Platelet aggregation in patients with atrial fibrillation taking aspirin or warfarin.
C M Helgason, J A Hoff, G T Kondos and L D Brace
Stroke. 1993;24:1458-1461
doi: 10.1161/01.STR.24.10.1458
Stroke is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1993 American Heart Association, Inc. All rights reserved.
Print ISSN: 0039-2499. Online ISSN: 1524-4628
The online version of this article, along with updated information and services, is located on the
World Wide Web at:
http://stroke.ahajournals.org/content/24/10/1458
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published
in Stroke can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.
Once the online version of the published article for which permission is being requested is located, click
Request Permissions in the middle column of the Web page under Services. Further information about this
process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Stroke is online at:
http://stroke.ahajournals.org//subscriptions/
Downloaded from http://stroke.ahajournals.org/ by guest on March 4, 2014
1458
Platelet Aggregation in Patients With Atrial
Fibrillation Taking Aspirin or Warfarin
Cathy M. Helgason, MD; Julie A. Hoff, RN, MPH;
George T. Kondos, MD; Larry D. Brace, PhD
Background and Purpose: Although warfarin and perhaps aspirin may be effective in preventing
thromboembolism in patients with nonvalvular atrial fibrillation, some patients develop cerebral
infarction despite these therapies. The purpose of this study was to determine inhibition of platelet
aggregation in patients on aspirin and platelet reactivity in those on warfarin in the Stroke Prevention in
Atrial Fibrillation study.
Methods: Twenty-four patients in the Stroke Prevention in Atrial Fibrillation study at the University of
Illinois at Chicago, 17 on enteric-coated aspirin 325 mg/d and 7 on warfarin to produce an International
Normalized Ratio of 2.0 to 4.5, had platelet aggregation studies performed during a 10-month period and
interpreted by an investigator blinded to therapy. Epinephrine, adenosine diphosphate, collagen, and
arachidonic acid were used as aggregating agents. Compliance was determined by pill count for those
patients on aspirin.
Results: Seven patients taking aspirin had partial and 10 had complete inhibition of platelet aggregation.
Three of seven patients on warfarin had hyperaggregable platelets. Compliance was 80% or greater for those
patients taking aspirin. One patient on warfarin had partial inhibition of platelet aggregation.
Conclusions: Some patients in the Stroke Prevention in Atrial Fibrillation trial on aspirin 325 mg/d did
not achieve complete inhibition of platelet aggregation. Others had hyperaggregable platelets. These
findings suggest platelet-dependent mechanisms for aspirin and warfarin failure to prevent stroke in these
patients. (Stroke. 1993;24:1458-1461.)
KEY WORDs * aspirin * atrial fibrillation * platelet aggregation * stroke prevention * warfarin
arfarin has been shown to produce a relative
risk reduction for brain and systemic embolism in patients with nonvalvular atrial fibrillation (NVAF) in five clinical studies.1-5 Through its
inhibitory action on the production of functional clotting factors, warfarin is thought to prevent red clot
formation in chambers where there is stasis, the presumed mechanism for thrombus formation in the heart
in atrial fibrillation.6 Warfarin is not expected to inhibit
platelet aggregation, however, and a thrombus itself is a
stimulus for platelet adhesion and aggregation and
additional thrombus growth. In addition, abnormal endocardial tissue surfaces and carotid stenosis may be
found in patients with NVAF, suggesting platelet-dependent mechanisms for thrombus formation in this
situation.78 Nonetheless, the value of warfarin anticoagulation for the prevention of stroke in patients with
NVAF seems well established.
The efficacy of aspirin in the setting of NVAF, however,
is less clear. Although aspirin therapy did significantly
W
Received April 15, 1993; final revision received May 20, 1993;
accepted May 21, 1993.
From the Departments of Neurology (C.M.H., J.A.H.), Medicine (Section of Cardiology) (G.T.K.), and Pathology (L.D.B.),
University of Illinois at Chicago College of Medicine.
