Manual Hyperinflation Improves Alveolar
Recruitment in Difficult-to-Wean Patients
Suh-Hwa Maa, Tzong-Jen Hung, Kuang-Hung Hsu, Ya-I Hsieh,
Kwua-Yun Wang, Chun-Hua Wang and Horng-Chyuan Lin
Chest 2005;128;2714-2721
DOI 10.1378/chest.128.4.2714
The online version of this article, along with updated information
and services can be found online on the World Wide Web at:
http://chestjournal.org/cgi/content/abstract/128/4/2714
CHEST is the official journal of the American College of Chest
Physicians. It has been published monthly since 1935. Copyright 2007
by the American College of Chest Physicians, 3300 Dundee Road,
Northbrook IL 60062. All rights reserved. No part of this article or PDF
may be reproduced or distributed without the prior written permission
of the copyright holder
(http://www.chestjournal.org/misc/reprints.shtml). ISSN: 0012-3692.
Downloaded from chestjournal.org on September 19, 2007
Copyright © 2005 by American College of Chest Physicians
Manual Hyperinflation Improves
Alveolar Recruitment in Difficult-toWean Patients*
Suh-Hwa Maa, DSN; Tzong-Jen Hung, MD; Kuang-Hung Hsu, PhD;
Ya-I Hsieh, MS; Kwua-Yun Wang, MS; Chun-Hua Wang, MD; and
Horng-Chyuan Lin, MD
Study objectives: To investigate the effect of manual hyperinflation (MH) in patients with
atelectasis associated with ventilation support.
Design: Patients were randomized to either an experimental group or a control group.
Setting: Pulmonary ICUs from two hospitals.
Patients: Twenty-three patients with atelectasis associated with ventilation support.
Interventions: The MH technique was at a rate of 8 to 13 breaths/min for a period of 20 min each
session, three times per day for 5 days. The control group received their standard prescribed
mechanical ventilation without supplemental MH. Sputum contents (wet/dry weight ratio,
viscosity), respiratory system capacity (spontaneous tidal volume [VT], maximal inspiratory
pressure, rapid shallow breathing index [f/VT], chest radiograph signs, and PaO2/fraction of
inspired oxygen [FIO2]) were measured just prior to the MH at day 0 as baseline, and at day 3 and
day 6 of the study.
Measurements and results: There were significant improvements in scores over the 6-day study in
the experimental group compared to the control group in spontaneous VT (p ⴝ 0.035) and chest
radiograph signs (p ⴝ 0.040), and a trend toward improvement of f/VT (p ⴝ 0.066) and PaO2/FIO2
(p ⴝ 0.061) after adjustment for covariates. Other outcome variables did not differ significantly
between the experimental and control groups.
Conclusions: MH performed on patients with atelectasis from ventilation support significantly
improved alveolar recruitment.
(CHEST 2005; 128:2714 –2721)
Key words: alveolar recruitment; atelectasis; difficult to wean; manual hyperinflation
Abbreviations: ANOVA ⫽ analysis of variance; Fio2 ⫽ fraction of inspired oxygen; f/Vt ⫽ rapid shallow breathing
index; MH ⫽ manual hyperinflation; OR ⫽ odds ratio; Pimax ⫽ maximal inspiratory pressure; Vt ⫽ tidal volume
ventilation is indicated in acute reM echanical
versible respiratory failure. However, patients
receiving mechanical ventilation may have an increased risk of sputum retention, atelectasis, and
*From the School of Nursing (Dr. Maa), Department of Business
Administration (Dr. Hsu), Department and Graduate Institute of
Health Care Management, and Department of Thoracic Medicine II (Drs. C-H Wang and Lin), Chang Gung University,
Tao-Yuan; Department of Thoracic Medicine (Dr. Hung), Wei
Gong Memorial Hospital, Miao-Li; Department of Nursing (Ms.
Hsieh), Taipei Veterans General Hospital, Taipei; and School of
Nursing (Ms. K-Y Wang), National Defense Medical Center,
Taipei, Taiwan.
This study was supported by the National Science Council of
Taiwan, contract No. NSC 90 –2314-B-182– 062.
Manuscript received February 2, 2005; revision accepted May 3,
2005.
Reproduction of this article is prohibited without written permission
from the American College of Chest Physicians (www.chestjournal.
org/misc/reprints.shtml).
Correspondence to: Suh-Hwa Maa, DSN, School of Nursing,
Chang Gung University, 259, Wen-Hwa First Rd, Kwei-San,
Tao-Yuan, Taiwan, ROC; e-mail: shmaa@mail.cgu.edu.tw
pneumonia,1,2 making ventilation weaning more difficult3 and resulting in excess morbidity and mortality. The cost of maintaining patients on prolonged
ventilation in the ICUs of acute care hospitals are
high.4 Thus, every effort should be made to determine which patients can be rapidly extubated so as to
keep the weaning period to a minimum. Previous
evidence suggests that manual hyperinflation (MH)
can mobilize pulmonary secretions, reverse atelectatic alveoli, and increase alveolar oxygenation. Many
clinical studies have reported the short-term benefits
of MH on sputum clearance,3,5 reexpansion of atelectasis,5– 8 improvement of dynamic compliance,9
and oxygenation.10 –12 However, the lack of standardized methods for the delivery of MH makes the
synthesis and interpretation of the findings difficult.
