals. Despite this, AC configurations have the advantage of ease of use and familiarity for the typically trained EEG or sleep technician. The transducer connects directly into the AC headbox, which is already in the patient room. Most commonly, a 1.5 mm safety connector is used in this configuration. This is not true of all recorders, though, and it is best to verify the correct input connector before purchasing a transducer. DC signals, however, must be connected to a special DC input on the polygraph, which may not be on the headbox. Figure 3.2: Effect of differing time constants. Use of DC Input for Nasal Cannula Pressure Signal The best way to record a good NP airflow signal is to use a DC amplifier or input port. This bypasses the need to worry about low frequency filter settings. The placement of the DC ports varies from recorder to recorder. Some systems place the DC ports in the tech room while others position them at the patient bedside. If they are located far from the patient in the tech room, it will be necessary to obtain an extension cable. The most common DC input connector is a 1/8” mini-phone jack but this is by no means universal. If you are unsure of the correct DC configuration for your Polygraph, contact the host Polygraph manufacturer. Sampling Rate When signals are recorded on a digital system, i.e., a computer, the actual values are not stored continuously, but rather are sampled at a set frequency. Sampling rate is often referred to as the “digitizing rate” or “sampling frequency”. This is the number of discrete values per seconds that are stored to represent the signal. For example, a sampling rate of 10Hz means that the value of the recorded signal amplitudes will be measured at 10 equally spaced “samples” in each second. These can be displayed as a “continuous” tracing by having the computer connect the points on the display to make a waveform. A higher sampling rate therefore provides a more refined expression of the data. Unfortunately, this comes at the cost of increased file size (more points to store). The assignment of the correct sampling rate is determined by weighing the complexity of the waveform on any given channel against the amount of space required to record the channel. For example, EEG channels (which are inherently more complex than respiratory channels because they vary rapidly) require more definition to be correctly interpreted and are therefore recorded with higher sampling rates, e.g., 100-256 or more samples per second. Respiratory channels are typically recorded with a lower sampling rate (10-50 samples per second) because further sampling of the data may provide no additional usable information. When a signal is sampled, distortion of the data can occur if the sampling rate is too low relative to the “natural” frequencies occurring in the signal (aliasing). For this reason, a good general rule of thumb, based on theoretical considerations, is to set the sampling rate to no less than twice the highest frequency contained in the signal, which is often determined by the value chosen for the high filter setting (Nyquist limit). The following table gives some reasonable settings. Table 3.1 shows some typical recommended filter and sample rate settings for the various types of outputs available from NP airflow transducers. Table 3.1 Recommended Filter Settings and Sampling Rates Pressure Transducer Output Signal Sensitivity Time Constant (Low Filter) High Filter Sampling Frequency Unfiltered Output (Low Level AC) 30µV/mm * (Variable ) 3 – 6 seconds (0.01 - 0.03Hz) 70Hz or higher 140 – 200Hz Unfiltered Output (High Level DC) Varies NA 70Hz or higher 140 – 200Hz Filtered Output (Low Level AC) 30µV/mm (Variable*) 3 – 6 seconds (0.01 - 0.03Hz) 5Hz or higher 10Hz or higher Filtered Output (High Level DC) Varies NA 5Hz or higher 10Hz or higher Snoring Output (Low Level AC) 30µV/mm * (Varies ) 10Hz or lower (>0.016 seconds) 70Hz or higher 140 – 200Hz Snoring Output (High Level DC) Varies NA 70Hz or higher 140 – 200Hz ** ** ** DC Signals are referred to as “high level” signals because the signals are transduced at a higher output voltage than AC signals. A typical DC voltage might be 2V peak to peak while a typical AC signal (“low level”) might be 600µV peak to peak. The specific sensitivity settings may also vary for some transducer systems. * Varies from patient to patient. **Varies from patient to patient and for a specific polygraph. Chapter 4 Extraction of the Snoring Signal from the Pressure Waveform Once properly collected, the raw (unfiltered) pressure waveform from a nasal cannula contains more than just the respiratory airflow. Breathing is a signal represented by the slow changes in pressure. In addition, fast vibrations made during snoring show up on the pressure signal, (Figure 4.1). As a result, by altering the filtering settings, the waveform may be conditioned to display respiration only (Figure 4.2) or snoring only (Figure 4.3). Figure 4.1: The unfiltered pressure waveform. In the above example, you will note both the flattening of the waveform (characteristic of flow reduction) with fast activity (snoring) superimposed on the third and fourth breaths. By adjusting the high frequency filter to 5 - 15Hz, the snoring is removed, leaving a respiratory waveform only. Figure 4.2: The pressure waveform filtered for respiration only. Conversely, if the raw waveform is conditioned by setting a low frequency filter to 10Hz and a high frequency filter to 70Hz or greater, only the snoring is captured. The reliability of the snoring information captured in this fashion has not been rigorously compared to that obtained with a microphone or other snoring sensor. However, it is our impression that this signal is as reliable as these other sensors and has the advantage of a lower background noise. In addition, the nasal cannula is not subject to the application issues associated with those devices (loosened tape, the influence of external physical characteristics of the patient, etc.). Figure 4.3: The pressure waveform filtered for snoring only. Chapter 5 Common Problems Poor Nasal Pressure Flow Signal – Patient Issues. In the example below (Figure 5.1), a loss of amplitude in the NP airflow signal is apparent. The loss of either inspiratory or expiratory flow can occur with poor positioning of the nasal prongs on the cannula (they must be inside the nares to function properly). It is possible to trim the prongs somewhat to improve the comfort of the patient but care must be taken to insure that a sufficient amount of tubing remains to fully capture the signal. A small piece of tape applied to either side of the cannula may insure that the prongs remain well positioned throughout the night. Signal loss may also result from a complete blockage of the cannula tubing due to secretions, but this is rare if the patient does not have clinically evident rhinorhea. Furthermore, the signal amplitude varies from patient to patient. This is inversely related to the size of the patient’s nares. In other words, a large nostril may promote a low amplitude signal and a small nostril may promote a larger signal. Oral breathing may occur– but a complete cessation of nasal breathing is rare during sleep. Recent data suggests that this occurs in only 1 – 2% of the overall recording time.11 Partial oral breathing is more common, but when this occurs cyclical changes in the shape and amplitude of NP flow signal are still indicative of respiratory events albeit that a sensitivity adjustment may be required. Many pressure users utilize an oral thermistor or a nasal-oral cannula to address the issue of oral breathing. Figure 5.1: Poorly positioned cannula. During wakefulness, the respiratory signal may be chaotic and should not be overinterpreted. With practice this can be recognized by the presence of large breaths with irregular frequencies. The tracing below, (Figure 5.2), shows a 2-minute transition from wake to sleep (second half). Note that the irregular amplitudes and frequencies stabilize with the onset of sleep. Figure 5.2: Sleep onset. Poor Nasal Pressure Flow Signal – Technical Factors. The most common problem is an incorrect filter setting when the AC output of the PTAF is used. The AC time constant of the recording device must be longer than 3-5 sec (low frequency filter of 0.05 - 0.01Hz or lower). When the time constant is too short, a square signal (such as the calibration wave) will decay and may cause flow-limited inspirations to appear biphasic, (Figure 5.3). Strictly speaking, the NP airflow signal should be collected as a DC signal when this low frequency filter / time constant requirement cannot be met by the host recorder. Figure 5.3: Signal decay from short time constant. Another commonly made mistake is in establishing the correct polarity of the channel. To determine if the polarity is correct, check to insure that the negative (upward) deflections correspond to inhalation and that the downward deflections correspond to exhalation. In general, when the polarity is correct, amplitude and morphological changes are reflected on the top of the waveforms. That is to say, flattening or rounding of the waveform should be apparent on the tops of the waveforms while the lower part of the waveform should be more characteristically “sharp”, as shown below in Figure 5.4 and Figure 5.5. Figure 5.4: Correctly oriented NP channel. Figure 5.5: Inverted NP signal. Chapter 6 Nasal Pressure Airflow and NCPAP The same analysis of airflow characteristics that is used during diagnostic studies performed with a NP airflow signal (using a cannula) can be applied during the titration of nasal CPAP. Using this information about flow waveforms may improve CPAP titration by identifying sub-optimal pressures through the presence of “flow limitation.” While many