Journal of Antimicrobial Chemotherapy (2009) 64, 109– 117
doi:10.1093/jac/dkp132
Advance Access publication 27 April 2009
Pharmacokinetic variability of antiretroviral drugs and correlation
with virological outcome: 2 years of experience in routine
clinical practice
Massimiliano Fabbiani1*, Simona Di Giambenedetto1, Laura Bracciale1, Alessandra Bacarelli2,
Enzo Ragazzoni2, Roberto Cauda1, Pierluigi Navarra2 and Andrea De Luca1
1
Institute of Clinical Infectious Diseases, Catholic University, Rome, Italy; 2Institute of Pharmacology,
Catholic University, Rome, Italy
Received 9 December 2008; returned 30 January 2009; revised 17 March 2009; accepted 18 March 2009
Objectives: To assess the inter-individual and intra-individual plasma concentration variabilities of
non-nucleoside reverse transcriptase inhibitors (NNRTIs) and protease inhibitors (PIs) in routine
clinical practice and to investigate their relationships with virological failure.
Methods: We retrospectively enrolled HIV-infected patients undergoing therapeutic drug monitoring
(TDM) of NNRTIs and PIs during routine outpatient visits. Plasma drug concentrations were measured
by HPLC-UV and were considered therapeutic if above the proposed minimum efficacy trough concentration. Inter-individual and intra-individual variabilities were evaluated through the coefficient of
variation (CV).
Results: A total of 457 PI and 172 NNRTI plasma concentrations were measured from 363 patients (HIVRNA <50 copies/mL in 70.8%, median CD4 count 434 cells/mm3). NNRTIs showed less inter-individual
(CVinter 54.8% versus 84.3%) and intra-individual (CVintra 19.0% versus 38.1%) pharmacokinetic variabilities than PIs. Intra-individual variability was constantly lower than inter-individual variability for each
drug. Subtherapeutic drug concentrations were observed in 106 samples (16.9%). Older age (P 50.020)
and higher viral load (P 50.013) were associated with subtherapeutic levels. Patients with therapeutic
levels had a viral load of <50 copies/mL more frequently than those with subtherapeutic levels (74.8%
versus 63.2%, P 50.020). The estimated proportion with virological failure at 24 weeks was 0.21 in
patients with suboptimal baseline drug levels and 0.08 in those with optimal levels (P< 0.001). In the
multivariate analysis, therapeutic drug levels showed an independent negative association with virological failure (P5 0.004).
Conclusions: A wide inter-individual and limited intra-individual pharmacokinetic variabilities, together
with the demonstration of a concentration–response relationship, suggest that TDM is a useful tool for
the clinical management of patients treated with NNRTIs or PIs.
Keywords: HIV, therapeutic drug monitoring, inter-individual and intra-individual variability
Introduction
Combination antiretroviral therapy (cART) has markedly
changed the prognosis of HIV-infected patients, reducing
AIDS-related morbidity and mortality.1 Despite its success,
cART still lacks sufficient potency and durability: in fact, in a
proportion of patients, antiretroviral regimens fail to suppress
viral replication in the long term.2 Reasons for treatment failure
are multifactorial and may include poor adherence, development
of antiviral resistance and pharmacokinetic factors.
On the basis of the existence of plasma concentration–response
and concentration–toxicity correlation for non-nucleoside reverse
transcriptase inhibitors (NNRTIs) and protease inhibitors (PIs),
therapeutic drug monitoring (TDM) has been proposed to optimize
the exposure to these agents.3 In fact, differences in drug absorption, distribution, metabolism and elimination among individuals
.....................................................................................................................................................................................................................................................................................................................................................................................................................................
*Corresponding author. Istituto di Clinica delle Malattie Infettive, Università Cattolica del Sacro Cuore, Largo F. Vito 1, 00168 Rome, Italy.
Tel: þ39-0630155366; Fax: þ39-063054519; E-mail: massifab@alice.it
.....................................................................................................................................................................................................................................................................................................................................................................................................................................
109
# The Author 2009. Published by Oxford University Press on behalf of the British Society for Antimicrobial Chemotherapy. All rights reserved.
For Permissions, please e-mail: journals.permissions@oxfordjournals.org
Fabbiani et al.
can determine variable plasma PI and NNRTI concentrations:4 – 7
antiretroviral drug levels may drop below effective concentrations,
promoting treatment failure and selection of drug-resistant virus.
Moreover, drug–drug or drug–food interactions may also
contribute to inter-individual variability.8
A further requirement for the feasibility of TDM in clinical
practice is a low intra-individual variability. Factors that may
influence intra-individual variability could be food interactions,
concomitant medications, inaccurate reporting of medication
timing and non-adherence with regular drug intake.3 However,
data on intra-individual variability of antiretroviral drug concentrations are scarce and additional studies are required to address
this issue.4,9,10
Results of randomized trials evaluating the clinical benefit of
TDM in patients undergoing treatment for HIV are controversial.11 – 17 As a consequence, TDM is only recommended in particular clinical scenarios where drug concentrations are difficult
to predict such as for the management of drug interactions, in
patients with liver impairment, in patients with malabsorption,
during pregnancy and in children.18
We aimed to assess the inter-individual and intra-individual
pharmacokinetic variabilities of NNRTI and PI concentrations
in routine clinical practice. Furthermore, we investigated the
occurrence of subtherapeutic drug concentrations, their correlates
and relationships with subsequent virological failure to assess
the potential relevance of routine TDM use in the clinical
management of patients receiving cART.
Materials and methods
antiretroviral regimen, concomitant medications, CD4 cell count and
HIV-1 RNA load. All subsequent viral load measurements until
48 weeks after baseline were also collected. When available, we analysed the genotypic resistance test performed before TDM and interpreted it according to the ANRS interpretation system (version 17).20
Blood sampling for TDM
The TDM service was systematically available, but since this study
was conducted in the clinical practice and TDM request was left to
the judgement of individual clinicians, criteria for using TDM could
differ. In our department, TDM results are reported to clinicians
together with the time of blood sampling and last drug intake.
