Polycystic ovary syndrome is associated with negatively variable
advertisement

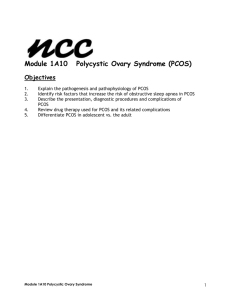
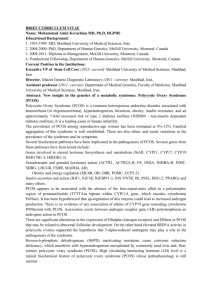
Polycystic ovary syndrome is associated with negatively variable impacts on domains of health-related quality of life: evidence from a meta-analysis Yanan Li, M.M.,a Yan Li, M.D., Ph.D.,a Ernest Hung Yu Ng, M.D.,b Elisabet Stener-Victorin, Ph.D.,a,c Lihui Hou, M.D.,a Taixiang Wu, M.D., Ph.D.,d Fengjuan Han, M.D., Ph.D.,a and Xiaoke Wu, M.D., Ph.D.a a Department of Obstetrics and Gynecology, National Key Laboratory and Unit of Infertility, Clinical Trial Base, First Affiliated Hospital, Heilongjiang University of Chinese Medicine, Harbin, People’s Republic of China; b Department of Obstetrics and Gynecology, University of Hong Kong, Hong Kong, People’s Republic of China; c Institute of Neuroscience and Physiology, Department of Physiology, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden; and d Chinese Clinical Trial Registry, Chinese Evidence-Based Medicine Centre, Chinese Cochrane Centre, INCLEN CERTC, West China Hospital, Sichuan University, Chengdu, People’s Republic of China Objective: To systematically review the literature to identify the impact of polycystic ovary syndrome (PCOS) on specific health-related quality of life domains. Design: Meta-analysis. Setting: N/A. Patient(s): The outcomes of 423 patients and 285 controls from 5 articles that used the Short Form 36 (SF-36) questionnaire were used for meta-analysis. Intervention(s): N/A. Main Outcome Measure(s): The SF-36 dimensions including physical function, physical role function, body pain, general health, vitality, social function, emotional role function, and mental health were evaluated. Result(s): Compared with controls, women with PCOS had lower scores in all SF-36 dimensions: physical function (mean differences [MD], 5.46; 95% confidence intervals [CI], 8.52, 2.41), physical role function (MD, 5.76; 95% CI, 8.49, 3.03), body pain (MD, 4.55; 95% CI, 7.99, 1.11), general health (MD, 11.34; 95% CI, 19.53, 3.15), vitality (MD, 15.14; 95% CI, 17.43, 12.84), social function (MD, 15.95, 95% CI, 18.57, 13.33), emotional role function (MD, 23.86; 95% CI, 27.51, 20.21), and mental health (MD, 13.83; 95% CI, 16.13, 11.53). Conclusion(s): The meta-analysis showed that women with PCOS score lower in each dimension of the SF-36, mostly in the emotional role function. (Fertil Steril 2011;96:452–8. 2011 by American Society for Reproductive Medicine.) Key Words: Polycystic ovary syndrome, SF-36, quality of life, meta-analysis Polycystic ovary syndrome (PCOS) is a common endocrine disorder affecting 5% to 10% of women of reproductive age (1). Its etiology is unknown, and its presentation varies (2). According to the Rotterdam consensus (3), the diagnosis of PCOS requires at least 2 of the following 3 conditions: [1] oligoovulation or anovulation, [2] clinical and/or biochemical signs of hyperandrogenism, and [3] polycystic ovaries and the exclusion of other etiologies. PCOS is associated Received March 16, 2011; revised May 20, 2011; accepted May 23, 2011; published online June 24, 2011. Y.L. has nothing to disclose. Y.L. has nothing to disclose. E.H.Y.N. has nothing to disclose. E.S-V. has nothing to disclose. L.H. has nothing to disclose. T.W. has nothing to disclose. F.H. has nothing to disclose. X.W. has nothing to disclose. Supported by the National Clinical Trial Base of Chinese Medicine in Gynecology (http://www.satcm.gov.cn/zhuanti/lcyjjd/tzgg/20090519/ 130039.shtml), National Public Welfare Projects for Chinese Medicine (201107005; 200807021). Yanan Li and Yan Li contributed equally to this work. Reprint requests: Xiaoke Wu, M.D., Ph.D., or Fengjuan Han, M.D., Ph.D., Department of Obstetrics and Gynecology, National Key Laboratory and Unit of Infertility, Clinical Trial Base, First Affiliated Hospital, Heilongjiang University of Chinese Medicine, Harbin 150040, People’s Republic of China (E-mail: xiaokewu2002@vip.sina.com or hanfengjuan2004@163.com). 