- Wiley Online Library
advertisement

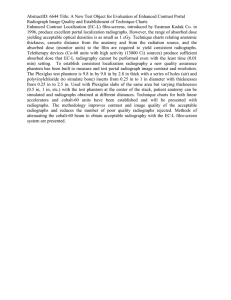
Australian Dental Journal 2009; 54:(1 Suppl): S27–S43 doi: 10.1111/j.1834-7819.2009.01141.x Radiographs in periodontal disease diagnosis and management EF Corbet,* DKL Ho,* SML Lai* *Periodontology, Faculty of Dentistry, The University of Hong Kong. ABSTRACT Radiographs are an integral component of a periodontal assessment for those with clinical evidence of periodontal destruction. A close consideration of the current approach to periodontal diagnosis compatible with the current classification of periodontal diseases reveals that radiographs only inform with respect to diagnosis for a small proportion of conditions. The area in periodontal assessment in which radiographs play a pivotal role is in treatment planning. A variety of radiographic exposure types assist in the development of periodontal treatment plans. This ‘‘therapeutic yield’’ can be achieved by panoramic oral radiographs supplemented by selective intra-oral views. Digital panoramic oral radiographs viewed on screen appear to offer advantages over printouts or films. Newer imaging approaches, such as cone-beam computed (digital volume) tomography, may come to show some usefulness but experience has shown that digital subtraction radiography will probably remain a research tool without much clinical application. Keywords: Radiographs, periodontitis, diagnosis, treatment, imaging. Abbreviations and acronyms: CADIA = computer-assisted densitometric image analysis; CEJ = cemento-enamel junction; CT = computed tomography; DSR = digital subtraction radiography; DVT = digital volume tomography; GTR = guided tissue regeneration. INTRODUCTION It is generally widely accepted that radiographs supplement clinical examination in establishing the diagnosis and guiding the treatment plan for a patient affected by those periodontal diseases which have contributed to destruction of the periodontal attachment. A range of findings of relevance to clinically evident periodontal conditions can become apparent on radiographs. Radiographs can provide key information of relevance to periodontal decision making which is not capable of being captured by clinical examination, such as length of root(s) with remaining bony support. Published reviews on radiographs and imaging in periodontology this decade – 2000 onwards There have been at least four previous reviews on radiographs and imaging in periodontology since the turn of this century. Each of these reviews has had a different emphasis and each will be introduced briefly. Each review rewards careful study and each has taken a different approach to this topic. ª 2009 Australian Dental Association Tugnait and colleagues1 in 2000 reviewed the usefulness of radiographs in diagnosis and management of periodontal diseases. Their review aimed to cover periodontally significant diagnostic information obtainable from conventional radiography and to consider how, with respect to periodontal therapy, radiographs may influence patient management. The studies reviewed were selected on the basis of offering information on the role of radiographs in the diagnosis of periodontal diseases and in guiding management of periodontal diseases at various stages of treatment. Furthermore, evidence for the value added by the viewing of radiographs was critically reviewed. That review concluded that various features of periodontal diagnostic interest are apparent on radiographs, that the visualization of these may be dependent on the radiographic view chosen, that a relationship exists between clinical attachment and radiographic bone height, and that radiographs can be used in all stages of periodontal care, although some decisions may be made following clinical assessment only. That thought provoking review, however, noted that any evidence of the benefit gained from radiographs taken for periodontal patients was, up to the year 2000, sparse. Further, the S27 EF Corbet et al. literature reviewed poorly addressed the extent to which radiographs influenced treatment decisions and treatment outcomes. The authors concluded that clinicians should critically appraise the traditional role of radiographs in the diagnosis and management of periodontal disease to ensure that all radiographs do indeed provide clearly defined benefits to patients. Hausmann2 in 2000 reviewed radiographs and digital imaging in periodontal practice. Hausmann’s review first considered the terminologies ‘‘accuracy’’ and ‘‘reproducibility’’ in imaging, and covered how to produce standardized X-radiographs and how to manage serial X-radiographs once these have been digitized. Then he considered what alveolar bone height indicated no bone loss, taken as 1.9 mm from the cementoenamel junction (CEJ) in molar sites on bitewing radiographs3 and what cut-off can be used to indicate a change in alveolar bone height, taken as 0.71 mm for routine paralleling periapical radiographs.4 He noted the correlation between the radiographic bone height and clinical attachment level and then dealt with methods of digital image subtraction and considered what investigations such approaches may allow for. He concluded his review optimistically by forecasting that linear radiographic measurements of digitized and computer managed images, rather than just visual inspection of radiographs, will in the not-too-distant future, measured from the year 2000, be commonplace in the management of patients with periodontal diseases. He noted that subtraction radiography (being able to tell differences in structures recorded between one standardized digital or digitized radiograph and another) could be of great use to the practising periodontist. Mol5 in 2004 extensively reviewed imaging methods in periodontology covering why and when to use the following imaging: intra-oral and extra-oral radiography, digital radiography, digital subtraction radiography, computed tomography (CT) and ‘‘new frontier’’ imaging including cone-beam CT. In considering ‘‘where do we go from here?’’, Mol notes that the digital era is in its infancy but that current non-digital approaches to handling radiographic images can be improved upon, nonetheless concluding that there is little doubt that periodontists of the future will be using more advanced imaging modalities. Tugnait and Carmichael6 in 2005 reviewed the use of radiographs in the diagnosis of periodontal disease. That review, written basically for general practitioners, had as a focus the selection of radiographs following clinical examination and taken only on the basis of clinical findings, noting that each exposure should be justified. Bragger,7 also in 2005, reviewed radiographic parameters, their biological significance and clinical use. His review considered conventional versus digital S28 imaging methods, the radiographic parameters obtainable in daily practice – linear measurements from landmarks to alveolar bone crest and tooth and root lengths, angular defects, defect angles, furcation radiolucencies – noting the influence of methodological errors. Bragger considered the perception of biological processes which can be derived from radiographic images and dealt in some detail with the clinical use of radiographs, reviewing the role that radiographs have in establishing a periodontal diagnosis, creating a treatment plan, estimating disease risk, and documenting tissue stability, breakdown or remodelling. He noted that image processing, such as digital subtraction, is a pure research tool, a different conclusion to that of Hausmann.2 Thus, there is a series of recent reviews to which readers of the Australian Dental Journal can refer in building up a picture of the utilities of radiographs (and newer imaging methods) in the diagnosis of periodontal diseases and to some extent in the treatment of these diseases. However, some questions remain, questions raised directly in these recent reviews or issues not themselves directly considered heretofore. This review raises for consideration issues to do with periodontal diagnosis, questioning the exact role of radiographic imaging, covers the usefulness of panoramic radiography in periodontal assessment and in treatment planning decision making, considers the practicalities of digital imaging in periodontology, shares experiences with digital subtraction radiography and considers possible utilities of cone-beam computed (digital volume) tomography in periodontology. Radiographs in periodontal disease diagnosis In this issue, Highfield8 has dealt with the current situation regarding diagnosis based on the outcome of an International Workshop for Classification of Periodontal Diseases.9 The word ‘‘diagnosis’’ is derived through Latin from the two Greek words, romanized as ‘‘dia’’ meaning ‘‘to split’’ or ‘‘apart’’, and ‘‘gnosis’’ meaning ‘‘to learn’’. Thus, diagnosis really implies being able to separate one (or more) conditions from another (or others). In medicine this telling apart of different departures from normal, or health, in a person constitutes diagnosis. In Periodontology 2000, Armitage10 proposed that a ‘‘periodontal diagnosis’’ is a ‘‘label’’ which clinicians place on a person’s periodontal condition or disease. This label given to a person’s periodontal condition (if departing from what is considered normal form for a given racial group) or disease should conform, or be convertible, to current classification of periodontal diseases (and conditions). Highfield8 has provided a more convenient and simplified summary of the current classification. The use of radiographs in arriving at the ‘‘label’’ to attach to a ª 2009 Australian Dental Association Radiographs for diagnosis and management person’s periodontal condition or disease is considered according to the structure given by Highfield.8 