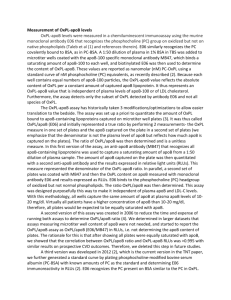
Preparation of Soluble ApolipoproteinsA-I, B, and C
advertisement

CLIN. CHEM. 29/10, 1731-1735 (1983)
Preparation of Soluble ApolipoproteinsA-I, B, and C-Il by a
ChromatofocusingColumn Method, and Evaluation of Their Concentrations
in Serum in Pulmonary Disease
Math Jauhlalnen,1 Math La(tlnen,1Jukka Marnlemi,2Karl Liippo,3Ilkka Penttll#{228},1
and Eino Hietanen4
A chromatofocusing column method for isolating ApoB is
described. LDL is first isolatedby sequential ultracentrifugation and delipidatedwith n-butanol/diisopropytether. Chromatofocusing of Ap0LDL yielded a large ApoB peak at p1
5.0-5.3. ApoA-l and ApoC-li were prepared analogously,
with HDL and VLDL as the source of apoprotein. Antisera
were raised in rabbits, and electroimmunoassay techniques
were used for determination. ApoB was water-soluble after
chromatofocusing. Intra-assay precision (CV) was 4.7% for
ApoA-I, 7.8% for ApoB in the ‘rocket” electrophoresis.
Interassay precision (CV) was 6% for ApoA-l and 8% for
ApoB. Apolipoprotein concentrations were measured in sub-
jects who had undergone lung resectionand patients with
obstructive pulmonary disease. After lung resection, the
concentrationof ApoA-I in serumwas significantlydecreased
(p < 0.001) and that of ApoB significantlyincreased (p <
0.001) as compared with controls. The ApoA-l/ApoB ratio
was significantlylower in the lung-resection group. ApoA-l
and ApoB concentrationswere unchanged in chronic obstructive pulmonary disease. ApoC-lI concentrations in each
group were similar to those for control subjects. Of the lipids,
values for total cholesterol were above normal after lung
resection(p < 0.002), as were those for triglycerides (p <
0.02).
AddItIonalKeyphrases:lung resection
chronic obstructive pulmonary disease
electroimmunoassay standardization
cholesterol
triglycerides . “rocket” immunoelectrophoresis
The liver and intestine
evidently
are the main sites of
synthesis of apolipoproteins
and formation of lipoprotein
particles (1). Normal synthesis of apolipoproteins is essential for the formation of these particles. ApoB5 appears to be
necessary
for the transport
of triglycerides from liver and
intestine, and ApoB-containing
lipoproteins can be viewed
as the transport
medium
for plasma triglycerides
(2). Tnacylglycerols are transported
in the blood in large particles,
mainly in chylomicrons
and very-low-density
lipoproteins
(VLDL) (3,4). The triacylglycerols within these particles are
hydrolyzed by lipoprotein lipase (LPL; EC 3.1.1.34) in such
extrahepatic tissues as adipose tissue, muscle, and lung (5).
This enzyme is activated by a peptide, apolipoprotein C-il
(ApoC-il) (6). For normal lipoprotein metabolism the reac‘Department
of Clinical Chemistry, Alava Hospital Laboratory,
Kaartokatu
9 70620 Kuopio 62, Finland.
2The Rehabilitation Research Centre of the Social Insurance
Institution, Turku, Finland.
‘Department
Finland.
4Department
Nonstandard
of Diseases
of Physiology,
of the Chest, University
University
of Turku,
of Turku, Finland.
abbreviations: Ape, apolipoprotein; LPL, lipopro-
tam lipase; VLDL, very-low-density
lipoprotein;
LCAT, lecithin:
cholesterol acyltransferase; HDL, high-density lipoprotemn; LDL,
low-density lipoprotein; d, relative density (specific gravity).
Received April 25, 1983; accepted June 20, 1983.
tion catalyzed
by lecithin:cholesterol
acyltransferase
(LCAT; EC 2.3.1.43) is essential. Apolipoprotein A-I (ApoA1) is its specific cofactor and is the main structural protein in
HDL (7). Determination
of ApoB or the ratio ApoA-IJB can
perhaps be used to evaluate the risk for atherosclerosis (8).