452 with several mental health problems, including depression and anxiety (4–10), suicide attempts (11, 12), body dissatisfaction (13), eating disorders (14–18), diminished sexual satisfaction (19–21), and lowered health-related quality of life (HRQoL) (22, 23). Because treatment for PCOS is symptom oriented, individualized management should be aimed at relieving symptoms and improving HRQoL. In its 1946 constitution, the World Health Organization defined health as ‘‘a state of complete physical, mental, and social wellbeing and not merely the absence of disease or infirmity’’ (WHO definition of Health, Preamble to the Constitution of the World Health Organization as adopted by the International Health Conference, 1946). This definition represented a departure from defining health solely in terms of death and disease. Later, HRQoL was defined as the ‘‘physical, psychologic and social domains of health, seen as distinct areas that are influenced by a person’s experiences, beliefs, expectations and perceptions’’ (24). HRQoL assessments have an important role in measuring chronic disease (25) and may assist in clinical decision making regarding choice of treatment and policy decisions. Furthermore, randomized controlled trials now often include HRQoL measures as valid and useful end points along with traditional clinical outcomes (26). Fertility and Sterility Vol. 96, No. 2, August 2011 Copyright ª2011 American Society for Reproductive Medicine, Published by Elsevier Inc. 0015-0282/$36.00 doi:10.1016/j.fertnstert.2011.05.072 PCOS is a metabolic, hormonal, and psychosocial disorder that adversely affects a patient’s quality of life (10, 27, 28). Jones et al. (29) performed a systematic review focusing specifically on HRQoL measurement in women with PCOS. However, the relative degree of impairment in each domain differed among samples, and it was not clear which aspect of HRQoL was most negatively affected. In this study, our goal was to systematically review the effects of PCOS on specific HRQoL domains compared with the results of healthy controls. MATERIALS AND METHODS Search Strategy To identify eligible studies, we searched the electronic databases MEDLINE, EMBASE, CINAHL, EMBR, CNKI, Wanfang, and Vip from inception through December 2009, using the terms (‘‘quality of life’’ [MeSH] OR ‘‘health-related quality of life’’ OR ‘‘health status measurement’’ OR ‘‘subjective health status’’ OR ‘‘quality of life questionnaire’’) AND (‘‘polycystic ovary syndrome’’ [MeSH] OR ‘‘polycystic ovarian syndrome’’ OR ‘‘polycystic ovaries’’). The search was restricted to literature in English and Chinese. We then perused the reference sections of all relevant studies or reviews, manually searched key journals and abstracts from major annual meetings in the field of endocrinology, and contacted experts on the subject in an effort to identify relevant unpublished data. The data search and screening of titles, abstracts, and full-text articles were completed independently by 2 reviewers (Yanan Li and Yan Li). Any discrepancy was solved by consultation with a third reviewer (Ng). Eligibility of Relevant Studies Studies that reported HRQoL in women with PCOS and healthy, agematched controls were considered suitable for this review. Studies were excluded if they appraised a single dimension because HRQoL is defined as a multidimensional concept that encompasses physical, emotional, and social aspects associated with a disease or its treatment. Studies that used ad hoc questionnaires/instruments were also excluded, as were reviews, letters to the editor, and studies using data from the same group. If the outcomes for which we were looking were not reported in the study, the study authors were contacted to ask for additional information; the trials were excluded if additional information was not available. Data Extraction Information from each study was extracted independently by 2 reviewers (Yanan Li and Yan Li), using a piloted data extraction form. General characteristics of the study (author, journal, year of publication, design, ethnicity, study size, and number of cases), characteristics of the PCOS and control groups (selection criteria, age, body mass index [BMI], androgen levels, Ferriman-Gallway score, and global acne score), methodology (HRQoL measurement method, study quality), and results (means SD) were recorded when available and double-checked. If necessary, the data set was completed through communication with the authors. Two reviewers (Yanan Li and Yan Li) assessed the quality of included studies using the Newcastle-Ottawa scale for assessing the quality of nonrandomized studies in meta-analysis (30). RESULTS Search Results The search strategy identified 746 studies (Fig. 1). A total of 703 publications were excluded because they were repetitions, appeared in more than 1 database, or were not relevant or specific to the study topic, as judged from the title, abstract, and full text. Eleven studies