16 Imaging Basics: Signal-to-Noise Ratio
advertisement

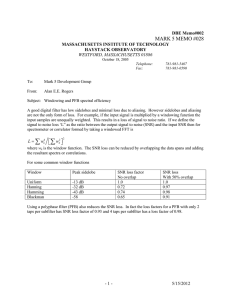
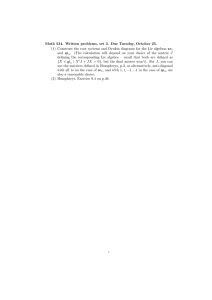
16 Imaging Basics: Signal-to-Noise Ratio The images in this case illustrate the critical concept of signal-to-noise ratio (SNR) in MR. SNR, as the term implies, is the ratio of MR signal to noise, specifically for the spatially encoded voxel. MR images acquired with a low SNR appear somewhat “grainy” to the eye (Figs. 16.1a, 16.2a), especially when compared with images acquired with higher SNR (Figs. 16.1b, 16.2b). However, what is most relevant clinically is the contrast-to-noise ratio (CNR), not the SNR. The higher the contrast between two structures, the less SNR required for differentiation. To distinguish tissues that have similar contrast, high SNR is required. For example, the difference between gray and white matter (small white arrows, Fig. 16.2b) is much easier to see in Fig. 16.2b (with higher SNR) than in Fig. 16.2a. What determines the signal in a spatially encoded voxel? MR signal is directly proportional to the size of the voxel. The larger the voxel, the greater the number of hydrogen protons and thus the greater the MR signal. Larger voxels, however, result in reduced spatial resolution (see Chapter 15). The parameters that affect the size of the voxel in a 2D acquisition are field of view (FOV), the number of phase encoding steps (acquired phase encoding matrix), the number of frequency-encoding steps (acquired frequency or read matrix), and the slice thickness. As stated, SNR is directly proportional to the size of the voxel. So, for example, doubling the slice thickness will double the voxel volume and double SNR. However, the FOV affects the voxel volume in two dimensions. As such, redu­cing the FOV by a factor of 2 would reduce the voxel volume and SNR by a factor of 4. Turning to a consideration of noise, the noise in a voxel is proportional to the square root of the sampling bandwidth (an operator-defined variable) for the voxel divided by the square root of the total number of times the voxel is sampled. The parameters that affect the number of times the voxel is sampled, and thus the noise in the voxel, are the number of phase encoding steps, the number of slices encoded (for a 3D acquisition only), and the number of signals averaged (NSA). NSA is the number of times each line of k space is sampled and is also known as the number of excitations (NEX) or acquisitions, depending on vendor. NSA is the parameter most often increased in the clinical setting to increase SNR. The problem with increasing NSA to increase SNR (in this case by reducing the noise) is that the total scan time is directly related to the NSA whereas the SNR is related to the square root of the change in NSA. For example, if NSA (and thus scan time) is increased by a factor of 4 (the difference between A and B in Figs. 16.1 and 16.2), SNR will only increase by a factor of the square root of 4 (and thus 2). As noted, SNR is also inversely proportional to the square root of the sampling (receiver) bandwidth of the encoded voxel. For example, if one were to reduce the receiver bandwidth by a factor of 2, SNR would increase by a factor of the square root of 2. Although receiver bandwidth does not affect scan time, reducing the receiver bandwidth does increase chemical shift artifact (see Chapter 100), which can be more problematic at higher field strengths. Fig. 16.1 presents thin section sagittal T1-weighted images, with the only difference between (a) and (b) being NSA. One signal average was used for (a), and four for (b), with the scan times being 1:12 and 4:48 min:sec, respectively. Referencing the prior discussion, increasing NSA by a factor of 4 results in a twofold increase in SNR, reflected by the 38 Runge_CH16.indd 38 9/29/13 5:37 AM 39 a b Fig. 16.1 a b Fig. 16.2 r­ eduction in “graininess” in the image, but at the cost of a fourfold increase in scan time. The patient has long-standing compensated hydrocephalus due to a small tectal mass (arrow) causing obstruction of the cerebral aqueduct. Fig. 16.2 presents axial T2-weighted ­images with the difference between (a) and (b) again being a fourfold increase in scan time, translating to a twofold improvement in SNR. An expansile mass fills the left cavernous sinus (black arrow, b), representing residual tumor (meningioma) in this postoperative patient. The lesion is encasing the carotid artery (the central black flow void). Note the improved depiction of the carotid artery and its interface with surrounding tumor in (b), due to the improved SNR. The “graininess” of the image in (a) can be ­appreciated, when compared with (b), due to the lower SNR. However, the difference is less evident than in Fig. 16.1. If SNR in a scan is already fairly high, then increasing SNR further will be of little benefit (and be difficult to appreciate), in part explaining this observation. Runge_CH16.indd 39 9/29/13 5:37 AM