I. Gingival diseases11 Both A. Plaque induced, and B. Non-plaque induced, gingival diseases can be diagnosed on the basis of clinical findings, and the results of further investigations, without the need for radiographs. Also, there is recognition in the 1999 classification that plaque induced gingivitis may occur on a reduced periodontium which is not undergoing progressive destruction.11 It is possible, if clinical records (chartings and study casts) are comprehensive and accurate, for stability of a reduced periodontium to be assessed without the need for radiographs, although radiographs should of course reveal further alveolar bone loss, but such radiographic evidence would in normal clinical circumstances only be a confirmatory finding of new or recurrent periodontitis. II. Chronic periodontitis12 Both A. Localized and B. Generalized chronic periodontitis are characterized by pocket formation and ⁄ or gingival recession, both clinically detectable without radiographs. Chronic periodontitis can be divided into localized if less than 30 per cent of available sites display clinical attachment loss, and generalized if more than 30 per cent of sites display clinical attachment loss. This differentiation is made on the basis of clinical findings and so radiographs are not required, although radiographs may be used but may mislead. Chronic periodontitis can be further characterized by various degrees of severity on the basis of measures of clinical attachment loss. Therefore, for the assessment of the severity of chronic periodontitis, radiographs are not required although radiographs may be used, but are not essential. The manner in which radiographs may mislead in the assessment of extent is that the chronic periodontitis may have been treated and while the radiographs may show (and here because conventional radiographs do not allow for an interpretation of buccal and lingual sites and so only interproximal sites can be assessed and calculated) the extent of the number of interproximal sites, or teeth, with bone loss however it is the presence or absence of the clinical signs apparent only on clinical examination which indicate extent of current chronic periodontitis. Similarly in the determination of the severity of chronic periodontitis from the estimation of alveolar bone heights shown on conventional radiographs, the chronic periodontitis might have been previously successfully treated and so the assessment of severity is an assessment of the severity of the previous chronic periodontitis and not of the current status. ª 2009 Australian Dental Association The diagnosis of chronic periodontitis is made on the basis of periodontal pockets and ⁄ or recession. In some clinical situations restorations may impede the accessibility of the periodontal probe into a pocket and ⁄ or may obscure the CEJ and so compromise the clinical assessment of the presence and severity of chronic periodontitis. In such a situation radiographic evidence of alveolar bone loss may be helpful. Similarly, subgingival calculus or root surface topographies or malformations may impede the passage of the periodontal probe. In these situations radiographic evidence of alveolar bone loss may be helpful as it may direct the attention of the examining clinician to probe carefully sites or teeth with evident radiographic bone loss. III. Aggressive periodontitis13 Both A. Localized and B. Generalized aggressive periodontitis share the common features of chronic periodontitis, pockets and ⁄ or recession. However, there is or has been rapid attachment loss and bone destruction and, where possibly noted, a familial aggregation can be elicited, and apart from the periodontitis the patients are otherwise clinically healthy. It was suggested13 that the diagnosis may be based on clinical, radiographic and historical data, although it can be questioned whether radiographs are required for the diagnosis. The issue is that the diagnosis of aggressive periodontitis can be made with recourse to laboratory testing.13 The differentiation between A. Localized: first molar ⁄ incisor presentation with interproximal clinical attachment loss on at least two permanent teeth, one of which is a molar and involving no more than two teeth other than first molars and incisors; and B. Generalized: interproximal clinical attachment loss affecting at least three permanent teeth other than first molars and incisors, needs to be made clinically and radiographs are not required. The diagnosis ought not be made on the basis of radiographs alone, and given that the key feature is clinical attachment loss, radiographic examination is not required for the diagnosis of aggressive periodontitis, although the localized form may present with a very characteristic ‘‘mirror image’’ pattern of bone destruction. IV. Periodontitis as a manifestation of systemic disease Highfield8 notes that this classification, periodontitis as a manifestation of systemic disease, proposes only those diseases in which the periodontitis is a manifestation of the disease process and does not include disease states or medications which modify existing periodontitis. Periodontitis as a manifestation of a disease process can be diagnosed and characterized on the basis of the S29 EF Corbet et al. findings from a clinical examination without the need for radiographs. V. Necrotizing periodontal diseases14 Necrotizing periodontal diseases are divided into A. Necrotizing ulcerative gingivitis, an infection characterized by gingival necrosis presenting as ‘‘punchedout’’ papillae, with gingival bleeding and pain. A characteristic foetid breath and pseudomembranes covering the ulcerations, which themselves bleed readily on being disturbed, may be noted; and B. Necrotizing ulcerative periodontitis in which there is not only necrosis of gingival tissues but also necrosis of periodontal ligament, and alveolar bone. Both of these diagnoses are established on the basis of the symptoms and the clinical signs, and radiographs are not required. VI. Abscesses of periodontium15 Abscesses affecting periodontal tissues were divided into: A. Gingival abscess, a localized prevalent infection that involves the marginal gingiva or interdental papilla; B. Periodontal abscess, a localized purulent infection within the tissues adjacent to a periodontal pocket; and C. Pericoronal abscess, a localized purulent infection within the tissue surrounding the crown of a partially erupted tooth. A periodontal abscess may lead to the destruction of periodontal ligament and alveolar bone whereas a gingival abscess and a pericoronal abscess probably will not give rise to radiographically detectable bone loss. Conventional radiographs may, therefore, allow for the differentiation between a gingival abscess and a periodontal abscess but clinical findings alone should be sufficient to allow for this differentiation. Highfield8 notes that periodontal abscesses may result from root fractures or cemental tears. Such misfortunes may not be apparent radiographically, but if detected on radiographic examination than the radiograph(s) can be said to have been an aid in determining the underlying cause for the diagnosed condition, but any radiograph(s) did not serve, as is often implied, as an ‘‘aid to diagnosis’’, because the diagnosis of a periodontal abscess was made on the basis of the clinical findings. VII. Periodontitis associated with endodontic lesions16 Simply reducing all categories of combined periodontalendodontic lesions, without any need to determine which component preceded or were the cause or the result of the other, is a pragmatic approach which has been adopted for the diagnosis of lesions in which there is any coalescence of endodontic and periodontal pathologies. A primary periodontal lesion which mimics an endodontic lesion is still just solely a periodontal S30 lesion and so is not a ‘‘perio-endo’’ lesion. Similarly, an endodontic lesion with a sinus draining through the periodontal ligament, which after successful endodontic therapy completely resolves without the need for any periodontal therapeutic intervention, is only an endodontic lesion and is not a ‘‘perio-endo’’ lesion. Hence, all that needs to be diagnosed is a coalescence of periodontal and endodontic pathologies and this is termed a combined periodontal-endodontic lesion. For this diagnosis the standard conventional intra-oral radiographic exposures for diagnosing periapical periodontitis, usually periapical radiographs, are required, and if periodontal pathology is evident clinically a longcone paralleling technique17 is preferred for the taking of the periapical radiographs. The use of gutta-percha cones inserted into any sinus opening to trace the origin of a draining lesion is a very useful approach at the time of exposing a paralleling periapical radiograph in the diagnosis of combined lesions. VIII.Developmentaloracquireddeformitiesandconditions As Highfield8 notes, this category of the current classifications seems to have been added for completeness. Another interpretation is that these seem to be included in the classification because clinical periodontology devotes some time and energy to correcting, or at least managing these, and if these were not included in the classification then the justification for the expenditure of clinical effort and the use of clinical time could be questioned. It is only for tooth-related conditions18 that there may be a periodontal diagnostic imperative for radiographic examination. Whether radiographs are required for the establishment of a diagnosis compatible with the current classification system (I to VIII) is summarized in Table 1. Clinical assessment of the need for radiographic examination in periodontal patients The Australian Radiation Protection and Nuclear Safety Agency’s Code of