were excluded because they were reviews or letters to the editors or because the full text was not available. Of the remaining 32 studies, 16 had no healthy control group and were excluded (31–46). Eight studies were excluded because insufficient data were available; in 5 studies (22, 23, 47–49), the results were presented only as medians or in figures and no additional results were obtained after contact with the original authors. In one study (50), results were presented only in physical sum and psychologic sum but not in every dimension; in 2 studies (51, 52), in-depth semistructured interviews rather than self-report questionnaires were used. Two studies (53, 54) were excluded because the CHQ-CF87 scores coincided with those in a previous study by the same authors (55), suggesting sample duplication. Finally, 5 studies (19, 20, 28, 56, 57) using the same questionnaire, Short Form-36 (SF-36), were included in the metaanalysis. Description of Studies The characteristics of the included studies are briefly described in Table 1. One study reported that a significantly greater proportion of patients with PCOS currently had an unfulfilled wish to conceive a child (PCOS, 42%; controls, 6%) (19). Another study reported statistically significant differences related to the number of pregnancies, miscarriages, and infertility problems. With respect to pregnancies, a higher percentage of women who were pregnant and had delivered children was noted among healthy women (82.5%) in comparison with 24.0% of women with PCOS (P<.05). Six percent of women with PCOS had miscarriages in their medical history, and 50.0% of this group was diagnosed and treated for infertility, whereas no miscarriages or infertility problems were found in the control group (20). FIGURE 1 Flow chart for the systematic review. Statistical Analysis The scores on questionnaires used to evaluate HRQoL in women with PCOS and controls in each study were extracted as mean differences (MD) SD. MD and 95% confidence intervals (CI) were calculated for scores in all studies eligible for the meta-analysis and combined by using fixed- or random-effects model (DerSimonian–Laird random-effects method), when appropriate. Statistical heterogeneity in the results of different studies was examined by c2 tests for significance. P<.05 was considered statistically significant. Inconsistency across studies was quantified with the value of I2. A rough guide to interpretation of I2 is as follows: 0% to 40%, might not be important; 30% to 60%, may represent moderate heterogeneity; 50% to 90%, may represent substantial heterogeneity; and 75% to 100%, considerable heterogeneity. To assess the extent of publication bias, a funnel plot may be used. The meta-analysis was conducted with Review Manager (version 5.0.25). Fertility and Sterility Li. HRQoL in women with PCOS. Fertil Steril 2011. 453 454 Li et al. TABLE 1 HRQoL in women with PCOS Characteristics of studies included in the review. Elsenbruch et al., 2003 (19) Hahn et al., 2005 (28) Case-control study Germany Age-matched, healthy women 30.1 9.8/24.4 5.3 Case-control study Germany Age-matched, healthy women 31.0 9.3/24.0 5.3 Case-control study Poland Age-matched, healthy women 24.6 3.8/22.1 2.9 Case-control study China Age-matched, healthy women 24.57 3.91/21.08 2.15 Case-control study China Age-matched, healthy women N/A 12 5/3 2 2.7 0.9/1.1 0.6 2.7 1.2/1.3 0.6 1990 NIH 9.2 5.8/3.0 2.0 2.7 0.9/1.3 0.6 2.7 1.2/1.3 0.6 1990 NIH N/A N/A N/A 2003 Rotterdam N/A N/A N/A 2003 Rotterdam Questionnaires SF-36, SCL-90-R, FLZ SF-36, SCL-90-R, VASs 12.7 6.1/2.7 2.1 N/A N/A PSE and 2003 Rotterdam SF-36, ISS SF-36, SCL-90-R, LSIA, VASs SF-36, SAS, SDS SF-36 scores (PCOS/control) 1 Physical function 2 Physical role function 3 Body pain 4 General health 5 Vitality 6 Social function 7 Emotional role function 8 Mental health Total Design of study N/A 71 37/90 21 73 30/85 26 N/A 43 20/60 20 66 30/80 27 49 44/87 27 53 20/70 18 N/A Cross-sectional 81 21/88 20 76 32/90 21 74 28/85 26 62 20/62 18 43 20/60 20 67 24/80 27 62 40/87 27 57 20/70 19 N/A Cross-sectional 89.9 11.1/93.7 8.1 73.5 30.8/87.5 22.6 64.8 25.1/72.6 19.8 46.3 15.9/60.1 18.9 57.3 16.4/71.2 17.7 70.6 21.5/82.6 17.8 67.7 28.6/5.8 11.4 57.5 17.9/69.9 15.1 N/A Cross-sectional 82.41 11.41/90.90 5.41 N/A N/A 50.37 16.91/70.61 11.97 58.22 15.15/77.20 8.87 N/A N/A 60.51 14.70/77.76 10.48 N/A Cross-sectional 80 11/83 11 78 13/81 10 76 12/77 19 58 13/69 19 51 17/62 11 69 10/86 12 63 19/84 15 58 14/69 14 533 