Fate, complications and MRI implications of retention anchor suture
advertisement

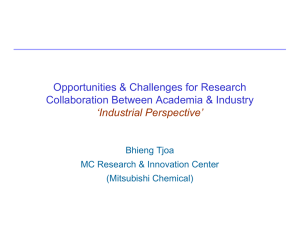
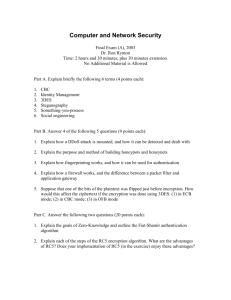
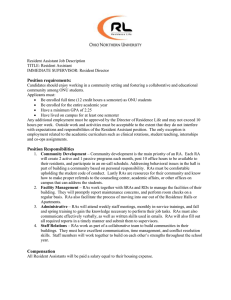
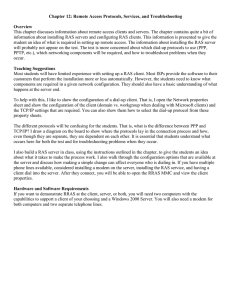
Pediatr Radiol (2013) 43:1009–1016 DOI 10.1007/s00247-013-2627-z PICTORIAL ESSAY Fate, complications and MRI implications of retention anchor suture placed during gastrostomy in children Surendra Narayanam & Vicente de Oliveira & Ganesh Krishnamurthy & Elhamy Bekhit & Madeleine Sertic & Hai-Ling Cheng & Bairbre L. Connolly Received: 27 August 2012 / Revised: 15 November 2012 / Accepted: 27 November 2012 / Published online: 17 February 2013 # Springer-Verlag Berlin Heidelberg 2013 Abstract Retrograde radiologic gastrostomy is one of several techniques used for placing a gastrostomy and is a common technique used in children. The use of a retention anchor suture (RAS) is an important component of this procedure. This pictorial essay explores the normal course and passage of the RAS, as well as abnormal migration, various complications and the implications of the RAS with regard to MRI safety. Keywords T fastener . Retention anchor suture . Gastrostomy . Pediatrics Introduction Although different methods—surgical, endoscopic and radiologic methods— are available for performing gastrostomies in children, the percutaneous radiologic retrograde gastrostomy S. Narayanam (*) : V. de Oliveira : M. Sertic : B. L. Connolly Diagnostic Imaging, Division of Image Guided Therapy, The Hospital for Sick Children, 555 University Ave, Toronto, Canada M5G 1X8 e-mail: nrssbabu@gmail.com G. Krishnamurthy Department of Radiology, The Children’s Hospital of Philadelphia, Philadelphia, PA, USA E. Bekhit Medical Imaging, RCG Melbourne, Melbourne, Australia H.-L. Cheng Diagnostic Imaging, The Hospital for Sick Children, 555 University Ave, Toronto, Canada M5G 1X8 using a retention anchor suture (RAS) is a technique commonly employed [1–4]. An alternative term for the RAS is a T fastener. A fundamental component of all methods of gastrostomies is gastropexy, which refers to the fixation of the anterior wall of the stomach to the anterior abdominal wall. Single or multiple gastropexies can be done depending on operator preferences and institutional practice. In retrograde radiologic gastrostomy, gastropexy, although not obligatory, is facilitated by a RAS. One of the RAS commonly used consists of a tiny longitudinal piece of metal with blunt ends, with a thread attached to its center (Cope Pediatric Gastrointestinal Suture Anchor Set, Cook, Bloomington, IN). The suture is a braided polytetrafluoroethylene (PTFE) impregnated polyester fiber. Its metal part is made up of a central metal core with a metallic wire wrapped around the core. The pediatric RAS is 1.3 cm in length and 0.025 inches (~0.063 cm) in diameter; the adult RAS is 2.0 cm in length and 0.038 inches (~0.095 cm) in diameter (Fig. 1). The number of RAS used during the gastrostomy varies from zero to four, depending on operator preference as well the requirements of the fixation [2, 5–10]. As the RAS is not expensive (in the order of $30 Canadian for two) and the potential advantages significant and complications uncommon, the risk–benefit balance may be considered in favor of its use. There are no strict guidelines for when to use a pediatric versus an adult RAS. The pediatric RAS is commonly used when performing a gastrostomy procedure in infants and children (e.g., up to approximately 35 kg, 10 years of age, thin abdominal wall), whereas the adult RAS may be used in older teenagers (e.g., more than 40 kg, > 12 years of age, thick abdominal wall). Little is known in the literature about the RAS in terms of the natural course of its passage, and its normal and 1010 Pediatr Radiol (2013) 43:1009–1016 Fig. 1 Retention anchor suture (RAS) used in enterostomy tube insertion. a Magnified view of the RAS with thread attached to its center. b Pediatric (top), adult (bottom) RAS for comparison abnormal appearances. Kim et al. [1] described 25/248 anchor-related complications in their series (breakdown of string in five, early release of anchor in nine, migration into peritoneal space in eight, and expulsion from body in three patients). Although we have had experience using the RAS in children for years, we paid little attention to it until recently, as issues or complications related to the RAS are uncommon. However, after a 4-year-old child presented to our service when she developed focal pain at her gastrostomy tube (G-tube) site following an MRI study, we decided to review the fate of RAS in children following G-tube placement. Clinical examination