The variability in the types of MH circuit (selfinflating manual resuscitation bags vs oxygen-powered, manual resuscitation bags), the method of MH
2714
Clinical Investigations in Critical Care
Downloaded from chestjournal.org on September 19, 2007
Copyright © 2005 by American College of Chest Physicians
delivery (technique of pausing at full inspiration vs
pressing half of the resuscitator), and the variability
in the dosage of MH (ie, duration) all point toward
the need for further development of the knowledge
base in order to guide best practice.
Manual hyperinflation is defined as inflating the
lungs using oxygen and manual compression to
provide a tidal volume (Vt) exceeding baseline Vt,
and using a Vt that is 50% greater than that
delivered by the ventilator, requiring a peak inspiratory pressure of from 20 to 40 cm H2O.13 Four
factors are considered important in performing the
MH technique: the application of larger-than-normal Vt breaths,14,15 use of a slow inspiratory flow
rate,16,17 an inspiratory pause,18,19 and a pressure
manometer.20,21 In addition, the quick release of
pressure on expiration leading to a rapid flow of air
can simulate the effect of a cough.11,22,23
Even though no comprehensive studies have been
done that incorporate and evaluate all four of the
important MH techniques, there is support from
clinical and research literature on the theoretical
foundations and effectiveness of each of the factors
separately. First, the use of larger-than-normal Vt is
based on the hypothesis that by delivering a largervolume breath over time, MH may increase the
expiratory flow rate and assist in moving secretions
toward more proximal airways, where they can be
cleared by suctioning.24 Second, the rate of inflation
of the lung as a whole is a function of inflation
pressure, compliance, and airway resistance. Nunn25
described the response to passive inflation of the
lungs by the development of a constant airway
pressure. If a constant inflation pressure is maintained, an alveolus with half the compliance but
twice the resistance of another alveolus will increase
in volume by half the volume change of the other
alveolus. Thus, the relative distribution of gas between the two alveoli is independent of the rate or
duration of inflation. In addition, using both hands to
compress the bag can produce a Vt that is 50%
greater than that delivered by the ventilator.26 Furthermore, the rate at which the bag is compressed,
rather than the resistance of the circuit itself, is the
main influence on the peak inspiratory flow
rate.16,17,27 A fast inflation rate that does not allow
the reservoir bag to fill adequately, and reduces the
fraction of the inspired oxygen (Fio2).28,29 Moreover,
delivering an increased Vt via MH may generate
adequate transpulmonary pressure gradients to overcome alveolar atelectasis. Atelectatic alveoli do not
reexpand immediately when the ventilator cycles
with the inspiratory phase because a variable period
of time is required before the alveolar critical opening pressure is reached.30 Therefore, the third important factor, the use of an inspiratory hold during
www.chestjournal.org
MH, is thought to maintain these pressure gradients
for an appropriate length of time. This technique
may influence the distribution of the ventilation25
and allow time for alveolar inflation or enlargement,
as well as the recruitment or unfolding of interdependent atelectatic alveoli. Finally, a pressure manometer can improve the performance of MH and
optimize both the safety and the effectiveness of the
treatment.31 Although there is no consensus about
specific safe upper limits for peak airway pressure,
barotraumas manifest at peak airway pressures of 26
to 64 cm H2O as demonstrated by several animal
studies.20 Therefore, it is reasonable and prudent to
minimize the peak airway pressure as much as
possible during MH or any other ventilatory support
procedure.32
This study examines the effect of MH in patients
with atelectasis associated with ventilation support.
The foundation for the practice of MH in this study
is based on the best evidence available from clinical
and research literature, and incorporates all four
factors of MH technique considered to be important,
as described above. The hypothesis of this study is
that those in the experimental group should have
improved sputum contents (wet/dry weight ratio,
viscosity), respiratory system capacity (spontaneous
Vt), maximal inspiratory pressure (Pimax), an improved rapid shallow breathing index (f/Vt), as well
as improved chest radiograph signs and oxygenation
ratio (Pao2/Fio2).