52/611 62 Cross-sectional Study type Location Control BMI (kg/m2) (PCOS/control) FG score Testosterone (nmol/L) LH/FSH ratio PCOS diagnostic criteria Drosdzol et al., 2007 (20) Wang et al., 2007 (56) Wang et al., 2009 (57) Vol. 96, No. 2, August 2011 Note: Values are presented as means SD, unless otherwise indicated. FG ¼ Ferriman-Gallwey; FLZ ¼ fragebogen zur lebenszufriedenheit; ISS ¼ index of sexual satisfaction; LSIA ¼ life satisfaction index A; N/A ¼ not available; NIH ¼ national institutes of health; PSE ¼ polish society of endocrinology; SAS ¼ self-rating anxiety scale; SCL-90-R ¼ symptom checklist 90; SDS ¼ self-rating depression scale; VASs ¼ visual analogue scales. Li. HRQoL in women with PCOS. Fertil Steril 2011. FIGURE 2 FIGURE 2 Continued Meta-analysis of studies on the HRQoL of women with PCOS. Forest plots for MDs of all dimensions of SF-36. (A) Pooled data on the physical function dimension showed lower values (P¼.0005) in women with PCOS than healthy controls, without significant among-study heterogeneity (P¼.05). (B) Pooled data on the physical role function dimension showed lower values (P<.0001) in women with PCOS than healthy controls, with significant among-study heterogeneity (P¼.003). (C) Pooled data on the body pain dimension showed lower values (P¼.01) in women with PCOS than healthy controls, without significant among-study heterogeneity (P¼.08). (D) Pooled data on the general health dimension showed lower values (P¼.007) in women with PCOS than healthy controls, but there was significant among-study heterogeneity (P<.00001). (E) Pooled data on the vitality dimension showed lower values (P<.00001) in women with PCOS than healthy controls, without significant among-study heterogeneity (P¼.07). (F) Pooled data on the social function dimension showed lower values (P<.00001) in women with PCOS than healthy controls, without significant among-study heterogeneity (P¼.59). (G) Pooled data on the emotional role function dimension showed lower values (P<.00001) in women with PCOS than healthy controls, without significant among-study heterogeneity (P¼.1). (H) Pooled data on the mental health dimension showed lower values (P<.00001) in women with PCOS than healthy controls, without significant among-study heterogeneity (P¼.23). studies, potential publication bias was not assessed using a funnel plot or other corrective analytical methods (58). Overall there was a mean Newcastle-Ottawa scale score of 5.6 out of 9 (range, 5–6). Meta-Analysis A meta-analysis of 5 studies (19, 20, 28, 56, 57) that used SF-36 was performed. Unfortunately, we could not obtain scores from all dimensions. Included studies reported data on 708 women (423 with PCOS and 285 healthy controls), and the number of subjects included in these studies ranged from 90 to 211. In only 1 of the 5 studies was the total score of SF-36 given (7). Therefore, data from each dimension of SF-36 were calculated in the meta-analysis (Table 1). Dimensions Analysis Physical function Four studies (20, 28, 56, 57) compared scores on the physical function dimension in women with PCOS and controls. Women with PCOS had significantly lower values (MD, 5.46; 95% CI, 8.52, 2.41; P¼.0005), without heterogeneity among studies (P¼.05) (Fig. 2A). Li. HRQoL in women with PCOS. Fertil Steril 2011. Risk of Bias in Included Studies No study reported incomplete outcome data; therefore, there is high risk of selective reporting bias. One study (19) reported that the proportional difference between women with PCOS and controls of an unfulfilled wish to conceive a child was likely to be related to a selective bias. The protocols of included studies were unavailable, and detailed information could not be obtained from primary authors. The outcomes of these 5 included studies might have been influenced by selective reporting bias. Because there were fewer than 10 included Fertility and Sterility Physical role function Four studies (19, 20, 28, 57) compared scores on the physical role function dimension in women with PCOS and controls. Women with PCOS had significantly lower values (MD, 5.76; 95% CI, 8.49, 3.03; P<.0001), with heterogeneity among studies (P¼.003) and I2 ¼ 78% (Fig. 2B). Body pain Four studies (19, 20, 28, 57) compared scores on the body pain dimension in women with PCOS and controls. Women with PCOS had significantly lower values (MD, 4.55; 95% CI, 7.99, 1.11; P¼.01), without heterogeneity among studies (P¼.08) (Fig. 2C). General health Four studies (20, 28, 56, 57) compared scores on the general health dimension in women with PCOS and controls. 