revealed the RAS extruding through her stoma. Her pain resolved following manual removal of the RAS (Fig. 2). Fig. 2 A 4-year-old girl with a low-profile button type of gastrostomy tube (G-tube). a The orientation of the RAS (arrow) is in the same axis as the button. b The girl complained of a focal pain at the insertion site. On examination, the RAS was seen partially extruded from the tract. c The RAS was removed manually using a forceps, with resolution of symptoms The aim of this pictorial essay is to review for the diagnostic and interventional radiologist some procedural aspects of the RAS, various appearances of the RAS, complications and MRI-related implications of the suture. Historical perspective The original description of the gastropexy device was the “Brown/Mueller T fastener” in 1986 [7]. The original device consisted of a needle with side slot near its tip for keeping the metal part of the T fastener, with the nylon thread running along the side of the needle. In the same year, Cope [11] also introduced a different design of anchor device, which is the basis of the current RAS commonly used. Pediatr Radiol (2013) 43:1009–1016 1011 Technique The technique described here is just one method of retrograde percutaneous gastrostomy in children and reflects our practice. Many variations of this technique are possible. The procedure of gastrostomy tube (G-tube) insertion can be performed under local anesthetic alone, sedation or general anesthesia in children. A dilute barium enema may be used to outline the colon so as to avoid traversing it. The liver and spleen edges are usually marked with sonography. The stomach is inflated with air and localized with a combination of sonography and fluoroscopy. A single pediatric RAS is loaded manually into an 18-G needle (Fig. 3), which is used to puncture the stomach. We virtually never use more than one RAS for G-tube, as compared to cecostomy tubes where we routinely use two RAS. In situations of high risk for separation of the anterior gastric wall from the abdominal wall (e.g., patient on peritoneal dialysis), we may consider using more than one. Once the intragastric position of the needle is confirmed with a contrast injection (Fig. 4), a 0.035-inch (~0.089 cm) straight wire is advanced through the needle, displacing the RAS into the stomach, while simultaneously maintaining access to the stomach. The needle is removed over the wire keeping gentle tension on the thread of the RAS. Dilatation of the track is performed over the wire. External traction on the thread helps to oppose the anterior gastric wall to the abdominal wall during dilatation. Care needs to be taken at this point not to exert too much pull on the thread of the RAS as it may cause the thread to snap. A pigtail catheter is placed over the wire into the stomach. The choice of size of the pigtail catheter is at the discretion of the operator and generally depends on the size of the child (e.g., 8 Fr in an infant, 10 Fr in a young child and 12 Fr in an older child or teenager); however, this will vary from institution to institution and from one interventionalist to another. Normally, the RAS attains an orientation either in the longitudinal or transverse axis, parallel to gastric and abdominal wall. Once the tube is in place, the thread needs to be secured. The adult RAS comes with a needle attached to suture it to the skin. The pediatric RAS, on the other hand, does not have a suturing needle. It may be secured by rolling the thread of the RAS over a small piece of gauze and the thread then kept taut with tape; e.g., Steri-Strips (3 M, St. Paul, MN) to prevent it unraveling. Apposition of the Fig. 3 Schematic diagram of the RAS preloaded in the hollow of the access needle with thread passing through the needle and hanging from its hub Fig. 4 Schematic diagram of the RAS loaded in the access needle with syringe filled with contrast agent attached; note the thread of the RAS is still hanging from the hub. Contrast medium is used to ensure the position of the tip of the needle is within the stomach; later, the RAS is deployed into the stomach using a guidewire stomach to the abdominal wall promotes healing and formation of a short tract (Fig. 5). The thread of the RAS is cut externally after a period of time (e.g., 1–2 weeks). The optimum time to cut the thread of the RAS is debatable. Once the thread is cut, the metallic portion falls into the gastric lumen and in due course it passes per rectum. However, prompt evacuation of the RAS does not always happen. Abnormalities Angle and alignment Traction on the thread of pediatric RAS can cause bending at the center of the metal portion of RAS, which then attains