laboratory CPAP units possess the ability to export an airflow signal themselves (or an “estimated patient flow” signal in which any constant leak flow is subtracted out of the electronic signal), most of the simple systems used in the home setting do not have this feature. The same hardware that is used to record NP airflow can also be used to monitor airflow during nasal CPAP. This also allows some of the special features of the processed signal to be utilized, e.g., snoring detection. There are several ways to hook up such a system with the CPAP circuit. The specific techniques that can be used depend upon the details of the transducer. In-Line Pneumotach The best technique for measuring a true “flow” signal is to use an in-line pneumotach. This device provides a small in-line resistance in the CPAP tubing. The pressure drop across this resistance is proportional to flow, but pressure must be detected at two sites. See Figure 6.1 for additional detail. Dual Hose Connection A variation on this takes advantage of the natural resistance of the CPAP circuit. Thus, the hose itself becomes a type of “pneumotachograph” and pressure drop from start to finish of the hose is proportional to flow. Again, pressure must be detected at two sites, but no separate pneumotachograph is needed. See Figure 6.2 for additional detail. The Single Hose Mask Connection Pressure can be measured in the CPAP mask directly and assume this is proportional to flow. With this approach, only one pressure needs to be measured. See Figure 6.3 for additional detail. Cannula Under the Mask The last option is to use an unmodified nasal cannula under the CPAP mask. While apparently the simplest solution, this has several disadvantages, which are discussed under Figure 6.4, and we do not generally recommend this approach. See Figure 6.4 for additional detail. In-Line Pneumotach Figure 6.1 The highest fidelity airflow signal is obtained with the use of an in-line pneumotach, the “gold standard” device for measurement of airflow. This technique requires a measurement of the difference between two pressures (above and below the pneumotachograph), thus a dual port transducer. In this configuration of flow monitoring, a pneumotach is placed in the CPAP circuit just below the mask or at the CPAP generator output. The signal that is produced by the drop in pressure in this device is relatively easy to set up and can be used with any CPAP generator. The signal from a pneumotach can be calibrated to actual airflow if one so desires. It thus provides not only respiratory waveforms, but also information about leak flow from the CPAP system. However, this last advantage can be one of the problems with the use of a pneumotach at this location. Since any flow from the CPAP generator will be detected, the airleak between the pneumotach and the patient will also be included in the measured airflow and will create an offset. One solution to this is to use a transducer that has an AC coupled output (or an AC amplifier with a long time constant), which will remove this baseline offset. Dual Hose Connection Figure 6.2 Simply using the CPAP hose in place of the “pneumotach” can produce an airflow signal of high quality, comparable to that from a pneumotach. This circuit involves sampling the pressure at each end of the CPAP tube. Like the in-line pneumotach, it requires the use of a dual port pressure transducer, as the difference between two pressures is the signal sought. This configuration provides an excellent signal, but does require some additional materials and setup time. The materials required would be two in line pressure taps (O2 “Tees” work well) and an additional one-foot length of CPAP circuit. To correctly set up this circuit, place the “Tee” adapters on each end of the 6-8 foot long CPAP tubing. The one-foot extension of tubing (or adapters) should connect the CPAP unit with one of the “Tee” adapters. Although the “Tee” could be attached directly to the CPAP generator, the use of a short extra tube helps to minimize noise transmitted from the generator. The other “Tee” adapter is attached near the mask. The nipple of the “Tee” closest to the CPAP should be connected to the negative ( - ) port of the transducer with small diameter e.g., O2 tubing. The “Tee” closest to the mask should be connected to the positive (+) port. With this circuit, a generally excellent flow signal can be obtained, although no actual pneumotachograph is used. The Single Hose Mask Connection Figure 6.3 Pressure fluctuations in the CPAP mask itself are created by the patient’s inspiratory and expiratory airflow. These pressure fluctuations are superimposed on the CPAP pressure signal and are roughly proportional to this patient’s airflow, provided the pressure at the CPAP generator does not vary much (as is the goal of CPAP). In this circuit configuration, the pressure signal must be processed so only the fluctuations