Europace (2013) 15, i26–i31
doi:10.1093/europace/eut116
Automatic remote home monitoring of
implantable cardioverter defibrillator lead and
generator function: a system that tests itself
everyday
Niraj Varma*
Cardiac Pacing and Electrophysiology, Department of Cardiovascular Medicine, Cleveland Clinic (NV), 9500 Euclid Avenue, Cleveland, OH 44195, USA
Received 25 March 2013; accepted after revision 29 March 2013
The implantation of cardiac electronic devices (CIEDs) has increased exponentially over the last decade in response to widening indications. Assessment of post-implant system performance is an important responsibility but challenging in view of increasing volume, device complexity, and
advisory notices. Automatic remote home monitoring (HM) may satisfy these difficult monitoring demands. When tested, HM enhanced the discovery of system issues (even when asymptomatic) and enabled prompt clinical decisions regarding conservative vs. surgical management. This
form of remote monitoring may form a device management model in which near-continuous remote surveillance of CIED performance is combined with automatic self-declaration of system problems, enabling prompt medical decisions. The ability to collect detailed device-specific data,
with component function assessed daily, sets a precedent for longitudinal evaluation of lead and generator performance. These characteristics
have significant ramifications for CIEDs in general and patient safety.
----------------------------------------------------------------------------------------------------------------------------------------------------------Keywords
Defibrillators † Monitoring † Follow-up † Remote monitoring
Introduction
The implantation of cardiac electronic devices (CIEDs) has increased
exponentially over the last decade in response to widening indications. Compromised CIED system (generator/lead) integrity
demands prompt evaluation. Its discovery requires rigorous postimplant monitoring. This is a physician responsibility expressed in
several position statements and consensus recommendations and
now also often demanded by patients.1 – 3 The task is daunting in
view of increasing volume and complexity of implantable devices,
and added burdens imposed by advisory notices. (Fortunately,
current era CIEDs are exceptionally reliable, and component
failure is infrequent. In relative terms, leads represent the weak
link). Conventionally, patients are seen regularly according to calendarbased schedules [e.g. 3 monthly for implantable cardioverter defibrillators (ICDs)/cardiac resynchronization therapies]. However, this
method will miss potentially serious problems occurring between
interrogations, which is when they are most likely to occur.
Remote monitoring of patients with implantable devices promises
resolution of some of these challenges. This rationale underlied
announcements from professional societies for ‘development and
utilization of wireless and remote monitoring technologies’, carrying
the expectation of early detection and correction of device malfunction.1,3 However, ‘early’—especially important in an era of multiple
advisories—remains undefined. Expectations are for as soon as possible, but the capability of remote monitoring to deliver this function
may extend from months to minutes, according to the system
selected.4,5 For example, inductive (wand-based) systems depend
on patient (and hospital) adherence to scheduled follow-ups (e.g. 3
monthly) which is erratic, and continue to fail to disclose asymptomatic interim problems.5 – 7 This is not acceptable as an early warning
system.
Automatic wireless transmission technologies potentially overcome several of these obstacles. Changes in device (or patient) condition can be notified almost immediately.4 This form of advanced
remote monitoring system, pioneered by Biotronik with Home MonitoringTM (HM), effectively provides near-continuous surveillance
without patient participation, enabling both detection of asymptomatic events and cataloguing performance history on remote servers.
Diagnostic ability may be aided by automatically wirelessly transmitted electrograms (e.g. Figure 1). Daily transmissions generate highresolution parameter trending and enable assessment of changes
* Corresponding author. Tel: +1 216 444 2142; fax +1 216 445 6161, Email: varman@ccf.org
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2013. For permissions please email: journals.permissions@oup.com.