There are few reports concerning different pulmonary
diseases and lipid metabolism. The pulmonary capillary bed
is the first large endothelial surface with which chylomicrons come in contact after their secretion into the plasma
compartment. In addition to respiration and a role in the
regulation of steroid metabolism (9-11), synthesis of the
surface-active material that lines the alveoli is an essential
function of lung tissue (12). In addition to taking part in the
synthesis of surfactant, pulmonary LPL may act to remove
accumulated
triglyceride-rich
particles from the lungs in
cases of fat embolism (14); LPL activities increase in both
serum and lung during experimental
fat embolism (15).
We describe here a chromatofocusing method for isolating
soluble ApoB from the LDL fraction. In addition, electroimmunoassay standardization is described
for it and ApoA-I.
Furthermore, we have measured different lipids, ApoA-I,
ApoB, ApoC-il, and enzyme activities in subjects with lung
resection and in patients with chronic obstructive pulmonary disease to see if these impaired lung functions
have
any effect on these variables.
Materials and Methods
Subjects
Patients.
We studied 15 patients who had had lung
resection: four women, ages 49 to 63 years, and 11 men, ages
51 to 69 years. The obstructive-disease
group consisted of
eight men, ages 43 to 63 years.
Controls.
The control group consisted of 35 persons: 21
men, ages 25 to43y,
and 14 women, ages 25 to 38 years.
None had any history of lung disease. They were selected
without conscious bias from the staff and clients of the
Rehabilitation
Research Centre of the Social Insurance
Institution, Turku.
Procedures
Preparation
of lipoproteins.
All lipoprotein fractions were
isolated by ultracentrifugal
flotation in a Kontron TGA 65
ultracentrifuge.
The centrifugations
were performed
at 8#{176}C
for 18 h at 105 000 x g (16). Densities were adjusted with
KBr. VLDL were isolated by ultracentrifugation
of pooled
normolipemic sara at d = 1.006. After centrifugation,
VLDL
were refloated at d = 1.006, with use of NaCl solution to
remove contaminating proteins. This fraction was used for
ApoC-il isolation (17). LDL and HDL were isolated at d =
1.063 and 1.210, respectively. These fractions were also
washed at appropriate densities.
Lipoprotein fractions were delipidated by a method modified from Cham and Knowles (18). The extraction mixture
consisted of n-butanolldiisopropyl
ether (1:2 by vol), with
extraction at room temperature. After a 1-h extraction, two
CLINICALCHEMISTRY, Vol. 29, No. 10, 1983 1731
additional
extractions
were carried out with diisopropyl
The curve for ApoB was slightly curvilinear and the calibraether. The residual ether was removed at 37 #{176}C,
under
tion curves for the assay were used in the concentration
reduced pressure.
range 0.4-2.5 g of ApoB per liter of serum (r = 0.981, for the
whole range, including curvilinearity).
The nonlinear reIsolation
of apolipoproteins
A-I, B, and C-H. ApoA-I,
ApoB, and ApoC-il were fractionated by a chromatofocusing
gion was omitted.
The intra-assay CVs calculated
from
measurements
on 10 samples of pooled serum were 4.7% for
method (19). The source of ApoA-I was apoHDL, and A-I
was eluted at p1 7.7, as described earlier (20). When delipiApoA-I and 7.8% for ApoB. Corresponding interassay values
dated LDL (apoLDL) was chromatofocused,
the column was
were 6% for ApoA-I, 8% for ApoB.
Lipid
analysis.
Venous blood for serum analysis was
equilibrated
with imidazole hydrochloride (35 mmol/L, pH
sampled the morning after an overnight fast. Concentra7.7) containing, per liter, 3 mol of urea and 5 mL of Triton Xtions of total cholesterol, free cholesterol, and triglycerides
100 surfactant.
ApoLDL (50 mg) was eluted with pH 4.1
in the serum was measured by enzymatic assays (Boeh‘Polybuffer 74 HC1” (Pharmacia
Fine Chemicals, Uppsala,
ringer Mannheim GmbH, Mannheim, F.R.G.). HDL-cholesSweden) diluted sixfold with distilled water containing 3
mol of urea and 5 mL of Triton X-100 per liter. After elution,
terol was measured enzymatically
after VLDL and LDL
fractions corresponding to the ApoB peak were dialyzed
were precipitated with dextran sulfate/MgC12 (25).
overnight against a pH 7.4 solution containing, per liter, 10
Results
mmol of Tnis, 100 mmol of NaCl, 10 mmol of NaN3, and 100
mg of EDTA, then for 30 h against distilled water. The
Isolation of Apoprotein B
dialyzed
fractions were lyophilized and stored at -80 #{176}C.