Results are interpreted based on clinical and viro-immunological
data: the expert advice of a clinical pharmacologist is always available upon request of the treating clinician. Generally, when subtherapeutic drug levels are found, adherence counselling is performed
and drug interactions are checked. Drug levels can then be
re-evaluated and a dose adjustment is considered if low levels are
still present.
Blood was collected before the morning antiretroviral drug
intake to measure Ctrough and the time of the last drug intake and of
blood sampling were recorded for each patient. In the case of
patients taking efavirenz or atazanavir in the evening hours, middosing interval samples were also collected.
To evaluate pharmacokinetic variability, only samples collected
12+2 or 24+2 h after the last treatment intake were considered in
patients taking drugs twice or once daily, respectively. Nevertheless,
when efavirenz or atazanavir were administered at bedtime, samples
collected 12+2 h after the drug intake were also analysed: however,
in this case, pharmacokinetic variability was measured separately
from the levels measured 24+2 h after drug intake.
Patients
We performed an observational retrospective cohort study. We
enrolled all HIV-infected patients who underwent TDM of NNRTI
and PI plasma concentrations during routine outpatient visits from
1 January 2006 to 31 December 2007 at the Infectious Diseases
Clinic of the ‘Agostino Gemelli’ hospital in Rome, Italy (cohort of
1625 HIV-infected patients of which 1371 on antiretroviral therapy
at study time). To be eligible, patients had to: (i) be receiving a PI
or NNRTI as a component of a cART regimen for at least 4 weeks,
in order to allow for measurement of steady-state plasma antiretroviral concentrations; and (ii) have a measured trough concentration
(Ctrough), or mid-dosing interval concentration for atazanavir or efavirenz given at bedtime. Patients treated with darunavir were
excluded from this analysis given that minimum effective concentrations for this agent have not yet been established. All patients at
the clinical centre gave written, informed consent to be included in
observational studies. This informed consent was approved by the
local institutional Ethics Committee.
At study entry, all patients were treated with dosages currently
recommended for NNRTIs and boosted or unboosted PIs,19 with the
exception of two patients with hepatic impairment who were taking
unboosted saquinavir 1000 mg twice daily. The following demographic, clinical and laboratory variables were collected for each
subject at the time of TDM sampling (baseline): gender, age, weight,
ethnicity, co-infection with hepatitis B virus (HBV) or hepatitis C
virus (HCV), conditions that may impair drug exposure ( pregnancy,
cirrhosis, renal and gastrointestinal impairment), risk factors for HIV
infection, previous exposure to suboptimal therapy (defined as an
antiretroviral therapy based on a single or dual agents), previous
virological failure, history of AIDS-defining events, current
Determination of plasma drug levels
Drug levels were measured by a validated HPLC-UV method,21
modified for the quantification of all investigated antiretroviral drugs
(limit of quantification 0.05 mg/L).
Briefly, blood samples (5 mL) were drawn into EDTA tubes and
transported on ice to the laboratory, then immediately centrifuged
for 10 min at 2000 g at 48C. Plasma was decanted and stored at
2208C until analysis.
For the preparation of internal quality controls (QCs) used for
the validation of the assay, independent stock and working solutions
containing the compound of interest were prepared and spiked in
blank human plasma to achieve concentrations of 50, 500 and
5000 ng/mL (low, medium and high concentration, respectively).
Validation of the assay was performed during 5 separate days.
Accuracy of the assay was defined as the difference between the
mean values of the QC samples and the expected value; in our
system, such a difference was ,15% for the 500 and 5000 ng/mL
concentrations and ,20% for the 50 ng/mL concentration, for both
intra- and inter-assay variabilities. The precision of the assay was
defined by the coefficient of variation (CV) calculated for each level
of QC concentration in intra- and inter-assay tests; we found CV
values consistently ,15%, or ,20% in the case of the low QC
level. These results met the FDA criteria of acceptability for accuracy and precision of bioanalytical methods.22
The accuracy of the present method was also repeatedly estimated
from the analysis of four sets of two unknown samples of external
QCs from the INSTAND e.V. (Duesseldorf, Germany) (WHO
Collaborating Centre for Quality Assurance and Standardization in
Laboratory Medicine), a QC programme for antiretroviral drugs.
110
Pharmacokinetic variability of antiretroviral drugs
Definition of therapeutic drug levels
Based on previously published data, drug concentrations were considered therapeutic if they were above the proposed minimum efficacy trough concentration: 1.0 mg/mL for efavirenz, 3.0 mg/mL for
nevirapine, 0.15 mg/mL for atazanavir, 0.40 mg/mL (measured as
amprenavir concentration) for fosamprenavir, 0.10 mg/mL for indinavir, 1.0 mg/mL for lopinavir, 0.80 mg/mL for nelfinavir, 0.10 mg/mL
for saquinavir and 20.5 mg/mL for tipranavir.19 For atazanavir administered at bedtime and measured in the morning (C12), a previously
validated efficacy threshold of 0.23 mg/mL was chosen, as
described.23 Ritonavir was only administered in a boosting (nontherapeutic) dose and was not included in the analysis.
Ctrough measurement (or C12 for efavirenz and atazanavir) and
12 because they only monitored darunavir plasma levels.
Finally, a total of 629 plasma antiretroviral concentrations
meeting the selection criteria were measured in 363 patients
(26.5% of the total number of patients on antiretroviral therapy
in our cohort). Table 1 summarizes the demographic and clinical
characteristics of this population.
