Disownership of left hand and objects related to it in a
advertisement

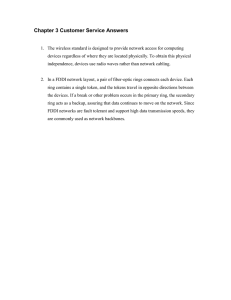
Cognitive Neuroscience and Neuropsychology 1 11 NeuroReport 8, 293–296 (1996) WE describe a woman with right brain damage who denied the ownership of her left hand and of extracorporeal objects (e.g. rings) which were worn on the left hand itself. When the same objects were worn on the right hand or were held by the examiner, the patient correctly recognized them as her own. Other personal objects unrelated to the left hand (e.g. pins, earrings, comb) were always correctly recognized as her own. Thus, by inference, the mental image of one’s body may include inanimate objects which had been in contact or in close proximity with the body itself. These findings provide, for the first time, experimental support to the speculative notion of an extended body schema. Key words: Anosognosia; Extended body schema; Right brain damage; Somatoparaphrenia Introduction 11 11 1p Salvatore Aglioti,CA Nicola Smania,1 Michela Manfredi2 and Giovanni Berlucchi Dipartimento di Scienze Neurologiche e della Visione, Sezione Fisiologia Umana, Strada Le Grazie 8, I-37134, Verona; 1Servizio Recupero e Rieducazione Funzionale, Policlinico Borgo Roma, Verona; 2Dipartimento di Scienze Neurologiche e della Visione, Sezione Neurologia, Verona, Italy 11 11 Disownership of left hand and objects related to it in a patient with right brain damage Neurological and psychological evidence suggests that the spatial representations for mapping the body and extracorporeal objects are largely independent from one another.1–5 The construction and maintenance of a body image rely upon the interaction among visual, labyrinthine, proprioceptive, tactile and visceral inputs as well as between these inputs and the mental representation that one has of one’s own body.4,6 Self-awareness and the conscious self–non-self distinction are related in various and complicated ways to bodily sensations. According to James,7 the nucleus of the ‘me’ is always the bodily existence felt to be present at the time; however, this feeling may include non-corporeal items that are perceived in association with the body, such as clothes or other material belongings. James also pointed out that it is difficult, if not impossible, to draw a precise and permanent boundary between what a person calls ‘me’ and what he or she calls ‘mine’, a statement which applies to paraphernalia and bodily parts alike. Thus, at least theoretically, the mental image of one’s body may include objects that had been in contact or in close proximity with the body itself. This body image can be regarded as an extended body schema. For example, a probe may become, at least temporarily, part of the body image of a surgeon as well as a stick may be part of the body schema of a blind man.8 In line with this © Rapid Science Publishers CA Corresponding Author hypothesis is the anecdotal evidence from amputee patients who report the sensation of a tight ring on their phantom hand.4,9 Although hypotheses about an extended body schema have been formulated since the last century, the present study is the first to provide experimental evidence supporting such hypotheses. Materials and Methods C.B., a 73-year-old, right handed, housewife with 5 years of schooling suffered a right hemisphere stroke on November 4, 1995 (Fig. 1). On admission, she presented with motor and sensory deficits to her left hemisoma. Left extrapersonal and personal neglect with strong denial of ownership of the left hand was observed. According to her son, soon after the stroke his mother asked him to remind doctors to take away the hand that they had left in her bed. When first seen by us, 4 days after the stroke, the patient appeared well orientated as to time and place. She was able to remember her telephone number and perform within normal limits in a short-term memory digit span test. C.B. showed a striking anosognosia10–12 for her left-side sensorimotor defects. She denied having any problem with her left hemisoma but complained about an aching right hip-joint which had been operated several years before. Like other patients with large lesions to the right side of the brain13,14 C.B. resolutely denied the ownership of her Vol 8 No 20 December 293 S. Aglioti et al 111 Table 1. Description of the objects used in the experimental sessions. The possible effect of dimension, weight and material