Practice for Radiation Protection in Dentistry19 and its Safety Guide for Radiation Protection in Dentistry20 both make it abundantly clear that there is a responsibility for clinical assessment for the need for dental radiography to be performed, unless an emergency situation dictates otherwise, and for this to precede the radiographic exposure. Radiography must not be a substitute for clinical investigation, and routine use of X-radiographs as a component of periodic examinations or at any given frequency cannot be condoned. This code of practice and safety guide presumably offer the most definitive available advice to dentists in Australia on radiography in dentistry and the advice should be heeded, specifically all the advice given on minimizing exposure to ionizing radiation. ª 2009 Australian Dental Association Radiographs for diagnosis and management Table 1. Radiographs in periodontal diagnosis Diagnosis Radiographs required for establishing diagnosis Gingival diseases Chronic periodontitis Aggressive periodontitis Periodontitis as a manifestation of periodontal diseases Necrotizing periodontal diseases Abscesses of the periodontium Periodontitis associated with endodontic lesions Developmental or acquired deformities and conditions Not required Not required Not required but sequential radiographs may display rapid bone loss Not required Not required Not required but may reveal cause Required, as if for endodontic diagnosis Required really only for some tooth related Table 2. Clinical periodontal findings not captured on radiographs Table 3. Conventional radiography – findings relating to predisposition to periodontal diseases Gingival redness Gingival swelling Gingival bleeding Gingival recession Gingival enlargement Bleeding on probing Probing pocket depths Tooth hypermobility Suppuration Calculus* – usually approximally Overhanging radiopaque restorations* – usually approximally Root anomalies ⁄ malformations Root features Cemental tears Many of the clinically important features of periodontal diseases are not evident on radiographs (Table 2), but nonetheless radiographic investigation is only ever warranted after careful clinical examination and recording. In the event of clinical signs of periodontitis, probing pocket depths and ⁄ or recession, being encountered in a clinical examination, radiographic examination yields some information on: evident bone levels; evident patterns of bone loss, even or angular; tooth-root lengths, morphologies and topographies; and importantly length of tooth-root radiographically surrounded by alveolar bone. Clinical attachment loss (probing pocket depth plus recession, or probing depth from the detected CEJ to the pocket depth when there is no recession) is the diagnostic yardstick for periodontitis and also the calculating tool for determining clinical severity of periodontitis, but remaining tooth-root support is the major complementary estimation provided only by radiographic imaging, which while not diagnostic, is of pivotal concern in treatment planning decisions, in prognosis estimation, and, in fact, in contributing hugely to the eventual outcome, the retention of periodontitis affected teeth in acceptable function for life. Some findings which relate to a predisposition to periodontal disease are only evident radiographically (Table 3). Diagnostic yield of radiographs in clinical periodontology Surprisingly, there is really only one published study which has investigated what was called ‘‘diagnostic yield’’21 in periodontology. This study involved clinical ª 2009 Australian Dental Association *Detectable clinically. examination of 300 subjects, 55 of whom had previous radiographs, and a first treatment plan was developed. Then a full-mouth radiographic survey (paralleling periapical and bitewing radiographs) was performed and a second treatment plan was developed. The first and second treatment plans were compared, and ‘‘diagnostic yield’’ was the term given to the difference between the first and second treatment plans. From what was proposed by Armitage,10 a periodontal diagnosis is the label put on a person’s periodontal disease or condition. This means that unless ‘‘hopeless tooth ⁄ teeth’’ is a label, which is not put on a periodontal condition in any event, then this study did not investigate ‘‘diagnostic yield’’ but rather investigated the impact of radiographs on treatment planning in clinical periodontology, which could perhaps be better termed a ‘‘therapeutic yield’’. The major differences in treatment plans between the first and second plans were to do with teeth to be extracted, and then restorative, endodontic and prosthodontic treatment decisions. It appears from this study that radiography in clinical periodontology informs treatment planning more than it does diagnosis and, apart from decisions to do with extractions, the therapeutic yield lies in the other aspects of treatment needs: endodontic, restorative and prosthodontic. Hence, in compliance with Australian guidelines19,20 radiographic examination in clinical periodontology is only justified if changes in treatment plans from those treatment plans developed on the basis of clinical examination supplemented by any already available radiographs are anticipated. Often radiographs are prescribed to confirm already established treatment decisions, and while sometimes this may be justified to form a basis for informed consent for instance, confirmatory radiographs are not usually to be condoned. If the clinical findings, for S31 EF Corbet et al. example, indicate that a tooth is hopeless due to extreme and symptomatic hypermobility accompanied by advanced loss of clinical attachment, a radiograph exposed purely to document this assessment of the tooth being hopeless, based as it is on the clinical findings, is not justified. In reality, exposure of the patient to additional radiation would only be warranted if the tooth could be salvaged following the study of a radiograph. The clinical findings, if accurately recorded in a patient’s records are sufficient documentation of the findings, and a ‘‘for the record only’’ radiograph is not advised. Further, in prescribing dental radiographs in Australia all the advice given19,20 should be followed. It has been proposed elsewhere that failure to minimize the x-ray dose exposure through the use of E-speed films and rectangular collimating devices may constitute a medico-legal issue.22 Indeed, the positioning device shown in Fig 1b is for a cylindrical cone and not for a rectangular collimating device. When manufacturers of positioning devices have been specifically questioned on the lack of rectangular positioning devices, the reply has been that rectangular collimating devices are not popular, and thus there would not be a demand among those who purchase x-ray equipment. Certainly, in Sweden23 and England and Wales,24 published reports have suggested the (a) manufacturers’ assessments to be correct, documenting as they do that concern for minimizing radiation exposure is not widespread. However, the situation in Australia with respect to general and specialist dentists’ adherence to x-ray dose reduction practices is not known at present. This would make a worthwhile study. Radiographic features impacting upon treatment decisions There are many features to do with bone and teeth evident on conventional radiographs, in addition to those relating to caries, endodontic, restorative and prosthodontic conditions, which can impact on periodontal treatment planning. These are listed in Table 4. One ‘‘paper case’’ based study with and without radiographs in periodontal diagnosis and treatment planning25 showed that the availability of radiographs, as in the earlier ‘‘diagnostic yield’’ study,21 resulted in more extractions being planned. These two studies strongly support the contention that radiographs inform periodontal treatment planning by revealing not what has been lost but what is remaining. What is remaining can be viewed from two aspects: (1) what clinical challenges remain, in terms, for instance, of debriding sufficiently well the root surfaces of incompletely separated (fused) roots of molar teeth or teeth with radiographically evident root grooves ⁄ flutings on roots; and (2) how much length of root appears to remain embedded in alveolar bone, which estimation is allowed by radiographic examination and which is not discernable from the clinical examination. Conventional radiographic views to assist periodontal treatment planning Conventional bitewing radiographs (b) Horizontal bitewing radiographs, while useful for approximal caries detection, are not so useful in informing periodontal treatment and treatment planning if bone loss is in any way advanced. Vertical bitewing radiographs, whereby the film is placed with its long axis at 90º to the placement for horizontal Table 4. Conventional radiography – findings of periodontal interest impacting upon treatment decisions Fig 1. (a) Vertical (left) and horizontal (right) bitewing tab positions. (b) Vertical bitewing film holder. S32 Bone levels Bone loss – even or angular patterns Intra(infra) – bony defects Root morphologies ⁄ topographies Furcation radiolucencies Endodontic lesions Endodontic mishaps Developmental anomalies Root length and shape(s) remaining in bone ª 2009 Australian Dental Association Radiographs for diagnosis and management Fig 2. A Kwikbite ⁄ Parobite positioning device for a rectangular collimating device for both vertical and horizontal bitewing radiograph exposures, inserted into a round cone positioning ring. bitewing radiography, can be very helpful if clinically there is nothing suggestive of any previous endodontic therapy or current periapical periodontitis alone or in combination with periodontal destruction. The vertical