We found the modified chromatofocusing
column techApoC-il was fractionated from apoVLDL as detailed elsenique to be suitable for fractionating ApoB as well as ApoAwhere (17). Homogeneity
of all apoproteins used in this
I and ApoC-il (17,20).
ApoB eluted in the p1 range 5.0-5.3
study was checked by polyacrylamide gel electrophoresis in
(Figure 1), and this large peak had two shoulders
(11-i and
SDS and urea (21), by a modified Laemmli discontinuous
11-2). Two other peaks eluted, just at the beginning of the
buffer system (22), and by double immunodiffusion
techrun (p1 7.6) and during salt elution (peaks I and ifi). These
niques with use of specific antisera
raised against
each
protein fractions did not react with the antiserum to fraction
apoprotein.
il. The proteins represented by the shoulders il-i and 11-2
Preparation
of antisera. Antiserum against ApoC-Il was
gave a slight reaction with this antiserum.
prepared as described elsewhere (17). Anti-ApoA-I and antiApoB were prepared in New Zealand White rabbits. The
Electroimmunoassay of ApoA-l and ApoB
purified proteins, dissolved in sterile isotonic saline and
Figures 2 and 3 show standard
curves for the ApoA-I and
mixed with equal volumes of Freund’s complete adjuvant,
were injected into the upper back of rabbits. Three booster
ApoB electroimmunoassay.
When the standard curves were
injections were given at intervals of four weeks, again with
constructed with pooled serum containing known amounts
the proteins solubilized in saline and mixed with incomplete
of ApoA-I and ApoB, the reactions with antisera were
adjuvant. With this schedule, rabbits produced precipitating
similar and the curves were parallel.
antibodies of sufficient titer. Antisera to ApoA-I, ApoB, and
The temperature
at which the secondary standard
is
ApoC-il were found to be specific, as judged from double
stored is critical. ApoB values significantly declined, from
immunodifluision according to Ouchterlony (23).
820 to 650 mg of ApoB per liter, within two months when
Electroimmunoassay
of apoproteins.
ApoC-Il rocket electhe standard
was preserved at -20 #{176}C.
The decline began
trophoresis was performed as described earlier (17). ApoA-I
after one month of storage, until which time ApoA-I and
and ApoB concentrations were determined by quantitative
ApoC-il values did not change. This effect was not found
when storage was at -80 #{176}C.
immunoelectrophoresis
according to Laurell (24). Antiserum concentrations
were 5 pL/mL of gel for ApoA-I and 7.5
ApoA-I, ApoB, and ApoC-Il in Controls and Patient
4JmL of gel for ApoB. Agarose, 10 g/L of barbital buffer (10
Groups
mmol/L, pH 8.7, ionic strength 0.02) containing, per liter, 70
mmol of glycine and 40 mmol of Tris, was the best combinaApoprotein concentrations
are presented in Figure 4.
tion for quantifring both ApoA-I and ApoB. Wells 4 mm in
ApoA-I concentration was significantly lower in lung-resecdiameter were filled with 10 L of serum diluted with buffer
tion patients, the concentrations being about 68 and 72% of
containing 10 mL of Triton X-100 per liter, 50-fold for ApoAthe values for the obstructive-disease
and control groups,
I and 30-fold for ApoB determination. Electrophoresis was
for 2.5 h in the case of ApoA-I, 3.5 h for ApoB. The slides
05
[ii
were then blotted, thoroughly washed in saline, dried, and
stained with Blau R (Serva, Heidelberg, F.R.G.). The basic
calibration curves were constructed with purified apopro:t
80
teins dissolved in electroimmunoassay
buffer. Pooled nor03
mal serum, for which the ApoA-I and B concentrations had
70
previously been established by electnoimmunoassay
against
3 02
50
ApoA-I and B reference material prepared as described
50
above, was used for secondary calibration (1:30, 1:40, 1:60,
00
‘.‘-ui.-&_
and 1:80 dilutions for.ApoA-I; 1:10, 1:20, 1:30, and 1:40
L.’
dilutions for ApoB). Pooled serum was frozen batchwise at
0
30
30
CO
50
88
-80#{176}C.
