Case report Is transmission of HIV-1 in non
advertisement

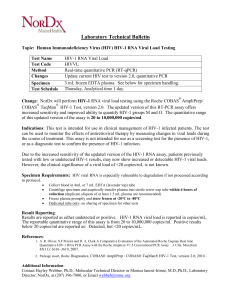
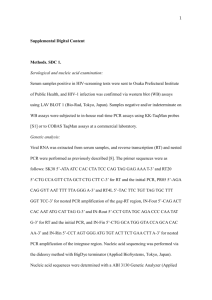
Antiviral Therapy 13:729–732 Case report Is transmission of HIV-1 in non-viraemic serodiscordant couples possible? Martin Stürmer 1*, Hans W Doerr 1, Annemarie Berger 1 and Peter Gute 2 JW Goethe University Hospital, Institute for Medical Virology, Frankfurt, Germany Infektiologikum, Frankfurt, Germany 1 2 *Corresponding author: E-mail: M.Stuermer@em.uni-frankfurt.de Several studies have shown that HIV-1 transmission in serodiscordant couples is significantly reduced when the plasma viral load (pVL) in the infected partner is low or undetectable. However, residual infectivity in the seminal compartment despite undetectable pVL has also been shown. Here we report HIV-1 transmission in a serodiscordant couple despite successful antiretroviral therapy of the HIV-infected partner. The newly infected partner had a negative HIV-1 screening ELISA when his HIV-1-­positive partner was already on antiretroviral treatment with undetectable pVL, which remained undetectable beyond the time of seroconversion in the initially negative partner. Frozen blood samples were analyzed phylogenetically from the HIV-1-positive patient and the newly infected partner before treatment and shortly after seroconversion, respectively; they showed a true relationship. On the basis of these data, the present report suggests that transmission of HIV-1 can occur despite undetectable pVL. This should be added to the discussion of prevention strategies, which should not advise the abandonment of safer-sex practices without referring to the relatively low but not impossible risk of HIV-1 transmission in this context. One major obstacle in the realization of prevention strategies is the belief that the risk of HIV-1 transmission in discordant couples virtually disappears due to a low or undetectable plasma viral load (pVL) if the infected partner is on highly active antiretroviral therapy (HAART; reviewed in [1]). Previous studies have demonstrated that a lower pVL is associated with decreased sexual transmission in discordant heterosexual partnerships [2], possibly due to a simultaneous decrease of HIV RNA in semen [3]. Quinn and colleagues [2] reported no transmission in discordant heterosexual partnerships in Uganda when the pVL was <1,500 copies/ml (51 couples, median follow-up of 22.5 months). Moreover, Vernazza and colleagues [3] showed that the likelihood of having detectable HIV in semen with undetectable pVL was low: only 2/114 patients were observed with detectable HIV RNA in semen, and both were included very early in their study. In addition, a mathematical model calculated the heterosexual transmission probability as 3 per 10,000 episodes of intercourse with 1,000 copies of HIV RNA in semen per ejaculate [4]. On the basis of these data the risk of transmission should be rated as very low. However, it has been shown that there might be residual low level viral load in the seminal compartment [3,5], and the present report suggests that sexual transmission at the individual level may occur despite an undetectable pVL (<50 copies/ml). The index patient is a 39 year old homosexual man diagnosed as HIV-1-seropositive on 14 January 1999. He started HAART on 15 July 2000 using a therapy regimen well-established in the Frankfurt HIV cohort comprising zidovudine, lamivudine and efavirenz [6]; on 13 September 2002 efavirenz was replaced by nevirapine due to toxicity. Shortly after the start of treatment, pVL (quantified using the Cobas Amplicor HIV-1 Monitor test kit version 1.5 UltraSensitive assay [Roche Diagnostics GmbH, Mannheim, Germany] with a limit of detection of 50 copies/ml) was <50 copies/ml (7 November 2000). The index patient’s pVL remained undetectable beyond the time point when his partner seroconverted and the CD4+ T-cell count reached adequate levels (Figure 1). Both the patient and the treating physician have independently confirmed that no other sexually transmissible disease (STD) could be detected clinically or by any laboratory parameter. The index patient’s partner is also a 39 year old homosexual man. He was found to be HIV-1-­seronegative in June 2002; this test was carried out anonymously at the local public health department and therefore a printed report is unavailable. However, the time period of the test has been confirmed by both the patient and the treating © 2008 International Medical Press 1359-6535 