bitewing radiograph can be facilitated by placing the ‘‘tab’’ on which the patient bites at 90º to its position for horizontal bitewings (Fig 1a), or by using a vertical bitewing holder (Fig 1b) through which, if there is a cone positioning ring, a reasonable degree of reproducibility can be achieved for subsequent sequential radiographs. There is one Swiss product called the Hawe Paro-Bite Centring Device which can be inserted into a round positioning device which assists in the positioning of rectangular cones for vertical and horizontal bitewings (Fig 2). The assistance provided by such a positioning aid is advised to reduce the need for repeat radiographs and hence the need for unnecessary x-ray exposure. For intact arches, probably two vertical bitewing radiographs per posterior sextant are required. Figure 3 shows one vertical bitewing with bone levels and defects apparent revealing root morphologies of roots in need of debridement. Not all root apices are evident and hence some periapical bone is not visible. Conventional periapical radiographs Periapical radiographs when exposed for periodontal purposes should use long-cone paralleling projections, preferably with rectangular collimators. Full-mouth surveys of paralleling periapical radiographs have been considered to be a ‘‘gold standard’’ for periodontal diagnosis and treatment planning. For some this view still persists. For instance, the European Federation of Periodontology still calls for this full-mouth series of periapical radiographs in case presentations by candidates at the conclusion of higher education and training in periodontology. However, there is no basis for considering a full-mouth series of paralleling periapical ª 2009 Australian Dental Association Fig 3. A vertical bitewing, with bone levels and intrabony defects apparent. radiographs to influence periodontal treatment decisions any more than, say, panoramic radiographs. The pictorial heading banner of the website* of the Australian and New Zealand Academy of Periodontology shows a gloved hand holding a panoramic radiograph. If a panoramic radiograph is available, having been exposed for whatever purpose, that radiograph may alone be sufficient,26 or a panoramic radiograph may be supplemented by selected intra-oral radiographs which numbered less than four per patient to reach the ‘‘gold standard’’ in one study.27 It has been shown that if seven periapical radiographs supplement a panoramic oral radiograph then the effective radiation dose exceeds that of a full-mouth series of periapicals,28 but if the number is less than four, then there is a reduction in radiation exposure and yet the ‘‘gold standard’’ in terms of information can be achieved. Conventional panoramic oral radiographs Modern panoramic oral radiography achieves decent images suitable, with perhaps only modest intra-oral supplementation, for periodontal treatment planning purposes. The differences in any ‘‘yield’’, even with an older generation of panoramic radiograph machines *URL: ‘http://anzap.org.au’. Accessed 20 March 2009. S33 EF Corbet et al. and technology, in comparison with periapicals,29 and bitewings,30 and bitewings and periapicals,31 and periapicals and clinical probing32 were small, and for newer panoramic radiograph technologies difference in any ‘‘yield’’ are apparently even smaller.33 Panoramic radiography in a group of periodontal maintenance patients, that is patients previously affected by periodontal disease which had been treated and who were undergoing supportive periodontal care, showed ‘‘great agreement’’ with long cone intra-oral radiographs.34 Two of the recent reviews1,6 have dealt with the issue of paralleling periapical series versus panoramic oral radiographs. The features of interest for periodontal assessment noted on periapical radiographs are also capable of being noted on panoramic radiographs (Table 5). For many practitioners the radiographic features of interest on a panoramic, supplemented where necessary by a small number of intra-oral views, is sufficient for the management of periodontal diseases. Tugnait and Camichael6 note how there has been a pragmatic shift by many towards panoramic radiographs in the investigation of patients with periodontal diseases, in view of time efficiency, greater patient tolerance, and often a lower radiation exposure. Cost savings are also more and more an issue, and while the machinery for panoramic oral radiography is not cheap, it is nowadays relatively cheaper than formerly, and the time taken for producing a full-mouth periapical series is a costly investment if there is little by way of yield. The American Academy of Periodontology (AAP) in its 2000 Parameter on Comprehensive Periodontal Examination35 holds that ‘‘radiographs that are current, based on the diagnostic needs of the patient, Table 5 (after Tugnait et al.1). Detectable features of interest on radiographs Bone levels Bone loss – even – angular Furcation involvement Calculus Radio-opaque restorative margins – deficiency – overhang Root morphologies Root length embedded in alveolar bone Widened periodontal ligament space Approximal root caries Root canal fillings Periapical periodontitis, cysts, granulomas Impacted third molars Retained roots Fractured roots Cemental tears Cysts ⁄ tumours S34 Periapical Panoramic Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Often Sometimes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Sometimes Yes should be utilized for proper evaluation and interpretation of the status of the periodontium … Radiographs of diagnostic quality are necessary for these purposes’’. It further states ‘‘Radiographic abnormalities should be noted’’.35 Panoramic radiographs fulfil these conditions (Table 5) and allow for the identification of radiographic abnormalities. The point made by the AAP that there should be some record made of what was detected on the radiographs is advice given in many jurisdictions. While available, the radiograph(s) reveal all that can be discerned, but if the radiograph(s) is(are) not available for whatever reason, then having some written record of the findings should obviate the need for any additional repeat radiograph to compensate for the temporary unavailability of the radiograph(s). The AAP in its 2001 Position Paper on ‘‘Guidelines for periodontal therapy’’36 holds that ‘‘interpretation of a satisfactory number of updated, diagnostic quality periapical and bitewing radiographs or other diagnostic imaging needed for implant therapy’’ is required. The AAP contends that intra-oral radiographs, such as periapical films and vertical or horizontal bitewings, provide a considerable amount of information about the periodontium that cannot be obtained by any other non-invasive means.37 Panoramic radiographs certainly do provide a considerable amount of information (Table 5) and they also inform on treatment planning. The situation of the AAP becomes clear on viewing the AAP website* (‘‘Search Our Site’’: ‘‘Panoramic’’ in the gateway to ‘‘Members Only’’ AAP Insurance Policy Statement – Radiographs in Periodontics), where it is stated: ‘‘The American Academy of Periodontology believes that panoramic radiographs have limited value in the diagnosis of periodontal disease …’’ This, however, is only a ‘‘belief’’. A casual view of the world reveals that not all share the same beliefs. The authors of this review do not share the same belief as the AAP. The expense, time and physical inconvenience in having all periodontitis patients subjected to a full-mouth series of periapical and bitewing radiographs on the basis of a belief can be questioned, as it is in this review. The American Board of Orthodontics is more reasonable in its advice, only requiring six intra-oral radiographs to supplement a panoramic view for adults for comparison of pre-treatment and post-treatment crestal bone levels and root status.38 One earlier study shows how dearly belief systems with respect to full-mouth periapical surveys can be held.39 In this American study, the proportion of patients who had the results from a screening clinical examination and a panoramic radiograph but who were still judged by independent examiners to be in need of full-mouth periapical series was the same as for those patients who only had the *URL: ‘http://www.perio.org/index_pro.html.’ Accessed 20 March 2009. ª 2009 Australian Dental Association Radiographs for diagnosis and management clinical screening results. In that study, patients were slated by the examiners for the full-mouth series of periapical radiographs on the basis of the case type into which they fell. Recommendations for the full-mouth periapical radiograph series was made on the basis of case type, and information available from the panoramic was not used because in the examiners’ opinions that particular case type demanded the full-mouth periapical series, because it seems that was what they had been taught. When dental teaching hospitals in the United Kingdom and Ireland were surveyed,40 the most commonly taken views to assess periodontal status were panoramic radiographs with selected periapical radiographs. Hopefully, graduates from these dental schools will follow their teaching, while constantly evaluating the state of knowledge and experience in this field and being prepared to change practice as new evidence emerges. Further, panoramic radiographs have been shown to reveal in a majority (63 per cent) of periodontal patients some form of dental abnormality unrelated to periodontal disease.41 General radiologists in Australasia have had recent advice on the interpretation of dental panoramic radiographs42 and should thus be available for consultation, as would be other dental specialists in Australia, if abnormalities detected were to be out of the ordinary. Panoramic radiographs may not reveal alveolar bony defects as accurately as periapical radiographs.43,44 However, that is not the issue. The issue must be whether there is any additional therapeutic yield from any greater accuracy in representation of alveolar bone destruction revealed on periapical radiographs. A small study was conducted in Hong Kong in which part-time clinical dental teachers were asked to develop periodontal treatment plans on the basis of, in the first instance, a complete periodontal charting, study casts and a panoramic radiograph. The 35 patient records chosen were of adult patients with, what would now be diagnosed as, chronic periodontitis and who had at least six teeth per quadrant. After a one-year wash-out period, the same clinical records camouflaged, and study casts were given along with, on this second occasion, not the panoramic radiograph but a fullmouth series of paralleling periapical radiographs which at the time of the charting had been prescribed by a dental surgeon in the clinic in compliance with his previous teaching. The individual treatment plans derived on the first and second occasion were almost identical. Between examiners there was variation in treatment plans regarding periodontal surgery, as has been reported from elsewhere,45 and extractions. However, each individual part-time clinical dental teacher developed almost identical treatment plans from clinical findings and panoramic radiographs (of an earlier generation) as they did from the clinical findings and the full-mouth paralleling periapical radiograph series. Hence, there was no perceptible ‘‘therapeutic yield’’ from the additional full-mouth periapical radiograph series, such as that shown in Fig 4. The full-mouth series of periapical radiographs shown in Fig 4 is mounted on a clear, not a traditionally black, background. The Australian Safety Guide for Radiation Protection in Dentistry20 suggests mounting radiographs on a ‘‘mask’’ which eliminates stray light around the radiograph, and provision for magnification is also suggested as being advisable. The periapical radiographs in Fig 4 are mounted on a clear background because each radiograph should be viewed against a light-box using a viewing box with in-built magnifying lens (Fig 5). Such viewing boxes are available and are highly recommended not only for conventional periapical and bitewing radiographs, but also for the study of conventional panoramic oral radiographs in assessing crestal bone loss and alveolar bony defects. While panoramic radiography may be less accurate in the representation of bony defects than intra-oral radiography,43,44 this has little therapeutic effect in practice. For instance, many therapeutic decisions to do with the management of bony defects are not Fig 4. A full-mouth periapical radiograph series. ª 2009 Australian Dental Association S35 EF Corbet et al. Fig 5. A radiograph viewing box to provide magnification and to block out ambient light in use. determined by the radiographic appearance, but rather by the intra-operative appearance of the tooth-roots and the bony defects. Guided tissue regeneration (GTR), it has been concluded in a systematic review,46 achieves 1.22 mm more gain in clinical attachment level at pocket sites than open flap (access flap) debridement. Narrow and deep infrabony defects have been shown to respond radiographically and, to some extent at least, clinically more favourably to GTR than wide and shallow defects, and depth was more indicative of favourable response than the angle of the defect.47 This finding was confirmed in a follow-up study.48 GTR requires a surgical approach to the defects. The surgical approach allows for direct intraoperative assessment of defect depths and angles. No reliance should be made on the radiographic assessment of the bony defect. The most that the radiographic assessment of defect depth and width might indicate would be a preparedness to consider GTR as a therapeutic alternative. The findings with respect to the defect on flap reflection – whether the defect is contained or circumferential, indeed whether the tooth is treatable and retainable or not – determine the S36 applicability of the GTR approach. This is decided intra-operatively and not on the basis of the radiographic assessment alone, if indeed at all. In a systematic review,49 Emdogain (an enamel matrix derivative) was found to have improved probing attachment levels by 1.2 mm and probing pocket depth reduction by 0.8 mm compared to open (access) flap debridement, although these results have to be interpreted with caution. The effectiveness of Emdogain is also dependent to an extent on defect depth and defect morphology. Emdogain has been shown to be very successful, over a nine-year period, in deep defects50 and in angular defects.51,52 The depth of defect and its suitability for Emdogain regeneration are all made intra-operatively. Questions of interest to the operator – such as ‘‘is the defect a deep defect?’’, ‘‘is it contained or circumferential?’’, ‘‘are the root surfaces amenable to debridement?’’ – can all be answered on the basis of the intra-operative direct assessment. The pre-surgical radiographic assessment again may only indicate that Emdogain might be considered in the surgical treatment of that defect. Also, for Emdogain regenerative therapy, as for GTR, often in the clinical situation on surgical reflection of flaps, defects reveal themselves to be topographically well suited to regenerative approaches, when the pre-surgical radiographic assessment had not suggested such. In these clinical circumstances, the radiographic assessment has not guided the eventual treatment approach adopted. If an adjunctive regenerative approach had proved to work with non-surgical periodontal therapy for specific infrabony defect depths and configurations, but not for others, then pre-treatment radiographic accuracy in representing defects would be at a premium. Sadly, however, Emdogain has been shown to offer no advantage when applied as an adjunct to non-surgical periodontal therapy.53–55 Hence for most therapeutic decisions, and thus offering satisfactory ‘‘therapeutic yield’’, panoramic oral radiography is, notwithstanding its less accurate depiction of radiographically evident alveolar bone defects, of great therapeutic use. Digital panoramic radiography versus conventional film panoramic radiography There has, up to the present, been very little direct comparison between digital panoramic radiographs and conventional film panoramic radiographs in periodontal assessment. One study compared the efficacy of the Orthophos DS Digital panoramic system with conventional film obtained from the Orthophos Plus (both Sirona, Bensheim, Germany) and found that the conventional film outperformed the digital panoramic in the detection of periodontal findings.56 However, based on a couple of years practical experience of using digital panoramic oral radiographs, the authors’ ª 2009 Australian Dental Association Radiographs for diagnosis and management (a) (b) Fig 6. (a) Digital panoramic. (b) Zoomed-in portion of lower left posterior sextant. experience is that there is an advantage in periodontal assessment. The digital panoramic system with which the authors have experience uses a Kodak 8000C Digital Panoramic Machine (from Kodak-Trophy, Croissy-Beaubourg, France) using Kodak Dental Software, to feed into a patient database held on Trophy DICOM software which is transferred into the hospital’s patient management system. An example of a digital panoramic is given in Fig 6a and a ‘‘zoomed-in’’ portion of that image is shown in Fig 6b. The ability to manipulate the panoramic images, such as zooming in and changing contrast, has proved a very useful feature in assessment of bony defects and root morphologies, and open (access) flap debridement surgeries have confirmed an impression of a greater ability in anticipating the shape, depth and extent of bony defects following study of digital panoramic radiographs compared to viewing conventional panoramic oral radiographs. The ability to zoom in and magnify defects and to adjust dynamically the contrast and brightness allows for vastly improved ‘‘visualization’’ of bone levels and intra-bony defects. To date one study has shown that periapical periodontitis was more scoreable on screen from digital panoramic radiographs than on printed digital panoramic radiographs, supporting the advantages gained from manipulating the digital panoramic oral images in assessing bony lesions rather than interpreting only one static panoramic oral image.57 ª 2009 Australian Dental Association Digital intra-oral radiography The authors’ experience with digital intra-oral radiograph for periodontal assessment is somewhat less encouraging but nonetheless generally positive. There are two approaches to digital imaging, direct digital imaging and indirect digital imaging. ‘‘Direct’’ is achieved by using a solid state sensor to detect x-rays. For intra-oral use these sensors are bulky and inflexible, and require a cable connection. These sensors must convert x-ray detection to electronic signals for subsequent electronic processing to produce usable images. These direct digital images can be of high quality. Readers are referred to earlier reviews2,5 for the further information on direct digital imaging in periodontal assessment. Since these reviews2,5 have been published, there has been not much change to the conclusion that alveolar bone measurements are reproducible, using both direct digital and conventional radiographs, and that direct digital radiographs do not enhance examiner agreement over conventional radiographs.58 Of course digital images, derived from direct digital imaging, or indeed also indirectly derived, can be studied using image