Frohon
No
To expose antigenic determinants of ApoA-I and ApoB,
Fig. 1. Chromatofocusing of delipidated apoLDL in a bead-formed
polybuffer (PBE 94; Pharmacia, Uppsala, Sweden) exchanger gel
we used 10 mL of Triton X-100 per liter in the barbital
column
sample diluent. This slightly increased the measured ApoAColumn bed height 32 cm, diameter1 cm. Sample volume: 5 mL containing 50
I and ApoB content and improved the shapes of the rockets.
mg of apoLDL. Elution rate: 25 mLJh. 5-mL fractions were collected, with
The curve was linear over the range 0.6-2.4 g of ApoA-I per
continuous measurement of absorbance at 280 nm and of pH. Salt elution begun
liter of serum (r, the coefficient of regression, was 0.996).
at point indicated by aimw and S (NaCI, 1 mol/L)
DC
._-‘
/\
-
-
#{176}
:0
.,/,
1732
CLINICAL CHEMISTRY,
Vol. 29, No. 10, 1983
40
perimental
groups. As compared with the control group
(Figure 5), the lung-resection
group had higher cholesterol
(p <0.002) and triglyceride (p < 0.02) concentrations.
There
were no differences in these lipid values between chronic
obstructive
patients
and controls. HDL-cholesterol
showed a
tendency to be higher in the obstructive-disease
group than
in the lung-resection
group. HDL-cholesterol
values did not
differ between the lung-resection
group and controls.
30
E
E
ci
a 20
DIscussion
a,
U
0
10
2.0
1.0
Apotipoprotein
3.0
A-I
5.0
4.0
(mg/lOOmLl
Fig. 2. Relation between rocket height and ApoA-l content of purified
ApoA-I(X) and secondary standard (0)
The regressionequationrefers to the curvemade with purified
ApoA-l(X).Insert:
typical
patternsfor different concentrations
of ApoA-l standards (the first four
rocketsat the left
side for secondarystandard,and the othertourrocketsfor
purified ApoA-l)
40
-
30
-
E
E
a’
U
0
yo2.468
0.9846
20
10
2.16
-
-
2.5
5.0
10.0
15.0
Apolipoprotein
B (mg/lOOmL)
Fig. 3. Standard curve for ApoBelectrolmmunoassay
The two curves were constructed with a purified ApoB (X) and a secondary
standard (0). The regressionequation refers to the upper curve (X). The insert
rockets made either with purified protein (the four
rockets on the left) or with a secondary standard (the other three rockets)
showspatternsof typical
(p < 0.001 in both cases). ApoB was clearly
increased in the lung-resection
group, by about 28% as
compared with the obstructive-disease
group (p < 0.02) and
38% compared
with controls (p < 0.001). The ApoA-JJApoB
ratio showed a good discrimination
between controls, obstructive disease, and the lung-resection group (controls vs
resection group, p < 0.001; chronic obstructive
group vs
resection group, p < 0.002). Total serum ApoC-il concentrations in the 15 lung-resection
patients were statistically
no
different from the other two groups.
respectively
Lipid Analysis
Figure 5 depicts the total cholesterol, free cholesterol,
HDL-cholesterol,
and triglyceride concentrations
in the ex-
Many different techniques
have been applied to obtain
purified apolipoproteins
from lipoprotein fractions, the most
common probably being gel filtration
and ion-exchange
chromatography
(26,27). However, these methods are quite
laborious and time consuming. As earlier reported (19,20),
the chromatofocusing
technique is useful for apoVLDL and
apoHDL fractionation. When delipidated apoLDL was chromatofocused
with detergent in the elution buffer, the fraction containing
ApoB maintained
its water-solubility
after
lyophilization
and also was soluble in electroimmunoassay
buffer (pH 8.7). In addition, with different apoLDL preparations the principal soluble ApoB peak repeatedly appeared
in the same pH range. The insolubility
of this protein in
water after isolation is certainly
the main reason for the
slow progress in elucidating its primary structure
or its use
for method standardization
(28,29). In the solution, protein
precipitation
was noticed if the pH was <8.0. This pHdependence of ApoB precipitation varies with the detergent
used. A DEAE-Sepharose
column method (30) also yields
apoLDL that is water soluble.
