Continuous Eligibility
for Children Under
Medi-Cal:
Cost Estimates for
Six-Month and Twelve-Month
Coverage Extension Options
May 1999
Prepared for the Medi-Cal Policy Institute by
Copyright © 1999 Medi-Cal Policy Institute
All rights reserved.
ISBN 1-929008-18-X
Table of Contents
A.
EXECUTIVE SUMMARY ............................................................................................................................... 1
B.
OVERVIEW OF CONTINUOUS ELIGIBILITY PROVISIONS................................................................ 3
C.
IMPLEMENTATION OF CONTINUOUS ELIGIBILITY IN OTHER STATES ..................................... 5
STATE PROGRAM DESIGN FEATURES ..................................................................................................................... 5
ADMINISTRATION AND IMPLEMENTATION ISSUES ................................................................................................. 6
REDETERMINATION PROCESS ................................................................................................................................. 7
BUDGET PROCESS .................................................................................................................................................... 7
COST EXPERIENCE TO DATE................................................................................................................................... 7
D.
CONTINUOUS ELIGIBILITY MODEL OPTIONS..................................................................................... 9
E.
DESCRIPTION OF MODELING APPROACH.......................................................................................... 10
STAGE 1: ESTIMATING ADDED MONTHS OF COVERAGE USING SIMULATION MODEL ........................................... 11
Step 1: Array Each Individual’s Eligibility by Month ..................................................................................... 13
Step 2: Create Rules for “Retrospectively Modeling” Continuous Eligibility ................................................ 14
Step 3: Count Months of New Eligibility for Each Design Option.................................................................. 15
Step 4: Extrapolate 5 Percent Sample to Full Medi-Cal Program.................................................................. 17
STAGE 2: ESTIMATING MEDICAL COSTS PER ADDED MONTH OF COVERAGE ...................................................... 18
Step 5: Identify Applicable Aid Categories (Those Who Would Receive Continuous Eligibility) ................... 18
Step 6: Identify Monthly Claims Costs for Selected Population........................................................................ 19
Step 7: Estimate Costs of Previously “Uncovered” Months for Fee-For-Service Population.......................... 19
Step 8: Estimate Costs of Previously “Uncovered” Months for Managed Care Population ............................ 20
Step 9: Trend the PMPM Cost Base .................................................................................................................. 22
Step 10: Derive Total Design Option Costs ...................................................................................................... 22
F.
SENSITIVITY ANALYSES ........................................................................................................................... 25
G.
HEALTHY FAMILIES OFFSETS................................................................................................................ 30
H.
ADMINISTRATIVE SAVINGS/COSTS ...................................................................................................... 31
I.
CONCLUSIONS AND “BEST ESTIMATE” ............................................................................................... 33
The Lewin Group, Inc.
Continuous Eligibility -- Modeling Projected Costs
A. Executive Summary
The Lewin Group was engaged by the Medi-Cal Policy Institute to analyze the financial costs
and savings of implementing continuous Medi-Cal eligibility provisions for children, as allowed
under the 1997 Balanced Budget Act. Specific tasks include: reviewing recent Federal
legislation and guidance, surveying other states that have implemented these provisions,
conducting an analysis of the impact of these options on California Medi-Cal expenditures, and
estimating the administrative costs and savings associated with implementation.
This document presents our report on the costs of implementing various Medi-Cal continuous
eligibility coverage modifications for children. Our best estimate is that if all children under age
19 are awarded six months of continuous Medi-Cal eligibility at each redetermination, the annual
added costs to Medi-Cal (state share only) will range from $48-57 million. If all of these
children are awarded twelve months of continuous eligibility, the annual added costs to Medi-Cal
(state share only) will range from $149-177 million. Costs during the initial year, when the
coverage modification is being phased in, will be considerably lower. The state share of Year 1
costs range from $24-$29 million for the 6-month option to $54-$65 million for the 12-month
option.
Providing eligible Medi-Cal children with 6 months of continuous eligibility will increase the
number of Medi-Cal covered children at a given point in time by approximately 140,000 –
roughly a five percent increase above the average number of children currently covered. A 12month continuous eligibility option will increase the average number of Medi-Cal eligible
children by approximately 431,000 at any given point in time – roughly a 16 percent increase.
Note that the additional coverage does not bring any new children into Medi-Cal, it allows those
who are enrolled to maintain coverage for longer periods of time and thus increases the number
of children covered at any given point in time.
These net enrollment and cost increases assume that no additional changes will be made to the
eligibility process. Programmatic changes that make it easier for persons to qualify for Medi-Cal
(e.g., creation of more generous eligibility standards, streamlining of the application form) will
increase the net costs of continuous eligibility, because they will add to the numbers of children
who initially access coverage. Programmatic changes that make it easier for children and adults
to remain on Medi-Cal (e.g., reduction of the quarterly reporting requirements) will increase
overall Medi-Cal costs because both children and adult coverage levels would increase.
However, such a program change would decrease the net costs attributable to the implementation
of continuous eligibility because there would be fewer coverage gaps to fill for Medi-Cal
children.
Due to the patterns of eligibility currently observed in the Medi-Cal program, the 12-month
continuous eligibility provision is approximately three times as costly as the 6-month provision,
The difference in coverage between the two options is illustrated in Exhibit A.
The Lewin Group, Inc.
Page 1
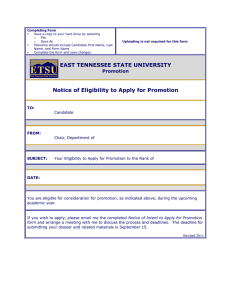
Exhibit A. Difference Between 6 and 12 Month Option for Hypothetical Individual
Jan ‘96
Feb ‘96
Mar ‘96
Apr ‘96
May ‘96
Jun ‘96
Jul ‘96
Aug ‘96
Sep ‘96
Oct ‘96
Nov ‘96
Dec ‘96
Jan ‘97
X=covered month; O=non-covered month
Coverage in absence of continuous eligibility
Simulation of 6 month continuous eligibility
Simulation of 12 month continuous eligibility
O X X X O O O O O O O O O
O X X X X X X O O O O O O
O X X X X X X X X X X X X
In this example, the child would lose Medi-Cal coverage as of April in the absence of continuous
eligibility provisions. The child would receive three additional months of coverage under the 6month provision, and nine months of additional coverage under the 12-month provision.1
Exhibit A also provides an example, albeit a greatly simplified one, of how The Lewin Group
developed its continuous eligibility simulation model and used it to arrive at the cost estimates in
this report. In order to simulate the costs of continuous eligibility, we used the State’s five
percent sample eligibility files and discerned the degree to which continuous eligibility would
have resulted in added months of Medi-Cal coverage for each child in the five percent sample
file. This simulation approach was used separately for the 6-month and 12-month design
options. We then worked with the corresponding claims files for the same five percent sample
population to determine the average costs of added months of coverage for various groupings of
Medi-Cal children. Total costs were derived by extrapolating the findings from the five percent
sample population to the demographic mix of all Medi-Cal children as of October 1998, and by
trending costs forward to the earliest possible years of continuous eligibility implementation
(2000 and 2001).
These estimates were developed for use by policymakers, health care professionals, advocates,
and others who are interested in or involved in Medi-Cal coverage expansion issues. Our report
is intended to walk the reader step-by-step through the details of the methodology and
assumptions used to produce the cost estimates. The Medi-Cal Policy Institute is preparing a
summary document of these findings that includes additional policy considerations and broader
policy implications of continuous eligibility.
1
The example illustrates an individual who originally had a three-month eligibility span. In this case, the eligibility
determination is presumed to occur in the first month of the span. See Attachment 1 for a complete description of the expected
effect of the program based on an individual’s historical eligibility patterns.
The Lewin Group, Inc.
Page 2
B.
Overview of Continuous Eligibility Provisions
Once a state grants Medicaid eligibility to a beneficiary, the state is required to perform a
periodic redetermination (reverification of family size, income, and resources) to ensure that
continued Medicaid eligibility is warranted. Subject to each state’s policy, redeterminations can
occur as frequently as every month or as infrequently as every 12 months; California currently
performs Medi-Cal redeterminations for most Medi-Cal enrollees every three months using the
Quarterly Reporting process. If a family experiences a rise in income—even if it is temporary—
the family may lose coverage during the next redetermination if their income level is greater than
the Medicaid threshold. If the family has a subsequent drop in income, they must repeat the
entire Medicaid application process in order to become re-enrolled. In addition, families are
required to self-report any changes in income or assets that would affect their eligibility between
redeterminations, and may be dropped from Medicaid if their self-reported income is greater than
Medicaid allows.