of the objects was taken into account. The golden pin, for example, shared all the above features with the rings. The key-ring was put on the fourth finger in a ring-like fashion with the aim of examining the effect of a relationship with the left hand as close as possible to that of the rings. Object 0111 Belonging Related to to patient disowned body part Ring with diamonds/garnet Gold ring with an R Watch with brown strap Small gold pin Earrings Blue comb Holy icon (Santa Rita) Holy icon (Mother Mary) Knife with a white handle Clock Ring with a lapis lazuli Ring with a diamond Watch with a black strap Brown comb Brush Key ring (with key) Scissors Padlock 0111 Y Y Y Y Y Y Y Y Y Y N N N N N N N N Y Y Y N N N N N N N Y Y Y N N N N N Category 1 1 1 2 2 2 2 2 2 2 3 3 3 4 4 4 4 4 FIG. 1. CT transverse cuts, taken 6 days after the stroke, show a large area of cortical and subcortical infarction. The white progressive numbers on the left lower corner of each cut indicate a caudal to rostral progression. 0111 0111 0111 111p left hand and insisted that it had been left in her bed by the doctors. On verbal command, she could touch her left ear, eye, shoulder, elbow, and knee, but only with great effort could she touch her left hand. Moreover, after touching the hand she typically stated that it was not her own. The ownership of other body parts was correctly acknowledged. Her knowledge about prototypical human figures was preserved because she had no problems in reporting that human bodies typically consist of one head, one trunk, two eyes, two ears, one nose, two hands, two arms, two legs, two feet. When we first saw the patient, she wore two rings on her left ring finger, namely her wedding ring and a ring with two lateral, small diamonds and one central big garnet. She also wore on her right fourth finger a large golden ring with an R on its plate surface. C.B. not only denied the ownership of her left hand, but she also denied ever having seen the rings worn on her left hand; by contrast, she recognized the ring on her right hand and reported many details about it (e.g. ‘this ring was made from a necklace, about 10 years ago’). We took the wedding ring away and moved the garnet ring from the left to the right hand. Surprising as it may seem, now the patient was not only able to recognize the ring as her own, 294 Vol 8 No 1 20 December 1996 but was also able to retrieve much autobiographical information related to it (e.g. ‘I remember quite clearly that this ring had been given to me by my late husband’). A few seconds later we replaced the garnet ring on the disowned left hand and asked C.B. to describe the ring and report its owner. The patient described the ring adequately and also admitted that it looked similar to the one which was on her right hand one minute before; however, she appeared genuinely convinced that both the hand and the ring belonged to the doctor. Moreover, the gold ring (which was correctly recognized as her own when worn on the right hand), was no longer labelled as her own when put on the disowned left hand. Both the rings were correctly recognized as her own when held by the examiner in front of her. To assess the phenomenon systematically, we used objects with combinations of the two attributes relevant to the task, namely ownership and perceptuorepresentational relationships with the disowned body part (Table 1). C.B. was tested in three experimental sessions, 4, 5, and 6 days after the stroke. Each session, lasting about 2 h, began with specific questions about the ownership of different body segments. On each experimental trial, one object was put in the right or Body image and brain damage 1 the left hand. The patient’s left hand was positioned in the right space or along the bodily midline by the examiner. All testing sessions were videorecorded and results were scored with the help of the film sequences. Results 11 11 11 11 11 1p A standard neurological examination revealed a left somatosensory deficit, mild for the lower limb and severe for the upper limb. There was a left hemianopia on a confrontation test. The patient showed perfect recognition of objects by active and passive touch with the right hand. Because of her sensorimotor deficits she was unable to manipulate objects with the left hand. In a condition of passive tactile exploration where the left hand was guided by the examiner, the patient was unable to recognize any objects. Visual