There were 457 (72.7%) determinations of PIs and 172
(27.3%) of NNRTIs from plasma samples. Atazanavir (n ¼ 229,
36.4%), efavirenz (n¼ 149, 23.7%) and lopinavir (n ¼ 131,
20.8%) were the most frequently measured drugs. A pre-TDM
genotypic resistance test was available in 318 (50.6%) instances:
possible resistance or resistance to the measured antiretroviral
Statistical analysis
Categorical variables were compared with the x 2 test or, when
appropriate, Fisher’s exact test; for continuous variables, comparisons were based on the non-parametric Mann–Whitney U-test.
Inter-individual and intra-individual pharmacokinetic variabilities
were evaluated through the CV calculated as the quotient of the
standard deviation divided by the mean plasma concentration 100.
In the calculation of pharmacokinetic variability, drug measurements below the lower limit of quantification of the assay
(,0.05 mg/L) were arbitrarily considered as having a concentration
of 0.04 mg/L.
For virological failure, the time-to-event analysis was performed
using the Kaplan–Meier method. Follow-up was truncated at the
time of virological failure, the date of interruption of the monitored
drug, the date the patient had their last viral load measured or at
48 weeks after baseline, whichever occurred first. In the main analysis, virological failure was defined as not achieving a viral load ,50
copies/mL after 24 weeks of follow-up in patients with detectable
(.50 copies/mL) baseline HIV-RNA levels; patients with undetectable viral load were considered to fail in case of a rebound to
.1000 copies/mL on a single occasion or to .200 copies/mL on at
least two consecutive instances. In the latter case, the date of the
first viral load .200 copies/mL was used as the date of failure. In a
subgroup analysis, we selected only patients with baseline
HIV-RNA ,200 copies/mL: the same criteria for virological failure
were employed.
Univariate and multivariate Cox’s regression models were used
to investigate predictors of virological failure. All variables tested in
the univariable model were included in the multivariable analysis.
For the association between drug level and virological response,
when more than one plasma concentration was available for the
same patient, we considered each sample separately and evaluated
the subsequent 48 weeks virological response in each instance.
However, we also performed a sensitivity analysis evaluating only
the first sample of a patient or using the average concentration of
multiple samples from each patient.
A two-tailed P value of ,0.05 was considered statistically significant. All analyses were performed using the SPSS Version 13.0
software package (SPSS Inc., Chicago, IL, USA).
Table 1. Patients’ baseline characteristics (n ¼363)
n (%) or median
(inter-quartile range)
Male sex
Age (years)
215 (59.2)
43 (37 –48)
Italian born
314 (86.5)
Ethnicity
Caucasian
Black African
Latin American
others
326 (89.8)
18 (5.0)
14 (3.9)
5 (1.4)
Injecting drug users
89 (24.5)
Pregnancy
15 (4.1)
HBV/HCV co-infection
Time from HIV diagnosis (years)
Past AIDS-defining events
Treatment naive
128 (35.3)
10 (5– 15)
124 (34.2)
66 (18.2)
Past suboptimal therapy
138 (38.0)
Past virological failure
166 (45.7)
Months since starting regimen
9 (3– 19)
Regimen
PI-based
NNRTI-based
PIþ NNRTI
247 (68.0)
100 (27.5)
16 (4.4)
Results
Backbone
TDF þFTC or 3TC
ZDV þ3TC
ABC þ3TC
d4Tþ3TC
others
198 (54.5)
51 (14.0)
36 (9.9)
9 (2.5)
69 (19.0)
Patients’ characteristics and plasma drug concentrations
CD4 cell count (cells/mm3)
434 (286 –621)
From January 2006 to December 2007, TDM was performed in
448 out of the 1371 patients on antiretroviral therapy in our
cohort. Of these, 73 were excluded because their drug level
measurement did not correspond to the definitions required for
Viral load (copies/mL)
49 (49 –81)
TDF, tenofovir; FTC, emtricitabine; 3TC, lamivudine; ZDV, zidovudine;
ABC, abacavir; d4T, stavudine.
111
Fabbiani et al.
drug was found in 15.4% (n ¼ 49) of these, according to the
ANRS interpretation system.
Drug concentration was optimal in 83.1% of the cases; subtherapeutic concentration was observed in 106 measurements
(16.9%), including 47 (7.5%) in which drugs were below the
limit of detection. After the detection of subtherapeutic drug
levels, treatment changes were performed in only 11 of the 106
(10.4%) cases (4 dose adjustments and 7 drug substitutions).
Inter-individual and intra-individual drug concentration
variabilities
Inter-individual variability was evaluated in a subset of 541
drug measurements: 232 determinations were performed on
samples collected 12+2 h after the last treatment intake for
twice-daily regimens and 68 on samples collected 24+2 h for
once-daily regimens; in addition, 111 efavirenz and 130 atazanavir measurements were performed 12+2 h after the last intake
because the drugs were administered at bedtime. Inter-individual
coefficients of variation (CVinter) are shown in Table 2. Overall,
a high inter-individual variability was observed. When drugs
were categorized according to classes, NNRTIs showed less
inter-individual variability than PIs fmedian CVinter 54.8%
[inter-quartile range (IQR) 52.5– 70.0] versus 84.3% (IQR
79.8 –127.5), respectively; P ¼ 0.102g.
When more than one measurement of the same drug was
available for the same patient, intra-individual pharmacokinetic
variability was evaluated. The median interval between the first
and the last measurement used to calculate intra-individual
variability was 9 months (IQR 4 – 13). Table 2 shows median
intra-individual coefficients of variation (CVintra) for each drug.
NNRTIs showed less intra-individual variability than
PIs: median CVintra 19.0% (IQR 10.4– 40.4) versus 38.1% (IQR
15.3 –73.8), respectively (P ¼ 0.011). Intra-individual variability
was lower than inter-individual variability: comparing both drug
classes and each drug, CVintra appeared constantly lower than
CVinter (Table 2).