Materials and Methods
Patient Selection
Thirty-three patients with atelectasis due to ventilatory support
were recruited at the pulmonary ICUs from two hospitals; of
these 33 patients, 23 completed all of the study procedures. This
study was a two-group, prospective, randomized study lasting 6
days. Patients were assigned to one of two groups: standard care
with supplemental MH (experimental group, n ⫽ 10) or standard
care only (control group, n ⫽ 13). The Institutional Ethical
Committee approved the study protocol, and all patients gave
informed written consent. The inclusion criteria consisted of the
following: age ⱖ 40 years; ventilation support ⬎ 7 days and a
positive end-expiratory pressure from 6 to 8 cm H2O; pulmonary
atelectasis; excessive secretions (⬎ 30 mL/d); and spontaneous
Vt ⬍ 250 mL and/or Pimax ⬍ 25 cm H2O and/or Vt ⬍ 400 mL
under ventilator assistance. Pulmonary atelectasis was diagnosed
using the following: (1) chest radiography showing increased
infiltration, and (2) physical examination revealing weakness or
muteness of the sounds in the involved area. The structural
changes that develop in atelectasis increase the density of the
lungs. The increase in lung density resists radiograph penetration
and is revealed on radiograph films as increased opacity (ie,
whiter in appearance). Thus, the more severe the atelectasis, the
denser the lungs, and the whiter the radiograph film. Patients
were assessed clinically and with a chest radiograph at recruitment to ensure the absence of a Fio2 ⱖ 0.6 requirement,
CHEST / 128 / 4 / OCTOBER, 2005
Downloaded from chestjournal.org on September 19, 2007
Copyright © 2005 by American College of Chest Physicians
2715
pulmonary pathology (for example, ARDS), active infection,
acute cardiovascular dysfunction, or other systemic diseases. The
trial took place between January 2001 and June 2001. There were
three different types of ventilation systems used throughout this
study (models 7200, 740, or 760; Nellcor Puritan Bennett;
Temecula, CA).
Standard Care
All subjects were asked to continue any current prescribed
medication (such as anticholinergic inhaled agents, inhaled corticosteroids, theophylline, prednisolone, or erythromycin) and
chest physiotherapy (such as chest percussion, positioning, and
suction) throughout the experiment. For the control group, these
were the only prescribed treatments. None of the subjects
received any sedation or narcotics.
MH
To ensure that uniform and correct techniques were employed,
MH was administered by only one investigator. A 2.0-L reusable
manual resuscitator (model 2153 MR100 plus; Galemed Corporation; Taipei, Taiwan) was used to deliver the MH breaths, and
was connected to a flow of 100% oxygen at 15 L/min (calibrated
with an oxygen analyzer). A force meter (Inspiratory Force
Meter; Boehringer Laboratories; Norristown, PA) was connected
between the resuscitator and the patient. Patients received MH
to a peak airway pressure of 20 cm H2O by use of the resuscitator.
The resuscitator was slowly compressed with both hands, and an
inspiratory breath was maintained for 3 to 5 s at the end of
pressing half of the resuscitator, and then completely pressing the
resuscitator. Expiration was passive and unobstructed to facilitate
expiratory flow with no positive end-expiratory pressure applied.
Sufficient time was allowed for the resuscitator to fill completely
prior to the next breath. Airway suctioning of the endotracheal
tube was performed using size 14 catheters (Pahsco; Pacific
Hospital Supply; Taipei, Taiwan) at the end of the MH procedure. The MH procedure was carried out at a rate of 8 to 13
breaths/min for a period of 20 min for each session tid (at 7:40
am, 11:40 am, and 3:40 pm) for 5 days on days 1 to 5 of the study.
Sputum Sampling
Nurses were instructed to collect and record the total amount
of daily sputum (milliliters per 24 h) throughout the study. An
aliquot of sputum from each patient’s total amount of daily
sputum was freeze-dried (at – 80°C, at a negative pressure of 40
cm H2O) overnight to measure the wet/dry weight ratio.
The viscosity of the sputum was measured using a viscometer
at room temperature (25°C) with distilled water as a control,
using sputum sampled by nurses at 7 am on days 0 (baseline), 3,
and 6 of the study. After receiving chest percussion, the sputum
was collected by airway suctioning of the endotracheal tube into
a sterile pot.
Measurement of Respiratory System Capacity
Respiratory system capacity measurements were obtained 30
min after sputum sampling and just prior to the 7:40 am MH on
days 0 (baseline), 3, and 6 of the study. The spontaneous Vt score
was measured during ventilation disconnection (Haloscale
Wright Respirometer; Ferraris Medical Limited; Middlesex, UK)
by a respiratory therapist as spontaneous respiratory volume
(milliliters) per minute divided by respiratory rate per minute.
The Pimax was measured during ventilation disconnection with
the inspiratory force meter by the respiratory therapist. A
unidirectional expiratory valve pressure-manometer was connected to the endotracheal tube or tracheostomy, the port was
occluded at end-expiration for 20 s, and after three spontaneous
maximal inspiratory efforts the Pimax was recorded.33,34 The f/Vt
score was measured during mechanical ventilation as a calculation of the ratio of the respiratory rate per minute (frequency) to
the Vt setting (liters) from the display on the ventilation. A
portable radiograph machine was used, and a staff radiologist
reported the chest radiograph findings each morning. Scores
were given as 1 (improved) or 2 (not improved).