Immunochemical
quantitation procedures
demand that,
in the assay system being used, the antigen in the test
samples must behave identically with the standard
samples
(31). In this study, standardization of our pool Serum against
different ApoA-I and ApoB preparations gave reproducible
results, and the rockets formed by ApoA-I and serum and by
ApoB and serum had the same shape. This agrees well with
earlier results for ApoA-I (32, 33). Of all the apoproteins,
standardization of ApoB has been one of the most difficult.
Several methods have used earlier to isolate LDL preparations for quantification of ApoB (34, 35). However, during
storage at either 4#{176}C
or -20 #{176}C
solutions of LDL reportedly
(36) became opalescent, precipitate formed, and there was
loss of ApoB immunoreactivity.
Using plasma samples,
Havekes (36) found ApoB immunoreactivity
to be constant
at 4#{176}C
or -20 #{176}C
for at least 80 days, which accords well
with our observations. We found that pooled serum containing known amounts of ApoB as the assay standard could be
stored at -80 #{176}C
with no change in immunoreactivity
for six
months.
The linear concentration ranges used for ApoA-I and
ApoB assays in this study agree well with recently published values; the range reported
for ApoA-I was 0.75-3.90
g/L (33) and for ApoB 0.50-2.40
g/L (35) and 0.55-2.10 g/L
(37).
For the patient
with lung resection
we found
ApoA-I and significantly
greater
ApoB concentrations
as compared with controls. Earlier,
workers found significant
decreases
of ApoA-I and HDLcholesterol concentrations
during peripheral
vascular disease (38). In the lung-resection
group HDL-cholesterol
was
unchanged. There appear to be at least two ApoA-containing particle populations in the HDL fraction (39). Possibly
ApoA-I-containing
particles decrease relatively more than
HDL-cholesterol
after lung-resection.
Furthermore,
because
the lung-resection
group had high triglyceride
concentrations, the fractional catabolism
of ApoA-I might be enhanced (40). Reportedly,
the best differentiation
between
significantly
group
diminished
CLINICAL CHEMISTRY, Vol. 29, No. 10, 1983
1733
2
-
.
90
#{149}
80
3
70
if
-j
-j
0
2
0
0.
0
0.
..
50
40
:t
#{149}
30
*
4
4
60
4-
S
a’
4
#{149}
______
‘I..
8
p<
1
.8..
--
20
0.001’ p< 0.02”
p< 0.001
p<0.002
p>0.05
10
p>0.05”
C
E
0
C
E
0
C
E
0
C
E
0
Fig. 4. Left to right:Apolipoprotein A-I, B, A-I/B, and C-Il values in serum ofcontrols(C),lung-resectiongroup (E), and chronic-obstruction
cases (C)
Resection (p’) values
arecomparedwithcontrols,
and chronic-obstruction (p”) values
arecomparedwiththeresection-group. Therewerenotstatistically significant
differences between controls and obstructive-disease patients
10
3.
3.
3
#{149}
9
6
-,
-J
E
67
6
.
.
.
,
6
E
E2
62
0
-4
U)
a
-
01
>
cl
1
0
±1
#{149}
0
0
0
<0002
C
Fig.
p>0.O5
E
5. Left to right: Total
p>O.05
C
0
cholesterol,
obstructive-disease patients
(C)
E
p>0.05
p>005’
‘
E
0
p>0.05”
p<0.02
C
0
E
p>0.05
0
free cholesterol, HDL-cholesterol, and tnglycerides in controls(C), lung-resection group (E) and chronic-
The statistical significances (p” and p#{176})
are compared as in Rgure4
normal individuals
and atherosclerotic
patients can be
obtained by use of the ApoB and ApoA-J/B ratio (8,29). Thus
the lung-resection
group may have an increased
risk for
atherosclerotic
vascular
changes.
A recent report claims that patients
with chronic expiratory airflow obstruction
and increased work of breathing
also have higher HDL-cholesterol
concentrations
(41), but
our study does not confirm this.
The LPL activator ApoC-Il concentrations
did not differ in
the two groups of patients as compared with controls,
although the triglyceride concentration was increased in the
resection group. In addition LPL activity was the same in
each group. Carlson and Ballantyne (42) observed that the
ApoC-HJC-ffl ratio of d < 1.006 lipoproteins was lower in
patients with hypertriglyceridemia
than in normotriglyceridemic subjects. Perhaps, after lung resection, synthesis of
LPL activator
protein is less than that of LPL inhibitor
protein (ApoC-ifi) (5), and this may affect pulmonary LPL
activity and facilitate slightly higher triglyceride concentrations.