Correlates of therapeutic drug concentrations
Patients’ demographic and clinical characteristics, split according to the presence of subtherapeutic or therapeutic drug levels,
are shown in Table 3. In a univariate analysis, older age
(P ¼ 0.020) and higher contemporary viral load (P ¼ 0.013) were
statistically associated with subtherapeutic levels. When TDM
was performed, patients with therapeutic levels had a viral load
of ,50 copies/mL more frequently than those with subtherapeutic levels (74.8% versus 63.2%, P ¼ 0.020). No statistically significant differences across the two groups were observed with
regard to gender, weight, ethnicity, HBV/HCV co-infection,
pregnancy, concomitant use of cytochrome P450 inducers or
gastric acid-reducing agents. Of note, in the only patient with
documented malabsorption (Crohn’s disease), the drug level was
suboptimal.
Therapeutic concentrations were observed in 154 (89.5%)
NNRTI measurements and in 369 (80.7%) PI measurements
(P ¼ 0.012). Both NNRTIs and boosted PIs reached optimal
plasma levels in a significantly higher percentage than
unboosted PIs (89.5% and 85.9% versus 60.5%, respectively;
P, 0.001 for each comparison). Among the samples with subtherapeutic concentrations, drugs were below the limit of detection in near half of the cases (47/106, 44.3%) and PIs were more
frequently undetectable than NNRTIs (45/88, 51.1% versus
2/18, 11.1%, P ¼ 0.004).
Table 4 gives proportions of measurements showing therapeutic and subtherapeutic levels for each drug. Therapeutic
Table 2. Inter-individual (CVinter) and intra-individual (CVintra) variabilities of each antiretroviral drug
Inter-individual variability
EFVa12 h
EFVb24 h
NVP
ATVa12 h
ATVb24 h
FPV
IDV
LPV
NFV
SQV
TPV
Intra-individual variability
samples, n
concentration, mean (SD)
CVinter (%)
patients, n
no. of samples, median (range)
CVintra, median (IQR)
111
6
21
130
62
41
5
121
16
15
12
2.53 (2.16)
2.01 (1.10)
5.77 (2.89)
1.64 (1.4)
0.62 (0.88)
2.26 (1.83)
0.89 (0.74)
7.06 (4.48)
1.88 (1.44)
0.81 (1.15)
37.45 (42.42)
85.1
54.8
50.1
85.4c
141.5e
80.8g
83.2
63.4
76.9
140.8
123.1
22
2 (2–6)
19.9 (10.3 –41.6)
5
23d
10f
9
1
22
2
4
2
2 (2–3)
2 (2–6)
2 (2–6)
3 (2–4)
4
2 (2–4)
2 (2–2)
2 (2–4)
3 (2–3)
16.3 (12.0 –27.1)
29.9 (14.2 –96.6)
44.2 (31.5 –54.8)
28.2 (20.5 –34.2)
66.9
37.4 (11.8 –66.7)
80.2 (53.6 –106.8)
109.6 (73.2 –128.3)
40.2 (39.1 –41.2)
EFV, efavirenz; NVP, nevirapine; ATV, atazanavir; FPV, fosamprenavir; IDV, indinavir; LPV, lopinavir; NFV, nelfinavir; SQV, saquinavir; TPV, tipranavir;
SD, standard deviation.
a
Administered at bedtime and measured 12+2 h after intake.
b
Measured 24+2 h after intake.
c
ATV12 h unboosted (n ¼41), CVinter 105.9%; ATV12 h/ritonavir (n ¼89), CVinter 74.7%.
d
ATV12 h unboosted, n¼10 patients; ATV12 h/ritonavir, n¼13 patients.
e
ATV24 h unboosted (n ¼20), CVinter 78.0%; ATV24 h/ritonavir (n¼42), CVinter 115.3%.
f
ATV24 h unboosted, n ¼3 patients; ATV24 h/ritonavir, n¼7 patients.
g
FPV unboosted (n¼8), CVinter 96.2%; FPV/ritonavir (n ¼33), CVinter 75.4%.
112
Pharmacokinetic variability of antiretroviral drugs
Table 3. Comparison of demographic and clinical characteristics in samples with therapeutic and subtherapeutic plasma
antiretroviral concentrations
Male sex
Age (years)
Weight (kg)
Caucasian
HBV/HCV co-infection
Pregnancy
Injection drug users
Treatment naive
Use of cytochrome P450 inducersa
Use of gastric-acid-reducing drugsb
CD4 cell count (cells/mm3)
Viral load (copies/mL)
Viral load ,50 copies/mL at TDM
Therapeutic levels (n¼ 523, 83.1%)
Subtherapeutic levels (n ¼106, 16.9%)
P
323 (61.8)
43 (38 –48)
69 (59 –78)
466 (89.1)
190 (36.3)
16 (3.1)
128 (24.5)
85 (16.3)
21 (4.0)
13 (2.5)
454 (297 –664)
49 (49 –61)
391 (74.8)
64 (60.4)
45 (41 –49)
68 (58 –78)
96 (90.6)
40 (37.7)
4 (3.8)
31 (29.2)
15 (14.2)
4 (3.8)
5 (4.7)
473 (332 –699)
49 (49 –175)
67 (63.2)
0.875
0.020
0.537
0.697
0.870
0.937
0.364
0.693
1.000
0.205
0.612
0.013
0.020
Values are expressed as n (%) or median (IQR).
a
Rifamycins and phenobarbital.
b
Proton pump inhibitors, H2 receptor antagonists and antacids.
concentrations were reached most frequently by efavirenz
(89.9%) and less frequently by tipranavir (50.0%). Efavirenz and
lopinavir achieved optimal levels more often than atazanavir,
saquinavir and tipranavir (89.9% and 89.3% versus 79%, 62.5%
and 50.0%, respectively, P,0.05). For single PI drugs, those
boosted with ritonavir were prone to achieve therapeutic levels
more frequently than those without ritonavir boosting; in
particular, statistically significant differences were observed for
atazanavir versus atazanavir/ritonavir (60.0% versus 87.4%
therapeutic levels, respectively, P,0.001).