455 Women with PCOS had significantly lower values (MD, 11.34; 95% CI, 19.53, 3.15; P¼.007), but there was significant among-study heterogeneity (P<.00001) and I2 ¼ 89% (Fig. 2D). Vitality Five studies (19, 20, 28, 56, 57) compared scores on the vitality dimension in women with PCOS and controls. Women with PCOS had significantly lower values (MD, 15.14; 95% CI, 17.43, 12.84; P<.00001), with heterogeneity among studies (P¼.07) (Fig. 2E). Social function Four studies (19, 20, 28, 57) compared scores on the social function dimension in women with PCOS and controls. Women with PCOS had significantly lower values (MD, 15.95; 95% CI, 18.57, 13.33; P<.00001), and there was no significant heterogeneity among studies (P¼.59) (Fig. 2F). Emotional role function Four studies (19, 20, 28, 57) compared scores on the emotional role function dimension in women with PCOS and controls. Women with PCOS had significantly lower values (MD, 23.86; 95% CI, 27.51, 20.21; P<.00001), without heterogeneity among studies (P¼.1) (Fig. 2G). Mental health Five studies (19, 20, 28, 56, 57) compared scores on the mental health function dimension in women with PCOS and controls. Women with PCOS had significantly lower values (MD, 13.83; 95% CI, 16.13, 11.53; P<.00001), without amongstudy heterogeneity (P¼.23) (Fig. 2H). DISCUSSION The present systematic review has demonstrated that women with PCOS have lower HRQoL than women without the disorder. The meta-analysis was conducted to show for the first time that women with PCOS scored lower in each dimensions of SF-36, particularly in the emotional role function. The meta-analysis included only studies with age-matched controls because our objective was to compare patients with PCOS with age-matched women. Studies that used population normative data (23, 48, 49), patients with other diseases (32, 47), or different ethnic populations (33, 35) as controls were excluded from this meta-analysis, as were studies without controls (34). The high statistical heterogeneity of the physical role function (I2 ¼ 78%) and general health (I2 ¼ 89%) dimensions may represent substantial or considerable heterogeneity in the included studies, which might decrease the generalizability of the results regarding HRQoL for women with PCOS. These dimension outcomes should be explored in future studies. PCOS is a heterogeneous disorder, and its main symptoms are infertility, menstrual dysfunction, hirsutism, and obesity—all of which may cause physical dysfunction and psychosocial stress. BMI would be a significant confounder in the majority of the studies given the BMI differences between patients and controls. However, it has been reported that not only overall anxiety symptom burden but also several individual anxiety symptoms distinguished women with PCOS from a control group matched for age, body weight, and BMI (59). In the study by Coffey et al. (47), the psychologic dimension was more affected than the physical dimension as measured with SF-36. Jones 456 Li et al. HRQoL in women with PCOS et al. (34) found that the ‘‘role limitation-emotional’’ was the poorest area of health, with mean scores of 50.4 on the SF-36 questionnaire, which had the greatest negative impact on HRQoL in women with PCOS. Our systematic review confirmed these conclusions and extended our evidence based on the meta-analysis. In previous studies, PCOS was associated with decreased QoL and self-rated mental symptoms (19, 28). In one study (11), PCOS was also linked to psychiatric syndromes as verified by structured clinical assessments. Thus, clinicians should be aware that women with PCOS are at high risk for common affective and anxiety disorders, as well as suicide attempts. Elsenbruch et al. (60) found an interesting phenomenon—that having a partner who supports the wish for a child constitutes a protective factor and improves the emotional well-being of patients. So they argued that it is important to address not only the risk factors (e.g., obesity and hirsutism) but also protective factors, such as effective coping strategies (e.g., the ability to have a healthy relationship despite the clinical symptoms of PCOS). Generic instruments are designed to gauge HRQoL over a broad spectrum of diseases and thus may not be sensitive enough to measure HRQoL in specific illnesses (61). For example, in the study of Coffey et al. (47), controlling for BMI abolished differences in all domains of