Nurses also recorded the ventilator volume and measured the
cuff pressure (Control-inflator; VBM Medizintechnik; Sulz am
Neckar, Germany) at least once or twice daily for patients with
tracheostomy. The volume needed to attain a full seal should be
recorded at least once or twice daily. The need for increasingly
larger volumes indicates an expanding trachea. The pressure was
kept at levels ⬍ 20 mm Hg. If there was an air leak in the cuff or
cuff inflation system, nurses reinflated the cuff via a stopcock. If
the ventilator could be set to compensate for the leak, the patient
was not reintubated. If significant aspiration or inadequate
ventilation was present, a new tube was inserted.
Oxygenation Ratio
Pao2/Fio2 was measured during mechanical ventilation as
derived from arterial blood gas analysis and the Fio2 on days 0
(baseline) and 6 of the study. A calibrated blood gas analyzer
(model 278; Ciba-Corning; Medfield, MA) was used for arterial
blood gas analysis, and the Fio2 was read from the display on the
ventilator obtained just prior to MH.
Statistical Analysis
Statistical software (version 10.0; SPSS; Chicago, IL) was used
for data analysis. 2 test and Fisher Exact Test were used to assess
the success of the randomization process in achieving two
comparable groups. A t test was performed to establish the
baseline stability of the dependent variables. A repeated-measures analysis of variance (ANOVA) was performed to compare
scores over time between the experimental and the control
groups on each of the seven dependent variables measured at
each of the three time points: day 0 (baseline), day 3, and day 6
of the study. This method accounted for six covariates: sex (male,
female), age, setting (medical center, local hospital), intubation
(endotracheotomy, endointubation), logarithm of length of ventilation prior to enrolment, and logarithm of total sputum
amount.35 The null hypothesis is that there is no interaction
between group and study duration, ie, the 5 days of treatment
with repeated measures on days 0, 3, and 6. There is a gradual
increase in treatment effect if there is interaction between the
group and the duration of the treatment. The Mantel-Haenszel
2 test for categorical data, adjusted odds ratio (OR), and
multiple logistic regression were performed on the chest radiograph scores. The OR was calculated as the odds in favor of
clinical improvement in the treatment group divided by the odds
in favor of clinical improvement in the control group. Significance was indicated at p ⬍ 0.05.
Results
Sample
Initially, 33 patients agreed to participate in this
investigation; of these, 10 patients withdrew. Twenty-three patients (n ⫽ 23) completed the full course
2716
Clinical Investigations in Critical Care
Downloaded from chestjournal.org on September 19, 2007
Copyright © 2005 by American College of Chest Physicians
of treatment. The attrition rate in this experiment
was high (30%), perhaps because of the characteristics of respiratory failure from mechanical ventilator
support. Of the 10 patients who dropped out, 3 died
(1 from the experimental group and 2 from the
control group), 4 withdrew voluntarily (3 from the
experimental group and 1 from the control group),
and 3 received oxygen content ⬎ 50% during the study
period (1 from the experimental group and 2 from the
control group). As most of the withdrawals were for
medical reasons, there is reason to hypothesize that
some of these patients might have benefited from MH.
In addition, there were no statistically significant differences in baseline demographics, clinical characteristics, or outcome measurements between those who
withdrew and the remaining participants.
Patient Characteristics
Table 1 lists the sample baseline demographic and
clinical characteristics including intubation, setting,
and length of ventilation prior to enrollment. There
were no statistically significant differences between
the subjects of the two groups. The sample contained
more men (n ⫽ 17) than women (n ⫽ 6); 74% of the
subjects were ⬎ 65 years of age, 100% were married,
and 74% had no history of smoking. All subjects were
receiving mechanical ventilation for at least 7 days
prior to study entry. The average Fio2 was 35%;
pneumonia was diagnosed in 17 persons, and lowerlobe atelectasis was found in 19 persons.
Table 1—Characteristics of Subjects*
Characteristics
Experimental Control
All
p
Group
Group Subjects Value†
Total subjects, No.
10
Sex
Male
8 (80)
Female
2 (20)
Age, yr
ⱖ 65
7 (70)
ⱕ 64
3 (30)
Cigarette history
No
6 (60)
Yes
4 (40)
Intubation
Tracheostomy
3 (30)
Endotracheal tube
7 (70)
Setting
Medical center
8 (80)
Local hospital
2 (20)
Length of ventilation prior
to enrollment, d
7
5 (50)
8 to 13
2 (20)
ⱖ 14
3 (30)
13
Outcome Measures
Outcome measure scores are compared in Table 3,
and the mean scores and the p value for their
group ⫻ time interaction in repeated-measures ANOVAs adjusted for covariates are listed. The spontaneous
Vt and chest radiograph scores show significant differences between the experimental and control groups,
and the f/Vt and Pao2/Fio2 scores show a trend toward
improvement in the experimental group compared to
the control group.
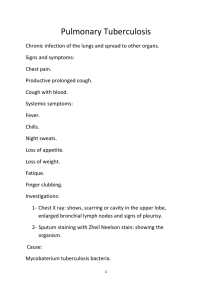
In the experimental group, spontaneous Vt scores
of 196.3 mL at baseline increased to 270.5 mL on
day 6 (indicating an improvement) compared to the
control group, which increased from 208.49 mL at
baseline to 220.14 mL on day 6 (p ⫽ 0.035; Fig 1).