Reprint requests to Dr Cathy M. Helgason, University of Illinois
at Chicago College of Medicine, Department of Neurology (m/c
796), 912 S Wood St, Chicago, IL 60612.
reduce stroke incidence in the Stroke Prevention in Atrial
Fibrillation (SPAF) study, other studies have not shown a
similarly beneficial effect; however, given the different
doses of aspirin used in the studies, their results are
difficult to compare.1-3 Recent studies suggest that different doses of aspirin may be needed to inhibit platelet
aggregation and that a given dose of aspirin may not
achieve the same effect in all patients.9'10
Although the mechanisms that underlie the failure of
aspirin or warfarin therapy to prevent stroke in NVAF
patients are not fully understood, aspirin failure in some
patients may be related to inadequate dose to achieve
complete antiplatelet effect as well as to the lack of
inhibition of the clotting mechanism, while failure in
warfarin-treated patients may be related to lack of
inhibition of platelet function, particularly when the
patient has hyperaggregable platelets. To begin addressing these issues, the present study attempted to
determine whether aspirin at the dosage given in the
SPAF study (325 mg/d) could completely inhibit platelet aggregation and to determine the state of platelet
reactivity in patients taking warfarin.
Subjects and Methods
Twenty-four patients in the SPAF study at the University of Illinois at Chicago had platelet aggregation
studies performed during a 10-month period. All platelet aggregation studies were interpreted by the same
Downloaded from http://stroke.ahajournals.org/ by guest on March 4, 2014
1459
Helgason et al Platelet Aggregation in Atrial Fibrillation
% AGGREGATION
% AGGREGATION
100
ion ,
80
ADPP
EPI
60
40
3
4
5
6
TIME IN MINUTES
7
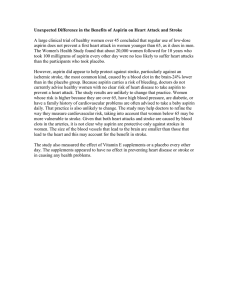
FIG 1. Tracings of normal or hyperaggregable responses to
platelet-aggregating agents. Responses shown are typical for
500 gumol/L arachidonic acid (AA) (free acid), 5 ,imol/L
adenosine diphosphate (ADP), 5 ,umol/L epinephrine (EPI),
and 0.8 1ig/mL collagen (COL). Responses of hyperaggregable platelets look essentially the same but at lower concentrations of agonists.
investigator (L.D.B.), who was blinded to medication.
Seventeen patients were taking 325 mg/d of aspirin, and
the other 7 patients were taking warfarin to achieve an
International Normalized Ratio (INR) of 2.0 to 4.5.
Institutional Review Board permission was obtained
(No. 91-631).
Preparation of platelet-rich plasma (PRP) was performed in the following manner. Blood was drawn using
19- to 21-gauge butterfly needles, plastic syringes, and
multiple syringe technique. Blood was immediately
placed in plastic tubes containing citrate anticoagulant
(9 parts blood to 1 part anticoagulant) and mixed. PRP
and platelet-poor plasma (PPP) were prepared by standard centrifugation techniques at room temperature
and kept sealed in plastic tubes until tested. A platelet
count on the PRP was performed on an Abbott/Unipath
CellDyne 3000SL (Abbott Park, Ill), and if the count
exceeded 400 000/,L, it was adjusted to approximately
350 000/I,u with autologous PPP.