are used to measure airflow. The advantage of the single hose to mask connection is its simplicity. This technique requires no additional cabling by the lab staff and is clearly one of the few possibilities for those who possess a pressure transducer with only one port for tubing. Unfortunately, though, this circuit requires a transducer that measures pressure in the range typical of that of CPAP (as opposed to the other circuits which directly measure the differential pressure between two sites). Pressure fluctuations during breathing (for which the transducers used with the nasal cannula are generally optimized) are in the range of 2cm H2O. While on CPAP, these fluctuations occur on a background of the set CPAP pressure, which may be up to 20cm H2O, and a transducer optimized for the nasal cannula may be incapable of measuring these higher pressures. In addition, flow turbulence in the mask may affect the quality of the signal and signal dampening may occur as CPAP pressures are raised. Turbulence may obscure any derived snore signal by creating an excessively thick baseline. Finally, the assumption that pressure fluctuations in the mask are proportional solely to patient breathing may be incorrect. Specifically, some CPAP generators are deliberately designed to minimize these pressure swings (and may even have a sensor in the mask for pressure feedback). These devices intentionally alter output flow from the CPAP generator in response to mask pressure fluctuations, and may render the single hose signal unusable. Cannula Under the Mask Figure 6.4 This technique is typically employed with a single port transducer. It is easily configured as it is identical to the use of the nasal cannula alone. As with the single hose mask connection, the transducer must be capable of measuring pressures in the CPAP pressure range. The signal obtained may be somewhat more stable than that obtained by simply connecting the pressure transducer directly to the CPAP mask. However, the snoring signal derived may still be contaminated with some background CPAP noise, but less than with the direct mask connection. There may be some signal dampening as well due to the CPAP blower feedback control of pressure, but again less than with a simple mask connection. The major objection to this approach is patient comfort and potential mask leaks. Some patients may find that the cannula and the mask combine to irritate the skin where the cannula passes under the mask. Chapter 7 Scoring Atlas Figure 7.1: Apnea – Apnea is detected as a flat signal on the NP airflow. There is a tendency for small breaths (severe hypopnea) to appear as apnea on the NP airflow signal. Note the minimal fluctuation present on the thermocouple signal despite flat NP airflow signal. Figure 7.2: Hypopnea – Hypopnea is detected as a clearly reduced amplitude of the NP airflow signal. This may be more a more obvious reduction than that seen on the thermocouple signal. Normal inspiration has a sinusoidal appearance on the NP airflow signal. During obstructive hypopnea there is frequently progressive flattening of the inspiratory signal. Snoring may appear simultaneously. Figure 7.3: Flow limitation – Elevated upper airway resistance events are detected when the NP airflow does not show a reduction in amplitude to the level of hypopnea but clearly demonstrates “flattening” (which indicates inspiratory flow limitation). Note that there may be no indication of abnormality on the thermocouple channel. Figure 7.4: Better event definition – Events on the NP airflow signal are often easier to identify than on other respiratory channels and the reduction in amplitude during the event may be more severe. Figure 7.5: Severe flow limitation and apnea – Some apnea events begin as episodes of severe flow reduction and transition to apnea. These events may be scored as hypopnea if only a thermistor is used. Figure 7.6: Sustained flow limitation – The flattened inspiratory airflow contour on the NP airflow signal may occur as a transient event (hypopneas or RERAs) or in sustained runs. These are particularly common during delta sleep and may indicated sustained elevated upper airway resistance without arousal. Sustained flattened inspiratory airflow contour may overlap with “benign” snoring. Figure 7.7: Flow limitation without hypopnea – Patients may experience periods of flow limitation that do not generate neuro-cortical arousal. This is particularly common during slow-wave sleep when the arousal threshold is depressed. In the absence of arousal, these periods probably do not represent clinical disturbance. Figure 7.8: Flow limitation with snoring – Although it is possible that a patient may experience non-disruptive snoring (so called “primary” snoring) most patients that snore do exhibit some degree of sleep fragmentation. The cause of this fragmentation may appear ambiguous when a thermocouple is used for