“Continuous eligibility” is a Medicaid provision that allows beneficiaries eligible for Medicaid to
remain eligible for a specified period of time, regardless of changes in income or resources.2
Prior to 1997, continuous eligibility for Medicaid was only available for pregnant women for up
to 90 days following delivery, and infants under age 1.3,4 The Balanced Budget Act of 1997
(BBA) extended to states the option to offer up to 12 months of continuous eligibility for
children under 19.5 States can elect to provide continuous eligibility for certain age groups (e.g.,
children under the age of 6) or all children. However, states cannot extend continuous eligibility
to children who qualify for Medi-Cal because they are medically needy.6 Currently, 10 states
offer continuous eligibility under the new BBA rules.7
A primary benefit of continuous eligibility is that it limits this “cycling” of persons on and off of
Medicaid due to temporary fluctuations in income. This enables beneficiaries to receive health
services, especially preventive services, on a predictable basis, and to begin a course of treatment
with knowledge that services will be covered until some date in the future. It also potentially
reduces some administrative burdens, particularly in the case of managed care programs where
continuous eligibility can reduce the volume of disenrollment and re-enrollment processing for
the health plans and for the State.
The Balanced Budget Act also addresses funding for continuous eligibility. The federal and state
matching funds for services provided during the continuous eligibility period depend on both
2
Because some states conduct eligibility redeterminations as infrequently as every 12 months, individuals in those states may
have effectively had continuous eligibility between redeterminations unless they reported an increase in income or resources
between redeterminations.
3
Per §1902 (e)(4) and (5) of the Social Security Act.
4
Another related option available to states is guaranteed eligibility for managed care populations. Guaranteed eligibility allows a
Medicaid beneficiary enrolled in a managed care organization to remain enrolled in the MCO for a specified period of time (not
to exceed 6 months), regardless of changes in income or resources. Guaranteed eligibility is not limited to children but is applied
to all beneficiaries, regardless of age. While this provision has been available to states for many years, the BBA expanded the
number of organizations that meet the definition of “managed care organization” from just Medicare certified medical plans and
FQHC-based plans to other types of HMOs and primary care case management programs.
5
Per §1902(e)(12) of the Social Security Act.
6
§1902(e)(12) does not cross-reference §1902(a)(10)(c), which describes the medically needy eligibility group.
7
AL, AR, CT, LA, MD, MI, NE, NM, SC, and WA.
The Lewin Group, Inc.
Page 3
Title 19 (Medicaid) and Title 21 (State Children’s Health Insurance Program) rules. The match
rate for children eligible for Medi-Cal under pre-1997 rules will be the regular Title 19 match
rate (51.23 percent), and funds spent on these children will have no effect on the state’s Title 21
allotment. The match rate for children eligible for Medicaid under an expansion group permitted
by the BBA (in CA, 14 to 18 year olds under 100 percent of the federal poverty level) will be the
enhanced Title 21 match rate (65.86 percent), and the federal matching funds will be paid from
the state’s Title 21 allotment.
The Lewin Group, Inc.
Page 4
C.
Implementation of Continuous Eligibility in Other States
In order to gain a better understanding of the operational challenges faced by states that are
implementing continuous eligibility in their Medicaid programs, The Lewin Group interviewed
Medicaid staff in five states that have submitted continuous eligibility state plan amendments to
HCFA. Below is a brief summary of continuous eligibility under the Medicaid or CHIP
programs in Connecticut, Indiana, Maryland, New Hampshire, and New Mexico, followed by
details regarding each state’s experience in the design, implementation, and funding of the
continuous eligibility option. Operational, administrative, and financial impacts the states have
already experienced are also addressed to the extent states conveyed this information.
State Program Design Features
•
Connecticut: Connecticut provides health coverage for Medicaid and CHIP through the
HUSKY program, which has three components—HUSKY A, HUSKY B, and HUSKY Plus.8
Part A provides Medicaid coverage for children under 19 in families with incomes up to 185
percent of the federal poverty level. Part B (CHIP) is separate from Medicaid, and provides
coverage to uninsured children in families up to 300 percent of the FPL. Participants in both
HUSKY Part A and B remain continuously eligible for 12 months, unless the child turns 19
or moves from the State. Redeterminations for both programs are performed annually.
•
Indiana: Indiana expanded its Medicaid program, first to cover children between the ages of
14 and 18 up to 100 percent of FPL, and then to cover all Medicaid-eligible children up to
age 18 to 150 percent of FPL. Eligibility redeterminations are conducted on an annual basis
for those higher-income families eligible for Medicaid only – meaning 12-month continuous
eligibility is in effect for these persons. Redeterminations are conducted on a quarterly basis
for those receiving Medicaid and food stamps.
•
Maryland: In 1996, Maryland developed an 1115 waiver program (HealthChoice) for all
Medicaid recipients in the State. The terms of the waiver allow the State to guarantee all new
Medicaid enrollees (adults and children) six months of Medicaid eligibility from the point in
which they enroll in a managed health care plan. In 1998 the State expanded Medicaid
eligibility for children under age 19 in families with incomes up to 200 percent of the FPL.
Maryland has not implemented continuous eligibility for children.
•
New Hampshire: New Hampshire expanded the Medicaid program for newborns and infants
up to age one in families that have incomes up to 300 percent of the federal poverty level
(FPL). The State plans to use CHIP funds to provide subsidized coverage for children
between the ages of 1 and 19 years in families who have incomes between 186 percent and
300 percent of the FPL. A child who is enrolled in a managed care plan through Medicaid or
8
HUSKY Plus, part of HUSKY Part B, provides supplemental mental and physical health coverage to medically eligible children
through programs for intensive physical and behavioral health needs.
The Lewin Group, Inc.
Page 5
the subsidized program will continue to be eligible for six months unless they reach the
maximum age, move from the State, or fail to pay premiums.
•
New Mexico: In July 1998, New Mexico expanded health care coverage under Medicaid to
SOBRA children (14 to 18 year olds) in families under 185 percent of the FPL. On March 1
of this year, New Mexico further expanded Medicaid to cover all children between 185 and
235 percent of the FPL. However, children in the 185 to 235 percent expansion group are
required to pay nominal co-pays for some services (the State received an 1115 waiver of
certain Medicaid requirements in order to be able to adopt cost sharing). The State offers a
twelve-month continuous eligibility period to all eligible children, including those in the
share-of-cost group.
Administration and Implementation Issues
In Connecticut, the option to provide 12 months of continuous eligibility to children in the
HUSKY program was strongly supported by the State legislature and the Governor. To
operationalize the continuous eligibility option in the HUSKY Part A program, Connecticut
created a new “deemed” eligibility category in its eligibility system. When a child is granted
eligibility for HUSKY Part A, the system automatically assigns the child 12 months of
eligibility. If a family self-reports (as required) an increase in income during the 12-month
period, and that increase would cause the child to lose eligibility if not for the 12-month
guarantee, the child’s eligibility category is changed to “deemed” status. This change is invisible
to the child, and the system continues to pay claims until the end of the 12-month period. The
“deemed” eligibility code enables the State to precisely track the number of children eligible for
HUSKY Part A solely because of the 12 month continuous eligibility option, as well as the costs
associated with these children, and ensure that the redetermination and follow-up processes are
conducted properly. 9
New Mexico has offered 12 months of continuous eligibility to all Medicaid-eligible children
(including the SOBRA expansion group) since July 1998, although continuous eligibility was
effectively in place prior to this for some families because Medicaid redeterminations for
poverty-level groups are conducted only once a year. The State conducted an extensive outreach
campaign for parents to ensure that they were aware of the provision and brought their children
in for timely redeterminations. New Mexico does not track whether persons would have lost
eligibility but for the continuous provision (e.g., after a self-reported increase in income). The
State was therefore unable to provide figures on the number of children affected by this
provision.
9
Between July 1998 (the first month of the program) and January 1999, 3,724 children who would have lost their eligibility
retained their coverage because of the 12 month continuous eligibility option. The average monthly caseload for children under
the age of 21 in Connecticut was about 125,000 in 1996.
The Lewin Group, Inc.
Page 6
Redetermination Process
States must periodically review each family’s (or individual’s) eligibility for Medicaid through a
periodic reassessment of family income and household composition. The process used for these
eligibility redeterminations varies considerably from state to state.
Most states that have implemented continuous eligibility have done so on a rolling basis; that is,
a family or child would appear for a redetermination under whatever schedule (monthly,
quarterly) was used under the old system, at which time a full continuous span would be granted.
Typically, children in the middle of a span as of the date the State began implementing
continuous eligibility would not begin their continuous eligibility period until their next
scheduled redetermination.
In Connecticut, children who remain fully eligible throughout the 12-month period are
automatically assigned a redetermination date, at which time their eligibility is reevaluated. If
the child or family remains eligible, the child is granted an additional 12 months of eligibility.
However, if the child is only eligible through “deemed” status at the end of the 12-month period,
the child is dropped from the eligibility rolls and a redetermination is not automatically
scheduled. If the family at some point in the future experiences a decrease in income, it can
reapply for HUSKY Part A, and if eligibility is granted, the child will retain it for an additional
12 months.