Platelet aggregation studies were performed using a
model PAP4 aggregometer (BioData Corp, Hatboro,
Pa) as previously described.9 Briefly, PRP was placed in
each of four siliconized cuvettes and incubated for 1
minute at 37°C. An aggregating agent was then added to
each tube, and aggregation was recorded for 10 minutes
at 37°C with constant stirring at 1000 rpm. When saline
was added to test for spontaneous aggregation, the
recording time was extended to 20 minutes. If full
(normal) aggregation responses were obtained with the
initial concentrations of agents used (arachidonic acid
[AA], 500 ,umol/L; adenosine diphosphate [ADP], 5.0
,mol/L; epinephrine, 5.0 ,umol/L; and collagen, 0.8
,ug/mL), the aggregating agent was progressively titrated to the lowest concentration that produced a full
response. If less than full responses were obtained with
the initial concentrations, the concentration of each
agent was doubled to determine whether full responses
could be obtained. In interpreting aggregation responses and patterns, platelets were considered to show
increased sensitivity to an agent when a full aggregation
response was obtained with .100 ,umol/L AA, .1
,umol/L ADP, <0.4 ,ug/mL collagen, or <0.5 ,umol/L
0
AA
4
OL
20
T
0
1
2
3
4
5
6
TIME IN MINUTES
7
8
9
10
FIG 2. Tracings show partial inhibition as a result of aspirin
ingestion. ADP indicates 5 ,umol/L adenosine diphosphate;
EPI, S gsmol/L epinephrine; COL, 0.8 ,g/mL collagen; and
AA, 500 gtmolIL arachidonic acid. Note slow but steady rise
in epinephrine-induced aggregation.
epinephrine. Platelets were considered to be hyperaggregable if increased sensitivity to more than one agent
and/or the presence of spontaneous aggregation was
detected (Fig 1). For patients taking aspirin, platelets
showed partial inhibition when there was a full AA
response, and/or the ADP response was normal, and/or
epinephrine caused more than primary aggregation,
and/or the collagen response was normal, slightly decreased, or decreased (Fig 2). Platelets were considered
to show complete inhibition if there was no AA response, the ADP response was less than normal, epinephrine and collagen responses were absent or markedly decreased, and spontaneous aggregation was not
detected (Fig 3).
Blood for prothrombin time/INR testing was collected by venipuncture into citrate anticoagulant, centrifuged to prepare PPP, and tested with a commercial
thromboplastin reagent (International Sensitivity Index,
2.0) on an Ortho Koagulab 16S (Raritan, NJ) automated coagulation analyzer set to automatically calculate the INR. Results are reported as prothrombin
time/control ratio as required by SPAF protocol.
For those patients on aspirin, compliance was determined by pill counts at the follow-up closest to the date
of the platelet aggregation studies. For those patients on
warfarin, the prothrombin time ratio (required by
% AGGREGATION
100
80
60
40
20
0
1
2
3
4
5
6
7
8
9
10
TIME IN MINUTES
FIG 3. Tracings show complete inhibition as a result of
aspirin ingestion. ADP indicates 5 ,umol/L adenosine diphosphate; EPI, 5 ,mol/L epinephrine; COL, 0.8 pg/mL collagen;
and AA, 500 ,umol/L arachidonic acid.
Downloaded from http://stroke.ahajournals.org/ by guest on March 4, 2014
1460
Stroke Vol 24, No 10 October 1993
SPAF) represents that obtained at follow-up closest to
the platelet aggregation study.
Results
In aspirin-treated patients, 7 of 17 patients had
partial inhibition (Fig 2), and 10 patients had complete
inhibition of platelet aggregation (Fig 3). Compliance
ranged from 80% to 1 % in these patients but was not
always correlated with the degree of platelet aggregation inhibition. Three of 8 patients with less than 100%
compliance had complete inhibition; 2 of 7 patients with
greater than 100% compliance had partial inhibition of
platelet aggregation.
Three of 7 patients taking warfarin had hyperaggregable platelets (Fig 1); 3 had normal platelet reactivity,
and 1 had partial inhibition of platelet aggregation.
Despite warnings to refrain from taking platelet-inhibiting agents while taking warfarin, we assume that the
partial inhibition of platelet aggregation observed in 1
warfarin-treated patient resulted from inadvertent consumption of a compound containing aspirin or an
aspirin-like agent.