Home monitoring of ICD system function
i27
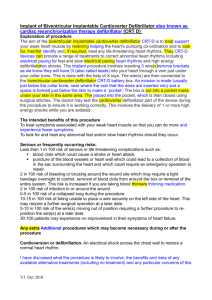
Figure 1 (Left) Event notifications suggestive of AF (top) but accompanying wirelessly transmitted intracardiac electrograms indicate that the abnormality was caused by lead noise, likely due to fracture. Lead impedance trend (not shown) was normal. The automatically transmitted accompanying electrogram of the event was very useful, permitting the diagnosis of a false-positive mode switch in this case. (Right) Non-physiological
signals due to electromagnetic interference. Event notification received for an aborted shock detected at 7:16 pm. The accompanying automatic
wirelessly transmitted electrogram shows gross artefact on both atrial and ventricular leads. The subject was asymptomatic but in response to
the notification was seen in-office within 24 h. (Compiled with permission from Varma et al.13)
that are significant. For example, with a sudden change in lead impedance of an ICD lead under Class 1 recall, absolute value remained
within specifications, but deviation from historical trend triggered
event notification (Figure 2). The combination of two or more parameter deviations, as illustrated, may improve specificity of the alert, e.g.
linking of non-sustained ventricular tachycardia (VT) events to an impedance deviation improved detection of lead failure.8 These processes, individualized in each patient, improve the value of alerts
received.
This automatic daily surveillance technology which self-declares
significant problems as and when they occur, even when the
patient is unaware of them, has obvious application to monitoring
CIED function. Several short reports support this. For example,
failure of an ICD to properly charge its capacitors and deliver appropriate therapy,9 inappropriate VT detection caused by supraventricular tachycardia, and intermittent T-wave oversensing were all
diagnosed by remote alert transmissions intracardiac electrogram
and managed by urgent non-routine follow-ups. In another assessment of lead failure (n ¼ 54 patients), 80% of patients were asymptomatic at first episode of oversensing, and symptomatic problems
were reduced with those managed with HM (27.3%) vs. without
(53.4%, P ¼ 0.04). Events were notified 54 days after the last ICD interrogation and 56 days before next scheduled visit, i.e. reaction time
was advanced by almost 2 months to avoid adverse events.10
The utility of remote device management illustrated by these
earlier reports was confirmed prospectively in the randomized
TRUST trial, which tested the hypothesis that HM would be superior
to conventional care for surveillance of system integrity and function,
and that device initiated event notifications would enable early detection of ICD dysfunction as called for in societies’ statements.11 Since
HM had demonstrated high fidelity transmission with virtually immediate notification ability in pilot studies,4 TRUST also tested whether
early detection could be achieved the ‘same day’ in real-world practice. The results were revealing. Although the number of patients
developing problems were equal in both study arms, expected in a
large well-randomized trial, the number of detections of ICD
system dysfunction were greater with HM. Conventional monitoring
grossly under-reported occurrence of ICD dysfunction, and this loss
progressively enlarged with time (Figure 3). Notably, 47% of all
detected events were asymptomatic—such clinically silent events
would have remained undiscovered with conventional care until
next in-person evaluation, possibly several months distant to time
of occurrence. The capacity for early detection with HM was examined in detail. The majority (51%) of events were detected the same
day, even when asymptomatic. Lapses (i.e. discovery .24 h) likely
resulted from delays by handling facilities, i.e. although remote monitoring provides a considerable advance over conventional in-person
evaluations, early reaction ability nevertheless demands consistent
i28
N. Varma
Figure 2 Implantable cardioverter defibrillator generator with automatic wireless remote monitoring coupled to a Fidelis (MDT 6949) lead. Two
event notifications that were transmitted immediately on occurrence of lead fracture, occurring silently during sleep at 4:43 am, 6 weeks after last
clinic follow-up on November 14. Left: Two occurrences of detection in VF zone are noted (top) and flagged (red exclamation mark on yellow background). The accompanying wirelessly transmitted electrogram demonstrated irregular sensed events (markers indicate coupling intervals as short
as 78 ms) with VF detection (marked). No therapy was delivered indicating spontaneous event termination. Right: The second event report is a separate notification in response to the same event indicating a lead impedance alert. Lead impedance trend had been stable below 600 V in prior weeks,
but then suddenly increased .500 V triggering an event notification (red dot) although this absolute value was still within specifications. Electrogram
definition was modest in first-generation device with wireless intracardiac electrogram transmission (Lumos). Current generation devices transmit
electrograms with improved resolution (1/128 s) and longer duration including post-detection sequences (e.g. Figure 1). (Compiled with permission
from Varma39.) The clinic received these notices and informed the patient who was then reviewed urgently within 24 h and treated with lead extraction and replacement. The case demonstrates the value of remote monitoring with daily automatic surveillance and rapid, automatic (i.e. without
patient participation) event notification to the clinic of fault detection which enabled prompt intervention. Without automatic wireless remote monitoring, presentation may have occurred later with inappropriate shocks or catastrophically with failure of pacing or VF sensing.