Budget Process
Few states were able to provide detailed information on the process for estimating the cost of
adding continuous eligibility for children to the State’s Medicaid program. However, two states
were able to summarize the process used to develop their initial budget estimates. Maryland
used a person-level database to project the costs of six months of eligibility for each recipient
who was eligible for fewer than 6 months during FY 1994. The average monthly payments per
person by eligibility category were utilized to calculate the costs for the remaining months of
eligibility for each person. Summing across all persons who had fewer than 6 months of
eligibility and trending forward the costs at 8 percent annually resulted in an estimate of about
$15 million in additional costs for the first full year of the program, in which approximately
300,000 persons enrolled.
Indiana followed a similar process. The budget office developed the person-level database by
first isolating those eligibility categories that were subject to redeterminations more frequently
than one year from those who would not be affected by the new provision (e.g., infants under age
1 who automatically get one year, other categories that are not income-based). The State then
collected 36 months of data on the remaining continuously enrolled children, to estimate the
costs of providing coverage for those children who were not continuously enrolled. Indiana
estimated that continuous eligibility would increase costs by $16.3 million for 33,310 children in
the first year.
Cost Experience to Date
Most states had too little actual experience with the continuous eligibility option to be able to
provide information on actual cost impacts to the Medicaid program due to the provision.
The Lewin Group, Inc.
Page 7
Several states commented that for various reasons, administrative costs might not be reduced as
much as hoped. For example, Indiana state staff pointed out that continuous eligibility will not
have much effect on the number of redeterminations that are performed, since the parents must
still come in for redeterminations. If Medicaid is expanded to higher income levels than other
welfare programs (such as food stamps), only the children at these higher income levels will
qualify, so for this small segment there will be fewer redeterminations. Indiana has found that
educating local social services caseworkers about the Medicaid, expanded Medicaid, and CHIP
programs has been a significant start-up expense. Staff in New Mexico also mentioned the costs
of outreach added to the total administrative financial burden of the program.
The Lewin Group, Inc.
Page 8
D.
Continuous Eligibility Model Options
To project costs of continuous eligibility for Medi-Cal children, The Lewin Group has prepared
cost estimates for six design configurations. The configurations are based on two potential spans
for continuous eligibility (6 months and 12 months), and three potential age groups (0-6 years, 014 years, and 0-18 years). These alternatives were developed to provide policy makers with a
range of program options and their budgetary impacts. The table below summarizes the six
configurations.
Age Group Covered
Duration of Continuous
Eligibility
1
0 to 6-year-olds
6 months
2
0 to 14-year-olds
6 months
3
0 to 18-year-olds
6 months
4
0 to 6-year-olds
12 months
5
0 to 14-year-olds
12 months
6
0 to 18-year-olds
12 months
The Lewin Group does not discuss the pros and cons of each option, beyond costing out
alternative design scenarios. It is important to note, however, that continuous eligibility, while
providing the benefits of coverage and continuity of coverage, also raises the possibility for
unnecessary payments to be made. The 12-month design option provides the greatest amount of
assured Medi-Cal coverage. However, given that about 60 percent of Medi-Cal children are
enrolled in capitated health plans, the 12-month option also holds the holds the greatest potential
for unnecessary payments to be made. In the example in Exhibit A, if the child left Medi-Cal
because of relocation or because private insurance was secured, continuous eligibility would
bring about no added costs to Medi-Cal in the fee-for-service setting. However, in the managed
care setting it is quite possible that the capitation would be paid throughout the period of
continuous eligibility. The State and managed care plans could take steps to ameliorate
overpayments (e.g., track utilization within the health plans to assure that the pediatric capitation
rates are being accurately established). However, these options are not explored here.
The Lewin Group, Inc.
Page 9
E.
Description of Modeling Approach
The Lewin Group used a two-stage approach to develop an estimate of the cost of implementing
each of the six configurations above. In the first stage, we estimated the number of months of
coverage that would be added per person if the 6-month or 12-month continuous eligibility
options were implemented.
In the second stage, we estimated the monthly costs of each added month of coverage in each age
group (0-6, 0-14, and 0-18). By multiplying each combination of these numbers, we determined
the total medical costs of implementing continuous eligibility for each configuration.
The estimates are based on recent Medi-Cal eligibility and cost data. Of tremendous value in
this regard is the 5 percent sample file created by DHS’s Fiscal Forecasting and Data
Management Branch. This data file tracks the eligibility of approximately 250,000 Medi-Cal
beneficiaries on a monthly basis across three years, and includes all of these persons’
corresponding medical claims. Periods of eligibility associated with retroactive eligibility, and
the claims costs associated with these periods, are included in the file on the same basis as
nonretroactive eligibility and claims. After estimating the additional eligible months that would
result from continuous eligibility, additional steps were required to extrapolate data from the
sample used in the model to the entire Medi-Cal population, and to account for medical inflation.
The process used to develop the cost estimates can be summarized as follows:
Stage 1: Estimate Added Months of Coverage Using Simulation Model
Step 1: Array each individual’s eligibility by month
Step 2: Create rules for “retrospectively modeling” continuous eligibility
Step 3: Count months of new eligibility for each design option
Step 4: Extrapolate 5 percent sample to full Medi-Cal program
Stage 2: Estimate Medical Costs Per Added Month of Coverage
Step 5: Identify applicable aid categories (eligible for continuous eligibility)
Step 6: Identify monthly claims costs for selected population
Step 7: Estimate costs of previously “uncovered” months, fee-for-service population
Step 8: Estimate costs of previously “uncovered” months, managed care population
Step 9: Trend the PMPM cost base
Step 10: Derive total net costs
The Lewin Group, Inc.
Page 10
The remainder of the document describes each of these steps in detail and presents the results.
Stage 1: Estimating Added Months of Coverage Using Simulation Model
We selected from the 5 percent sample those individuals who could be eligible for continuous
eligibility under the broadest scenario – that is, all enrolled children except the following:
•
Persons in a Share-of-Cost (SOC) aid category
•
Persons in a state-only aid category
•
Persons in a minor consent aid category
•
Persons receiving only postpartum coverage
Note that while medically needy and medically indigent children are excluded from continuous
eligibility under the federal legislation, these aid categories are included in our modeling because
they meet the income requirements for Medi-Cal and would thus be considered eligible for
continuous eligibility regardless of their medical condition. Consequently, if continuous
eligibility were implemented, these beneficiaries would be included in the initiative.
The distribution of Medi-Cal children by aid category is shown in Exhibit B on the following
page, along with indicators as to whether children in this category would be eligible to receive
continuous eligibility (an “X” in the “Classification” column indicates that the aid category is
excluded). The other letters in the “Classification” column in Exhibit B denote Lewin’s
categorizations of the included aid categories into groups with reasonably similar per member
per month (PMPM) medical costs, as shown below.
Classification Codes:
C
CalWorks and Related Populations (including percent of FPL programs)
D
Disabled (includes blind)
E
Emergency services only
F
Foster children
I
Infant programs
M
Medically needy and medically indigent
P
Pregnancy-related
T
Tuberculosis services
X
Excluded from continuous eligibility
The Lewin Group, Inc.
Page 11
EXHIBIT B. Medi-Cal Children As of October 1998
By Age and Aid Category
Aid
Category
October 1998 Eligibles
<1
1-6
7-12
13-14
15-18 Male
15-18 Female
TOTAL
Classification
1
3
23
35
12
59
52
184
C
2
2
9
26
6
21
32
96
M
3
41
6,025
8,665
2,015
1,113
1,279
19,138
C
4
20
1,262
2,955
787
479
464
5,967
M
1
X
5
C
1
X
6
1
8
1
14
1
1
20
22
528
768
245
239
244
2,046
D
23
1
1
3
2
2
1
10
M
11
12
2
3
3
31
M
1
D
2
X
5
D
24
1
1
26
1
1
27
1
28
1
1
1
3
30
47,919
417,519
369,358
92,933
62,688
71,059
1,061,476
C
32
2
168
153
31
19
27
400
C
33
10
66
70
8
6
7
167
P
34
34,978
87,559
68,105
19,472
21,271
24,110
255,495
M
35
15,623
123,878
95,247
23,973
16,855
17,540
293,116
C
36
1
3
X
37
44
522
952
370
511
512
2,911
X
38
5,541
85,097
64,538
15,413
22,865
22,279
215,733
C
39
650
10,617
9,081
2,317
1,673
1,596
25,934
C
3C
191
3,112
2,794
710
600
590
7,997
C
3E
5
17
26
2
2
4
56
X
1
2
X
2
3H
3L
1
2
3M
6
13
4
2
5
32
X
3
8
3
3
2
19
X
3N
2
19
29
7
7
7
71
X
3P
9
63
102
60
56
60
350
C
3R
771
8,929
14,816
5,092
4,261
4,435
38,304
C
3U
6
42
31
9
4
5
97
X
40
409
2,421
4,763
2,133
3,479
2,443
15,648
F
42
3,044
27,387
26,221
7,910
6,324
6,243
77,129
F
43
3
1
1
1
6
X
3
16
8
3
897
927
P
45
465
1,161
1,047
500
685
689
4,547
M
47
37,823
5,182
1
43,006
I
48
1
2
11
10
575
599
P
4
1
5
P
44
49
continued on next page
The Lewin Group, Inc.