SF-36, which may suggest that women of normal weight with PCOS have normal HRQoL. However, the differences measured by an HRQoL questionnaire for women with PCOS (PCOSQ) remained even after adjustment for BMI. Actually, even normal-weight women with PCOS felt that they had problems with their weight. Disease-specific instruments could more directly address the specific problems of women with PCOS (e.g., weight, body hair, infertility) who are significantly affected on the PCOSQ, which would not be identified by a generic questionnaire (i.e., SF-36) because there are no items pertaining to these dimensions. On the contrary, the findings cannot be compared with those of samples affected by other diseases and their healthy controls, which precludes an assessment of the relative impact of the specific problems. The only PCOSspecific instrument currently available to measure HRQoL, PCOSQ, appears to be reliable and valid. The sensitivity of the instrument has not been confirmed, and more work is needed to confirm this property of the questionnaire in different countries and ethnicities. Moreira et al. (62) thought that previous research on PCOS conducted within a medical or psychiatric framework had failed to explore women’s own experience, such as impaired female identity (51), and believed that a nonspecific instrument could not correctly evaluate the psychologic impact of the disease. They suggested that qualitative approaches be incorporated to gain an adequate understanding of the psychosocial impact of PCOS. Studies combining quantitative and qualitative methods may reveal complementary results. In conclusion, this review demonstrated that PCOS has a significant negative impact on HRQoL, especially on the emotional role function domain. Considering the insufficient evidence, this conclusion should be interpreted with caution. PCOS affects women both psychologically and physically according to the SF-36. Welldesigned and well-conducted studies with expanded sample sizes on the HRQoL of women with PCOS should be conducted in different countries and ethnicities. Vol. 96, No. 2, August 2011 REFERENCES 1. Norman RJ, Dewailly D, Legro RS, Hickey TE. Polycystic ovary syndrome. Lancet 2007;370:685–97. 2. Azziz R, Carmina E, Dewailly D, DiamantiKandarakis E, Escobar-Morreale HF, Futterweit W, et al. Task Force on the Phenotype of the Polycystic Ovary Syndrome of the Androgen Excess and PCOS Society. The Androgen Excess and PCOS Society criteria for the polycystic ovary syndrome: the complete task force report. Fertil Steril 2009;91:456–88. 3. Rotterdam ESHRE/ASRM–Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum Reprod 2004;19:41–7. 4. Bruce-Jones W, Zolese G, White P. Polycystic ovary syndrome and psychiatric morbidity. Psychosom Obstet Gynaecol 1993;14:111–6. 5. Rasgon NL, Rao RC, Hwang S, Altshuler LL, Elman S, Zuckerbrow-Miller J, et al. Depression in women with polycystic ovary syndrome: clinical and biochemical correlates. J Affect Disord 2003;74:299–304. 6. Gorwood P. Generalized anxiety disorder and major depressive disorder comorbidity: an example of genetic pleiotropy? Eur Psychiatry 2004;19:27–33. 7. Weiner CL, Primeau M, Ehrmann DA. Androgens and mood dysfunction in women: comparison of women with polycystic ovarian syndrome to healthy controls. Psychosom Med 2004;66:356–62. 8. Hollinrake E, Abreu A, Maifeld M, Van Voorhis BJ, Dokras A. Increased risk of depressive disorders in women with polycystic ovary syndrome. Fertil Steril 2007;87:1369–76. 9. Bishop SC, Basch S, Futterweit W. Polycystic ovary syndrome, depression, and affective disorders. Endocr Pract 2009;15:475–82. 10. Jedel E, Waern M, Gustafson D, Landen M, Eriksson E, Holm G, et al. Anxiety and depression symptoms in women with polycystic ovary syndrome compared with controls matched for body mass index. Hum Reprod 2010;25:450–6. 11. M ansson M, Holte J, Landin-Wilhelmsen K, Dahlgren E, Johansson A, Landen M. Women with polycystic ovary syndrome are often depressed or anxious—a case control study. Psychoneuroendocrinology 2008;33:1132–8. 12. Kerchner A, Lester W, Stuart SP, Dokras A. Risk of depression and other mental health disorders in women with polycystic ovary syndrome: a longitudinal study. Fertil Steril 2009;91:207–12. 13. Himelein MJ, Thatcher SS. Depression and body image among women with polycystic ovary syndrome. J Health Psychol 2006;11:613–25. 14. McCluskey SE, Lacey JH, Pearce JM. Binge-eating and polycystic ovaries. Lancet 1992;340:723. 