13_Sturmer.indd 729 729 22/7/08 13:25:38 M Stürmer et al. Figure 1. Changes of plasma viral load and CD4+ T-cell count values over time for the index patient 1x106 1,600 AZT/3TC/EFV AZT/3TC/NVP 1,400 1x105 1x104 1,000 1x103 800 600 1x102 400 10 200 0 Jul 98 CD4+ T-cell count, cells/mm3 Viral load, log10 copies/ml 1,200 0 Dec 99 Apr 01 Sep 02 Jan 04 May 05 Changes of plasma viral load (solid line) and CD4+ T-cell count (dotted line) values over time for the index patient. The start of the respective therapy regimen is indicated by arrows. Possible time of transmission (last negative and first positive HIV test of the newly infected partner) is indicated by a grey area. AZT, zidovudine; EFV, efavirenz; NVP, nevirapine; 3TC, lamivudine. physician. Additionally, the head of the local public health department confirmed that there were only two HIV-1positive test results at his department in June and July 2002, one belonging to a female patient and one to a known HIV-positive patient. The first positive HIV antibody test for the index patient’s partner was reported on 12 July 2004. Shortly after, his pVL was 21,800 copies/ml and CD4+ T-cell count was 338 cells/mm3. He remained untreated, with pVL and CD4+ T-cell count ranging from 21,800–231,500 copies/ml, and 263–414 cells/mm3, respectively (data not shown). The relationship started in August 2000, both partners deny having any other sexual relationships from that time on. According to independent questioning, the couple practiced safer-sex at the beginning, but had unprotected anal sexual intercourse on several occasions starting in May 2003. To rule out the possibility that the initially HIV-1­negative partner acquired his infection through a third person, a phylogenetic analysis was carried out as reported elsewhere [7]. The analysis is based on protease and reverse transcriptase sequences that have been shown to be sufficient for the reconstruction 730 13_Sturmer.indd 730 of transmission events [8]. A sample from the index patient was available from before he started HAART in 1999 (‘index’ in Figure 2) and a sample from the newly infected partner was obtained shortly after the first positive HIV-1 test (‘partner’ in Figure 2). Samples from local control groups collected during the same time frame were also analyzed, some of which were known to be related as described elsewhere [7]. Figure 2 shows the relationship between the sequences obtained from the index patient and his partner; they are clearly closely related although the time points of sample collection were approximately 5 years apart. Both sequences formed a single cluster with a bootstrap value of 99; the distance between both sequences was 0.001 on a length of 1,176 bases and the mean average distance of all sequences was 0.033 (data not shown). Local control group samples known to be related clustered as expected, but none of them formed a cluster with the sequences from the index patient and his partner. To our knowledge, this is the first report showing HIV-1 transmission in a serodiscordant couple despite an undetectable pVL (<50 copies/ml) in the infected partner. Although many people discuss the likelihood © 2008 International Medical Press 22/7/08 13:25:38 Non-viraemic HIV-1 transmission Figure 2. Phylogenetic tree of the protease/reverse transcriptase region Cont 15 Cont-24 B-AF286365 Cont 20 B-AF075719 B-M17449 B-K02013 B-K03455 B-U12055 Cont 3 Cont 25 B-M38429 B-U63632 B-M38431 B-U43141 Cont 29 Cont 30 Cont 13 Cont 28 Cont 9 Cont 26 Cont 1 Cont 10 Cont 14 Cont 2 Cont 12 Cont 17 Cont 5 Cont 6 Cont 16 Cont 8 Index Partner Cont 7 B-U69593 Cont 18 Cont 23 B-K02007 B-M26727 Cont 22 B-U21135 Cont 11 B-M17451 Cont 4 Cont 27 Cont 19 Cont-21 N-AJ006022 0.01 Phylogenetic tree of the protease/reverse transcriptase region of GenBank isolates indicated by their subtype and accession number, local control group patient isolates indicated by ‘cont’ and consecutive numbering, and the isolates of the index patient (indicated by ‘index’) and his partner (indicated by ‘partner’). Trees were generated by a bootstrap test with 10,000 replications on the basis of the Neighbor-Joining method with Kimura 2‑parameter substitution module, and rooted against a subtype N isolate. Bootstrap values are shown on the nodes. Antiviral Therapy 13.5 13_Sturmer.indd 731 731 22/7/08 13:25:39 M Stürmer et al. of transmission events in this context, no such case has been reported in the literature yet. Recently, a new discussion about prevention strategies