Page 12
EXHIBIT B. Medi-Cal Children As of October 1998
By Age and Aid Category, cont'd
Aid
Category
4C
4K
54
55
58
59
5F
5K
5M
60
63
64
65
66
67
68
69
70
72
73
74
75
76
77
78
79
7A
7C
7H
7M
7N
7P
7X
82
83
8P
8R
TOTAL
<1
1-6
39
58
3
82
239
103
11
194
16,388
4,076
49
532
1
22,045
19
1,017
1,518
5
11
1
56
8
1
9
21
30
97,491
3,742
42
1
2
1
12
6,529
556
12
2
34,030
77
36,339
1
98,726
627
6
1
252,035
October 1998 Eligibles
7-12
13-14
15-18 Male
44
11
8
1
13
115
28
27
2
1
4
35,880
11,747
9,650
4,228
1,145
917
43
77
7
546
249
161
2
32,146
10,385
11,774
29
22
33
1,345
460
580
7
16
71
1
8
28
10
272
2
23
1
1
4
2
7
2
31
15-18 Female
15
7
20
3
10,652
829
3,186
327
7,658
28
290
1
3
6
15
7
1
1
42
1
31,203
5,531
27
7
2
106
7,162
1,697
10
88
167
649
4,073
967
14
324
1,108
4,365
893
4
326
4,240
963
37,571
433
6,377
108
5,949
118
9,488
164
3
1
2
149,666
40,428
35,770
43,534
TOTAL
175
21
275
10
84,556
11,298
3,373
2,009
3
85,526
136
3,703
1
19
42
166
86
21
97,774
3
3,765
1
44
2
2
54
53,332
9,644
67
745
4,411
2,826
1
192,141
1,527
6
7
557,772
Subtotal, Aid Categories Applicable to Continuous Eligibility (Classification not equal to "X"):
2,616,413
469.08%
Classification
F
M
C
P
O
C
P
M
X
D
M
D
X
D
X
D
I
P
C
X
E
X
X
X
X
X
C
P
T
X
X
X
X
M
X
X
X
Note that many aid categories are not listed in Exhibit B; these did not have any active Medi-Cal
eligibles as of October 1998. While several aid categories were excluded, the continuous
eligibility feature would be available to the vast majority of Medi-Cal children. As of October
1998, the included aid categories represented 99.5 percent of all Medi-Cal enrolled children.
The additional months of Medi-Cal coverage that continuous eligibility would cause were
estimated by simulating the introduction of this initiative across historical eligibility files, then
extrapolating the 5 percent sample information to the full Medi-Cal population. The steps taken
in this process are summarized below. The model simulates a January 1, 1996 start date for
implementation of continuous eligibility, and estimates the change in eligibility that would occur
between January 1996 and December 1997. Simulation over a 24-month time period permits
development of cost estimates for the phase-in period (Year 1), during which continuous
eligibility periods are granted upon annual eligibility redeterminations and for new eligibility
periods, and for a subsequent year (Year 2), which represents more of a “steady state” enrollment
level under continuous eligibility. In order to fully capture differences in the ways in which
continuous eligibility might be implemented and administered, we developed two different
scenarios to discern which months of non-eligibility would become eligible months.
Step 1: Array Each Individual’s Eligibility by Month
The 5 percent sample eligibility file tracks each person’s eligibility status month by month. For
each month, the coding shows whether or not the individual was enrolled in Medi-Cal and
his/her aid category, county, and, if applicable, health plan. This information was arrayed
throughout calendar years 1995, 1996 and 1997.
Aid categories and age/sex cohorts were ultimately grouped into clusters such that significant
differences in medical costs per person could be captured. Aid categories were first grouped into
“status codes” to aggregate persons with similar costs (e.g., disabled). These groupings are
summarized in Exhibit B and are also shown in Attachment 1, Table 3.10 The beneficiaries
were also grouped into six age/sex cohorts, both for purposes of permitting different age cut-offs
in the provision design and grouping persons with similar levels of expected per capita costs:
•
•
•
•
•
•
<1 Male & Female
1-6 Male & Female
7-12 Male & Female
13-14 Male & Female
15-18 Male
15-18 Female
10
Note that there are two minor differences between the classification described in Exhibit B and that described in Attachment
1. The original eligibility classification included two Aid Categories, Postpartum (#76) and Minor Consent (# 7M, 7N, 7P, and
7R) as eligible for continuous eligibility. These categories were included in the continuous eligibility simulations described in
Attachment 1. In the tables presented in Attachments 2 through 4, these categories are combined in the column labeled “Other
Excluded.” These categories are excluded from the calculations accumulating additional months under continuous eligibility.
Because of the very small number of eligible months associated with these aid categories, the inclusion of these aid categories in
the original simulation has virtually no impact on the final conclusions of the analysis.
The Lewin Group, Inc.
Page 13
Step 2: Create Rules for “Retrospectively Modeling” Continuous Eligibility
The next step involved analyzing the eligibility patterns of Medi-Cal eligibles and creating a set
of “rules” for discerning which non-covered months would become covered months if
continuous eligibility was in effect. These rules were applied to every child and adolescent in the
5 percent sample file.
Two different scenarios were modeled. Both scenarios assume that periods of continuous
eligibility will be granted only in the months of initial eligibility determination and
redetermination.11 The 5 percent sample data do not indicate which months represent eligibility
determination months; consequently, the scenarios establish rules for assigning this status to each
period or “span” of Medi-Cal enrollment. Since up to three months of retrospective eligibility
can be granted per eligibility period, and the start date of some eligibility periods occurs prior to
January 1995 and is therefore unknown, it is necessary to devise a method for determining where
continuous eligibility periods would be granted for each individual.
Under the “base scenario,” which is tracked throughout the main body of this report, we assumed
that some beneficiaries would not automatically be re-enrolled in Medi-Cal at the end of their
span of eligibility and that the expected number of retroactive months of eligibility varies by aid
category. We also modeled a “worst case” scenario, where we assumed that every recipient
remains enrolled for the entire three months between required filings of quarterly reports. In
other words, no beneficiaries were assumed to initiate disenrollment from Medi-Cal by selfreporting factors affecting their eligibility (e.g., income). Within that constraint, we assigned the
status of “annual eligibility determination month” to the calendar month that maximized the
number of additional covered months for each individual that would accrue under each
continuous eligibility policy. While this phenomenon clearly would not occur under a
continuous eligibility policy, we wanted to establish an aggressive upper bound estimate.
Unless specifically noted as using the “worst case” scenario, the tables and estimates described
throughout the remainder of this document are derived from the “base scenario” because we
believe it provides a more realistic depiction of the expected costs of continuous eligibility. A
detailed description of the rules used for each scenario is presented in Attachment 1.
While the rules are complex and involve several nuances to assign redetermination dates and
retrospective coverage periods, we are essentially awarding continuous eligibility in the
following manner under the base scenario:
•
Once continuous eligibility is implemented, children already covered by Medi-Cal receive an
initial period of continuous eligibility at their next redetermination.
•
All newly eligible children receive an initial span of continuous eligibility as of their initial
eligibility period (excluding assumed periods of retrospective coverage).
11
Once 6-month continuous eligibility is implemented, however, we assume that eligibility determination will happen on a 6month rather than a 12-month cycle.
The Lewin Group, Inc.
Page 14
•
At the end of a period of continuous eligibility, an additional span is awarded if the person
remained Medi-Cal enrolled for an additional two months in the original data. (This assumes
that those individuals who originally were disenrolled from Medi-Cal in the following month
and did not immediately re-enroll had lost eligibility or were unwilling to reapply.)
Otherwise, an additional span was not granted unless and until the child was successfully reenrolled in Medi-Cal.
•
Persons with coverage gaps that are not completely filled by continuous eligibility receive a
new continuous span each time they are re-enrolled in Medi-Cal.
•
There is no limit to the number of continuous eligibility spans a given child can be awarded,
except that no spans are permitted beyond the 19th birthday.
•
While Share-of-Cost (SOC) eligibles will not receive continuous eligibility, the simulation
identified situations where a person would have moved from a non-SOC aid category to an
SOC category, but where continuous eligibility would keep this person in the non-SOC
category. The reduction in months of SOC coverage as a result of this phenomenon were
tracked and factored into the analysis.