15. Jahanfar S, Eden JA, Nguyent TV. Bulimia nervosa and polycystic ovary syndrome. Gynecol Endocrinol 1995;9:113–7. 16. Michelmore KF, Balen AH, Dunger DB. Polycystic ovaries and eating disorders: are they related? Hum Reprod 2001;16:765–9. 17. Jahanfar S, Maleki H, Mosavi AR. Subclinical eating disorder, polycystic ovary syndrome—is there any connection between these two conditions through leptin—a twin study. Med J Malaysia 2005;60:441–6. 18. Naessen S, Carlstrom K, Garoff L, Glant R, Hirschberg AL. Polycystic ovary syndrome in bulimic women—an evaluation based on the new diagnostic criteria. Gynecol Endocrinol 2006;22:388–94. 19. Elsenbruch S, Hahn S, Kowalsky D, Offner AH, Schedlowski M, Mann K, et al. Quality of life, psychosocial well-being, and sexual satisfaction in women with polycystic ovary syndrome. J Clin Endocrinol Metab 2003;88:5801–7. Fertility and Sterility 20. Drosdzol A, Skrzypulec V, Mazur B, PawlinskaChmara R. Quality of life and marital sexual satisfaction in women with polycystic ovary syndrome. Folia Histochem Cytobiol 2007;45(Suppl 1):S93–7. 21. Janssen OE, Hahn S, Tan S, Benson S, Elsenbruch S. Mood and sexual function in polycystic ovary syndrome. Semin Reprod Med 2008;26:45–52. 22. Barnard L, Ferriday D, Guenther N, Strauss B, Balen AH, Dye L. Quality of life and psychological well being in polycystic ovary syndrome. Hum Reprod 2007;22:2279–86. 23. Ching HL, Burke V, Stuckey BG. Quality of life and psychological morbidity in women with polycystic ovary syndrome: body mass index, age and the provision of patient information are significant modifiers. Clin Endocrinol (Oxf) 2007;66:373–9. 24. Testa MA, Simonson DC. Assessment of quality-oflife outcomes. New Engl J Med 1996;28:835–40. 25. Guyatt G, Feeny DH, Patrick DL. Measuring health-related quality of life. Ann Intern Med 1993;118:622–9. 26. Crosby RD, Kolotkin RL, Williams GR. Defining clinically meaningful change in health-related quality of life. J Clin Epidemiol 2003;56:395–407. 27. Apridonidze T, Essah PA, Iuorno MJ, Nestler JE. Prevalence and characteristics of the metabolic syndrome in women with polycystic ovary syndrome. J Clin Endocrinol Metab 2005;90:1929–35. 28. Hahn S, Janssen OE, Tan S, Pleger K, Mann K, Schedlowski M, et al. Clinical and psychological correlates of quality of life in polycystic ovary syndrome. Eur J Endocrinol 2005;153:853–60. 29. Jones GL, Hall JM, Balen AH, Ledger WL. Healthrelated quality of life measurement in women with polycystic ovary syndrome: a systematic review. Hum Reprod Update 2008;14:15–25. 30. Ottawa Hospital Research Institute. The NewcastleOttawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Available at: http://www.ohri.ca/programs/clinical_epidemiology/ oxford.htm. Accessed February 15, 2011. 31. Cronin L, Guyatt G, Griffith L, Wong E, Azziz R, Futterweit W, et al. Development of a health-related quality of life questionnaire (PCOSQ) for women with polycystic ovary syndrome (PCOS). J Clin Endocrinol Metab 1998;83:1976–87. 32. Wong E, Cronin L, Griffith L, Irvine EJ, Guyatt GH. Problems of HRQL assessment: how much is too much? J Clin Epidemiol 2001;54:1081–5. 33. Hashimoto DM, Schmid J, Martins FM, Fonseca AM, Andrade LH, Kirchengast S, et al. The impact of the weight status on subjective symptomatology of the polycystic ovary syndrome: a cross-cultural comparison between Brazilian and Austrian women. Anthropologischer Anzeiger 2003;61:297–310. 34. Jones GL, Benes K, Clark TL, Denham R, Holder MG, Haynes TJ, et al. The Polycystic Ovary Syndrome Health-Related Quality of Life Questionnaire (PCOSQ): a validation. Hum Reprod 2004;19:371–7. 35. Schmid J, Kirchengast S, Vytiska-Binstorfer E, Huber J. Infertility caused by PCOS, health-related quality of life among Austrian and Moslem immigrant women in Austria. Hum Reprod 2004;19:2251–7. 36. Guyatt G, Weaver B, Cronin L, Dooley JA, Azziz R. Health-related quality of life in women with polycystic ovary syndrome, a self-administered questionnaire, was validated. J Clin Epidemiol 2004;57: 1279–87. 37. McCook JG, Reame NE, Thatcher SS. Health-related quality of life issues in women with polycystic ovary syndrome. J Obstet Gynecol Neonatal Nurs 2005;34: 12–20. 38. Lipton MG, Sherr L, Elford J, Rustin MH, Clayton WJ. Women living with facial hair: the psychological and behavioral burden. J Psychosom Res 2006;61:161–8. 39. Jedel E, Kowalski J, Stener-Victorin E. Assessment of health-related quality of life: Swedish version of polycystic ovary syndrome questionnaire. Acta Obstet Gynecol Scand 2008;87:1329–35. 