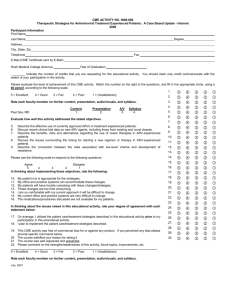
Predictors of virological response
A follow-up was available in 589 instances: virological failure
occurred in 17.1% of these with a median time to virological
failure of 17 weeks (range 0 –48). The association of drug
exposure with subsequent time to virological failure is illustrated
in Figure 1. In the whole population, the estimated proportion
with virological failure at 24 weeks was 0.21 in patients with
suboptimal baseline drug levels and 0.08 in those with optimal
plasma levels (log-rank test: P,0.001) (Figure 1a). In the subgroup of patients with baseline viral load ,200 copies/mL
(n ¼ 491), the estimated proportion with virological failure at
24 weeks was 0.09 in patients with suboptimal baseline drug
levels and 0.03 in those with optimal plasma levels (log-rank
test: P ¼0.012) (Figure 1b).
Predictors of virological failure were investigated by Cox’s
regression model (Table 5). In a univariate analysis, non-Italian
born patients, Black African versus Caucasian ethnicity, injecting drug users, patients with a longer time from HIV diagnosis,
those with a history of AIDS-defining events, those with previous exposure to suboptimal therapy, those on a more advanced
treatment line and higher baseline viral load showed a higher
risk of virological failure. Conversely, older patients, those with
no genotypic resistance test previously performed, those on
NNRTI-based as compared with boosted PI-based regimens,
those with higher CD4 cell count and with therapeutic drug
levels showed a lower risk of virological failure. In the multivariate analysis, history of AIDS-defining events, the use of
stavudine þ lamivudine as compared with tenofovir þ lamivudine
or emtricitabine as NRTI backbone, the use of a boosted
PI-based regimen and higher viral load showed an independent
association with virological failure, while older age and therapeutic drug levels conveyed a lower risk of virological failure.
Optimal drug levels were confirmed to be independent negative
predictors of virological failure also in the subgroup of patients
with baseline HIV-RNA ,200 copies/mL [adjusted hazard ratio
(aHR) 0.434, 95% confidence interval (CI) 0.218 – 0.865,
P ¼ 0.018].
In sensitivity analyses, using only the first sample or the
average concentration of multiple samples from each patient,
results were comparable to those reported in the main analysis:
first sample results, therapeutic versus subtherapeutic levels,
aHR 0.401, 95% CI 0.230 – 0.702, P ¼ 0.001; average concentration aHR 0.456, 95% CI 0.225 – 0.816, P ¼ 0.008.
Discussion
The demonstration of a relationship between plasma levels of
PIs and NNRTIs and their efficacy or toxicity suggests that
monitoring the concentrations of these drugs can be useful for
the clinical management of patients on cART. However, clinical
trials evaluating TDM implementation have shown conflicting
results: in fact, in patients undergoing TDM-driven interventions, a significantly higher virological suppression rate, demonstrated in some studies,11,12 has not always been confirmed.13 – 17
This highlights the need for new studies to explore this
approach.
We analysed the use of TDM in the clinical practice in a
large cohort of HIV-infected outpatients, represented mainly by
subjects with a virologically and immunologically controlled
disease. Since clinicians could be more likely to seek TDM in
patients who are suspected of having altered drug levels (e.g. for
113
1
All instances (n = 589)
Cumulative proportion with virological failure
1.0
0.8
0.6
P < 0.001
0.4
0.2
0.0
0
(b)
10
20
30
Weeks of follow-up
40
50
Instances with baseline viral load <200 copies/mL (n = 491)
1.0
Cumulative proportion with virological failure
EFV, efavirenz; NVP, nevirapine; ATV, atazanavir; FPV, fosamprenavir; IDV, indinavir; LPV, lopinavir; NFV, nelfinavir; SQV, saquinavir; TPV, tipranavir.
a
Boosted versus unboosted.
5 (35.7%)
9 (64.3%)
2
1 (50%)
1 (50%)
14
20 (12.6%)
4 (11.4%)
1 (20%)
139 (87.4%)
31 (88.6%)
4 (80%)
28 (40%)
3 (37.5%)
0 (0%)
42 (60%)
5 (62.5%)
1 (100%)
15 (10.1%)
3 (13%)
48 (21%)
7 (6.3%)
1 (16.7%)
14 (10.7%)
5 (27.8%)
6 (37.5%)
7 (50%)
134 (89.9%)
20 (87%)
181 (79%)
36 (83.7%)
5 (83.3%)
117 (89.3%)
13 (72.2%)
10 (62.5%)
7 (50%)
149
23
229
43
6
131
18
16
14
98
16
146
26
3
96
14
9
10
EFV
NVP
ATV
FPV
IDV
LPV
NFV
SQV
TPV
patients
samples
subtherapeutic
70
8
1
subtherapeutic
159
35
5
subtherapeutic
therapeutic
<0.001
0.106
1
(a)
therapeutic
samples
therapeutic
samples
Boosted
Unboosted
Total
Table 4. Percentages of therapeutic/subtherapeutic plasma levels for each antiretroviral drug and after dividing PIs according to pharmacokinetic boosting
Pa
Fabbiani et al.
0.8
0.6
0.4
P = 0.012
0.2
0.0
0
10
20
30
Weeks of follow-up
40
50
Figure 1. Kaplan– Meier estimates of the time to virological failure in
patients with subtherapeutic (broken line) and therapeutic (continuous line)
drug levels.
poor adherence, drug interactions, liver impairment or other concomitant illnesses), the study design could have introduced
potential sources of biases that must be considered when interpreting our results. Nonetheless, the data obtained can add further
scientific support to the use of TDM in the clinical practice.