recognition of objects or familiar faces was perfect. Extreme left hemispatial neglect was evident from line- and letter cancellation tasks and from a task of copying complex line drawings. Moreover, C.B. showed a marked head deviation towards the right hemispace and her eyes were magnetically captured by visual stimuli presented in the right hemispace. In spite of this rightward bias the patient could be instructed to align her head and eyes with the bodily midline. Paradoxical visual extinction15 was assessed by presenting two simultaneous stimuli, at about 10 and 20° to the right of a central fixation point. In spite of its retinal advantage, the 10° stimulus went unnoticed. Detection of tactile stimuli was assessed by delivering to the dorsum of each hand (lying in its homonymous hemispace) a sequence of unilateral or bilateral light touches.16 All left side stimuli in the bilateral stimulation condition were extinguished and only two of five left unilateral stimuli were detected, suggesting a severe somatosensory deficit. However, positioning the left hand in the right space was accompanied by a dramatic improvement in left hand accuracy under both unilateral and bilateral conditions, confirming that apparent somatosensory deficits may be caused by neglect.17 It is remarkable that when the left hand was in its heteronymous hemispace C.B. reported feeling stimuli on a hand that, in her opinion, did not belong to her. All objects were named and described correctly, but there was a selective impairment in attributing ownership of objects related to the disowned left hand (Table 2). On the first two testing sessions C.B. obstinately refused to admit that her left hand belonged to her. Instead, she maintained that the hand belonged to the examiner. On the third testing session the delusional symptom had partially faded. When, at the beginning of the session, the examiner touched C.B.’s left hand and inquired about the ownership of the hand she hesitated before saying that it was not her hand. Moreover, in three of four correct trials with objects in category 1, the patient recognized the hand as her own. Seventeen days after the stroke, in a testing session where the disowning phenomenon had completely cleared up, C.B. attribution of ownership to objects from all categories was fully veridical. Discussion In classical neurology, after Head and Holmes’18 humorous suggestion that the feather in the hat of an Edwardian woman could become part of her body schema, it has been widely held that the mental image of a person’s body may extend to inanimate objects which are in contact with or in close proximity to the body itself.8,18 James7 speculated that extrapersonal objects systematically associated with the body can be represented in memory either as ‘mine’ or as ‘me’, depending on whether they are considered in isolation or in conjunction with the associated body part. The representation of a body part would thus include a representation of the paraphernalia constantly associated with that part in the subjects’ past experience. Although this concept of an extended body schema has an intuitive appeal, so far no factual evidence has been provided in support of these speculations. In patient C.B., a lesion affecting the anatomical substrate of the physical self19 induced a resolute disownership of her paralytic left hand, which was attributed to other individuals. This pathological distortion of the body schema also seems to have affected the mental representation of extracorporeal objects that, in the patient’s previous experience, were systematically associated with parts of her own body. C.B. denied the ownership of her rings only when they were viewed on her left hand. Furthermore, the patient’s incorrect denial of ownership did not extend to other personal belongings not systematically associated with the disowned hand, even though they Table 2. Number of the hits out of the total number of trials in each experimental session for each category of objects. Hand Left Right Object category 1 2 3 4 1 2 3 4 Date of testing 8/11/95 9/11/95 10/11/95 0/6 4/4 2/2 4/4 4/4 4/4 2/2 4/4 0/6 4/4 6/6 4/4 6/6 2/2 4/4 4/4 0/6 2/2 5/5 4/4 6/6 2/2 4/4 2/2 Vol 8 No 1 20 December 1996 295 S. Aglioti et al 111 0111 0111 were presented in contact or in close proximity with that hand. When our patient viewed in her extrapersonal space or on her right hand the rings usually worn on her left