analyser tools. A study of one such tool concluded that a dental image analyser tool can reliably replace conventional measuring on intra-oral film radiographs for measuring bone in periodontitis patients.59 Such image analyser tools may well become more of mainstream devices for quantifying bone loss, and also post-periodontal therapy bone gain or bone level stability. Indirect digital imaging involves a latent image being acquired using a photostimulable phosphor plate, and then after the latent image is captured on this plate the image is scanned by laser to produce a usable image. The scanning process either erases the latent image on the plate so that the plate can be reused straight away without there being double imaging, or else the image on the plate is only degraded by laser scanning and must be erased by exposure to light. There are various advantages of indirect digital imaging over direct digital imaging. The plates can be the same sizes as intra-oral conventional x-ray films and so all conventional intraoral clinical approaches can be used. Also there is no need for a cable, patient tolerance is greater, and the expense is less. However, there are disadvantages. Depending on the approach, the image quality may not be as good as with the direct imaging. Direct imaging produces immediate images which is not necessarily so with indirect digital imaging. Further, the flexibility of the plate means that image distortion due to plate bending can occur, as with film bending in conventional radiography. If the plates are scratched, effectively they are ruined, and so plates must be treated with great care at all times. However, many other dental schools using the same hospital patient management system as used in S37 EF Corbet et al. Hong Kong, into which indirect digital images are fed, report very high quality images with great utilities. Some studies on marginal alveolar bone levels do confirm that indirect digital images had favourable measurement accuracy compared with film radiographs,60 while colourizing digital images using colour-coding algorithms did not produce greater accuracy in this respect.61 However, indirect digital bitewings have been shown to be no better than film bitewings in the assessment of alveolar bone loss.62 If decent images are produced from indirect digital imaging, there is no evidence to suggest that indirect digital intra-oral radiographs are inferior to conventional intra-oral radiographs in periodontal assessment and treatment planning. There is another approach to the management of radiographs, sometime erroneously also referred to as indirect digital imaging, and that is the digitization of exposed and processed conventional x-radiograph films using a flatbed scanner with a transparency adaptor. This is the approach used to date in the digital subtraction radiography (DSR) approach, considered below. The viewing possibilities, e.g., projection of such images, may improve interpretation,63 and such subsequent management of conventional intra-oral radiographs may facilitate the interpretation of periodontal bone defects,64 and of course image analysis tools can be used on these digitized radiographs. be made and attached to the film holders and the film holder must be reproducibly aligned to the x-ray beam collimating device (Fig 7). Once standardized serial periapical radiographs have been produced, these conventional radiographs must then be digitized using flatbed scanning devices. Obviously, this step can be omitted if direct or indirect digital images have been collected. Then there are various methods to determine the changes (+ indicating more bone ⁄ more bone density, – indicating less bone ⁄ less bone density) between two radiographic images. Reference aluminium wedges can be captured in the images which more easily allow for determination of density correction.65 Computer-assisted densitometric image analysis (CADIA)66 of the digitized standardized intra-oral radiographs is the method with which the authors have experience. A DSR system was developed at The University of Hong Kong which has been calibrated and validated.67 This DSR system has been used in a published study on a low-power laser system in periodontal therapy.68 It has also been used in clinical studies on comparing periodontal surgical therapy with repeated non-surgical Digital subtraction radiography Digital subtraction radiography (DSR) in periodontology basically allows the detection of small changes in alveolar bone, which might otherwise go undetected. For DSR to permit this to be realized, serial radiographs need to be taken with the best possible reproducible projection geometry and using standardized image processing. To optimize the projection geometry custom (patient-by-patient, area-by-area) bite blocks must Fig 7. A custom positioned periapical film holder with bite block attached to a collimating device for digital subtraction radiography. S38 Fig 8. Cone-beam Computed Tomography Machine (i-CAT, Imaging Sciences International, Hatfield, USA). ª 2009 Australian Dental Association Radiographs for diagnosis and management therapy, and on non-surgical therapy on post-menopausal females, comparing those taking with those not taking hormone replacement therapy. Thus, quite some experience with this approach has been gleaned. The conclusion would be in line with that of Bragger7 that DSR remains primarily a research tool for clinical trials. Mol5 discusses how it is often proposed that the time and effort involved in producing subtraction images of high quality to detect small changes is prohibitive in clinical practice. There are more issues to be considered. The storage of multiple custom bite blocks and holders is a very practical one. The time taken in the alignment of images prior to the CADIA is another. Slight variations in choice of the regions of interest are capable of producing contrary results. Also, if DSR detects a loss of bone density or volume, but clinically at that site there are no signs of gingival inflammation, no bleeding on probing and no probing pocket depth, then the reaction can be ‘‘so what?’’, because there is nothing in the routine clinical periodontal armamentarium which can be applied at such a site. Mol5 opines that at one level or another a price has to be paid for increased diagnostic utility. But when the DSR ‘‘diagnosis’’ does not suggest any clinically useful intervention, then not only the ‘‘price’’ but the ‘‘utility’’ can also be questioned. A further issue is what sites to select. Studies can focus on specific sites, such as furcations69 and can show favourable outcomes to therapy in terms of bone behaviour. A recent study of scaling and root planing had 13 subjects but each subject had only three sites included in the study.70 It can be questioned what is special or representative about the sites chosen. The DSR did reveal favourable outcomes to scaling and rooting planing, but studies on scaling and root planing have shown favourable effects on bone detectable by conventional radiography. DSR was used in the published study on low-power laser as an adjunct in periodontal therapy.68 It showed a biological and measurable early effect on bone, which could not be detected by clinical means, but again the question suggested is ‘‘so what?’’ as no clinically detectable benefit could be observed. A final issue in DSR is that periodontally involved teeth are often mobile and can be displaced by the bite block and ⁄ or the process of registering the bite prior to therapy, but such teeth can firm up, and for drifted teeth they may reposition themselves, in response to therapy. Then the custom bite block does not fit posttherapy and the serial images cannot be aligned and the altered tooth positions in the serial images cannot be corrected for. The American Academy of Periodontology Position Paper on Diagnosis of Periodontal Diseases37 very optimistically holds that future development of subtraction radiography techniques promises Fig 9. i-CAT Vision software interface, consisting of pan-map (upper right), horizontal section (upper left), vertical sections (lower right) and reconstructed 3-dimensional model (lower left). ª 2009 Australian Dental Association S39 EF Corbet et al. to have a profound impact on the diagnosis of periodontal diseases. The authors of this review could not in any way agree. Cone-beam computed tomography Computed tomography (CT) has been used in some studies in relation to periodontal defects.71,72 However, conventional CT does not offer any favourable costbenefit, dose exposure or therapeutic yield advantage in periodontal practice and is unlikely to find a routine place. Fig 10. Horizontal views of periodontal alveolar bony defects at upper left second premolar (25) to upper left second molar (27). Cone-beam geometry allows for reduced dose of radiation. This, in combination with ‘‘fast’’ receptors and the reduced cost of manufacturing the machines, has allowed for the introduction of cone-beam CT into dental ⁄ oral imaging. One difference between conebeam CT and conventional CT is that the cone-beam produces increased scatter on images making conebeam CT unsuitable for soft tissue, a major benefit of conventional CT, which in fact is an advantage in dental ⁄ oral radiography wherein only radio-opaque structures are generally studied. Machines specifically for dental ⁄ oral use have been brought to the market and are hugely impacting the field of dental ⁄ oral imaging. Figure 8 shows one such machine, which while less obtrusive than a medical CT machine, still requires space to accommodate it. However, it seems unlikely that these machines will soon become routine in general dental practices. Because the cone-beam geometry allows for a large volume of tissues to be scanned with a single