In the studied population, the majority of patients (83.1%)
had therapeutic drug levels. However, subtherapeutic concentrations were detected in 16.9% of samples: these subjects
showed an HIV-RNA ,50 copies/mL in a lower proportion than
those with therapeutic levels. In these circumstances, viral replication, even at a low level, can increase the risk of developing
drug resistance, promoting treatment failure and limiting the
future use of antiretrovirals.24
In our population, unboosted PI plasma levels were more frequently suboptimal than ritonavir boosted PIs and NNRTIs.
114
Pharmacokinetic variability of antiretroviral drugs
Table 5. Predictors of virological failure (uni- and multivariate Cox’s regression models)
Univariate analysis
Variable
Sex (female versus male)
Multivariate analysis
HR for virological failure (95% CI)
P
HR for virological failure (95% CI)
P
0.826 (0.548 –1.244)
0.360
0.656 (0.407–1.057)
0.083
a
Age (per 10 year more)
0.778 (0.619 –0.977)
0.031
0.701 (0.526–0.936)
0.016
Non-Italian born versus Italian born
1.737 (1.064 –2.834)
0.027
2.810 (0.902–8.750)
0.075
Ethnicity
Caucasian (ref.)
African
Latin American
others
1.00
2.302 (1.115 –4.754)
1.296 (0.566 –2.966)
1.143 (0.281 –4.645)
Injecting drug users (yes versus no)
0.152
0.039
0.024
0.540
0.852
1.00
1.163 (0.329–4.112)
0.281 (0.069–1.153)
0.168 (0.025–1.144)
0.815
0.078
0.068
1.548 (1.021 –2.346)
0.040
1.781 (0.925–3.431)
0.084
HBV/HCV co-infection
1.367 (0.922 –2.025)
0.120
0.867 (0.458–1.641)
0.660
Time from HIV diagnosis (per 1 year more)
1.045 (1.010 –1.080)
0.011
1.048 (0.996–1.103)
0.071
Past AIDS-defining events
1.882 (1.273 –2.783)
0.002
2.248 (1.594–3.762)
<0.001
1.613 (1.089 –2.391)
0.017
1.428 (0.794–2.570)
0.234
Past suboptimal therapy (yes versus no)
Susceptibility to measured drug in pre-TDM GRT
full susceptibility (ref.)
partial resistance or resistance
no previous GRT
b
0.152
0.001
1
1.583 (0.879 –2.851)
0.517 (0.335 –0.798)
Treatment line (per 1 line more)
1.305 (1.077 –1.580)
Type of NRTI backbone
TDF þFTC/3TC (ref.)
ZDVþ 3TC
ABCþ 3TC
d4Tþ3TC
others
1.00
1.198 (0.653 –2.197)
0.970 (0.494 –1.907)
1.892 (0.685 –5.229)
0.799 (0.482 –1.325)
Type of ‘third’ drug
PI/ritonavir (ref.)
NNRTI
PI unboosted
PIþ NNRTI
1.00
0.484 (0.276 –0.849)
0.692 (0.388 –1.233)
0.486 (0.223 –1.059)
Baseline viral load (per 1 log more)
0.126
0.003
1
1.099 (0.568–2.125)
0.627 (0.380–1.033)
0.780
0.067
0.007
1.134 (0.887–1.450)
0.315
0.539
0.560
0.930
0.219
0.385
0.093
1.00
1.187
1.470
4.187
0.845
(0.582–2.423)
(0.692–3.120)
(1.379–12.719)
(0.474–1.505)
0.029
0.637
0.316
0.012
0.567
0.006
0.011
0.211
0.069
1.00
0.562 (0.291–1.088)
0.484 (0.240–0.979)
0.298 (0.123–0.723)
0.087
0.043
0.007
2.239 (1.929 –2.599)
<0.001
2.098 (1.669–2.638)
<0.001
CD4 cell count (per 100 cells more)
0.884 (0.816 –0.958)
0.003
0.969 (0.892–1.052)
0.446
Therapeutic drug levels (versus subtherapeutic)
0.461 (0.300 –0.710)
<0.001
0.474 (0.286–0.787)
0.004
HR, hazard ratio; GRT, genotypic resistance test; NRTI, nucleoside/nucleotide reverse transcriptase inhibitor; TDF, tenofovir; FTC, emtricitabine;
3TC, lamivudine; ZDV, zidovudine; ABC, abacavir; d4T, stavudine.
a
When samples obtained from adolescents were excluded: HR 0.681, 95% CI 0.497– 0.934, P¼0.017.
b
According to the ANRS interpretation system.
Unboosted PI regimens are used in certain patient categories to
decrease adverse events, but these subjects are more prone to
develop low plasma concentrations with a higher risk of virological failure. Therefore, TDM can be particularly useful in this
setting where inter-individual pharmacokinetic variability is particularly striking.
When only samples with subtherapeutic drug concentrations
were considered, PIs were more frequently undetectable than
NNRTIs. This is in part due to the pharmacokinetic properties
of NNRTIs that have a long half-life and can be found in
plasma even days after the intake of the last dose.25 HIV treatment requires the concomitant use of multiple drugs for sustained viral suppression but, when TDM is performed using
plasma samples, only the concentration of selected agents (PIs
or NNRTIs) is usually monitored: this may not be adequate
under all circumstances. However, we found a strong association
115
Fabbiani et al.
between subtherapeutic plasma concentrations and higher rates
of virological failure during follow-up. Moreover, when analysing predictors of virological outcome, optimal drug levels were
independently associated with a lower risk of virological failure.