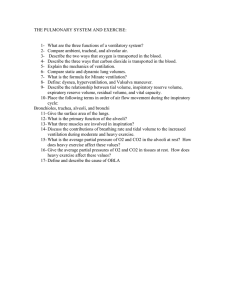
Furthermore, in the experimental group, f/Vt scores
of 216.59 at baseline decreased to 150.21 on day 6
compared to the control group, which decreased
from 174.04 to 164.74 (p ⫽ 0.066; Fig 2). Moreover,
in the experimental group, Pao2/Fio2 scores increased from 222.07 at baseline to 264.45 on day 6
compared to the control group, which decreased
from 228.64 to 203.53 (p ⫽ 0.061; Fig 3). Further, in
the experimental group, chest radiograph scores
improved 15.55-fold (95% confidence interval, 1.14
to 239.77; p ⫽ 0.040) after adjustment for covariates
23
0.46
9 (69)
4 (31)
17 (74)
6 (26)
0.54
10 (77)
3 (23)
0.20
11 (85)
2 (15)
17 (74)
6 (26)
5 (39)
8 (61)
8 (35)
15 (65)
0.51
0.31
8 (61)
5 (39)
16 (70)
7 (30)
0.40
3 (23)
3 (23)
7 (54)
Table 2—Comparison of Baseline Measurements
Between Groups (n ⴝ 23)*
17 (74)
6 (26)
8 (35)
5 (22)
10 (43)
*Data are presented as No. (%) unless otherwise indicated.
†2 and Fisher Exact Test.
www.chestjournal.org
Table 2 shows the actual values of the outcome
variables in all patients at baseline. Differences in
baseline values between the two groups were not
statistically significant except for the sputum
amount. The logarithm of the total sputum amount
was used as covariates in the repeated-measures
ANOVA model; therefore, the data from all the
subjects were included in the analyses.
Variables
Sputum content
Amount, mL/24 h
Wet/dry weight
ratio, %
Viscosity, min
Respiratory system
capacity
Spontaneous Vt, mL
Pimax, cm H2O
f/Vt
Oxygenation ratio
Pao2/Fio2
Experimental
Group (n ⫽ 10)
Control
p
Group (n ⫽ 13) Value†
186.50 ⫾ 116.57
27.82 ⫾ 11.48
94.62 ⫾ 53.64
19.29 ⫾ 13.67
0.02
0.13
9.67 ⫾ 17.91
8.57 ⫾ 12.60
0.87
196.30 ⫾ 80.87 208.49 ⫾ 54.56
27.00 ⫾ 16.87
20.92 ⫾ 10.46
216.59 ⫾ 146.62 174.04 ⫾ 66.62
0.67
0.30
0.36
222.07 ⫾ 93.94
0.90
228.64 ⫾ 131.84
*Data are presented as mean ⫾ SD.
†t test.
CHEST / 128 / 4 / OCTOBER, 2005
Downloaded from chestjournal.org on September 19, 2007
Copyright © 2005 by American College of Chest Physicians
2717
Table 3—Repeated-Measures ANOVA on Outcome Measures Between Experimental and Control Groups (n ⴝ 23)*
Outcome Measures
Sputum content
Sputum wet/dry ratio, %
Day 0 (baseline)
Day 1
Day 2
Day 3
Day 4
Day 5
Sputum viscosity, min
Day 0 (baseline)
Day 3
Day 6
Respiratory system capacity
Spontaneous Vt, mL
Day 0 (baseline)
Day 3
Day 6
Pimax, cm H2O
Day 0 (baseline)
Day 3
Day 6
f/Vt
Day 0 (baseline)
Day 3
Day 6
Chest radiographs
Improved/not improved, No.
Adjusted OR
95% confidence interval for OR
Oxygenation ratio
Pao2/Fio2
Day 0 (baseline)
Day 6
Experimental Group (n ⫽ 10)
Control Group (n ⫽ 13)
27.82 ⫾ 11.48
28.36 ⫾ 11.32
32.01 ⫾ 19.08
25.83 ⫾ 9.25
48.76 ⫾ 51.59
37.22 ⫾ 35.99
19.29 ⫾ 13.67
19.38 ⫾ 12.65
20.52 ⫾ 13.95
20.27 ⫾ 18.00
19.89 ⫾ 16.07
18.87 ⫾ 14.28
9.67 ⫾ 17.91
5.85 ⫾ 4.98
5.49 ⫾ 5.35
8.57 ⫾ 12.60
13.01 ⫾ 21.08
24.60 ⫾ 23.95
196.30 ⫾ 80.87
287.07 ⫾ 120.03
270.50 ⫾ 98.65
208.49 ⫾ 54.56
223.61 ⫾ 63.26
220.14 ⫾ 79.34
27.00 ⫾ 16.87
30.30 ⫾ 10.26
36.10 ⫾ 16.16
20.92 ⫾ 10.46
17.92 ⫾ 9.54
18.38 ⫾ 8.14
216.59 ⫾ 146.62
133.67 ⫾ 84.08
150.21 ⫾ 66.12
174.04 ⫾ 66.62
144.22 ⫾ 65.55
164.74 ⫾ 101.50
9/1
16.56
1.14–239.77
6/7
1.00
222.07 ⫾ 93.94
264.45 ⫾ 113.41
228.64 ⫾ 131.84
203.53 ⫾ 96.17
p Value†
0.831
0.145
0.035
0.194
0.066
0.040
0.061
*Data are presented as mean ⫾ SD unless otherwise indicated.