Step 3: Count Months of New Eligibility for Each Design Option
The implementation of continuous eligibility was modeled for each child in the 5 percent sample
database, as described above. Once the rules were programmed in Step 2, the following statistics
were tabulated for each month, Aid Category and age cohort.
•
Number of Medi-Cal covered months within the 5 percent sample database in each status
code and age/sex cohort during 1996 and 1997. These figures are summarized below in
Exhibit C and shown in detail in Attachment 2.
Exhibit C: Cumulative Number of Months of Eligibility in Each Age Cohort
Age cohort
1996
1997
•
0-18 Years
1,734,582
1,644,257
0-14 Years
1,505,636
1,422,145
0-6 Years
871,175
799,961
The number of Medi-Cal covered months within the 5 percent sample database under a 6month continuous eligibility option that hypothetically began in January 1996. These figures
are summarized below in Exhibit D and shown by month, status code, and age/sex cohort in
Attachment 3.
Exhibit D: Estimated Cumulative Number of Months of Eligibility in Each Age
Cohort Under 6 Months of Continuous Eligibility
Age cohort
1996
1997
•
0-18 Years
1,781,593
1,731,842
0-14 Years
1,543,527
1,494,042
0-6 Years
895,188
846,027
The number of Medi-Cal covered months within the 5 percent sample database under a 12month continuous eligibility coverage extension that hypothetically began in January 1996.
The Lewin Group, Inc.
Page 15
These figures are presented below in Exhibit E and are shown by month, status code, and
age/sex cohort in Attachment 4.
Exhibit E: Estimated Cumulative Number of Months of Eligibility in Each Age
Cohort Under 12 Months of Continuous Eligibility
Age cohort
1996
1997
•
0-18 Years
1,843,662
1,914,631
0-14 Years
1,594,228
1,642,813
0-6 Years
926,075
934,878
The net change in Medi-Cal covered months in each year (1996 is Year 1 in the simulation;
1997 is Year 2) under continuous eligibility. The detailed net change figures for a 6-month
coverage extension model are shown in Attachment 5. Similar figures for a 12-month
coverage extension model are shown in Attachment 6. Summary figures of the net change
in eligible months are shown on the first page of these attachments. The overall net
eligibility change within the 5 percent sample is presented in Exhibit F. Note that the Year 1
figures represent the start-up phase of continuous eligibility, and that the Year 2 figures
reflect full implementation. The Year 2 figures are most critical to the analysis as they
represent the ongoing annual number of additional months of coverage that continuous
eligibility would create. We would estimate that the number of added months of coverage in
Years 3, 4 and 5 would be closely similar to Year 2, for example (assuming the Medi-Cal
population’s size and distribution by aid category remain fairly stable).
The Lewin Group, Inc.
Page 16
Exhibit F: Net Change in Covered Months in the 5 Percent Sample Due to Continuous
Eligibility
(Figures not yet extrapolated to full Medi-Cal Program)
Net Covered Months
Added, 6-Month Model
Net Covered Months
Added, 12-Month Model
Year 1
< Age 1
Ages 1-6
Ages 7-12
Ages 13-14
Ages 15-18 Male
Ages 15-18 Female
Total
6,586
17,427
10,718
3,160
3,583
5,537
47,011
11,660
43,240
26,200
7,492
8,882
11,576
109,050
Year 2
< Age 1
Ages 1-6
Ages 7-12
Ages 13-14
Ages 15-18 Male
Ages 15-18 Female
Total
10,852
35,214
20,504
5,327
6,683
9,005
87,585
25,829
109,088
68,191
17,560
22,518
27,188
270,374
Age/Sex Cohort & Year
Step 4: Extrapolate 5 Percent Sample to Full Medi-Cal Program
Once the additional coverage months that continuous eligibility would generate for the 5 percent
sample population are estimated, it is necessary to extend this estimate to the full Medi-Cal
population. In creating this extrapolation, the estimate goes beyond simply multiplying the 5
percent sample figures by 20, and takes into account the difference between the size of the base
population in the 5 percent sample and the October 1998 100 percent eligibility file, by age/sex
cohort and aid category. We derived extrapolation factors for Year 1 using the average
distributions in the 1996 5 percent sample file as compared with the October 1998 100 percent
eligibility file, and for Year 2 using the average 1997 distributions. The resulting extrapolation
factors are shown in Attachment 7.
Detailed figures indicating the number of added coverage months created -- by groups of aid
categories (CalWORKS & Related, Disabled, Medically Needy, etc.) and age/sex cohort for each
of the first two years of implementation of continuous eligibility – are shown in Attachment 8
for the 6-month model and in Attachment 9 for the 12-month model. The totals across all aid
category groupings are shown in Exhibit G. The extrapolated numbers are lower than might be
expected because of the decline in the size of the Medi-Cal population between 1996-97 and
October 1998.
The Lewin Group, Inc.
Page 17
Exhibit G: Net Change in Covered Months in Full Medi-Cal Program Due to
Continuous Eligibility*
(Figures reflect estimate for entire Medi-Cal Program, as extrapolated from 5 percent
sample)
Net Coverage Months
Added, 6-Month Model
Net Coverage Months
Added, 12-Month Model
Year 1
< Age 1
Ages 1-6
Ages 7-12
Ages 13-14
Ages 15-18 Male
Ages 15-18 Female
Total
119,250
301,565
212,308
58,790
66,957
94,778
853,648
210,273
748,896
515,314
139,255
169,146
201,295
1,984,179
Year 2
< Age 1
Ages 1-6
Ages 7-12
Ages 13-14
Ages 15-18 Male
Ages 15-18 Female
Total
207,960
650,810
409,576
104,558
130,658
166,803
1,670,365
494,602
2,016,287
1,359,446
343,010
448,066
511,577
5,172,989
Age/Sex Cohort & Year
*Because of the decline in the size of the Medi-Cal population between 1996-97 and October 1998, the number
of recipients in the 5 percent sample is greater than 5 percent of the October 1998 population.
Stage 2: Estimating Medical Costs Per Added Month of Coverage
Once the figures from Step 4 are in hand, the total medical cost impact of continuous eligibility
can be derived by multiplying these added months of coverage by the assumed average monthly
costs per eligible. These per member per month (PMPM) cost estimates are derived in Steps 5
through 7.
Step 5: Identify Applicable Aid Categories (Those Who Would Receive Continuous
Eligibility)
As discussed earlier, most Aid Categories were assumed to be eligible for continuous eligibility.
Only those Aid Categories given a status code of “Excluded” or “SOC” (which denotes Share-ofCost) were deemed ineligible for the continuous eligibility. Virtually all Medi-Cal enrolled
children and adolescents – 99.5 percent of them – were included in the continuous eligibility cost
estimates.
The Lewin Group, Inc.
Page 18
Step 6: Identify Monthly Claims Costs for Selected Population
DHS facilitated Lewin’s modeling by aggregating monthly claims costs during 1997 for each
Medi-Cal eligible under the age of 19. Social security numbers are scrambled in the eligibility
files and claims files to preserve confidentiality, but are scrambled in a manner that still permits
linking monthly eligibility history to all of the individual’s claims.
In deriving per member per month (PMPM) costs, Lewin focused on those persons in the 5
percent sample file who had no periods of managed care enrollment during 1997. Since
capitation payments are not captured in the 5 percent sample files, the managed care population
needs to be excluded from PMPM cost calculations. Of the roughly 140,000 children in the 5
percent sample file, 90,246 persons had only fee-for-service coverage during 1997. This
population is deemed statistically large enough to derive credible PMPM cost estimates. In
addition, an examination of the distribution of the fee-for-service population by county assured
us of the geographic representativeness of this sample as well. Issues regarding managed care
selection bias within geographical areas are addressed in the Sensitivity Analyses section.
This population’s distribution by status code and age/sex cohort is shown in detail in
Attachment 10. The bottom half of Attachment 10 indicates the total months of Medi-Cal
coverage these persons received during 1997. The total 1997 claims costs of this population are
shown in detail in Attachment 11.
The PMPM costs, derived by dividing total costs by months of coverage, are shown in
Attachment 12. The figures in the top half of Attachment 12 depict average monthly costs of
Medi-Cal coverage based on the claims in the 5 percent sample files. Note that dental and some
mental health costs are not included in the 5 percent files because they are not paid through the
DHS claims system. These costs were estimated using other state data sources.
The anticipated PMPM cost of dental services is $10.30 PMPM, as provided by DHS Rate
Setting staff. The anticipated cost of the “missing” mental health services as of 1997 is $6.67
PMPM, derived from information obtained from MRMIB. These costs are incorporated in the
bottom half of Attachment 12. No adjustment is made for dental and mental health services for
persons under age 1, or for persons who have limited benefits (emergency services, pregnancyrelated services, TB-related services, etc.).