References
1. Jackson RL, Morrisett JD, Gotto AM. Lipoprotein structure and
metabolism. Physiol Rev 56, 259-316 (1976).
2. Herbert PN, Gotto AM, Fredrickson DS. Familial lipoprotein
deficiency. In The Metabolic Basis of Inherited Disease, 4th ed., JB
Stanbury, JB Wyngaarden, 1)8 Fredrickson, Eds., McGraw-Hill,
New York, NY, 1978, pp 544-588.
3. Eisenberg S. Levy RI. Lipoprotein metabolism. Adu Lipid Res
13, 1-89 (1975).
4. Have! RJ. Lipoprotem
37-59 (1975).
and lipid transport. Ada Exp Med Biol 63,
1134 CLINICALCHEMISTRY, Vol. 29, No. 10, 1983
5. Have! RJ, Fielding CJ, Olivecrona T, et al. Co-factor activity of
protein components of human very low density lipoproteins in the
hydrolysis
of triglycerides
by lipoprotein
lipase from different
sources. Biochemist,y 12, 1828-1833 (1973).
6. Krause RM, Herbert PN, Levy RI, Fredrickson
DS. Further
observations on the activation and inhibition of lipoprotein lipase
by apolipoproteins. Circ Res 23, 403-411 (1973).
7. Fielding PE, Fielding CJ. A cholesterol ester transfer complex in
human plasma. Proc Nati Acad Sci USA 77, 3327-3330 (1980).
8. Fruchart JC, Parra H, Cachera C, et al. Lipoproteins, apolipoproteins and coronary artery disease. Ric Clin Lab 12,101-106(1982).
9. Heinemann UO, Fishman AP. Nonrespiratory
functions of
mammalian lung. Physiol Rev 49, 1-47 (1969).
10. Hartiala J. Studies on pulmonary testosterone
metabolism.
Dissertation, University of Turku, Finland, 1976, pp 1-65.
11. Aitio A, Hartiala J, Uotila P. Glucuronide synthesis in the
isolated perfused rat lung. Biochem Pharmacol 25, 1919-1920
(1976).
12. Abe M, Akino T. Comparison of metabolic heterogeneity of
glycerolipids in rat lung and liver. Tohoku JExp Med 106,343-355
(1972).
13. Naimark A. Cellular dynamics and lipid metabolism in the
lung. Fed Proc Fed Am Soc Exp Blot 32, 1967-1971 (1973).
14. Dimant J, Shafrir E. Lipase activities in the lungs of rats
subjected to experimental hypertriglyceridemia and lung embolism.
Isr J Med Sci 10, 1551-1557 (1974).
15. Armstrong HJ, Kuenzig MC, Peltier LF. Lung lipase levels in
normal rats and treated with experimentally produced fat embolism. Proc Soc Exp Blot Med 124, 959-964 (1976).
16. Carbon K. Lipoprotein fractionation. J Clin Pathol 26, 32-37
(1973).
17. Jauhiainen
M, Laitinen M, Penttila I, et al. Determination of
human apolipoprotein
C-il by electroimmunoassay.
Studies on
standardization
and determination before and after physical train.
ing. mt i Biochem 15, 501-506 (1983).
18. Chain BE, Knowles BR. A solvent system for delipidation of
plasma or serum without protein precipitation. JLipidRes
17, 176181 (1976).
19. Jauhiainen
M. Fractionation of apolipoprotein from human
serum very low density lipoproteins by chromatofocusing.
Int J
Biochem 14, 415-420 (1982).
20. Jauhiainen
MS, Laitinen MV, Penttila IM, Puhakainen EV.
Separation of the apoprotein components of human serum high
density lipoprotein: Chromatofocusing,
a new simple technique.
Clin Chim Acta 122, 85-91 (1982).
21. Swank RT, Munkres KD. Molecular weight analysis of oligopeptides by electrophoresis in polyacrylamide gel with sodium
dodecyl sulfate. Anal Biochem 39, 462-477 (1971).
22. Laemmli UK, Favre M. Maturation of the head of bacteriophage T4. J Mol Blot 80, 575-599 (1973).
23. Ouchterlony C).Antigen-antibody
reactions in gels. VI. Types of
reactions in coordinated systems of diffusion. Acta Pathol Microbiol
Scand 32, 231-235
(1953).