†Treatment ⫻ time interaction in repeated-measures ANOVA, adjusted for sex, age, setting, intubation, logarithm of length of ventilation prior
to enrollment, and logarithm of total sputum amount.
Figure 1. Mean values of spontaneous Vt in both groups;
horizontal bars ⫽ ⫹ 1 SD. p ⫽ 0.035 refers to differences between groups over time, with changes only on day 3 and day 6
while adjusting for sex, age, setting, intubation, logarithm of
length of ventilation prior to enrollment, and logarithm of total
sputum amount. Higher spontaneous Vt values represent patients with atelectasis associated with ventilation support-improved alveolar recruitment.
Figure 2. Mean values of f/Vt in both groups; horizontal
bars ⫽ ⫹ 1 SD. p ⫽ 0.066 refers to differences between groups
over time, with changes only on day 3 and day 6 while adjusting
for sex, age, setting, intubation, logarithm of length of ventilation
prior to enrollment, and logarithm of total sputum amount.
Lower f/Vt values represent patients with atelectasis associated
with ventilation support-improved alveolar recruitment.
2718
Clinical Investigations in Critical Care
Downloaded from chestjournal.org on September 19, 2007
Copyright © 2005 by American College of Chest Physicians
Figure 3. Mean values of Pao2/Fio2 in both groups; horizontal
bars ⫽ ⫹ 1 SD. p ⫽ 0.061 refers to differences between groups
over time, with changes only on day 6 while adjusting for sex, age,
setting, intubation, logarithm of length of ventilation prior to
enrolment, and logarithm of total sputum amount. Higher Pao2/
Fio2 values represent patients with atelectasis associated with
ventilation support-improved alveolar recruitment.
compared with the control group. Scores in sputum
wet/dry weight ratio increased from 27.82% at baseline to 37.42% on day 6 in the experimental group
and decreased from 19.29 to 18.87% in the control
group; scores in sputum viscosity decreased from
9.67 min at baseline to 5.49 min on day 6 in the
experimental group, and increased from 8.57 to
24.60 min in the control group, Pimax scores of
27.00 cm H2O at baseline increased to 36.10 cm
H2O on day 6 in the experimental group, and
decreased from 20.92 to 18.38 cm H2O in the control
group after adjustment for covariates compared with
the control group, even though these changes were
not statistically significant.
Discussion
To our knowledge, this is the first study to examine
the potential benefits of MH to 20 cm H2O by
oxygen-powered, manual resuscitation bag with an
inspiratory breath-hold of 3 to 5 s, while pressing half
of the resuscitator, in a group of intubated patients
with atelectasis. In addition, this study employed
methodologic features that strengthened validity and
reliability of the findings, including the randomization of subjects to groups and multivariate analysis
controlling for known covariates.
Those receiving MH had statistically significant
www.chestjournal.org
improvement in respiratory system capacity and
oxygenation ratio, evidenced by the scores of spontaneous Vt and chest radiograph signs, and a trend
toward improvement of f/Vt and Pao2/Fio2 compared to the control groups, after adjusting for the
effects of sex, age, setting, intubation, logarithm of
length of ventilation prior to enrolment, and logarithm of total sputum amount. These results are not
consistent with the fact that the MH technique was
initially designed to enhance clearance of airway
secretions.27 Nevertheless, it supported the initial
hypothesis of this study, that MH improves alveolar
recruitment by delivering a larger-volume breath
over time,24 and by the development of a constant
airway pressure25 in patients with atelectasis from
mechanical ventilation. In addition, MH produced
no adverse events in the experimental group, as none
of the patients experienced pneumothorax, suffocation, or hypotension during or following MH.
However, potential limitations of this investigation
should be considered when interpreting the findings.
These include the following: many of the outcome
measures have a subjective component to them,
because the respiratory therapist who scored these
outcomes was not blinded; failure to obtain outcome data of successfully weaned patients before
they completed this study; length of ventilation;
and the small sample size. In addition, this model
did not account for cigarette consumption, length
of atelectasis, and the severity of the illness, all of
which could account for group differences over
time. Future studies should incorporate such risk
adjustment using standard severity of illness measures as APACHE (acute physiology and chronic
health evaluation)36 or sequential organ failure
assessment37 scores.