Step 7: Estimate Costs of Previously “Uncovered” Months for Fee-For-Service Population
For persons in the fee-for-service setting -- with or without continuous eligibility -- the
uncovered months can confidently be assumed to be lower cost, on average, than the known
covered months. This is because someone who currently requires expensive services, and who
has been eligible for Medi-Cal at a very recent point in time (but is not currently enrolled in
Medi-Cal), is quite likely to become retrospectively eligible once the costly services are
rendered. Costs paid during retrospective periods are captured in the 5 percent sample file; thus
the remaining uncovered months should be lower-than-average cost months in the fee-for-service
setting.
We have therefore assumed that, for persons who receive Medi-Cal coverage at some point
during a given year but who are ineligible at other times during the year, they either:
The Lewin Group, Inc.
Page 19
a) received no inpatient hospital care during uncovered periods; or
b) received inpatient hospital care during an uncovered period and subsequently received
retroactive Medi-Cal coverage for these expensive services.
Inpatient hospital costs were therefore removed from the PMPM costs of additional fee-forservice coverage months. There will be some instances where the extended Medi-Cal coverage
eliminates the need for someone to secure private insurance that was otherwise available to the
individual/family. In such instances, all claims costs – including inpatient costs, would represent
a net added cost. Our approach understates net costs relative to these individuals.
On the other hand, the retrospective coverage periods would pick up more than inpatient
services, and health care usage outside the inpatient arena could also prompt retrospective MediCal eligibility to occur. Our approach of removing only inpatient care overstates net costs for
these individuals.
We elected to make only the inpatient cost adjustment for two reasons. First, the two known
sources of potential error described above influence the results in opposite directions. Our
assumption reflects the middle ground. Second, we felt that the existence of coverage could well
increase the demand for services during uncovered months – and that health care usage might in
fact be more “average” if the uncovered months were in fact covered. Research studies have
also confirmed that usage and costs of covering uninsured persons have not varied greatly from
those of the previously insured population.
To make the adjustment, Lewin identified and removed inpatient costs from the 5 percent sample
and PMPM base applied to the additional enrolled months of fee-for-service Medi-Cal. These
percentages are shown in Attachment 13 and were removed from the PMPM costs as shown in
Attachment 14. The percentage reduction for inpatient services is applied to the 5 percent
sample figures prior to the addition of dental and mental health services.
Step 8: Estimate Costs of Previously “Uncovered” Months for Managed Care Population
Of the 2.6 million children covered by Medi-Cal in October 1998, over 1.5 million (59 percent)
were enrolled in some form of managed care program. Three adjustments to the PMPM cost
estimates for continuous eligibility were considered to account for the growth in managed care
enrollment: (1) savings to the State from managed care; (2) health status differences between the
managed care and fee-for-service populations; and (3) capitation issues related to retrospective
eligibility. These issues were addressed in the manner described below.
First, with regard to managed care savings as compared with fee-for-service costs, our
discussions with State staff indicated that, on average, the capitation rates paid to managed care
plans across the State, including county-organized health systems (COHS), represent about a six
percent savings versus expected fee-for-service costs levels. This intended cost savings is offset
to some degree by the State’s added cost of administering a Medicaid managed care program in
addition to the fee-for-service program. The base scenario assumes that the added administrative
costs of managed care offset the medical savings created by the discounted capitation rates.
Consequently, the fee-for-service PMPM cost estimates derived from the 5 percent sample file
were used directly in the model; no savings factor was applied for the managed care enrolled
The Lewin Group, Inc.
Page 20
portion of the population. Alternative assumptions are assessed in the Sensitivity Analyses
section.
Second, the managed care capitation rates used by the State assume no difference in health status
between the fee-for-service and managed care pediatric populations. For this reason, the fee-forservice PMPM cost estimates derived from the 5 percent sample file were used directly in the
model for both managed care and fee-for-service enrollees. Note that our model adjusts
reasonably well for the distribution of added covered months between disabled children,
medically needy children, and less costly pediatric subgroups.
Third, the State’s capitation rates are not adjusted to remove the high costs of retrospective
coverage months. (Retrospective months are, on average, higher-cost because expensive health
care events such as hospitalizations often trigger the need to apply for retrospective coverage.)
Therefore, the fee-for-service costs as identified in the 5 percent sample file again serve as a
legitimate proxy for HMO capitation rates.
In the base scenario, we have assumed that no net cost difference exists between a managed care
month and a fee-for-service month under continuous eligibility. In other words, each additional
month of coverage in managed care is assumed to impose the same net costs on the State as a
fee-for-service covered month. The capitation rates that exist for a small number of pediatric aid
categories were made available, were analyzed, and supported the notion that the 5 percent
sample files are accurately depicting PMPM costs for Medi-Cal children.
However, we have modeled in detail an alternative approach -- which assumes managed care
months to be higher cost. This analysis is included in the Sensitivity Analyses section and is
used as the high end of the range of “best estimates” that are put forth in this report.
Note that it will be important for DHS to refine its capitation rate structure under continuous
eligibility for two reasons. First, DHS should review its capitation rate setting methodology in
the context of the impact of expected utilization changes under continuous eligibility. The
assumed lower rates of inpatient utilization associated with continuous eligibility should also be
considered in capitation rate setting if continuous eligibility is implemented.
Second, current capitation payments have been developed specific to children only for a few aid
categories. Continuous eligibility would change the age mix considerably. If the additional
months of managed care coverage for children are paid by using an average capitation that
blends in the costs of covering adults in each aid category, DHS will significantly “over-pay” for
the costs of extending continuous coverage explicitly to children since this age group is less
costly than adults. If DHS continues to pay a single rate in each aid category, this rate will need
to be lowered to appropriately reflect the fact that more child and adolescent months of coverage
are being provided. Another option is for DHS to develop distinct capitation rates for children
and adolescents for all aid categories that have large numbers of children/adolescents. We
assume that the capitation payments will be appropriately adjusted to reflect changes in the
underlying population mix in conjunction with the implementation of continuous eligibility.
A final issue to address with regard to managed care is the potential benefit of continuous
eligibility for Medi-Cal health plans. We have estimated the cost impacts purely from the
The Lewin Group, Inc.
Page 21
perspective of the Medi-Cal program. However, the health plans are likely to find that
continuous eligibility provides the following advantages or opportunities for cost savings:
•
Reduced enrollment processing, including the printing and mailing costs associated with
distributing new member packets and membership cards, as well as staff time to conduct
orientation sessions and welcome calls and perform outreach and treatment planning;
•
Reduced disenrollment processing;
•
Greater overall enrollment levels and corresponding revenue streams;
•
Longer average duration of Medi-Cal enrollment, making preventive services and longerrange care management efforts more worthwhile for the plans to invest in. Stable enrollment
could make it easier to provide for and measure quality of care.
Likewise, similar types of benefits are likely to be experienced by primary care providers who
may find the administration of their Medi-Cal managed care panels to be simplified by fewer
enrollments and disenrollments.
It is possible that these advantages to continuous eligibility for health plans could result in some
financial savings to the State. We have not changed the financial projections to include such
potential savings to the State, however. These savings, if they materialized, would probably not
change the net costs of implementing continuous eligibility by more than a percentage point or
two.
Step 9: Trend the PMPM Cost Base
The 1997 PMPM costs were trended forward to Years 1 and 2 of continuous eligibility (2000 and
2001, respectively) using an annual trend factor of five percent. With the large influx of MediCal into capitated programs during the past few years, it has become increasingly difficult to
identify the average rate of increase in PMPM Medi-Cal claims costs. The five percent figure
reflects an approximate mid-point of the trend lines used by DHS in various Medi-Cal rate
development efforts from 1996-1999. Alternative percentage assumptions are discussed in the
Sensitivity Analyses section.
The cumulative trend factor used across the 1997 to 2000 period is 1.158 (5 percent per year,
compounded over three years), and is 1.216 for the period 1997 to 2001 (5 percent per year,
compounded over four years). The trended PMPM costs with inpatient services included are
shown in Attachment 15. Trended PMPM costs with inpatient services excluded are shown in
Attachment 16.
Step 10: Derive Total Design Option Costs
Once the above steps are completed, the medical costs of each design option for continuous
eligibility are readily derived. For any given subgroup of Medi-Cal eligibles, the total cost was
calculated by multiplying the assumed number of additional coverage months (Attachments 8
and 9) by that subgroup’s assumed PMPM cost (Attachment 16).
The Lewin Group, Inc.
Page 22
The results of these calculations for the base scenario are shown in detail in Attachment 17 for a
6-month provision and in Attachment 18 for a 12-month provision. These attachments depict
both the federal and state share of added Medi-Cal costs. The findings are summarized in
Exhibit H.
The Year 2 figures are the most important ones, as these numbers approximate the ongoing
annual costs of continuous eligibility once the program reaches a “steady state” level of
expanded eligibility. The Year 1 figures are much lower because the eligibility-enhancing
impact of continuous eligibility does not fully accumulate until all Medi-Cal recipients have
undergone at least one annual eligibility determination.