Discussion
The Copenhagen AFASAK and the SPAF studies
disagreed in their findings regarding the efficacy of
aspirin compared with placebo for the prevention of
stroke in patients with NVAF. 1,2 The latter study
showed a superiority of aspirin in this regard, with
nearly a 50% risk reduction in favor of aspirin. A
potential reason for the difference in aspirin efficacy is
that a different dosage of aspirin was used in the
Copenhagen AFASAK study (75 mg/d versus 325 mg/d
in the SPAF study). Neither study dosed aspirin with
regard to biologic efficacy, ie, inhibition of platelet
aggregation. Recent reports suggest that the ability of
aspirin to affect platelet aggregation may depend on the
dosage used as well as on the individual.9,10 The results
of the present study suggest that some patients in the
SPAF study who took 325 mg/d of aspirin did not
achieve complete inhibition of platelet aggregation as
measured by the methods described in the present
study. Whether the failure to achieve inhibition of
platelet aggregation in these individuals is clinically
significant for prevention of stroke is unknown at this
time. Likewise, it is unknown whether those AFASAK
study patients taking 75 mg/d failed to achieve inhibition of platelet aggregation.
The antithrombotic mechanisms of aspirin and warfarin are considered to be different. Whereas warfarin is
considered to inhibit red clot (red blood cell fibrin-rich)
formation in areas of stagnant flow in the atria or
ventricle of the heart in a patient with NVAF, aspirin
may be effective against white clot (platelet fibrin-rich)
formation where there is concomitant atherosclerotic
vascular disease of the carotid artery, mitral annulus
calcification, or other endocardial damage.7,8 Platelet
scintigraphy studies show active deposition of platelets
on intracardiac thrombus.'1 Although in one study warfarin was shown to inhibit this process, it is not expected
to affect platelet aggregation per se, and the effect of
aspirin on this process has not been shown.'1 Hyperaggregable platelets were discovered in three of seven
patients taking warfarin in the present study. While other
studies have described alteration in hemostatic function
and some platelet functions in patients with NVAF, we
are unaware of any study that has shown platelet hyperaggregability to be present in these patients.12 Hyperaggregability of platelets may be indicative of a prothrombotic state that would not be expected to be relieved by
or sensitive to warfarin therapy.13 In other studies, aspirin has been shown to decrease platelet hyperaggregability described in patients with other risk factors for
stroke.14-16 Whether those patients with atrial fibrillation
on warfarin but with hyperaggregable platelets would
require concomitant antiplatelet therapy for prevention
of thromboembolism is unknown at this time. Likewise, it
is unknown whether any of the patients assigned to
aspirin therapy had hyperaggregable platelets before
aspirin ingestion or whether the presence of such platelet
hyperaggregability relates to the incomplete inhibition of
platelet aggregation demonstrated in seven of the 17
patients in this study.
In summary, at our center, aspirin at the dosage used
in the SPAF study (325 mg/d) did not completely inhibit
platelet aggregation in all patients. This finding is
similar to that found in another study in which dose
escalation was needed (sometimes up to 1300 mg) to
achieve inhibition of platelet aggregation.9 In addition,
increased platelet reactivity (platelet hyperaggregability) may be present in some patients with chronic
NVAF, and this aspirin-sensitive mechanism for platelet-dependent thrombus formation would not be affected by warfarin. We hypothesize that the presence of
hyperaggregable platelets in warfarin-treated patients
and lack of complete inhibition of platelet aggregation
in aspirin-treated patients may be related to medication
failure in these patients.
Acknowledgments
This study was supported in part by funds from grant
R01NS2537412 from the National Institute of Neurological
Disorders and Stroke, Bethesda, Md. The authors gratefully
acknowledge the excellent technical expertise of JoAnne
Walker and Dianne Gibraski in performing platelet aggregation testing on the study patients. We would also like to thank
Jeanne Ward for her skills in preparing this manuscript.