We investigated several factors thought to influence
inadequate exposure to antiretroviral drugs. The lack of association between antiretroviral concentrations and investigated features (gender, ethnicity, body weight, injection drug use,
pregnancy, HBV or HCV co-infection) shows that, in clinical
practice, it is often difficult to identify patients predisposed to
developing low plasma drug levels, suggesting the utility of
routine TDM to improve cART success. We also investigated
whether the use of cytochrome CYP3A4 inducers or acidreducing agents could affect drug concentrations in our population and found no associations with the development of
subtherapeutic drug levels (Table 3). However, this study was
not designed to assess drug interactions in detail and from our
data we can only conclude that medications potentially interacting with the measured drug were administered in 9/106 (8.5%)
cases with subtherapeutic levels and in 34/523 (6.5%) cases
with therapeutic levels.
An important factor contributing to the prevalence of suboptimal plasma concentrations in our cohort may have been an
incomplete adherence to the prescribed therapy. In fact, nearly
half of all samples designated as subtherapeutic exhibited no
trace of drugs. Since our study was conducted retrospectively in
clinical practice, we could not assess the degree of adherence.
However, TDM has been claimed as an objective, although
incomplete, method to determine adherence and it may be
helpful for this purpose especially if used in conjunction with
other tools ( patients self-reporting, pill counts, pharmacy
records and electronic monitoring).
A potential limitation of our study is that we could not adjust
efficacy thresholds for individual drugs based on previously
selected drug resistance mutations. In subjects harbouring partially resistant viral strains, thresholds used to define therapeutic
range might have been inadequate, since reference concentrations for wild-type virus could be insufficient to suppress subpopulations with reduced susceptibility. However, current
guidelines18,19,26 do not include efficacy thresholds for patients
harbouring partially resistant virus (with the exception of tipranavir) and no definite data are yet available on plasma drug
minimum effective concentrations for those patients. We
addressed whether reduced susceptibility to the measured drug
could influence the association between therapeutic drug levels
and subsequent virological failure in a multivariable analysis,
but the adjusted association between drug levels and virological
outcome was still statistically significant. Nonetheless, only a
total of 7.8% of the studied cases’ virus had some level of resistance to the measured drugs, therefore our results can be mainly
applied to individuals carrying drug-susceptible virus.
Prospective studies are needed to define the efficacy thresholds
in patients harbouring drug-resistant viruses.
Many reports have demonstrated that, if antiretroviral concentrations are too low or too high, patients may have serious clinical consequences (i.e. insufficient virological response or
development of toxicity).4,5,27 Therefore, it is important to
increase our knowledge about the extent of inter-individual pharmacokinetic variability in outpatient routine clinical settings and
about factors that contribute to it. Our study confirmed high
levels of inter-patient variability for all antiretroviral drugs. Of
note, CVinter was more elevated for PIs than for NNRTIs. This
inter-individual variability in drug concentrations can be
explained by differences in absorption, distribution, metabolism
and elimination among different patients. Moreover, poor adherence, concomitant diseases, drug interactions and food requirements could also have played roles, particularly for PIs.
Intra-individual pharmacokinetic variability is a critical issue
in evaluating the utility of TDM. Since in the clinical practice it
is often difficult to obtain multiple samples for drug measurement from the same patient, clinicians must assume that interday variation of drug levels in each subject is minimal.
However, few studies have addressed this issue, sometimes with
conflicting results,4,9,10 and additional data are required,
especially for recently introduced drugs. We found a limited
intra-individual variability in our population, with lower values
for NNRTIs than for PIs (CVintra 19.0% versus 38.1%). CVintra
varied widely between drugs, with a minimum for nevirapine
(16.3%) and a maximum for saquinavir (109.6%). Noteworthily,
however, intra-individual variability was constantly lower than
inter-individual variability for drug classes as well as for individual antiretrovirals: this observation is an important prerequisite for the feasibility of TDM in clinical practice.
In conclusion, TDM seems to be a promising strategy to
increase the success of antiretroviral therapy but to date it has
been applied only in selected groups of patients. Our findings
about pharmacological features of antiretroviral drugs, such as
wide inter-individual variability and limited intra-individual variability, together with the demonstration of a concentration–
response relationship using pre-established efficacy thresholds,
suggest that TDM is a useful monitoring tool for patients on PI or
NNRTI therapy. However, well-designed trials are required in
order to assess the potential utility of TDM-based intervention
before it can be definitively recommended for routine clinical
practice.
Acknowledgements
The technicians of the Institute of Pharmacology are thanked for
their help for analysing the TDM samples.
Funding
This work was supported by Istituto Superiore di Sanità,
Ministero della Salute, Programma Nazionale AIDS, grants
50F.10, 30F.17 and 30F.18 and by EU contract FP6-2005IST-2004-027446 (Virolab) to A. D. L. Janssen-Cilag provided
a grant for protocol ‘Valutazione del TDM in corso di HAART
con inibitori della proteasi di nuova generazione’. A. B. was
supported by a grant from Boehringer-Ingelheim.
Transparency declarations
R. C. and A. D. L. have received speaker honoraria from or have
acted as an advisor for GlaxoSmithKline, Bristol – Myers
Squibb, Gilead, Abbott Virology, Boehringer Ingelheim, Merck
Sharp and Dohme, Pfizer and Bayer Diagnostics. P. N. has
received speaker honoraria from Boehringer-Ingelheim,
116
Pharmacokinetic variability of antiretroviral drugs
GlaxoSmithKline, Gilead and Janssen-Cilag. All other authors:
none to declare.
References
1. Palella FJ, Delaney KM, Moorman AC et al. Declining morbidity
and mortality among patients with advanced human immunodeficiency
virus infection. N Engl J Med 1998; 338: 853– 60.
2. Bartlett JA, Fath MJ, Demasi R et al. An updated systematic
overview of triple combination therapy in antiretroviral-naive
HIV-infected adults. AIDS 2006; 16: 2051– 64.
3. Back D, Gatti G, Fletcher C et al. Therapeutic drug monitoring in
HIV infection: current status and future directions. AIDS 2002; 16
Suppl 1: S5–37.