The Lewin Group, Inc.
Page 23
Exhibit H: Estimated Added Medi-Cal Costs Under Continuous Eligibility, Federal
and State Share Combined ($ Millions)
6-Month Design Model
Year 1 (2000)
Year 2 (2001)
0-18 Years
$49.2
$100.5
0-14 Years
$33.5
$71.0
0-6 Years
$19.7
$42.3
12-Month Design Model
Year 1 (2000)
Year 2 (2001)
0-18 Years
$113.7
$311.6
0-14 Years
$79.3
$220.7
0-6 Years
$46.0
$127.4
California’s state share of Medi-Cal spending is 48.77 percent. The State of California’s costs
are shown in detail in Attachment 19 for a 6-month design model and in Attachment 20 for a
12-month design model. These State-specific costs are summarized in Exhibit I.
Exhibit I:
Estimated Added Medi-Cal Costs Under Continuous Eligibility, State
Share Only ($ Millions)
6-Month Design Model
Year 1 (2000)
Year 2 (2001)
0-18 Years
$24.0
$49.0
0-14 Years
$16.3
$34.6
0-6 Years
$9.6
$20.6
12-Month Design Model
Year 1 (2000)
Year 2 (2001)
0-18 Years
$55.4
$151.9
0-14 Years
$38.7
$107.6
0-6 Years
$22.4
$62.1
As discussed earlier, the large difference in the relative costs of the two design models is due to
the patterns of eligibility currently observed in the Medi-Cal program. While the 6-month option
is estimated to increase the number of eligible months covered by Medi-Cal at a given point in
time by approximately 140,000, the 12-month option is estimated to increase the number of
covered months by approximately 431,000.
The Lewin Group, Inc.
Page 24
F.
Sensitivity Analyses
It was extremely difficult to arrive at several of the assumptions in the base scenario. To address
the uncertainty inherent in these types of analyses, the following variables were re-visited and
sensitivity analyses were performed using different assumptions than those used in the base
scenario. All sensitivity analyses were performed on Year 2, the key year to assess, and focused
on the State share of increased Medi-Cal costs (as opposed to the combined federal/state share).
It is important to emphasize that all the analyses assume that no changes will be made in the
process by which Medi-Cal eligibility is renewed and redetermined. Many alternative ways of
handling the renewal process have been considered by policy makers (e.g., easing or eliminating
quarterly reporting requirements). To the extent that any such changes are adopted that make it
easier for the Medi-Cal population to retain coverage, Medi-Cal costs will increase, but the net
costs attributable to implementing continuous eligibility could be dramatically lower than the
figures derived throughout this report.
1) Net Managed Care Costs Could be Higher Than Net Fee-For-Service Costs
Additional coverage months will occur in both managed care and fee-for-service (FFS). As of
October 1998, roughly 60 percent of Medi-Cal children were enrolled in a capitated health plan.
The base scenario assumes no difference in net PMPM costs to the State between a fee-forservice month and a managed care month.
As an alternative to the base scenario (called the “maximum managed care impact” scenario), we
assumed that the PMPM costs of additional months of managed care eligibility would be paid at
the full Medi-Cal capitation rates, which include both inpatient and outpatient costs, but that
there would be no offsets in fee-for-service payments except in the case of newborns. For the
under 1 age category, most inpatient costs occur at the time of birth and would not be indicative
of PMPM costs for the remaining months of the first year. The cost estimates reflect this by
using the non-inpatient costs for the under 1 age cohort for all additional months of eligibility
granted due to continuous eligibility. For all other age cohorts, we used the PMPM costs
including inpatient costs. The proportion of additional months assumed to occur in a managed
care setting are equal to the managed care penetration rates, by aid category and age/sex cohort,
reflected in the October 1998 100 percent eligibility file. For those aid category status groups
with managed care enrollment, the penetration rates varied by age/sex cohort (for the over age 1
cohorts) as follows:
CalWorks & Related:
Disabled:
Foster:
Medically Needy:
OBRA:
Pregnant Women:
The Lewin Group, Inc.
66% - 73%
24% - 28%
14% - 19%
50% - 56%
2% - 3%
1% - 2%
Page 25
These alternative assumptions do not change the number or mix of months of added coverage,
but they significantly increase the net costs of continuous eligibility. These changes are shown
in Exhibit J.
Exhibit J: Maximum Managed Care Impact Scenario, Year 2, State Share Only
(All Figures in $ Millions)
6-Month Design Model
Base Scenario
Higher Managed
Care PMPM Costs
% Difference
0-18 Years
$49.0
$57.9
0-14 Years
$34.6
$39.8
0-6 Years
$20.6
$23.9
+18%
+15%
+16%
12-Month Design Model
Base Scenario
Higher Managed
Care PMPM Costs
% Difference
2)
0-18 Years
$151.9
$180.1
0-14 Years
$107.6
$124.5
0-6 Years
$62.1
$72.6
+19%
+16%
+17%
The Number Of Children Accessing Medi-Cal Could Vary From The Base Scenario
Assumptions
The base scenario essentially freezes the number of Medi-Cal children at the levels observed as
of October 1998. Should enrollment of children in Medi-Cal increase (due to enhanced outreach
efforts, simplified application forms, changes in the economy, or other reasons), the costs
attributable to implementing continuous eligibility would increase as well.
Exhibit K shows the results of sensitivity analyses around the number of children covered by
Medi-Cal. If the number of Medi-Cal eligible children in the “CalWORKS and Related” aid
categories were to grow by 10 percent, the costs of continuous eligibility would increase by
roughly 5 percent. We chose this subgroup because it was deemed to reflect the most
comparable children, in terms of PMPM costs, who would potentially be added to the Medi-Cal
rolls as various organizations strive to reach and enroll Medi-Cal eligible children. The
CalWORKS and Related aid categories account for 51 percent of the added coverage months and
47 percent of added Medi-Cal costs in the base scenario. Exhibit K can also be used to model
other estimates of the costs of continuous eligibility should other numbers of additional children
become covered. For example, a 20 percent increase in the CalWORKS population would result
in roughly a 10 percent increase in the net costs of continuous eligibility.
The Lewin Group, Inc.
Page 26
Exhibit K: Impact of CalWORKS Population Growing by 10%, Year 2, State Share
Only (All Figures in $ Millions)
6-Month Design Model
Base Scenario
10% More
CalWORKS
Eligibles
% Difference
0-18 Years
$49.0
$51.0
0-14 Years
$34.6
$36.2
0-6 Years
$20.6
$21.6
+4%
+5%
+5%
12-Month Design Model
Base Scenario
10% More
CalWORKS
Eligibles
% Difference
3)
0-18 Years
$151.9
$159.1
0-14 Years
$107.6
$113.1
0-6 Years
$62.1
$65.1
+5%
+5%
+5%
The PMPM Trend Assumption of 5% Could Be Too High Or Too Low
Given that the PMPM trendline is compounded across multiple years, the cost estimates are
sensitive to the inflation factor that is used. While the 5 percent trend assumed in the base
scenario is a reasonable indicator of expected PMPM cost increases, the impact of using higher
and lower trend estimates was modeled. If the actual slope of PMPM cost increases for MediCal children is only two percent per year, the net costs of continuous eligibility would be 12.3
percent lower than the base scenario in Year 2. Similarly, if the average annual rate of increase
is eight percent, the net costs of continuous eligibility will be 11.9 percent higher than the base
scenario in Year 2.
4)
Managed Care Savings Could Occur Due To Discounted Capitation Rate
While the State’s capitation rates are typically set to reflect 94 percent of expected fee-forservice costs, the base scenario assumes that the added costs to the State of administering a
managed care program (in addition to administering a fee-for-service program) under Medi-Cal
will offset these medical cost savings. Note that the 94 percent figure represents rates in the twoplan model. The percentage of fee-for-service paid is negotiated in other managed care models
but the 94 percent figure is deemed to be a reasonable depiction of the statewide average.
The Lewin Group, Inc.
Page 27
As an alternative assumption, Lewin modeled the assumption that the added administrative costs
associated with managed care will only offset half of the medical cost savings (i.e., net costs in
managed care will be three percent below fee-for-service). For these calculations, the 3 percent
discount was applied to all capitated services, including inpatient care – but was not applied to
carve-out services such as mental health and dental care. Exhibit L indicates that this assumption
produces a net reduction (versus the base scenario) of 2 percent in the costs of continuous
eligibility.