clinic workflow routine. Indeed, device clinic oversight (and not
transmission breakdown) was the major cause of lapses of remote
follow-up in TRUST. This is important, since event triggers cover
an extensive range of potentially lethal system problems (e.g. elective
replacement indicator (ERI), lead fracture, high-voltage circuitry
failure12), especially since almost one-half of these were clinically
silent. Any delay in reaction is undesirable and potentially hazardous
(Figure 4).
The clinical merits of early detection with automatic remote HM
for patient and device care are significant. These included prompt decision making and intervention, e.g. surgically for lead failure, or conservatively with reprogramming to prevent potential inappropriate
therapies (Figures 1 and 2).13 Reprogramming changes accounted
for the majority of ‘actionable’ interrogations in the TRUST trial.14
This is important since programming may directly affect mortality.15
Hence, early notification of a need to optimize programming in any
particular patient (which is likely to change during device lifetime)
may be beneficial. The non-sustained ventricular arrhythmia notification may be triggered by system issues such as lead electrical noise
artefacts caused by fracture or non-physiological electrical signals,
and direct intervention to pre-empt shock delivery and reduce
patient morbidity.13,16 Interruption of repeated charge cycles
which occur in a significant minority of ICD patients is important to
prevent early battery exhaustion.17 In the multicentre ECOST trial,
clinical reactions enabled by early detection resulted in a large
reduction in the number of actually delivered shocks (272%), the
number of charged shocks (276%), the rate of inappropriate
shocks (252%), and at the same time exerting a favourable impact
on battery longevity.18 These advantages are especially apparent in
those in whom conventional follow-up is challenging, e.g. children.19
Advisories
Automatic remote monitoring may facilitate management of advisories (Figure 2). These largely encompass disintegration of highvoltage circuitry, battery depletion, and lead failure, which are captured by currently evaluated event triggers.20,21 Intensifying surveillance with conventional detection methods, such as increasing the
frequency of office visits, e.g. monthly22 are impractical, onerous,
and inefficient since problem incidence is low and this schedule is
likely to miss dangerous interim problems. Patient alert mechanism
such as beeps, are insensitive and prone to false-positive evaluations.23,24 In contrast, HM generators trigger immediate alerts on deviation from established trends. This reduces burden both for
patients to monitor their own devices frequently and for clinics responsible for large populations with a low incidence of typically
silent problems. Identification of the small number of affected
devices may permit elective replacement of these few and avoid unnecessary large-scale elective replacement. Continuous monitoring
may aid balanced management decisions since a similar malfunction
may confer different risks in different patients. For example,
Home monitoring of ICD system function
i29
Figure 3 Event-free survival rates in HM compared with conventional care in the TRUST cohort. Protocol required event notifications were
system related (end of service, ERI, atrial impedance ,250 or .1500 V, ventricular impedance ,250 or .1500 V, daily shock impedance
,30 or .100 V, shock impedance ,25 or .110 V); arrhythmia-related events (atrial burden .10%, SVT detected, VT1 detected, VT2 detected,
VF detected), and ineffective ventricular maximum energy shock (notified on first shock of any sequence in a given episode). (Compiled with permission
from Varma et al.13)
immediate replacement of a lead under advisory may be unnecessary
in patients who are not pacemaker-dependent. Hence, remote management has the potential to diminish morbidity/mortality, and
reduce associated hospital admissions with significant implications
for cost reduction. This ability may depend on the type of problem.