4. Marzolini C, Telenti A, Decosterd LA et al. Efavirenz plasma
levels can predict treatment failure and central nervous system sideeffects in HIV-1-infected patients. AIDS 2001; 15: 71 –5.
5. Veldkamp AI, Weverling GJ, Lange JM et al. High exposure to
nevirapine in plasma is associated with an improved virological
response in HIV-1-infected individuals. AIDS 2001; 15: 1089–95.
6. Torti C, Quiros-Roldan E, Tirelli V et al. Lopinavir plasma levels
in salvage regimens by a population of highly active antiretroviral
therapy-treated HIV-1-positive patients. AIDS Patient Care STDS
2004; 18: 629–34.
7. Molto J, Blanco A, Miranda C et al. Variability in non-nucleoside
reverse transcriptase and protease inhibitors concentrations among
HIV-infected adults in routine clinical practice. Br J Clin Pharmacol
2007; 63: 715–21.
8. Boffito M, Acosta E, Burger D et al. Therapeutic drug monitoring
and drug–drug interactions involving antiretroviral drugs. Antivir Ther
2005; 10: 469–77.
9. Nettles RE, Kieffer TL, Parsons T et al. Marked antiretroviral
variability in antiretroviral concentrations may limit the utility of therapeutic drug monitoring. Clin Infect Dis 2006; 42: 1189– 96.
10. Boffito M, Back DJ, Hoggard PG et al. Intra-individual variability
in lopinavir plasma trough concentrations supports therapeutic drug
monitoring. AIDS 2003; 17: 1107– 8.
11. Fletcher CV, Anderson PL, Kakuda TN et al. Concentrationcontrolled compared with conventional antiretroviral therapy for HIV
infection. AIDS 2002; 16: 551– 60.
12. Burger D, Hugen P, Reiss P et al. Therapeutic drug monitoring
of nelfinavir and indinavir in treatment-naive HIV-1-infected individuals.
AIDS 2003; 17: 1157–65.
13. Clevenbergh P, Garraffo R, Durant J et al. PharmAdapt: a randomised prospective study to evaluate the benefit of therapeutic monitoring of protease inhibitors: 12 week results. AIDS 2002; 16: 2311–5.
14. Bossi P, Peytavin G, Ait-Mohand H et al. GENOPHAR: a randomised study of plasma drug measurements in association with genotypic resistance testing and expert advice to optimise therapy in
patients failing antiretroviral therapy. HIV Med 2004; 5: 352–9.
15. Torti C, Quiros-Roldan E, Regazzi M et al. A randomised
controlled trial to evaluate antiretroviral salvage therapy guided by
rules-based or phenotype-driven HIV-1 genotypic drug-resistance
interpretation with or without concentration-controlled intervention: the
Resistance And Dosage Adapted Regimens (RADAR) Study. Clin
Infect Dis 2005; 40: 1828–36.
16. Khoo SH, Lloyd J, Dalton M et al. Pharmacologic optimisation of
protease inhibitors and nonnucleoside reverse transcriptase inhibitors
(POPIN)—a randomised controlled trial of therapeutic drug monitoring
and adherence support. J Acquir Immune Defic Syndr 2006; 41:
461 –7.
17. Best BM, Goicoechea M, Witt MD et al. A randomised controlled
trial of therapeutic drug monitoring in treatment-naive and experienced
HIV-1-infected patients. J Acquir Immune Defic Syndr 2007; 46:
433 –42.
18. Gazzard B, BHIVA Treatment Guidelines Writing Group. British
HIV Association guidelines for the treatment of HIV-1-infected adults
with antiretroviral therapy 2008. HIV Med 2008; 8: 563–608.
19. Panel on Antiretroviral Guidelines for Adults and Adolescents.
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults
and Adolescents. Department of Health and Human Services, 3
November 2008; 1–139. http://www.aidsinfo.nih.gov/ContentFiles/
AdultandAdolescentGL.pdf (1 December 2008, date last accessed).
20. French ANRS (National Agency for AIDS Research) AC11
Resistance Group. HIV Genotype Interpretation Rules. Version no. 17.
http://www.hivfrenchresistance.org/2008/Algo-2008.pdf
(17
March
2009, date last accessed).
21. Di Giambenedetto S, De Luca A, Villani P et al. Atazanavir and
lopinavir with ritonavir alone or in combination: analysis of pharmacokinetic interaction and predictors of drug exposure. HIV Med 2008; 9:
239 –45.
22. U.S. Food and Drug Administration. Guidance for Industry
Bioanalytical Method Validation. www.fda.gov/cder/guidance/index.htm
(1 December 2008, date last accessed).
23. Fabbiani M, Di Giambenedetto S, Ragazzoni E et al. Atazanavir
(ATV) plasma concentrations at different times after drug uptake:
associations with virologic response and hyperbilirubinemia (Abstract).
J Int AIDS Soc 2008; 11(Suppl 1): P243.
24. Harrigan PR, Hogg RS, Dong WW et al. Predictors of HIV
drug-resistance mutations in a large antiretroviral-naive cohort initiating
triple antiretroviral therapy. J Infect Dis 2005; 191: 339–47.
25. Smith PF, Dicenzo R, Morse GD et al. Clinical pharmacokinetics
of non-nucleoside reverse transcriptase inhibitors. Clin Pharmacokinet
2001; 40: 893–905.
26. La Porte CJL, Back DJ, Blashke TF et al. Updated guidelines to
perform therapeutic drug monitoring for antiretroviral agents. Rev
Antivir Ther 2006; 3: 4–14.
27. Durant J, Clevenbergh P, Garraffo R et al. Importance of protease inhibitors plasma levels in HIV-infected patients treated with
genotypic-guided therapy: pharmacological data from the VIRADAPT
study. AIDS 2000; 14: 1333–9.
117