24. Laurell CB. Quantitative estimation of proteins by electrophoresis in agarose gel containing antibodies. AnalBiochem
15,45-52
(1966).
25. Koetner GM. Enzymatic determination of cholesterol in highdensity lipoprotein fractions prepared by polyanion precipitation.
Clin Chem 22, 695-699 (1976).
26. Levy RI, Blum CB, Schaefer EJ. The composition, structure and
metabolism of high density lipoproteins. In Lipoprotein Metabolism,
H Greten, Ed., Springer-Verlag, Berlin, 1976, pp 56-64.
27. Schaefer EJ, Eisenberg 5, Levy RI. Lipoprotein apoprotein
metabolism. J Lipid Res 19, 667-687 (1978).
28. Shireman R, Kilgore IL, Fisher WR. Solubilization of apolipoprotein B and its specific binding by the cellular receptor for low
density lipoprotein. Proc Natl Acad Sd USA 74, 5150-5154(1977).
29. Koatner GM. Current methods for apolipoprotein evaluation in
normal and dyslipoproteinemic plasma. Ric Clin Lab 12, 155-161
(1982).
30. Soccoro L, Camejo G. Preparation
and properties of soluble,
immunoreactive apoLDL. J Lipid Res 20, 631-638 (1979).
31. Munscher G, Metzmann E, Ziegenbein W. Standardization of
immunochemical
apolipoprotein quantitation. Ric Clin Lab 12,
143-154 (1982).
G, Wiklund 0, Olofsson S-O, et al. Quantitation
of
human serum apolipoprotein A-I by electroimmunoassay. Studies
on some techniques for standardization
of the assay and determination of serum apolipoprotein A-I levels in a random population
sample of middle-aged men. Scand J Clin Lab Invest 40, 451-460
32. Fager
(1982).
33. Shapiro D, Ballantyne FC, Shepherd
onephelometry and electroimmunoassay
apolipoprotein A-I. Clin Chim Acta 103,
34. Reardon MF, Poapat ME, Uffelinan
J. Comparison of inunun-
for estimation of plasma
7-13 (1980).
KD, Steiner G. Improved
method for quantitation of B apoprotein in plasma lipoproteins by
electroimmunoassay. Clin C/tern 27, 892-895 (1981).
35. Rosseneu M, Vinaimont N, Vercaemst R, et al. Standardization
of inununoassay for the quantitation of plasma apoB protein. Anal
Biochem 116, 204-210 (1981).
36. Havekes L. Apparent loss of apolipoprotein B immunoreactivity of isolated low density lipoprotein during storage: Consequences
for the quantification of apolipoprotein B in human plasma. Clin
Chim Acta 116, 131-135 (1981).
37. Fruchart JC, Kora I, Cachera C, et al. Simultaneous measure-
ment of plasma apolipoproteins A-I and B by electroinununoassay.
Clin Chem 28, 59-62 (1982).
38. Bradley DD, Wingerd J, Petitti DB, et al. Serum high density
lipoprotein cholesterol in women using oral contraceptives, estrogens, and progestins. N Engi J Med 299. 17-20 (1978).
39. Atmeh RF, Shepherd J, Packard C.J.Subpopulations of apolipoprotein A-I in human high-density lipoproteins. Their metabolic
properties and response to drug therapy. Biochim Biophys Acta 751,
175-188 (1983).
40. Fidge N, Nestel P, Ishikawa T, et al. Turnover of apoproteins Aland A-il of human high density lipoprotein and the relationship to
other lipoproteins in normal and hyperlipidemic individuals. Metabolism 29, 643-653 (1980).
41. Tisi GM, Conrique A, Barrett-Connor E, Grundy SM. Increased
high density lipoprotein cholesterol in obstructive pulmonary dieease (predominant emphysematous type). Metabolism 30, 340-346
(1981).
42. Carlson LA, Ballantyne D. Changing relative proportion of
apolipoprotein C-il and C-rn of very low density lipoproteins in
hypertriglyceridemia. Atherosclerosis 23, 563-568 (1976).
CLINICALCHEMISTRY, Vol. 29, No. 10. 1983
1135

![Anti-Apolipoprotein B antibody [1605] ab20839 Product datasheet Overview Product name](http://s2.studylib.net/store/data/013579967_1-b32c8c251707bf7f1e09c69ff1411cf4-300x300.png)