For example, one-third of patients with Fidelis lead failure receive inappropriate shocks within 3 h, the time between the occurrence of
event and patient morbidity. This may be too short to permit intervention.23 The warning may be advanced by integrating automated
safety surveillance systems into remote monitoring databases.25
Future technology may incorporate an ability to adjust programming
to respond to failures detected during monitoring. Other significant
lead problems may occur without deviation of any electrical parameters.26
Databasing
Automatic warehousing of performance data retrieved daily from
large and complete patient cohorts (without errors associated with
manual data entry) permits long-term longitudinal evaluation of
system survival. This provides not only a mechanism to rapidly identify individuals who develop out-of-bounds values, but also an opportunity to define standards of performance for device components
and function.27,28 In comparison, other available techniques have significant limitations. For example, device function has been determined during sporadic conventional in-person follow-up and
symptomatic patient presentation, or analysis of voluntary return
of products which is vulnerable to reporting bias.29 These lend to inconsistent results. For example, 5-year lead malfunction rates varied
sharply from 2.5 to 15% in different studies.30,31 Even when a single
Figure 4 Days to detection of ICD problems in patients assigned
to remote HM. Overall, 22 of 43 (51%) were detected within 24 h.
(Compiled with permission from Varma et al.40)
component is being tracked (e.g. the Fidelis lead32) there is variation
in incidence of failure among different reports. Definitions of failure
themselves are inconsistent. In one study,30 problems were discovered during routine face-to-face follow-up and reprogramming
changes without surgical intervention were included in the ‘failure’
rate. In contrast, in another study 76% of lead malfunction came to
clinical attention because of inappropriate ICD therapies and the
i30
need for surgical revision defined failure.31 Both reports may underestimate the true incidence of lead failure if malfunctions are asymptomatic, occur intermittently, or result in death (only a minority of
devices are interrogated post-mortem). Hence, non-compulsory
follow-up methods generate inaccuracies and may undermine the important task of ICD component surveillance and assessment of reliability. In contrast, continuous remote monitoring, as currently
described, represents a more comprehensive evaluation mechanism,
working independently of symptoms or follow-up schedule, and permitting application of uniform definitions for out-of-range behaviour.
There are limitations. It is important to note that HM does not supplant the first post-implant in-person evaluation,33 important for assessment of wound healing, determination of chronic thresholds, and
setting of final pacing parameters. Problems such as lead perforations
or failures requiring revision and symptomatic reactions to implantation
(e.g. pacemaker syndrome, diaphragmatic pacing, and pocket infection)
cluster in this early post-implant. They occur more frequently with dualchamber or resynchronization units.34 – 36 However, subsequent to this
mandatory initial in-person evaluation, HM surveillance was demonstrated to be superior to regular office checks in the TRUST study.
These results described with HM, which has excellent transmission reliability37 may not be extrapolated readily to all proprietary technologies. Thus, in the CONNECT trial, which was structured similarly to
TRUST but used a different remote wireless technology, a large proportion of attempted transmissions simply failed.38 When alert transmissions for some conditions were successful, manual reset was
required to reactivate this notification ability, i.e. the ability for further
notification in the interim was lost until an otherwise unnecessary
in-person encounter could be arranged. This design, depending on
patient interaction and single transmissions vulnerable to failure,
limits its role as an early warning mechanism.
In summary, recent results indicate that HM is a stringent method
of post-implant ICD evaluation in which system components are
tested, reported, and databased daily. Warehousing of collected
data in his fashion will permit characterization of device behaviour,
determination of reliability, and definitions of abnormality. Certain
points require emphasis. The technology is automatic and maintains
high-intensity vigilance without the need for patient interaction, and
pre-specified ‘out-of-bounds’ conditions are flagged for attention,
enabling same day discovery (irrespective of follow-up schedule).