airflow but is often clearly related to respiration when NP airflow is used. Figure 7.9: Flow limitation without snoring – One of the more insidious forms of mild sleep disordered breathing is disruptive flow limitation seen in the absence of snoring. This condition is not easily identified by significant changes in other channels and, as a result, may be under-represented in the lab environment. The absence of snoring may lead a trained technologist to misinterpret a respiratory event as a leg jerk or transient arousal when a thermocouple is used. These events are usually clear when NP airflow is employed. Figure 7.10: Snoring without flow limitation – It is possible for arousals to be associated with cascading snoring and not a characteristically flattened nasal pressure signal. These events occur in the absence of flow limitation, although there is cascading snoring. Such events may be scored as RERA events. Figure 7.11: Variant flow signal during snoring – Fluctuations in the NP airflow signal are occasionally seen while the patient is snoring. It is important to remember that snoring, by definition, represents some degree of airway compromise but in the absence of neuro-cortical arousal should not be scored. Figure 7.12: Cannula and esophageal pressure – The AASM definition of a RERA is based on increasing esophageal pressure prior to arousal. The change in shape on the NP airflow signal is usually present and allows RERAs to be detected non-invasively from the NP airflow signal alone. Chapter 8 Frequently Asked Questions QUESTION 1: Should I use the AC or DC inputs?2, 12 The decision of whether to use the DC or AC inputs is based on a number of factors such as the number of available DC ports or pin inputs on the polygraph headbox, the filtering capability or configuration of your polygraph and the lab design. In general, the DC (high level) ports are preferred as the nasal cannula signal is a slowly varying respiratory signal and AC amplifiers are more suited to rapidly varying signals e.g., EEG. If an AC amplifier is used, a low filter setting of (preferably 0.01Hz) or lower (time constant of 3 seconds or longer) is required in order to correctly record the unfiltered and filtered flow signals. Either DC or AC inputs may be used as long as this filtering requirement can be met. QUESTION 2: What polygraph settings should I use? Pressure Transducer Output Signal Unfiltered Output (Low Level AC) Unfiltered Output (High Level DC) Filtered Output (Low Level AC) Filtered Output (High Level DC) Snoring Output (Low Level AC) Snoring Output (High Level DC) Sensitivity Time Constant (Low Filter) High Filter Sampling Frequency 30µV/mm (Variable*) 3 – 6 seconds (0.01 - 0.03 Hz) 70Hz or higher 140 – 200Hz Varies** NA 70Hz or higher 140 – 200Hz 30µV/mm (Variable*) 3 – 6 seconds (0.01 - 0.03 Hz) 5Hz or higher 10Hz or higher Varies** NA 5Hz or higher 10Hz or higher 30µV/mm (Varies*) 10Hz or lower (>0.016 seconds) 70Hz or higher 140 – 200Hz Varies** NA 70Hz or higher 140 – 200Hz *Varies from patient to patient. **Varies from patient to patient and for a specific polygraph. QUESTION 3: What is a sampling rate? (also referred to as the sampling frequency or digitizing rate) Computers record data as a series of points. The number of points per second to be recorded is the sampling rate. In other words, if a sampling rate of 10Hz is established, 10 equally spaced “samples” of the data are recorded as points, which are then connected by the computer to make a waveform. A higher sampling rate provides a more refined expression of the data, but increases the size of the file to be recorded. The assignment of the correct sampling rate is determined by weighing the complexity of the waveform on any given channel against the amount of space required to record the channel. For example, EEG channels are inherently more complex than respiratory channels and require more definition to be correctly interpreted and are therefore recorded with higher sampling rates. Respiratory channels are typically recorded with a lower sampling rate because further refining the data and increasing the file size provide no additional clinical yield. A general rule of thumb is to set the sampling rate to no less than twice the high frequency filter setting. QUESTION 4: What is the difference between a low frequency filter and a time constant? AC amplifiers are typically calibrated to a DC voltage (usually 50µV). When this voltage is passed through an AC amplifier a calibration signal, such as is shown to the left, is generated. The time required for the deflection to fall back to 37% of its full amplitude is known as the “fall time constant”. The low frequency filter causes this fall back to baseline. There is an inverse relationship between the time constant and the low filter setting. Increasing the low frequency filter will decrease the time constant and vice versa. In general, a