sweep resulting in a digital image, cone-beam CT is also known in some quarters as digital volume tomography (DVT). Cone-beam CT for assessment of periodontal defects has been applied in in vitro studies.73–77 These have all suggested that there ought to be an application for conebeam CT in vivo in the imaging of periodontal defects. There has, so far, been only one clinical report, of 12 patients, which suggests that cone-beam CT may provide detailed information about furcation involvements in patients with chronic periodontitis78 and so may influence treatment planning decisions. Obviously more research is required. A preliminary study is underway in Hong Kong on the utility of cone-beam CT in periodontal assessment and in informing treatment planning decisions in periodontitis patients. It takes longer for general dentists, periodontology trainees and Fig 11. Vertical views showing lingual furcation involvement at lower left first molar (36) and an extensive defect at palatal aspect of the upper left first molar (26). S40 ª 2009 Australian Dental Association Radiographs for diagnosis and management periodontists to come to decisions on the basis of studying cone-beam CT images than full-mouth paralleling periapical radiographs. This is self-evident as the cone-beam CT allows for bony defects and the root surfaces within the defects to be studies from different sectional views. Figure 9 shows the software interface of one type of cone-beam CT management software (the i-CAT Vision, Imaging Sciences International, Hatfield, PA, USA). The interface consists of four windows. The upper left window is the horizontal view of the arch and the lower right window is a series of the vertical views of a bony defect area. The lower left windows is the threedimensional stimulated reconstruction model of the region of interest. Operators of the viewing software can adjust the focal trough in the horizontal view shown in the upper left image, along the form of the arch in this window so that the pan-map image on the upper right window can be constructed according to this trough. The horizontal and vertical location bars can be adjusted to centre on the defect of interest in the other two windows. Figures 10 and 11 are the zoomed-in images of the periodontal defects centred in Fig 9. Figures 10 and 11 show how the three-dimensional appreciation of the defect and the tooth-roots can be elaborated. Operators can adjust the position of the image, power of zoom-in and zoom-out and contrast of the images in order to assess a particular region of interest. The thickness of the slices across an area of interest can also be adjusted down to an interval of 0.2 mm. These features of the software allow for an appreciation of the three-dimensional nature of defects to be built up, for the root morphologies and topographies to be studied, for buccal and lingual bony landmarks to be discerned, which is not possible in conventional radiography. This is more time consuming than just viewing periapical radiographs. The software to view the conebeam CT images has proved to be user friendly and easily mastered by computer savvy dentists. Also, the ability to take and manage good cone-beam CT images has been easily acquired. How useful cone-beam CT will prove itself in informing periodontal treatment decisions still has to be determined. In the era in which additional periodontal therapeutic approaches are combined with surgical access to the periodontal defects, intra-operative assessment will remain paramount, no matter how much further information is available from advanced imaging techniques. CONCLUSIONS Radiographs do not play a major role in periodontal diagnosis but are hugely useful in guiding periodontal treatment planning decisions. The possible therapeutic yield of any radiograph in periodontitis affected patients must be considered before exposing patients to radiation to produce the radiographs. Radiographs, except in ª 2009 Australian Dental Association emergency situations, should be prescribed only on the basis of a clinical assessment. Available radiographs can all inform, and further radiographs should only be considered in the light of clinical findings and the information gained from the study of available radiographs. Vertical bitewing radiographs are of practical use in periodontitis affected patients. Contemporary panoramic oral radiographs can reveal what can be detected on the basis of periapical radiographs, and a refusal to acknowledge this has more to do with beliefs than any evidence. Panoramic oral radiographs, supplemented by a limited number of selected intra-oral views, selected on the basis of the clinical findings and the appearance of the panoramic oral radiograph, can reach the ‘‘gold standard’’ with reduced radiation exposure. There is much research still to be performed on the therapeutic yield of additional radiographs. Digital panoramic oral radiographs, viewed through computers, seem to offer advantages over conventional film panoramic radiographs and printouts of digitally acquired panoramic radiographs. The loss in accuracy in panoramic oral radiographs compared to periapical radiographs in the depiction of alveolar bone defects may have little impact on treatment planning decisions, if these decisions need in the final analysis at the time of open (access) flap surgical periodontal therapy, such as the incorporation of regenerative approaches. Digital and digitized radiographs allow for the use of image analysis and measurement approaches, but how useful these prove themselves to be is at present unknown. Digital subtraction radiography will likely remain a research tool. The application of cone-beam CT in informing periodontal treatment decisions is only beginning to be investigated, and its application and utility remain to be elucidated. REFERENCES 1. Tugnait A, Clerehugh V, Hirschmann PN. The usefulness of radiographs in diagnosis and management of periodontal diseases: a review. J Dent 2000;28:219–226. 2. Hausmann E. Radiographic and digital imaging in periodontal practice. J Periodontol 2000;71:497–503. 3. Hausmann E, Allen K, Clerehugh V. What alveolar crest level on a bite-wing radiograph represents bone loss? J Periodontol 1991;62:570–572. 4. Hausmann E, Allen K. Reproducibility of bone height measurements made on serial radiographs. J Periodontol 1997;68:839– 841. 5. Mol A. Imaging methods in periodontology. Periodontol 2000 2004;34:34–48. 6. Tugnait A, Carmichael F. Use of radiographs in the diagnosis of periodontal disease. Dent Update 2005;32:536–538; 541–532. 7. Bragger U. Radiographic parameters: biological significance and clinical use. Periodontol 2000 2005;39:73–90. 8. Highfield J. Diagnosis and classification of periodontal disease. Aust Dent J 2009;54(1 Suppl):S11–S26. 9. Armitage GC. Development of a classification system for periodontal diseases and conditions. Ann Periodontol 1999;4:1–6. S41 EF Corbet et al. 10. Armitage GC. Periodontal diagnosis and classification of periodontal diseases. Periodontol 2000 2004;34:9–21. 11. CatonJ, Greenwell H, Mahanonda R, et al. Consensus report:dental plaque-induced gingival diseases. Ann Periodontol 1999;4:18–19. 12. Lindhe J, Ranney R, Lamster I, et al. Consensus report: chronic periodontitis. Ann Periodontol 1999;4:38. 13. Lang N, Bartold PM, Cullinan M, et al. Consensus report: aggressive periodontitis. Ann Periodontol 1999;4:53. 14. Lang N, Soskolne WA, Greenstein G, et al. Consensus report: necrotizing periodontal diseases. Ann Periodontol 1999;4. 15. Lang N, Soskolne WA, Greenstein G, et al. Consensus report: abscesses of the periodontium. Ann Periodontol 1999;4:83. 32. Akesson L, Hakansson J, Rohlin M. Comparison of panoramic and intraoral radiography and pocket probing for the measurement of the marginal bone level. J Clin Periodontol 1992;19:326– 332. 33. Kim TS, Obst C, Zehaczek S, Geenen C. Detection of bone loss with different X-ray techniques in periodontal patients. J Periodontol 2008;79:1141–1149. 34. Persson RE, Tzannetou S, Feloutzis AG, Bragger U, Persson GR, Lang NP. Comparison between panoramic and intra-oral radiographs for the assessment of alveolar bone levels in a periodontal maintenance population. J Clin Periodontol 2003;30:833– 839. 16. Lang NP, Soskolne WA, Greenstein G, et al. Consensus report: periodontic-endodontic lesions. Ann Periodontol 1999;4:90. 35. American Academy of Periodontology. Parameter on comprehensive periodontal examination. J Periodontol 2000;71:847– 848. 17. Updegrave WJ. The paralleling extension-cone technique in intraoral dental radiography. Oral Surg Oral Med Oral Pathol 1951;4:1250–1261. 36. Greenwell H. Committee on Research, Science and Therapy. Position paper: guidelines for periodontal therapy. J Periodontol 2001;72:1624–1628. 18. Ishikawa I, McGuire MK, Mealey B, et al. Consensus report: localized tooth-related factors that modify or predispose to plaque-induced gingival diseases and periodontitis. Ann Periodontol 1999;4:97. 37. Position paper: diagnosis of periodontal diseases. J Periodontol 2003;74:1237–1247. 19. Australian Radiation Protection and Nuclear Safety Agency. Code of Practice for Radiation Protection in Dentistry. Canberra: Australian Government and ARPANSA, 2005. 38. Grubb JE, Greco PM, English JD, et al. Radiographic and periodontal requirements of the American Board of Orthodontics: a modification in the case display requirements for adult and periodontally involved adolescent and preadolescent patients. Am J Orthod Dentofacial Orthop 2008;134:3–4. 20. Australian Radiation Protection and Nuclear Safety Agency. Safety Guide for Radiation Protection in Dentistry. Canberra: Australian Government and ARPANSA, 2005. 39. Kantor ML, Slome BA. Efficacy of panoramic radiography in dental diagnosis and treatment planning. J Dent Res 1989;68: 810–812. 