Asymptomatic issues are covered equally well. With regards to the
denominator, the very high reliability of implanted systems is to be
appreciated since dysfunction is infrequent, but this makes the task
of identifying these few especially challenging. However, remote
monitoring as described, directs virtually immediate attention to
patients developing problems, as and when they occur, thus effectively finding the proverbial needle in the haystack, a task beyond conventional means. In practice, this ability may be influenced by engineering
differences, transmission frequency, methods of alert notification,
and handling by receiving facilities.
In conclusion, automatic continuous remote monitoring represents an early warning system which can provide assurance to both
patients and their physicians.
Conflict of interest: N.V.: Modest—Biotronik, Boston Scientific,
Medtronic, St Jude Medical. Chair and PI of the TRUST trial;
member ALTITUDE Steering Committee.
N. Varma
References
1. Carlson MD, Wilkoff BL, Maisel WH, Carlson MD, Ellenbogen KA, Saxon LA et al.
Recommendations from the Heart Rhythm Society Task Force on Device Performance Policies and Guidelines Endorsed by the American College of Cardiology Foundation (ACCF) and the American Heart Association (AHA) and the International
Coalition of Pacing and Electrophysiology Organizations (COPE). Heart Rhythm
2006;3:1250 –73.
2. Wilkoff BL, Auricchio A, Brugada J, Cowie M, Ellenbogen KA, Gillis AM et al. HRS/
EHRA Expert Consensus on the monitoring of cardiovascular implantable electronic devices (CIEDs): description of techniques, indications, personnel, frequency and
ethical considerations: developed in partnership with the Heart Rhythm Society
(HRS) and the European Heart Rhythm Association (EHRA); and in collaboration
with the American College of Cardiology (ACC), the American Heart Association
(AHA), the European Society of Cardiology (ESC), the Heart Failure Association
of ESC (HFA), and the Heart Failure Society of America (HFSA). Endorsed by the
Heart Rhythm Society, the European Heart Rhythm Association (a registered
branch of the ESC), the American College of Cardiology, the American Heart Association. Europace 2008;10:707 –25.
3. Maisel WH, Hauser RG, Hammill SC, Hauser RG, Ellenbogen KA, Epstein AE et al.
Recommendations from the Heart Rhythm Society Task Force on lead performance
policies and guidelines: developed in collaboration with the American College of
Cardiology (ACC) and the American Heart Association (AHA). Heart Rhythm
2009;6:869 –85.
4. Varma N, Stambler B, Chun S. Detection of atrial fibrillation by implanted devices
with wireless data transmission capability. Pacing Clin Electrophysiol 2005;28(Suppl
1):S133 –6.
5. Crossley GH, Chen J, Choucair W, Cohen TJ, Gohn DC, Johnson WB et al. Clinical
benefits of remote versus transtelephonic monitoring of implanted pacemakers. J Am
Coll Cardiol 2009;54:2012 –9.
6. Schoenfeld MH, Compton SJ, Mead RH, Weiss DN, Sherfesee L, Englund J et al.
Remote monitoring of implantable cardioverter defibrillators: a prospective analysis.
Pacing Clin Electrophysiol 2004;27:757 –63.
7. Joseph GK, Wilkoff BL, Dresing T, Burkhardt J, Khaykin Y. Remote interrogation and
monitoring of implantable cardioverter defibrillators. J Interv Card Electrophysiol 2004;
11:161 – 6.
8. Swerdlow CD, Gunderson BD, Ousdigian KT, Abeyratne A, Sachanandani H,
Ellenbogen KA. Downloadable software algorithm reduces inappropriate shocks
caused by implantable cardioverter-defibrillator lead fractures: a prospective
study. Circulation 2010;122:1449 –55.
9. Neuzil P, Taborsky M, Holy F, Wallbrueck K. Early automatic remote detection of
combined lead insulation defect and ICD damage. Europace 2008;10:556–7.