a V shape with variable angles (Fig. 6). An obtuse angle V Fig. 5 Image shows one method of securing the thread of the RAS onto a roll of gauze with traction maintained using tape around the thread. This plays an important role in maintaining apposition of the stomach to the abdominal wall and formation of the short tract. During the healing phase it helps minimize leakage into the peritoneal cavity 1012 Pediatr Radiol (2013) 43:1009–1016 Fig. 6 Image shows bending and obtuse angle. a Image in a 3-year-old boy with gastrostojejunostomy tube placed with RAS (arrow) shows a bend at its center. b When there is traction on the thread of the RAS, there is a tendency for the RAS to bend at its center where the thread is attached into the shape of a V. Often, it forms an obtuse angle of the RAS is very common. If the angle of the V is very acute, it may slip in retrogradely into the tract and thus not serve its intended purpose. If the RAS lodges in the tract, it may cause symptoms such as focal pain, irritability and infection. Sometimes, it may get embedded in the gastric wall or stuck in the tract. At this point, fluoroscopy assessment combined with high-frequency sonography provides valuable information. Sonography easily identifies the gut signature, abdominal wall layers, and the location and shape of the RAS (Fig. 7), as well as any collection that may have formed around the RAS in the tract (Fig. 8). The RAS can orient itself parallel to the long axis of the G-tube, in which case it is liable to be extruded spontaneously out from the tract. It may be a cause of focal pain and occasionally require manual removal with forceps as shown in Fig. 2. Timing of passage After cutting the thread, within a few weeks the RAS will be passed in the stools. However, the speed with which it passes is quite variable. The passage can be delayed for Fig. 7 A 2-year-old girl with G-tube with high-resolution US shows a V-shaped RAS (arrow) within the stomach abutting the anterior gastric wall months, even years, or may fail to pass entirely, if stuck in the tract or embedded in the gastric wall. As routine postprocedure imaging is not always performed, the exact rate of passage is uncertain. Preliminary review of data shows that in approximately 90–93% patients, the RAS had passed by week 5. Position and passage Occasionally, the thread of the RAS may snap during deployment or dilatation if excessive traction is used. As a result, the RAS may fall into the gastric lumen or be pulled into the peritoneal cavity (Fig. 9). Normally after cutting the thread, the RAS passes per rectum in the stools. Incidental abdominal radiographs in the subsequent weeks following a G-tube insertion may show the RAS in various locations during its passage: free in the stomach cavity, in the duodenum (Fig. 10), in the small bowel, colon or rectum (Fig. 10). CT imaging may be helpful for evaluation of atypical locations of the RAS: examples show the RAS Fig. 8 An 8-year-old boy who underwent G-tube insertion 10 days prior presents with tenderness at the site of insertion; high-resolution US shows the access site in the anterior gastric wall (thick arrow) and a collection anterior to the stomach in which the RAS (thin arrow) is noted Pediatr Radiol (2013) 43:1009–1016 Fig. 9 A 9-year-old boy during a G-tube insertion procedure: The thread of the RAS snapped and resulted in intraperitoneal placement of the RAS (arrow). Another needle puncture (preloaded with a second RAS) was required, as shown. Contrast medium injection shows the position of the tip of the needle in the stomach outside the anterior gastric wall (Fig. 11) or deep to the posterior gastric wall in the lesser sac with a pseudocyst formation (Fig. 11). In children with dilated, flaccid, poorly peristalsing bowel, the RAS may fail to pass. Intervention may be required (Fig. 12). Occasionally, the thread of the RAS entangles in the loop of the G-tube itself and, despite cutting the thread, it will not pass. Opening the G-tube pigtail and rotating the pigtail may be needed to release the RAS (Fig. 13). 