low frequency filter attenuates the signals below the assigned frequency. QUESTION 5: What are the advantages of the nasal cannula/pressure transducer over a thermocouple or thermistor?2, 12 Temperature sensing devices (thermocouples and thermistors) have traditionally been used to measure airflow in Polysomnography. These devices, which sense temperature as a surrogate of airflow, are extraordinarily accurate when measuring frank apnea but are quite inaccurate when measuring moderate events such as hypopnea or RERA events. A measure of nasal airflow using a pressure transducer yields a much more accurate representation of the inspiratory flow reduction seen in these events. The nasal cannula pressure system, nearly as simple, uses a simple attachment to the patient (the cannula) and is comparable in cost. QUESTION 6: What about oral breathing?11 It has been estimated that clearly identifiable oral breathing only occurs for 1 – 2% of actual diagnostic recording time (Montserrrat abstract). Complete oral breathing may occur in patients with nasal pathologies, but is readily identifiable. In most cases of oral breathing, sufficient nasal breathing usually remains to allow for a NP reading. If oral breathing is a concern, this issue may be addressed by using a separate measure of the oral airflow, such as an oral thermocouple in combination with a nasal cannula. QUESTION 7: What does normal breathing look like? When measured by a nasal cannula, normal breathing appears as a series of “sinusoidal” inspiratory waveforms of equal deflection as depicted below. Figure 8.1 QUESTION 8: What is flow limitation and what does it look like?2 During inspiration, the collapsibility of the upper airway causes a Starling resistor-like behavior and results in a maximum flow, regardless of increases in effort. The normal “sinusoidal” inspiratory airflow becomes flattened (develops a plateau). The incomplete airway obstruction also causes inspiratory time to increase. Overall, this appears as a flattening of the waveform and is typically seen in breaths of decreased amplitude (Figure 8.2). These events are usually associated with increased respiratory effort and may represent either hypopneas or RERAs. To correctly see this flattening, a time constant setting of 3 – 6 seconds (low frequency filter 0.01 - 0.03Hz) should be established. Figure 8.2 QUESTION 9: What does an apnea look like? By definition, an apnea refers to a period of complete airflow reduction. In actual practice, apneas may be defined as periods of airflow reduction below a certain percentage of a “normal” or baseline breath. During apnea, the NP airflow signal tends to be either perfectly flat or have a lower amplitude than the thermistor. Definitions range from below 10% to 25% and are often subjectively determined. In clinical practice, most sleep centers would score events associated with oxyhemoglobin desaturations (usually 3-4%). A period of repetitive apneas is shown in Figure 8.3. Figure 8.3 QUESTION 10: What does a hypopnea look like? Hypopnea is defined as airflow decreased below a given percentage of the “surrounding baseline” and may also require the presence of some degree of oxyhemoglobin desaturation or arousal. Typically, a flow reduction of 25 – 50% should be seen in order to score an event as a hypopnea. Scoring for both apnea and hypopnea is often subjectively determined, but the event duration should typically be at least 10 seconds. In the scoring of hypopnea one might wish to keep in mind the nature of the relationship between the NP airflow signal and true flow. The nasal cannula actually records the square of airflow. Thus, a NP airflow signal that is 50% of the surrounding baseline is actually 70% of the surrounding flow. A NP airflow signal that is 25% of surrounding flow is actually 50% of the actual airflow. A typical hypopnea is shown in Figure 8.4. Note, in addition to an amplitude reduction there is a marked change in shape with prolongation of inspiratory time. Figure 8.4 QUESTION 11: Can nasal pressure airflow be used to measure increased upper airway resistance (UARS)? Upper airway events (also known as RERA events) are arousals preceded by subclinical respiratory events (events that do not meet the criterion for hypopnea or are not detected with a thermistor at all). Nasal airflow has been shown to be far more reliable than thermal elements in detecting the subtle flow limitation characteristic of these events (Rapoport et al). Figure 8.5 shows a typical event characterized by flow limitation with some reduction in amplitude that coincides with the increased respiratory effort and is followed by arousal. Figure 8.5 QUESTION 12: How is snoring identified with a nasal cannula? Snoring causes small, fast fluctuations in the NP signal. Through the use of a high pass filter (either in the transducer or in the recorder), these fluctuations can be captured and recorded. To