Further study on the effects of MH should be
conducted using different resuscitation circuits (such
as MH to 30 or 35 cm H2O), different subject groups
(such as receiving ventilatory support for ⬍ 7 days,
and differentiating between chronic and acute atelectasis), and different operators (such as physiotherapists, respiratory therapists, or nurses). Additional
studies are also needed to elucidate the long-term
outcomes such as time to extubation, time to discharge, ventilator-free days, and discharge status
(home, long-term pulmonary care, death). Specifications by the practitioner, and patient preferences for
treatment duration and frequency should also be
explored.
Conclusion
This study provides evidence that MH performed
in a stable patient with atelectasis associated with
CHEST / 128 / 4 / OCTOBER, 2005
Downloaded from chestjournal.org on September 19, 2007
Copyright © 2005 by American College of Chest Physicians
2719
ventilation can improve spontaneous Vt and chest
radiograph signs, and a trend toward improvement of
f/Vt and Pao2/Fio2. MH is a nursing intervention
that could be implemented without a physician’s
order, and has the potential to make a positive
impact on patient outcome. While this preliminary
study with a small sample size does not warrant
changes in clinical practice at this time, it does
contribute to the evidence base on the benefits of
MH in critically ill and ventilator-dependent patients. Further investigations are required to replicate this study with a larger sample size, evaluate
different techniques of MH, evaluate effects of MH
in different patient groups, and determine the longterm outcomes of MH. As we continue to build
evidence through additional studies, we may eventually be able to recommend practice guidelines for
the procedure of MH for health professionals to treat
various clinical conditions.
ACKNOWLEDGMENT: The authors like to express their appreciation to Ivo L. Abraham, PhD, RN, of Matrix45, LLC, and
the School of Nursing, University of Pennsylvania, Philadelphia,
PA, and Karen M. MacDonald, PhD, RN, of Matrix45, LLC,
Earlysville, VA, for the time and effort they spent commenting on
earlier versions of this article. The authors also like to acknowledge the contribution of the physiotherapy, nursing, and medical
staff of Chang Gung Memorial Hospital for their expert assistance, especially Dr. Han-Pin Kuo.
References
1 Konrad F, Schreiber T, Brecht-Kraus D, et al. Mucociliary
transport in ICU patients. Chest 1994; 105:237–241
2 Anderson J, Jenkins S. Physiotherapy problems and their
management. In: Webber B, Pryor J, ed. Physiotherapy for
respiratory and cardiac problems. London, UK: Churchill
Livingstone, 1993; 226 –227
3 Berney S, Denehy L. A comparison of the effects of manual
and ventilator hyperinflation on static lung compliance and
sputum production in intubated and ventilated intensive care
patients. Physiother Res Intern 2002; 7:100 –108
4 Wagner DP. Economics of prolonged mechanical ventilation.
Am Rev Respir Dis 1989; 140(suppl):14S–18S
5 Hodgson C, Denehy L, Ntoumenopoulos G, et al. An investigation of the early effects of manual lung hyperinflation in
critically ill patients. Anesth Intensive Care 2000; 28:255–261
6 McCarren B, Chow CM. Description of manual hyperinflation in intubated patients with atelectasis. Physiother Theory
Pract 1998; 14:199 –210
7 Rothen HU, Sporre B, Engberg G, et al. Re-expansion of
atelectasis during general anesthesia: a computed tomography
study. Br J Anaesth 1993; 71:788 –795
8 Stiller K, Geake T, Taylor J, et al. Acute lobar atelectasis: a
comparison of two chest physiotherapy regimens. Chest 1990;
98:1336 –1340
9 Barker M, Adams S. An evaluation of a single chest physiotherapy treatment on mechanically ventilated patients with
acute lung injury. Physiother Res Intern 2002; 7:157–169
10 Patman S, Jenkins S, Stiller K. Manual hyperinflation: effects
on respiratory parameters. Physiother Res Intern 2000;
5:157–171
11 Jones AYM, Hutchinson RC, Oh TE. Effects of bagging and
percussion on total static compliance of the respiratory
system. Physiotherapy 1992; 78:661– 666
12 Tweed WA, Phua WT, Chong KY, et al. Tidal volume, lung
hyperinflation and arterial oxygenation during general anaesthesia. Anaesth Intensive Care 1993; 21:806 – 810
13 Denehy L. The use of manual hyperinflation in airway
clearance. Eur Respir J 1999; 14:958 –965
14 Maxwell L, Ellis E. Secretion clearance by manual hyperinflation: possible mechanisms. Physiother Theory Pract 1998;
14:189 –197
15 McCarren B, Chow CM. Manual hyperinflation: a description
of the technique. Aust J Physiother 1996; 42:203–208
16 Baker AB, Colliss JE, Cowie RW. Effects of varying inspiratory flow waveform and time in intermittent positive pressure
ventilation: various physiological variables. Br J Anaesth 1977;
49:1221–1233
17 Pillet O, Choukroun ML, Castaing Y. Effects of inspiratory
flow rate alterations on gas exchange during mechanical
ventilation in normal lungs: efficiency of end-inspiratory
pause. Chest 1993; 103:1161–1165
18 Bindslev L, Santesson J, Hedenstierna G. Distribution of
inspired gas to each lung in anesthetized human subjects.