1013 Fig. 11 CT of G-tube and RAS. a A 12-year-old girl with G-tube placed 4 weeks prior. a Axial CT image shows G-tube and RAS. The position of the RAS (white arrow) is incidentally found to be outside the anterior gastric wall due to migration. b A 15-year-old boy with Gtube placed 4 weeks prior in an outside institution. He presented to us with abdominal pain, tenderness and fever. Axial CT image shows the position of the RAS (thin black arrow) posterior to the posterior gastric wall and with pseudocyst formation (thick white arrow). There is small sleeve of collection around the G-tube anterior to the anterior gastric wall (thin white arrow) A low-profile balloon button-type G-tube (MIC‐KEY Low Profile Gastrostomy Feeding Tube, Kimberly Clark, Mississauga, ON), which is usually placed after 6–8 weeks following a primary insertion, has a radioopaque stripe that can mimic a RAS (Fig. 14). It is not metallic and does not pose a problem for MRI. Some pigtail tubes contain a metallic strip in their hub (e.g., Mac-Loc Dawson-Mueller tube; Cook, Bloomington, Fig. 10 A 10-year-old boy with G-tube. The RAS thread had been cut externally 2 weeks earlier. a Radiograph shows the position of the RAS still in the duodenum (arrow). b Another child with G-tube placed 6 weeks prior. The RAS thread had been cut externally 4 weeks earlier. The pelvic radiograph shows the rectal position of the RAS (arrow) before it was evacuated in the stool Mimics of RAS 1014 Pediatr Radiol (2013) 43:1009–1016 Fig. 12 A 3-year-old boy with duodenal atresia postsurgical repair, Gtube placed 10 weeks prior. The thread had been cut externally 8 weeks earlier. Intermittent imaging showed the RAS alternating between the stomach and duodenum without distal propagation. a, b Snaring and removal of the RAS was performed using a gooseneck snare. c The RAS (white arrow) seen caught in the snare before it is taken out IN) that also mimics a RAS, if the hub portion is projected in the image (Fig. 15). Surgical staples can look like a RAS (Fig. 15); the latter are usually nonferromagnetic; but occasionally, it is difficult to distinguish multiple surgical clips from a RAS unless several views are taken. Recognition of the RAS is important when reviewing imaging studies from both a patient safety perspective as well as for optimal MR image quality. The RAS is made of ferromagnetic material. We tested the adult and pediatric RAS on the 1.5- and 3-T MRI scanner. Both showed similar and strong magnetic attraction (displacement force > 45° to an almost 90° angle). To investigate if displacement occurred when the RAS was embedded in tissue, we also tested it in water (nonviscous), honey (viscous), and tofu (soft solid) as different tissue-mimicking media. The RAS aligned with the magnetic field in water and honey, but no movement was observed in tofu, thus demonstrating that motion was not an issue when the RAS was embedded in solid tissue. With respect to heating, the risk of heating is low because although the RAS is made of a coiled wire around a central metal core, the adult suture is only 2 cm long, 0.038 inches (0.095 cm) diameter and the pediatric is only 1.3 cm long and 0.025 inches (0.063 cm) diameter. These dimensions are much smaller than those at Fig. 13 A 6-year-old girl came for her G-tube change as it was blocked. a Fluoroscopic image shows the RAS (white arrow) in the loop of the G-tube, even though the thread had been cut externally 5 weeks earlier. It was speculated that the thread of the RAS was entangled in the loop of G-tube. b, c During the tube change, the RAS was pushed away from the G-tube loop using the guidewire and the loop of the new tube was successfully formed away from the RAS (white arrow) MR imaging Pediatr Radiol (2013) 43:1009–1016 Fig. 14 A 12-year-old boy with a low profile button-type G-tube shows a linear radio-opaque stipe (thick black arrow), which mimics the RAS. The original RAS with obtuse V shape (thin black arrow) is seen in the left hypochondrium region just above the button, most likely in the stomach 1015 which resonance or high currents are established (i.e. loop circumference between 6 cm and 12 cm, and implant length between 12 cm and 24 cm), limits that essentially define when significant implant-related heating will occur. In children, the RAS can cause pain probably due to movement, as exemplified by the index case. It will also cause compromise to the image quality due to susceptibility artifact during MRI studies of the abdomen (Fig. 16). The most common indication for G-tube in children is neurological disorders, many of which require MRI of the central nervous system [12]. Given the ferromagnetic properties of the RAS, one approach is to ensure the RAS has passed before a child undergoes an MRI by reviewing any available relevant imaging on PACS and if necessary performing fluoroscopic screening. Additionally, in those children requiring both an MRI and a G-tube, all attempts can be made to perform the MRI prior to the G-tube placement; or Fig. 15 A 14-year-old boy with lateral view of the abdominal radiograph (a) shows a linear radio-opaque line due to the metal within the hub of the Mac-Loc Dawson-Mueller G-tube, this mimics the RAS (thin arrow) as it is usually secured on the abdominal wall. Hence, it may be seen