do this the signal is filtered through an AC amplifier with a low frequency cut off filter set at about 10Hz and a high pass filter set at 70Hz or above. The morphology of the NP waveform is very similar to that recorded using snoring microphones and vibraphones. An example of this is shown in Figure 8.6. Figure 8.6 QUESTION 13: What is the difference between a “filtered” and “unfiltered” airflow? With an unfiltered flow output, snoring information is displayed along with the flow signal on a single channel. A filtered flow signal uses a low pass filter (such as 5 to 10Hz) to remove the high frequencies such as that of snoring; what remains is the respiratory waveform. This is shown in Figure 8.6 above. It is important not to over filter, e.g., 1Hz low pass filter, the signal as this can remove components present in the signal during flow limitation. QUESTION 14: If I am already using a snore microphone or snore sensor, what benefits are derived from the unfiltered flow signal? An unfiltered flow signal allows snoring and flow to be recorded simultaneously and may be advantageous if you have a limited number of available channels. However, the signal is generally noisier and may be more difficult to interpret than if snoring and airflow are presented on separate channels. QUESTION 15: What if I do not want to use the snore channel? If your transducer has multiple outputs (such as filtered flow, unfiltered flow and snoring) you may use any or all of these based on your personal preference. It is not required that all outputs be recorded. If you have a limited number of available channels, an unfiltered flow signal will combine both snoring with airflow into a single signal. QUESTION 16: Can a nasal pressure airflow system be used with a capnograph? Since both etCO2 and NP are collected via nasal cannula, it would be necessary to use a dual lumen cannula. These are commercially available and used in oxygen saver devices. This also provides a method for measuring nasal airflow while simultaneously administering oxygen. QUESTION 17: Are there validation studies for nasal pressure technology? Numerous papers have been written validating the use of NP airflow for the measurement of airflow. Some useful references are noted in the bibliography. QUESTION 18: Can the nasal pressure airflow signal be calibrated? NP airflow over long periods of time is only a semi-quantitative measure and cannot be readily calibrated to tidal volume. However, as noted by Guyatt,7 calibration is possible for use over short periods though this would not be generally useful for sleep laboratories. In general, the definitions used in identifying respiratory events during sleep involve changes in amplitude relative to the surrounding region rather than absolute cutoffs that would require calibration. QUESTION 19: Can a nasal pressure transducer be used to measure esophageal pressure? In general, the pressure range of most nasal cannula pressure transducers is in the +/- 2 ( or +/- 20) cm H2O range while most esophageal pressure transducers can measure up to 50 cm H2O. Thus, a NP channel is not likely to be able to measure esophageal pressures. QUESTION 20: Can I use any cannula? Any cannula may be used though many manufacturers recommend cannulas designed specifically for use with a NP transducer. Care must be taken to insure that the cannula used does not occupy too large a portion of the cross section of the nares (over 50%) so that it acts as an obstruction to breathing in. Special cannulas, such as the dual lumen cannula mentioned above, are also available. QUESTION 21: Can children be studied using nasal cannula airflow? Pediatric cannulas are available in most respiratory therapy departments. Again, care should be taken with small children to insure that the cannula does not, itself, become an obstruction. QUESTION 22: Do the nasal prongs ever become clogged? It is possible for the nasal prongs to become clogged with secretions although in actual practice the occurrence is rare. In the laboratory this can be readily resolved by cleaning or changing the cannula. A signal can still be processed if one prong is clogged. QUESTION 23: Can the nasal prongs be trimmed if needed? Yes, but it is important to retain some of the prong for a good signal. To function properly the tip of the prongs must be inside the nose (to measure the pressure in the nares, not the pressure outside). QUESTION 24: Do I need to tape the cannula on the patient? Most cannulas are designed for simple but secure attachment to the patient. Whether using a strap around the head or tubes secured around the ears, the nasal cannula does not usually require any additional method to secure it to the patient. QUESTION 25: What methods should be used to connect the nasal pressure transducer to a CPAP unit? There are four possible methods recommended: 1. In-Line Pneumotach 2. Mask Connection 3. CPAP Mask over