Acta Anaesth Scand 1981; 25:297–302
19 Dammann J, McAslan T, Maffer C. Optimal flow pattern for
mechanical ventilation of the lungs. Crit Care Med 1978;
6:293–310
20 Redfern J, Ellis E, Holmes W. The use of a pressure
manometer enhances student physiotherapists’ performance
during manual hyperinflation. Aust J Physiother 2001; 47:
121–131
21 Hila J, Ellis E, Holmes W. Feedback withdrawal and changing compliance during manual hyperinflation. Physiother Res
Intern 2002; 7:53– 64
22 Hack I, Katz C, Eales C. Airway pressure changes during “bag
squeezing.” S Afr J Philos 1980; 36:97–99
23 Windsor H, Harrison G, Nicholson T. “Bag squeezing”: a
physiotherapeutic technique. Med J Aust 1972; 2:829 – 832
24 Clement AJ, Hubsch SK. Chest physiotherapy by the ‘bag
squeezing’ method. Physiotherapy 1968; 54:355–359
25 Nunn JF. Nunn’s applied respiratory physiology. 5th ed.
Oxford, UK: Butterworth-Heinemann, 2000; 166
26 Chulay M, Graeber GM. Efficacy of a hyperinflation and
hyperoxygenation suctioning intervention. Heart Lung 1988;
17:15–22
27 Maxwell L. Ellis ER. The effects of three manual hyperinflation techniques on pattern of ventilation in a test lung model.
Anaesth Intensive Care 2002; 30:283–288
28 Eaton JM. Adult manual resuscitators. Br J Anaesth 1984;
31:67–70
29 Glass C, Grap M, Corley M, et al. Nurses’ ability to achieve
hyperinflation and hyperoxygenation with a manual resuscitation bag during endotracheal suctioning. Heart Lung 1993;
22:158 –165
30 Galvis AG, Bowen A, Oh KS. Nonexpandable lung after
drainage of pneumothorax. Am J Respir Crit Care Med 1981;
136:1224 –1226
31 Goldstein B, Catlin EA, Vetere JM, et al. The role of in-line
manometers in minimizing peak and mean airway pressure
during hand regulated ventilation of newborn infants. Respir
Care 1989; 34:23–27
32 Haake R, Schlichtig R, Ulstad D, et al. Barotrauma: pathophysiology, risk factors, and prevention. Chest 1987; 91:608 –
613
33 Marini JJ, Smith TC, Lamb VJ. Estimation of inspiratory
muscle strength in mechanically ventilated patients: the
2720
Clinical Investigations in Critical Care
Downloaded from chestjournal.org on September 19, 2007
Copyright © 2005 by American College of Chest Physicians
measurement of maximal inspiratory pressure. J Crit Care
1986; 1:32–38
34 Caruso P, Friedrich C, Denari SDC, et al. The unidirectional
valve is the best method to determine maximal inspiratory
pressure during weaning. Chest 1999; 115:1096 –1101
35 Tukey JW. Exploratory data analysis. Reading, MA: AddisonWesley, 1977
www.chestjournal.org
36 Knaus WA, Draper EA, Wagner DP, et al. APACHE II: a
severity of disease classification system. Crit Care Med 1985;
13:818 – 829
37 Vincent JL, Moreno R, Takala J, et al. The SOFA score to
describe organ dysfunction/failure. Intensive Care Med 1996;
22:707–710
CHEST / 128 / 4 / OCTOBER, 2005
Downloaded from chestjournal.org on September 19, 2007
Copyright © 2005 by American College of Chest Physicians
2721
Manual Hyperinflation Improves Alveolar Recruitment in
Difficult-to-Wean Patients
Suh-Hwa Maa, Tzong-Jen Hung, Kuang-Hung Hsu, Ya-I Hsieh, Kwua-Yun
Wang, Chun-Hua Wang and Horng-Chyuan Lin
Chest 2005;128;2714-2721
DOI 10.1378/chest.128.4.2714
This information is current as of September 19, 2007
Updated Information
& Services
Updated information and services, including
high-resolution figures, can be found at:
http://chestjournal.org/cgi/content/full/128/4/2714
References
This article cites 33 articles, 8 of which you can access
for free at:
http://chestjournal.org/cgi/content/full/128/4/2714#BIBL
Permissions & Licensing
Information about reproducing this article in parts
(figures, tables) or in its entirety can be found online at:
http://chestjournal.org/misc/reprints.shtml
Reprints
Information about ordering reprints can be found online:
http://chestjournal.org/misc/reprints.shtml
Email alerting service
Receive free email alerts when new articles cite this
article sign up in the box at the top right corner of the
online article.
Images in PowerPoint format Figures that appear in CHEST articles can be
downloaded for teaching purposes in PowerPoint slide
format. See any online article figure for directions.
Downloaded from chestjournal.org on September 19, 2007
Copyright © 2005 by American College of Chest Physicians