40. Benson S, Hahn S, Tan S, Mann K, Janssen OE, Schedlowski M, et al. Prevalence and implications of anxiety in polycystic ovary syndrome: results of an Internet-based survey in Germany. Hum Reprod 2009;24:1446–51. 41. Wang RX. Elementary survey and analysis of TCM syndromes and quality of life in patients with polycystic ovary syndrome (D) [in Chinese]. Guangzhou, People’s Republic of China: Sun Yat-sen University; 2006. 42. van Wely M, Bayram N, Bossuyt PM, van der Veen F. Laparoscopic electrocautery of the ovaries versus recombinant FSH in clomiphene citrate-resistant polycystic ovary syndrome. Impact on women’s health-related quality of life. Hum Reprod 2004;19: 2244–50. 43. Clayton WJ, Lipton M, Elford J, Rustin M, Sherr L. A randomized controlled trial of laser treatment among hirsute women with polycystic ovary syndrome. Br J Dermatol 2005;152:986–92. 44. Hahn S, Benson S, Elsenbruch S, Pleger K, Tan S, Mann K, et al. Metformin treatment of polycystic ovary syndrome improves health-related quality of life, emotional distress and sexuality. Hum Reprod 2006;21:1925–34. 45. Harris-Glocker M, Davidson K, Kochman L, Guzick D, Hoeger K. Improvement in quality of life questionnaire measures in obese adolescent females with polycystic ovary syndrome treated with lifestyle changes and oral contraceptives, with or without metformin. Fertil Steril 2009;93:1016–9. 46. Thomson RL, Buckley JD, Lim SS, Noakes M, Clifton PM, Norman RJ, et al. Lifestyle management improves quality of life and depression in overweight and obese women with polycystic ovary syndrome. Fertil Steril 2010;94:1812–6. 47. Coffey S, Bano G, Mason HD. Health-related quality of life in women with polycystic ovary syndrome: a comparison with the general population using the Polycystic Ovary Syndrome Questionnaire (PCOSQ) and the Short Form-36 (SF-36). Gynecol Endocrinol 2006;22:80–6. 48. Elsenbruch S, Benson S, Hahn S, Tan S, Mann K, Pleger K, et al. Determinants of emotional distress in women with polycystic ovary syndrome. Hum Reprod 2006;21:1092–9. 49. Tan S, Hahn S, Benson S, Janssen OE, Dietz T, Kimmig R, et al. Psychological implications of infertility in women with polycystic ovary syndrome. Hum Reprod 2008;23:2064–71. 50. Benson S, Janssen OE, Hahn S, Tan S, Dietz T, Mann K, et al. Obesity, depression, and chronic low-grade inflammation in women with polycystic ovary syndrome. Brain Behav Immun 2008;22: 177–84. 51. Kitzinger C, Willmott J. ‘‘The thief of womanhood’’: women’s experience of polycystic ovarian syndrome. Soc Sci Med 2002;54:361. 52. Snyder BS. The lived experience of women diagnosed with polycystic ovary syndrome. J Obstet Gynecol Neonatal Nurs 2006;35:385–92. 53. Trent ME, Rich M, Austin SB, Gordon CM. Fertility concerns and sexual behavior in adolescent girls with polycystic ovary syndrome: implications for quality of life. J Pediatr Adolesc Gynecol 2003;16:33–7. 457 54. Trent M, Austin SB, Rich M, Gordon CM. Overweight status of adolescent girls with polycystic ovary syndrome: body mass index as mediator of quality of life. Ambul Pediatr 2005;5:107–11. 55. Trent ME, Rich M, Austin SB, Gordon CM. Quality of life in adolescent girls with polycystic ovary syndrome. Arch Pediatr Adolesc Med 2002;156: 556–60. 56. Wang JN, Ruan XY. Health-related quality of life issues in women with polycystic ovary syndrome [in Chinese]. J Practical Obstet Gynecol 2007;23: 610–3. 458 Li et al. 57. Wang YQ, Yang J, Xu WM, Yin TL, Li AB, Hu J. Quality of life in patients with polycystic ovary syndrome [in Chinese]. Chinese J Gen Practitioners 2009;8:127–9. 58. Egger M, Smith GD, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997;315:629–34. 59. Jedel E, Waern M, Gustafson D, Landen M, Eriksson E, Holm G, et al. Anxiety and depression symptoms in women with polycystic ovary syndrome compared with controls matched for body mass index. Hum Reprod 2010;25:450–6. HRQoL in women with PCOS 60. Elsenbruch S, Benson S, Hahn S. Reply: incorporating qualitative approaches is the path to adequate understanding of the psychosocial impact of polycystic ovary syndrome. Hum Reprod 2006;21:2724–5. 61. Jenkinson C. Assessment and evaluation of health and medical care: a methods text. Buckingham, United Kingdom: Open University Press; 1997. 62. Moreira SN, Azevedo GD. Incorporating qualitative approaches is the path to adequate understanding of the psychosocial impact of polycystic ovary syndrome. Hum Reprod 2006;21:2723–4. Vol. 96, No. 2, August 2011