10. Spencker S, Coban N, Koch L, Schirdewan A, Muller D. Potential role of home monitoring to reduce inappropriate shocks in implantable cardioverter-defibrillator
patients due to lead failure. Europace 2009;11:483–8.
11. Varma N. Rationale and design of a prospective study of the efficacy of a remote
monitoring system used in implantable cardioverter defibrillator follow-up: the
Lumos-T Reduces Routine Office Device Follow-Up Study (TRUST) study. Am
Heart J 2007;154:1029 –34.
12. Hauser RG, Kallinen L. Deaths associated with implantable cardioverter defibrillator
failure and deactivation reported in the United States Food and Drug Administration
Manufacturer and User Facility Device Experience Database. Heart Rhythm 2004;1:
399 –405.
13. Varma N, Michalski J, Epstein AE, Schweikert R. Automatic remote monitoring of
implantable cardioverter-defibrillator lead and generator performance: the
Lumos-T Safely RedUceS RouTine Office Device Follow-Up (TRUST) trial. Circ
Arrhythm Electrophysiol 2010;3:428 – 36.
14. Varma N, Epstein A, Irimpen A, Schweikert R, Shah J, Love CJ, Investigators T. Efficacy
and safety of automatic remote monitoring for ICD follow-up: the TRUST trial. Circulation 2010;122:325 –32.
15. Moss AJ, Schuger C, Beck CA, Brown MW, Cannom DS, Daubert JP et al. Reduction
in inappropriate therapy and mortality through ICD programming. N Engl J Med
2012;367:2275 –83.
16. Mabo P, Defaye P, Sadoul N, Davy J, Deharo J, Kacet S. Remote follow-up of patients
implanted with an ICD. The prospective randomized EVATEL study. 2011. http://spo.
escardio.org/eslides/view.aspx?eevtid=48&fp=2173
17. Varma N, Johnson MA. Prevalence of cancelled shock therapy and relationship to
shock delivery in recipients of implantable cardioverter-defibrillators assessed by
remote monitoring. Pacing Clin Electrophysiol 2009;32(Suppl 1):S42 –6.
18. Guedon-Moreau L, Lacroix D, Sadoul N, Clementy J, Kouakam C, Hermida JS et al. A
randomized study of remote follow-up of implantable cardioverter defibrillators:
safety and efficacy report of the ECOST trial. Eur Heart J 2012;15(Suppl 1):i17 –i25.
19. de Asmundis C, Ricciardi D, Namdar M, Chierchia G-B, Sarkozy A, Brugada P. Role of
home monitoring in children with implantable cardioverter defibrillators for
Brugada syndrome. Europace 2013;15(Suppl. 1):i17 –i25.
Home monitoring of ICD system function
20. Maisel WH, Sweeney MO, Stevenson WG, Ellison KE, Epstein LM. Recalls and safety
alerts involving pacemakers and implantable cardioverter-defibrillator generators.
JAMA 2001;286:793 –9.
21. Maisel WH, Stevenson WG, Epstein LM. Changing trends in pacemaker and implantable cardioverter defibrillator generator advisories. Pacing Clin Electrophysiol 2002;
25:1670 –8.
22. Medtronic. Physician Advisory Letter: Urgent Medical Device Information. 2007.
Sprint Fidelisw Lead Patient Management Recommendations. http://www.
medtronic.com/product-advisories/physician/sprint-fidelis/
PROD-ADV-PHYS-OCT.htm
23. Kallinen LM, Hauser RG, Lee KW, Almquist AK, Katsiyiannis WT, Tang CY et al.
Failure of impedance monitoring to prevent adverse clinical events caused by fracture of a recalled high-voltage implantable cardioverter-defibrillator lead. Heart
Rhythm 2008;5:775–9.
24. Swerdlow CD, Gunderson BD, Ousdigian KT, Abeyratne A, Stadler RW, Gillberg JM
et al. Downloadable algorithm to reduce inappropriate shocks caused by fractures of
implantable cardioverter-defibrillator leads. Circulation 2008;118:2122 –9.