hand, she recognized them as her own. This correct judgement probably occurred because the mode of stimulus presentation activated the ‘mine’ representation of the rings independent of that of the disowned hand. C.B.’s false judgement occurred only when the representation of the rings was activated conjointly with that of the repudiated hand. Since the left hand was no longer represented as ‘me’, the associated paraphernalia were also expunged from the body schema. It is remarkable that only in a condition in which the extrapersonal objects would normally be coded as ‘me’, the retrieval of autobiographical information about objects related to the disowned parts seemed impossible. This result would suggest that an object is represented in egocentric or in allocentric coordinates according to the ‘me’ or ‘mine’ labels attributed to it. Thus, in patient C.B., disowning or recognizing as her own the hand-rings complex depended on the dynamic integration of the appropriate reference frame with somatosensory and visual information, whether previous or current.6 Conclusion 0111 0111 The available information on the relation between denied body parts and paraphernalia related to them is extremely scanty. It has been anecdotally reported that a woman with right brain damage was puzzled by seeing her wedding ring on her disowned left hand.20 Equally anecdotal is our previous, unpublished observation of a woman with right brain damage in whom the disowned left hand was recognized as her own only when her wedding ring was put on the hand itself. Thus, C.B. differs from those previous cases and is the first known instance supporting the notion of an extended body schema. ACKNOWLEDGEMENTS: We wish to thank Dr J.C. Marshall and Dr J. Harris for their comments on an earlier draft of the manuscript. The financial contribution of MURST and the Consiglio Nazionale delle Ricerche, Italy, is gratefully acknowledged. References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. Reed CL and Farah MJ. J Exp Psychol 2, 334–343 (1995). Guariglia C and Antonucci G. Neuropsychologia 30, 1001–1009 (1992). Bisiach et al. Neuropsychologia 24, 759–767 (1986). Frederiks JAM. In: Frederiks JAM, ed. Handbook of Clinical Neurology, Vol. 4. Amsterdam: Elsevier, 1969: 207–240. Denes G. In: Boller F and Graffman J, eds. Handbook of Neuropsychology, Vol. 2. Amsterdam: Elsevier, 1989: 207–228 Lackner JR. Brain, 111, 281–297 (1988). James W. The Principles of Psychology. New York: Holt & Co., 1890. Critchley M. In: The Divine Banquet of the Brain. New York: Raven, 1979: 92–105. Melzack R. Sci Am 266, 90–96 (1992). Levine DN. Brain Cogn 13, 233–281 (1990). Ramachandran VS. Consciousness Cognition 4, 22–51 (1995). McGlynn SM and Schacter DL. J Clin Exp Neuropsychol 11, 143–205 (1989). Halligan PW, Marshall JC and Wade TD. Cortex 31, 171–182 (1995). Bisiach E, Rusconi ML and Vallar G. Neuropsychologia 29, 1029–1031 (1991). Heilman KM et al. In: Heilman KM and Valenstein E, eds. Clinic Neuropsychology. New York: Oxford University Press, 1993: 279–336. Bisiach E et al. Neuropsychologia 24, 471–482 (1986). Smania N and Aglioti S. Neurology 45, 1725–1730 (1995). Head H and Holmes G. Brain 34, 102–254 (1911). Melzack R. Trends Neurosci 13, 88–92 (1990). Bisiach E and Geminiani G. In: Prigatano GP and Schacter DL, eds. Awareness of Deficit After Brain Injury. New York: Oxford University Press, 1991: 17–39. Received 10 September 1996; accepted 24 September 1996 General Summary The present study provides the first experimental support to the speculative notion that objects external to the body may be included in one’s body image. We describe a woman with right brain damage in whom denial of the ownership of her left hand included extracorporeal objects (e.g. rings) which had been in close perceptual and representational contact with the left hand itself. When the same objects were worn on the right hand or were held by the examiner, the patient correctly recognized them as her own. Judgements of ownership were always correct when concerning objects unrelated to the denied body part (e.g. pins, earrings, comb). The disownership of left hand and objects related to it recovered with the same time course. This novel finding suggests that the mental image of one’s body may be extended to include inanimate objects which had been in contact or in close proximity with the body itself. 0111 111p 296 Vol 8 No 1 20 December 1996