in serodiscordant couples has been started; some experts even argue for no longer recommending safer-sex practices with the hitherto lack of published case reports supporting the epidemiological data. However, the current case suggests that transmission can occur in non-viraemic serodiscordant couples. The cluster formed in the phylogenetic analysis was unique and both the bootstrap value and the sequence similarity reached levels significantly associated with a true relationship of the two sequences, ruling out the possibility of transmission from a third person. The HIV-1-positive partner had a persistently undetectable pVL encompassing the time of the last negative (June 2002) and the first positive HIV-1 test (12 July 2004) of his initially HIV-1-negative partner, and the time between first undetectable pVL (7 November 2000) and the last negative HIV-1 screening test was 19 months. There are also some limitations regarding this case report. Although it has been shown that not all drugs reach sufficient concentrations in semen, the drugs used during the time period of possible transmission are known to penetrate the genital compartment quite well (reviewed in [9,10]). Already published data showed residual low level viral load in the seminal compartment, but mainly in the early phase of a suppressive HAART regimen [3,5]. Short periods of non-adherence or occurrence of other STDs might result in residual viral replication, so that transmission is more likely. This cannot be ruled out completely by the regular viral load determinations with undetectable pVL shown in Figure 1 (2002: 5 June, 4 September, 1 October, 16 October and 20 November; 2003: 26 February, 28 May, 20 August and 20 November; 2004: 26 February and 12 July), but both the index patient and the treating physician independently confirmed good adherence and the absence of any STDs. Although this case is of a retrospective nature dated back approximately 5 years, a continuously good adherence is based on the patient’s statement, and the seronegative HIV test in 2002 was done anonymously without an available written report, all data were independently and personally confirmed by the authors. Taken together, we feel confident that the present case report suggests that transmission can occur despite undetectable pVL. Therefore, we cannot support any recommendations that abandon the use of safer-sex practices in this context without mentioning the possibility of HIV-1 transmission. Disclosure statement The authors declare no conflicts of interest. References 1. Crepaz N, Hart TA, Marks G. Highly active antiretroviral therapy and sexual risk behavior: a meta-analytic review. JAMA 2004; 292:224–236. 2. Quinn TC, Wawer MJ, Sewankambo N, et al. Viral load and heterosexual transmission of human immunodeficiency virus type 1. Rakai Project Study Group. N Engl J Med 2000; 342:921–929. 3. Vernazza PL, Troiani L, Flepp MJ, et al. Potent antiretroviral treatment of HIV-infection results in suppression of the seminal shedding of HIV. The Swiss HIV Cohort Study. AIDS 2000; 14:117–121. 4. Chakraborty H, Sen PK, Helms RW, et al. Viral burden in genital secretions determines male-to-female sexual transmission of HIV-1: a probabilistic empiric model. AIDS 2001; 15:621–627. 5. Zhang H, Dornadula G, Beumont M, et al. Human immunodeficiency virus type 1 in the semen of men receiving highly active antiretroviral therapy. N Engl J Med 1998; 339:1803–1809. 6. Staszewski S, Morales-Ramirez J, Tashima KT, et al. Efavirenz plus zidovudine and lamivudine, efavirenz plus indinavir, and indinavir plus zidovudine and lamivudine in the treatment of HIV-1 infection in adults. Study 006 Team. N Engl J Med 1999; 341:1865–1873. 7. Sturmer M, Preiser W, Gute P, Nisius G, Doerr HW. Phylogenetic analysis of HIV-1 transmission: pol gene sequences are insufficient to clarify true relationships between patient isolates. AIDS 2004; 18:2109–2113. 8. Hue S, Clewley JP, Cane PA, Pillay D. HIV-1 pol gene variation is sufficient for reconstruction of transmissions in the era of antiretroviral therapy. AIDS 2004; 18:719–728. 9. Taylor S, Pereira AS. Antiretroviral drug concentrations in semen of HIV-1 infected men. Sex Transm Infect 2001; 77:4–11. 10. Chan DJ. Pathophysiology of HIV-1 in semen: current evidence for compartmentalisation and penetration by antiretroviral drugs. Curr HIV Res 2005; 3:207–222. Accepted for publication 15 April 2008 732 13_Sturmer.indd 732 © 2008 International Medical Press 22/7/08 13:25:39