in the expected positions of the RAS as it passes normally through the bowel. Normal RAS (thick arrow) was seen near the loop of the G-tube. b A 12-year-old boy underwent surgical resection of Wilm tumor with G-tube insertion. Flouroscopic image AP view shows multiple surgical staples mimic RAS (arrow); lateral view (not shown) of the same child separated the RAS anteriorly from the surgical staples posteriorly in the retroperitonium Fig. 16 A 12-year-old boy with G-tube insertion. a CT image in bone window shows RAS in the stomach (arrow). b Axial MRI at the same level shows susceptibility artifacts degrading the image quality. c Coronal MR image shows similar artifacts. d Image shows the attraction of the freely hanging RAS toward a magnet, highlighting the hazard of potential movement of a RAS in the magnetic field 1016 Pediatr Radiol (2013) 43:1009–1016 Fig. 17 A 6-year-old boy who presented with accidental dislodgement of the G-tube on fourth day post insertion. a Attempt to access the immature tract using a guidewire (white arrow) shows the wire in the subcutaneous plane in a false tract. Black arrow indicates RAS. b As the external thread of the RAS was still present rolled around the gauze, it provided a potential route to the gastric cavity. The thread was unrolled and used to regain access into the stomach by advancing an intravenous cannula over the thread. Once within the stomach, a guidewire was advanced alongside the thread. The cannula was removed and the new G-tube was advanced over the wire failing that to recommend deferring the MRI if clinically permissible, until it is shown the child has passed the RAS. References Access through immature stoma The RAS can be used to advantage. In the event of accidental tube dislodgement when the tract is very new, there may be difficulty in passing a wire or catheter through an immature stoma. In such cases, the thread of the RAS can be employed to access the stomach. By unwinding the thread from the gauze roll and advancing it through an intravenous cannula or a dilator, one can then advance the cannula over the thread through the tract, thus enabling access to be regained into the stomach (Fig. 17). From there, a new Gtube can be replaced. Conclusion RAS is an important component of the retrograde percutaneous radiologic gastrostomy procedure. It has a varied fate and may be retained in the patient and potentially cause the patient symptoms. It causes MR image degradation and also potentially pulls or moves during MR imaging. It behooves the diagnostic and interventional radiologist to be aware of these issues in interpreting images and understanding a patient’s symptoms. Conflicts of interest None 1. Kim JW, Song HY, Kim KR et al (2008) The one-anchor technique of gastropexy for percutaneous radiologic gastrostomy: results of 248 consecutive procedures. J Vasc Interv Radiol 19:1048–1053 2. Chait PG, Weinberg J, Connolly BL et al (1996) Retrograde percutaneous gastrostomy and gastrojejunostomy in 505 children: a 4 1/2-year experience. Radiology 201:691–695 3. Connolly B, Krishnamurthy G, Amaral J (2010) Upper gastrointestinal access in children: techniques and outcomes. Tech Vasc Interv Radiol 13:222–228 4. Dewald CL, Hiette PO, Sewall LE et al (1999) Percutaneous gastrostomy and gastrojejunostomy with gastropexy: experience in 701 procedures. Radiology 211:651–656 5. de Baere T, Chapot R, Kuoch V et al (1999) Percutaneous gastrostomy with fluoroscopic guidance: single-center experience in 500 consecutive cancer patients. Radiology 210:651–654 6. Rossi UG, Petrocelli F, Seitun S et al (2012) Percutaneous radiological gastrostomy: single-puncture double-anchor technique. Radiol Med. doi 10.1007/s11547-012-0885-7 [Epub ahead of print 22 October] 7. Brown AS, Mueller PR, Ferrucci JT Jr (1986) Controlled percutaneous gastrostomy: nylon T-fastener for fixation of the anterior gastric wall. Radiology 158:543–545 8. Chan SC, Ko SF, Ng SH et al (2004) Fluoroscopically guided percutaneous gastrostomy with modified gastropexy and a largebore balloon-retained catheter in patients with head and neck tumors. Acta Radiol 45:130–135 9. Funaki B, Zaleski GX, Lorenz J et al (2000) Radiologic gastrostomy placement: pigtail-versus mushroom-retained catheters. AJR Am J Roentgenol 175:375–379 10. Foster A, Given M, Thornton E et al (2009) Removal of Tfasteners 2 days after gastrostomy is feasible. Cardiovasc Intervent Radiol 32:317–319 11. Cope C (1986) Suture anchor for visceral drainage. AJR Am J Roentgenol 146:160–162 12. Friedman JN, Ahmed S, Connolly B et al (2004) Complications associated with image-guided gastrostomy and gastrojejunostomy tubes in children. Pediatrics 114:458–461