21. Weems RA, Manson-Hing LR, Jamison HC, Greer DF. Diagnostic yield and selection criteria in complete intraoral radiography. J Am Dent Assoc 1985;110:333–338. 40. Tugnait A, Clerehugh DV, Hirschmann PN. Survey of radiographic practices for periodontal disease in UK and Irish dental teaching hospitals. Dentomaxillofac Radiol 2000;29:376– 381. 22. Zinman E. Dental and legal considerations in periodontal therapy. Periodontol 2000 2001;25:114–130. 23. Svenson B, Soderfeldt B, Grondahl HG. Attitudes of Swedish dentists to the choice of dental X-ray film and collimator for oral radiology. Dentomaxillofac Radiol 1996;25:157–161. 24. Tugnait A, Clerehugh V, Hirschmann PN. Radiographic equipment and techniques used in general dental practice: a survey of general dental practitioners in England and Wales. J Dent 2003; 31:197–203. 25. Tugnait A, Hirschmann PN, Clerehugh V. Validation of a model to evaluate the role of radiographs in the diagnosis and treatment planning of periodontal diseases. J Dent 2006;34: 509–515. 26. Dundar N, Ilgenli T, Kal BI, Boyacioglu H. The frequency of periodontal infrabony defects on panoramic radiographs of an adult population seeking dental care. Community Dent Health 2008;25:226–230. 27. Molander B, Ahlqwist M, Grondahl HG. Panoramic and restrictive intraoral radiography in comprehensive oral radiographic diagnosis. Eur J Oral Sci 1995;103:191–198. 41. Osborne GE, Hemmings KW. A survey of disease changes observed on dental panoramic tomographs taken of patients attending a periodontology clinic. Br Dent J 1992;173:166– 168. 42. Boeddinghaus R, Whyte A. Dental panoramic tomography: an approach for the general radiologist. Australas Radiol 2006;50:526–533. 43. Pepelassi EA, Diamanti-Kipioti A. Selection of the most accurate method of conventional radiography for the assessment of periodontal osseous destruction. J Clin Periodontol 1997;24:557– 567. 44. Pepelassi EA, Tsiklakis K, Diamanti-Kipioti A. Radiographic detection and assessment of the periodontal endosseous defects. J Clin Periodontol 2000;27:224–230. 45. Cosyn J, De Bruyn H. Interclinician disparity in periodontal decision making: need for consensus statements on surgical treatment. J Periodontal Res 2007;42:311–317. 46. Needleman IG, Worthington HV, Giedrys-Leeper E, Tucker RJ. Guided tissue regeneration for periodontal infra-bony defects. Cochrane Database Syst Rev 2006:CD001724. 28. Jenkins WM, Brocklebank LM, Winning SM, Wylupek M, Donaldson A, Strang RM. A comparison of two radiographic assessment protocols for patients with periodontal disease. Br Dent J 2005;198:565–569; discussion 557; quiz 586. 47. Klein F, Kim TS, Hassfeld S, et al. Radiographic defect depth and width for prognosis and description of periodontal healing of infrabony defects. J Periodontol 2001;72:1639–1646. 29. Rohlin M, Kullendorff B, Ahlqwist M, Henrikson CO, Hollender L, Stenstrom B. Comparison between panoramic and periapical radiography in the diagnosis of periapical bone lesions. Dentomaxillofac Radiol 1989;18:151–155. 48. Eickholz P, Horr T, Klein F, Hassfeld S, Kim TS. Radiographic parameters for prognosis of periodontal healing of infrabony defects: two different definitions of defect depth. J Periodontol 2004;75:399–407. 30. Akesson L, Rohlin M, Hakansson J, Hakansson H, Nasstrom K. Comparison between panoramic and posterior bitewing radiography in the diagnosis of periodontal bone loss. J Dent 1989;17:266–271. 49. Esposito M, Grusovin MG, Coulthard P, Worthington HV. Enamel matrix derivative (Emdogain) for periodontal tissue regeneration in intrabony defects. Cochrane Database Syst Rev 2005:CD003875. 31. Akesson L, Rohlin M, Hakansson J. Marginal bone in periodontal disease: an evaluation of image quality in panoramic and intra-oral radiography. Dentomaxillofac Radiol 1989;18:105– 112. 50. Sculean A, Schwarz F, Chiantella GC, Arweiler NB, Becker J. Nine-year results following treatment of intrabony periodontal defects with an enamel matrix derivative: report of 26 cases. Int J Periodontics Restorative Dent 2007;27:221–229. S42 ª 2009 Australian Dental Association Radiographs for diagnosis and management 51. Pontoriero R, Wennstrom J, Lindhe J. The use of barrier membranes and enamel matrix proteins in the treatment of angular bone defects. A prospective controlled clinical study. J Clin Periodontol 1999;26:833–840. 52. Heden G, Wennstrom J, Lindhe J. Periodontal tissue alterations following Emdogain treatment of periodontal sites with angular bone defects. A series of case reports. J Clin Periodontol 1999;26:855–860. 53. Sculean A, Windisch P, Keglevich T, Gera I. Histologic evaluation of human intrabony defects following non-surgical periodontal therapy with and without application of an enamel matrix protein derivative. J Periodontol 2003;74:153–160. 54. Gutierrez MA, Mellonig JT, Cochran DL. Evaluation of enamel matrix derivative as an adjunct to non-surgical periodontal therapy. J Clin Periodontol 2003;30:739–745. 55. Giannopoulou C, Andersen E, Brochut P, Plagnat D, Mombelli A. Enamel matrix derivative and systemic antibiotics as adjuncts to non-surgical periodontal treatment: biologic response. J Periodontol 2006;77:707–713. 56. Ramesh A, Tyndall DA, Ludlow JB. Evaluation of a new digital panoramic system: a comparison with film. Dentomaxillofac Radiol 2001;30:98–100. 57. Ridao-Sacie C, Segura-Egea JJ, Fernandez-Palacin A, BullonFernandez P, Rios-Santos JV. Radiological assessment of periapical status using the periapical index: comparison of periapical radiography and digital panoramic radiography. Int Endod J 2007;40:433–440. 58. Pecoraro M, Azadivatan-le N, Janal M, Khocht A. Comparison of observer reliability in assessing alveolar bone height on direct digital and conventional radiographs. Dentomaxillofac Radiol 2005;34:279–284. 59. Teeuw WJ, Coelho L, Silva A, et al. Validation of a dental image analyzer tool to measure alveolar bone loss in periodontitis patients. J Periodontal Res 2009;44:94–102. 60. Li G, Engstrom PE, Nasstrom K, Lu ZY, Sanderink G, Welander U. Marginal bone levels measured in film and digital radiographs corrected for attenuation and visual response: an in vivo study. Dentomaxillofac Radiol 2007;36:7–11. radiography. A methodological study. J Clin Periodontol 1988; 15:27–37. 67. Woo BM, Zee KY, Chan FH, Corbet EF. In vitro calibration and validation of a digital subtraction radiography system using scanned images. J Clin Periodontol 2003;30:114–118. 68. Lai SM, Zee KY, Lai MK, Corbet EF. Clinical and radiographic investigation of the adjunctive effects of a low-power He-Ne laser in the treatment of moderate to advanced periodontal disease: a pilot study. Photomed Laser Surg 2009;27:287–293. 69. Cury PR, Araujo NS, Bowie J, Sallum EA, Jeffcoat MK. Comparison between subtraction radiography and conventional radiographic interpretation during long-term evaluation of periodontal therapy in Class II furcation defects. J Periodontol 2004;75:1145–1149. 70. Hwang YJ, Fien MJ, Lee SS, et al. Effect of scaling and root planing on alveolar bone as measured by subtraction radiography. J Periodontol 2008;79:1663–1669. 71. Naito T, Hosokawa R, Yokota M. Three-dimensional alveolar bone morphology analysis using computed tomography. J Periodontol 1998;69:584–589. 72. Pistorius A, Patrosio C, Willershausen B, Mildenberger P, Rippen G. Periodontal probing in comparison to diagnosis by CT-scan. Int Dent J 2001;51:339–347. 73. Mengel R, Candir M, Shiratori K, Flores-de-Jacoby L. Digital volume tomography in the diagnosis of periodontal defects: an in vitro study on native pig and human mandibles. J Periodontol 2005;76:665–673. 74. Misch KA, Yi ES, Sarment DP. Accuracy of cone beam computed tomography for periodontal defect measurements. J Periodontol 2006;77:1261–1266. 75. Mol A, Balasundaram A. In vitro cone beam computed tomography imaging of periodontal bone. Dentomaxillofac Radiol 2008;37:319–324. 76. Vandenberghe B, Jacobs R, Yang J. Detection of periodontal bone loss using digital intraoral and cone beam computed tomography images: an in vitro assessment of bony and ⁄ or infrabony defects. Dentomaxillofac Radiol 2008;37:252–260. 61. Li G, Engstrom PE, Welander U. Measurement accuracy of marginal bone level in digital radiographs with and without color coding. Acta Odontol Scand 2007;65:254–258. 77. Noujeim M, Prihoda T, Langlais R, Nummikoski P. Evaluation of high-resolution cone beam computed tomography in the detection of simulated interradicular bone lesions. Dentomaxillofac Radiol 2009;38:156–162. 62. Henriksson CH, Stermer EM, Aass AM, Sandvik L, Moystad A. Comparison of the reproducibility of storage phosphor and film bitewings for assessment of alveolar bone loss. Acta Odontol Scand 2008;66:380–384. 78. Walter C, Kaner D, Berndt DC, Weiger R, Zitzmann NU. Three-dimensional imaging as a pre-operative tool in decision making for furcation surgery. J Clin Periodontol 2009;36:250– 257. 63. Lanning SK, Best AM, Temple HJ, Richards PS, Carey A, McCauley LK. Accuracy and consistency of radiographic interpretation among clinical instructors in conjunction with a training program. J Dent Educ 2006;70:545–557. 64. Gomes-Filho IS, Sarmento VA, de Castro MS, et al. Radiographic features of periodontal bone defects: evaluation of digitized images. Dentomaxillofac Radiol 2007;36:256–262. 65. Allen KM, Hausmann E. Analytical methodology in quantitative digital subtraction radiography: analyses of the aluminum reference wedge. J Periodontol 1996;67:1317–1321. 66. Bragger U, Pasquali L, Rylander H, Carnes D, Kornman KS. Computer-assisted densitometric image analysis in periodontal ª 2009 Australian Dental Association Address for correspondence: Professor Esmonde Corbet Periodontology Prince Philip Dental Hospital 34 Hospital Road Hong Kong Email: efcorbet@hkusua.hku.hk S43