Cannula 4. Dual Hose Connection The specific methods, advantages and disadvantages of each are discussed in the main section of the primer. (Pages 15-19) QUESTION 26: Why do I get a distorted signal when connecting a tubing between the CPAP mask and a pressure transducer? Turbulence inside the mask and automatic flow adjustments by the CPAP generator (to maintain mask pressure) may distort the waveform. In addition, with some transducers the pressure offset produced by the CPAP may saturate the pressure transducer. See the main portion of the primer for suggestions as to how to overcome this. (Pages 15-19) QUESTION 27: Why do I get a heavy baseline on the snore channel when connected to a CPAP machine? Vibrations caused from the operation of the CPAP device may be detected and displayed as baseline noise. QUESTION 28: How high can the CPAP pressure be adjusted when using a pressure transducer ? This depends on the transducer. A dual port transducer arranged in a dual port configuration (using either a pneumotach or the CPAP hose) is the most stable as the constant pressure offset will be removed by the differential pressure transducer. A single port transducer attached to the mask may be vulnerable to the effects of turbulence or pressure saturation at higher pressures. QUESTION 29: What should I do if I cannot get a flow or snoring signal? 1. Check all transducer to Polygraph connections. 2. Verify proper Polygraph input selections. 3. Confirm Polygraph sensitivity, filter and sampling rate settings. 4. Check for plugged cannula tips. 5. Insure that the cannula is properly positioned on the patient and connected to the pressure transducer unit. 6. Verify that the battery, if present, is functioning. QUESTION 30: Why does the nasal pressure signal differ from the signal generated by a thermocouple or thermistor? The NP airflow signal gives a more accurate depiction of flow. Variability due to snoring or inspiratory flow reduction which are not visible in the thermal signal are readily detected with NP airflow. Long-time users of thermocouples or thermistors may mistake these fluctuations for background “noise”. A heavy baseline may also be picked up from operating CPAP units. QUESTION 31: What can cause a loss of signal strength during a PSG recording? 1. The cannula may have been displaced. 2. There may be material obstructing the nasal prongs. 3. The sensitivity and filter settings may have been inadvertently altered. 4. The battery may be dead, if present. Bibliography 1. Flemons W, Ward, Chair, American Association of Sleep Medicine Task Force (AASMTF) Sleep Related Breathing Disorders in Adults: Recommendations for Syndrome Definition and Measurement Techniques in Clinical Research. Sleep 22:5:667-689, 1999. 2. Ayappa I, Norman RG, Krieger AC, Rosen A, O'Malley RL, Rapoport DM. Non-Invasive Detection of Respiratory Effort-Related Arousals (RERAs) by a Nasal Cannula/Pressure Transducer System. Sleep 23:763-771, 2000. 3. Ballester E, Badia JR, Hernandez L, Farre R, Navajas D, Montserrat JM. Nasal Prongs in the Detection of Sleep-Related Disordered Breathing in the Sleep Apneoea/Hypopnea Syndrome. European Respiratory Journal 11:1128-1134, 1998. 4. Berg S, Haight JS, Yap V, Hoffstein V, Cole P. Comparison of Direct and Indirect Measurements of Respiratory Airflow: Implications for Hypopneas. Sleep 20:60-64, 1997. 5. Clark SA, Wilson CR, Satoh M, Pegelow D, Dempsy JA. Assessment of Inspiratory Flow Limitation Invasively and Non-Invasively During Sleep. Am J Respir Crit Care Med 158:713-722, 1998. 6. Epstein MD, Chicoine SA, Hanumara RC. Detection of Upper Airway Resistance Syndrome using a Nasal Cannula/Pressure Transducer. Chest 117:1073-1077,2000. 7. Guyatt, A.R., S.P. Parker, and M.J. McBride. 1982. Measurement of Human Nasal Ventilation Using an Oxygen Cannula as a Pitot Tube. Am Rev Respir Dis. 126:434-438, 1984. 8. Hernandez L, Ballester E, Farre R, Badia JR, Lobelo R, Navajas D, Montserrat JM. Performance of Nasal Prongs in Sleep Studies. Chest 119:442-450, 2001. 9. Hosselet JJ, Norman RG Ayappa I, Rapoport DM. Detection of Flow Limitation with a Nasal Cannula Pressure Transducer System. AJRCCM 157:1461-1467, 1998. 10. Hosselet J, Ayappa I, Norman RG, Krieger AC, Rapoport DM. Classification of Sleep-Disordered Breathing. Am J Respir Crit Care Med 163:398-405, 2001. 11. Montserrat JM, Farre R, Ballester E, Felez MA, Pasto M, Navajas D. Evaluation of Nasal Prongs for Estimating Nasal Flow. Am J Respir Crit Care Med 155:211-215, 1997. 12. Norman RG, Ahmed MM, Walsleben JA, Rapoport DM. Detection of Respiratory Events During NPSG : Nasal Cannula/Pressure Sensor Versus Thermistor. Sleep 20: 1175-1184, 1997. 13. Series F, Marc I. Nasal Pressure Recording in the Diagnosis of Sleep Apnea Hypopnea Syndrome. Thorax 54:506-510, 1999. Acknowledgements Pro-Tech wishes to thank Marietta Bellamy-Bibbs for her encouragement and editorial comments.