References
1. Petersen P, Boysen G, Godtfredsen J, Andersen ED, Andersen B.
Placebo controlled randomized trial of warfarin and aspirin for prevention of thromboembolic complications in chronic atrial fibrillation:
the Copenhagen AFASAK Study. Lancet. 1989;1:175-179.
2. The Stroke Prevention in Atrial Fibrillation Investigators: The
Stroke Prevention in Atrial Fibrillation Trial: final results. Circu-
lation. 1991;84:527-539.
3. The Boston Area Anticoagulation Trial for Atrial Fibrillation
Investigators. The effect of low dose warfarin on the risk of stroke
in patients with non-rheumatic atrial fibrillation. N Engl J Med.
1990;323:1505-151 1.
4. Connolly SJ, Laupacis A, Gent M. Canadian Atrial Fibrillation
Anticoagulation (CAFA) Study. J Am Coil Cardiol. 1991;18:
349-355.
5. Ezekowitz MD, Bridgers SL, James KE, and SPINAF Investigators. Interim analysis of VA cooperative study, Stroke Prevention in Non Rheumatic Atrial Fibrillation (SPINAF). Circulation. 1991;84(suppl 2):II-450. Abstract.
6. Cadroy Y, Horbett TA, Hanson SR. Discrimination between
platelet mediated and coagulation mediated mechanism in a model
Downloaded from http://stroke.ahajournals.org/ by guest on March 4, 2014
Helgason et al Platelet Aggregation in Atrial Fibrillation
7.
8.
9.
10.
11.
of complex thrombus formation in vivo. J Lab Clin Med. 1989;113:
436-448.
Tegeler CH. Carotid stenosis in atrial fibrillation. Neurology. 1989;
39(suppl 1):159. Abstract.
Fuster V, Verstraete M, eds. Thrombosis in Cardiovascular Disorders. Philadelphia, Pa: WB Saunders Co; 1992:218.
Helgason CM, Tortorice KL, Winkler SR, Penney DW, Schuler JJ,
McClelland TJ, Brace LD. Aspirin response and failure in cerebral
infarction. Stroke. 1993;24:345-350.
Toghi H, Konno S, Tamura K, Kimura B, Kawano K. Effect of low
to high doses of aspirin on platelet aggregability and metabolites of
thromboxane A2 and prostacyclin. Stroke. 1992;23:1400-1404.
Umemoto K, Fukunami M, Ohmori M, Kumagai K, Sakai A,
Yamada T, Kondoh N, Minamino T, Tsujimura E, Hoki N.
Dynamic process between the clotting and the lytic activities on
intracardiac thrombin: its relationship with systemic embolization.
Jpn Circ J. 1992;56:793-800.
1461
12. Gustafsson C, Blomback M, Britton M, Hamsten A, Svensson J.
Coagulation factors and the increased risk of stroke in non-valvular
atrial fibrillation. Stroke. 1990;21:47-51.
13. Hirsh J, Dalen JE, Deykin D, Poller L. Oral anticoagulants:
mechanism of action, clinical effectiveness, and optimal therapeutic range. Chest. 1992;102:312S-326S.
14. Eldrup-Jorgensen J, Flanigan DP, Brace LD, Sawchuk AP, Mulder
SG, Andersen CP, Schuler JJ, Meyer JR, Durham JR, Schwarcz
TH. Hypercoaguable states and lower limb ischemia in young
adults. J Vasc Surg. 1989;9:334-341.
15. Ferroni P, Gazzaniga PP. Evaluation of the clinical utility of
platelet aggregation studies in the long term follow up of patients
with atherosclerotic vascular disease. J Clin Lab Anal. 1992;6:
257-263.
16. Hirsh J, Dalen JE, Fuster V, Harker LB, Salzman EW. Aspirin and
other platelet active drugs: the relationship between dose, effectiveness, and side effects. Chest. 1992;102:327S-336S.
Downloaded from http://stroke.ahajournals.org/ by guest on March 4, 2014