25. Hauser RG, Mugglin AS, Friedman PA, Kramer DB, Kallinen L, McGriff D et al. Early
detection of an underperforming implantable cardiovascular device using an automated safety surveillance tool. Circ Cardiovasc Qual Outcomes 2012;5:189–96.
26. Abdelhadi RH, Saba SF, Ellis CR, Mason PK, Kramer DB, Friedman PA et al. Independent multicenter study of Riata and Riata ST implantable cardioverter-defibrillator
leads. Heart Rhythm 2013;10:361 –5.
27. Powell BD, Asirvatham SJ, Perschbacher DL, Jones PW, Cha YM, Cesario DA et al.
Noise, artifact, and oversensing related inappropriate ICD shock evaluation: ALTITUDE noise study. Pacing Clin Electrophysiol 2012;35:863 –9.
28. Gilliam FR, Hayes DL, Boehmer JP, Day J, Heidenreich PA, Seth M et al. Real world
evaluation of dual-zone ICD and CRT-D programming compared to single-zone
programming: the ALTITUDE REDUCES study. J Cardiovasc Electrophysiol 2011;22:
1023– 9.
29. Hauser RG, Hayes DL, Epstein AE, Cannom DS, Vlay SC, Song SL et al. Multicenter
experience with failed and recalled implantable cardioverter-defibrillator pulse generators. Heart Rhythm 2006;3:640 – 4.
i31
30. Kleemann T, Becker T, Doenges K, Vater M, Senges J, Schneider S et al. Annual rate of
transvenous defibrillation lead defects in implantable cardioverter-defibrillators
over a period of .10 years. Circulation 2007;115:2474 –80.
31. Eckstein J, Koller MT, Zabel M, Kalusche D, Schaer BA, Osswald S et al. Necessity for
surgical revision of defibrillator leads implanted long-term: causes and management.
Circulation 2008;117:2727 –33.
32. Hauser RG, Hayes DL. Increasing hazard of Sprint Fidelis implantable cardioverterdefibrillator lead failure. Heart Rhythm 2009;6:605–10.
33. Wilkoff BL, Auricchio A, Brugada J, Cowie M, Ellenbogen KA, Gillis AM et al. HRS/
EHRA expert consensus on the monitoring of cardiovascular implantable electronic
devices (CIEDs): description of techniques, indications, personnel, frequency and
ethical considerations. Heart Rhythm 2008;5:907 –25.
34. Brugada P. What evidence do we have to replace in-hospital implantable cardioverter defibrillator follow-up? Clin Res Cardiol 2006;95(Suppl 3):III3 –9.
35. Senges-Becker JC, Klostermann M, Becker R, Bauer A, Siegler KE, Katus HA et al.
What is the ‘optimal’ follow-up schedule for ICD patients? Europace 2005;7:319 –26.
36. Lee DS, Krahn AD, Healey JS, Birnie D, Crystal E, Dorian P et al. Evaluation of early
complications related to de novo cardioverter defibrillator implantation insights
from the Ontario ICD database. J Am Coll Cardiol 2010;55:774–82.
37. Varma N, Michalski J, Investigators T. Effect of transmission reliability on remote
follow-up in ICD patients: automatic home monitoring in the TRUST trial. Heart
Rhythm 2012;9:S1 –S564 (Abstract).
38. Crossley G, Boyle A, Vitense H, Chang Y, Mead RH. The clinical evaluation of remote
notification to reduce time to clinical decision (CONNECT) trial: the value of wireless remote monitoring with automatic clinician alerts. J Am Coll Cardiol 2011;57:
1181 –9.
39. Varma N. Remote monitoring for advisories: automatic early detection of silent lead
failure. Pacing Clin Electrophysiol 2009;32:525 –7.
40. Varma N, Pavri BB, Stambler B, Michalski J, Investigators T. Same-day discovery
of implantable cardioverter defibrillator dysfunction in the TRUST remote
monitoring trial: influence of contrasting messaging systems. Europace 2013;15:
697 –703.