Exhibit L: Managed Care Savings of 3% Assumed, Year 2, State Share Only
(All Figures in $ Millions)
6-Month Design Model
Base Scenario
Lower Managed
Care PMPM Costs
% Difference
0-18 Years
$49.0
$48.0
0-14 Years
$34.6
$33.9
0-6 Years
$20.6
$20.2
-2%
-2%
-2%
12-Month Design Model
Base Scenario
Lower Managed
Care PMPM Costs
% Difference
5)
0-18 Years
$151.9
$148.9
0-14 Years
$107.6
$105.3
0-6 Years
$62.1
$60.8
-2%
-2%
-2%
The Number of Added Coverage Months Could Be Higher Than Base Scenario
As described earlier, Lewin modeled a “worst case scenario” for counting added months of
eligibility detailed in Attachment 1. Under this scenario, the steady state (Year 2) added months
of eligibility granted for ages 0-18 would increase by 42.7 percent for 6-month continuous
eligibility as compared to the base scenario, and by only 13.7 percent for 12-month continuous
eligibility. Because the base scenario adds such a large volume of coverage under the 12-month
option, the worst-case scenario’s assumptions do not further increase coverage by as large a
margin as occurs in the 6-month option.
With regard to added months, the base scenario figures reflect the assumptions we believe to be
most appropriate and realistic – these worst case assumptions are presented simply to convey the
State’s maximum financial exposure in implementing continuous eligibility. These worst case
assumptions are shown in Exhibit M.
The Lewin Group, Inc.
Page 28
Exhibit M: Impact of Using Worst Case Scenario of Additional Months of Coverage,
Year 2, State Share Only (All Figures in $ Millions)
6-Month Design Model
Base Scenario
Worst Case
Scenario
% Difference
0-18 Years
$49.0
$70.1
0-14 Years
$34.6
$49.5
0-6 Years
$20.6
$29.5
+43%
+43%
+43%
12-Month Design Model
Base Scenario
Worst Case
Scenario
% Difference
The Lewin Group, Inc.
0-18 Years
$151.9
$173.2
0-14 Years
$107.6
$122.7
0-6 Years
$62.1
$70.8
+14%
+14%
+14%
Page 29
G. Healthy Families Offsets
The provision of continuous eligibility under Medi-Cal will to some degree reduce the number of
children enrolled in Healthy Families, since some children under age 19 who are granted
continuous eligibility would otherwise move from Medi-Cal to Healthy Families at some point
during the 6- or 12-month continuous eligibility period. However, the offsetting “savings” from
this phenomenon (vis-a-vis the cost estimates shown earlier) are expected to be rather small.
About 94,800 children were enrolled in Healthy Families as of April 1999, and Healthy Families
enrollment has been growing at an average monthly rate of 12,462 over the past six months.
With nearly 100,000 children losing Medi-Cal eligibility each month, clearly very few are
transitioning into Healthy Families. It is also worth noting that the Federal match under Healthy
Families is about 66 percent versus 51 percent in Medi-Cal. Thus, any enrollment that is shifted
from Healthy Families to Medi-Cal due to continuous eligibility will result in a lower Federal
match for those enrolled months, reducing the cost offset attributable to savings in the Healthy
Families program.
The continuous coverage cost adjustment due to Healthy Families is estimated in Exhibit N
below to be $0.7 million for the 6-month design model and $2.5 million for the 12-month design
model.
Exhibit N: Calculation of Healthy Families Offset
Number of added months, Year 2,
CalWORKS & Related aid categories
Percentage of added months assumed to be
covered by Healthy Families
Number of added months assumed to be
otherwise covered by Healthy Families
Average net cost per added month, Year 2
Total cost for added months covered by
Healthy Families
State share under Healthy Families (34%)
6-Month Design
Model
750,744
12-Month Design
Model
2,637,146
5%
5%
37,537
131,857
$54.78
$2,056,277
$55.64
$7,336,523
$699,134
$2,494,418
Note that substituting Medi-Cal coverage for Healthy Families coverage creates a net cost to the
State, due to the higher federal match for Healthy Families (66 percent) versus Medi-Cal (51
percent).
The Lewin Group, Inc.
Page 30
H. Administrative Savings/Costs
Administrative savings and costs are extremely difficult to estimate, since the manner in which
the continuous eligibility option would be administered is uncertain. Issues such as how a “case”
is defined under continuous eligibility could have an enormous financial impact, due to the
existing administrative fees paid to counties. We have sought to frame the issues below and in
some cases present some financial parameters of what the administrative cost impacts might turn
out to be, depending upon the State’s approach.
Savings:
Administrative savings might occur through decreased volume of quarterly reporting. However,
in most instances the head of household will need to continue to submit the same quarterly
reporting as would occur in the absence of continuous eligibility, since continuous eligibility
would not be awarded to adults. The savings from reduced quarterly reporting will only apply to
child-only cases.
Administrative savings might also occur through less need for face-to-face interviews as persons’
coverage gaps are “filled” by continuous eligibility. Again, however, the reduced administrative
costs would apply only to child-only cases where the need for a face-to-face meeting would truly
be eliminated. Roughly 7 percent of the children experienced an eligibility pattern of “on-offon” during 1997 and the intake fee of $119 can add up. However, we anticipate that a minority
of these situations would actually involve elimination of face-to-face meetings. The majority of
Medi-Cal children are not in child-only cases, and it seems that face-to-face meetings would
rarely occur with child-only cases in any event.
Another source of possible administrative savings relates to the Medi-Cal managed care
program. For each child that would otherwise be “on-off-on” of Medi-Cal, continuous eligibility
would reduce the costs of conducting outreach for Medi-Cal managed care plan selection and
enrollment processing. State staff were not able to quantify the per-child costs of Medi-Cal
managed care outreach and enrollment, but depending upon the volume of Medi-Cal enrollment
“cycling” that occurs, the administrative savings could be significant.
Note that guaranteed eligibility for children and adults who are enrolled in managed care is
permitted under the BBA. Further study of the costs of implementing this BBA provision in
some form could uncover greater administrative savings than can occur through implementing
continuous eligibility for children only.
Costs:
Sources of additional administrative costs due to continuous eligibility include:
•
Notwithstanding the avoidance of “intakes” described above, fees paid to counties to handle
eligibility could increase significantly under continuous eligibility. For example, the $21.34
monthly fee paid to counties for each case extrapolates to an annual cost of $96 million under
12-month continuous eligibility, if every added month of coverage is deemed an added “case
The Lewin Group, Inc.
Page 31
month.” The corresponding “worst-case” figure under a 6-month option is $31 million per
year. Such levels of additional administrative spending are obviously not expected, but the
magnitude of these potential costs highlights the importance of avoiding paying $21.34 per
added month when continuous eligibility is in many respects simplifying eligibility.
•
Re-designing system to permit case-splitting, giving children coverage but not adults. This
may lead to systems modification costs by the fiscal agent (EDS), as well as other systemrelated costs.
•
Creating new materials to explain the continuous Medi-Cal eligibility option.
•
Training eligibility workers to administer continuous eligibility, although such additional
training might well be rolled into other ongoing eligibility worker training initiatives and thus
create no net additional costs.
•
Adjusting health plan capitations to reflect a larger proportion of children and adolescents in
the managed care enrollment mix, as well as possible adjustments for the PMPM costs of
providing additional months of coverage for an existing population.
While we have not been able to confidently attach a cost to each administrative component
where net costs or net savings would occur, our opinion is that no net administrative savings are
going to occur for a child-only initiative that does not, in itself, substantially alter the volume and
nature of the Medi-Cal eligibility determination and redetermination processes. Most likely,
there would be a net additional cost to Medi-Cal to administer the continuous eligibility
initiative.
The Lewin Group, Inc.
Page 32
I.
Conclusions and “Best Estimate”
The Lewin Group’s best estimate is that added cost of the various design options for continuous
eligibility would fall somewhere between our base scenario and Sensitivity Analysis #1, in which
managed care months of coverage are assumed to have a higher cost. These ranges are shown in
Exhibit O below. The figures show Year 2, which represents the “steady state” phase of
continuous eligibility implementation and are thus representative of costs in each subsequent
year. Costs during the first year will be significantly lower during the ramping up period.
The low end of the range is derived by using the base scenario figures, less the Healthy Families
offsets (which for all ages are estimated at $0.7 million for the 6-month design option, and $2.5
million for the 12-month design option). The high end of the range is derived by using the
figures from Sensitivity Analysis #1, less the Healthy Families offsets.
Exhibit O: Range of Lewin’s “Best Estimates,” Year 2, State Share Only (All Figures
in $ Millions)
6-Month Design Model
Low End of Range
High End of Range
0-18 Years
$48.3
$57.0
0-14 Years
$34.1
$39.2
0-6 Years
$20.3
$23.5
12-Month Design Model
Low End of Range
High End of Range
0-18 Years
$149.4
$177.2
0-14 Years
$105.8
$122.5
0-6 Years
$61.1
$71.4
As a final note, The Lewin Group wishes to express our appreciation for the detailed assistance
provided throughout the project effort by numerous DHS staff – in promptly providing the data
needed to develop our estimates, in reviewing our initial drafts, and in helping shape the final
revisions.
The Lewin Group, Inc.
Page 33