Documento descargado de http://www.elsevier.es el 01/10/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.
Acta Otorrinolaringol Esp. 2012;63(1):15---20
www.elsevier.es/otorrino
ORIGINAL ARTICLE
Cochlear Implant in Patients With Sudden Unilateral Sensorineural
Hearing Loss and Associated Tinnitus夽
Ángel Ramos,a Rubén Polo,b Elisabeth Masgoret,a Ovidio Artiles,a Isidoro Lisner,a,∗
María L. Zaballos,a Cecilia Moreno,a Ángel Osorioa
a
Servicio de Otorrinolaringología, Complejo Hospitalario Universitario Insular Materno-Infantil, Las Palmas de Gran Canaria,
Spain
b
Servicio de Otorrinolaringología, Hospital Ramón y Cajal, Madrid, Spain
Received 27 March 2011; accepted 27 July 2011
KEYWORDS
Cochlear implant;
Tinnitus;
Sudden hearing loss
PALABRAS CLAVE
Implante coclear;
Acúfeno;
Hipoacusia súbita
Abstract
Introduction and objectives: To assess the efficacy of cochlear implantation in patients with
unilateral sudden sensorineural hearing loss and associated disabling tinnitus.
Methods: Ten patients suffering from severe-to-profound sudden hearing loss and tinnitus in
the affected ear received implants. The sample comprised 4 men and 6 women, with a mean
age of 42.7 years (range 34---62) at implantation. The severity of the tinnitus was evaluated with
the Spanish validated version of the Tinnitus Handicap Inventory (THI) and a visual analogue
scale. These assessments were obtained before and after implantation.
Results: Tinnitus suppression was observed in 2 patients. In 7 cases, we observed an improvement in the THI, in different degrees, and 1 patient remained without changes. Tinnitus
worsening was not found in the series studied.
Conclusions: Tinnitus reduction following cochlear implantation can be explained by several
mechanisms, such as habituation, acoustic masking, direct stimulation of the cochlear nerve and
reorganisation of cortical areas. Even though further research is required, cochlear implantation
is an effective method for the treatment of disabling tinnitus in patients with severe-toprofound unilateral sudden sensorineural hearing loss.
© 2011 Elsevier España, S.L. All rights reserved.
Implante coclear en pacientes con hipoacusia súbita unilateral y acúfeno asociado
Resumen
Introducción y objetivos: Valorar la eficacia del implante coclear en pacientes con hipoacusia
súbita unilateral y acúfeno incapacitante asociado.
夽 Please cite this article as: Ramos Á, et al. Implante coclear en pacientes con hipoacusia súbita unilateral y acúfeno asociado.
Acta Otorrinolaringol Esp. 2012;63:15---20.
∗ Corresponding author.
E-mail address: ilisner@hotmail.com (I. Lisner).
2173-5735/$ – see front matter © 2011 Elsevier España, S.L. All rights reserved.
Documento descargado de http://www.elsevier.es el 01/10/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.
16
Á. Ramos et al.
Métodos: Se han implantado 10 pacientes con hipoacusia súbita severa-profunda unilateral
y acúfeno asociado, entre los cuales 4 son varones y 6 mujeres, con media de edad a la
implantación de 42,7 años (rango: 34-62). Hemos evaluado la severidad del acúfeno mediante
el Tinnitus Handicap Inventory (THI) en su versión validada al castellano y una escala analógica
visual pre y postimplantación.
Resultados: Se ha observado una supresión del acúfeno en dos pacientes. Siete pacientes han
experimentado una mejoría del THI en distintos grados y no se han producido cambios en un
paciente. No ha habido empeoramiento del acúfeno en ningún caso de la serie estudiada.
Conclusiones: La reducción del acúfeno tras implantación coclear se puede deber a varios
mecanismos, tales como la habituación, enmascaramiento acústico, estimulación directa del
nervio coclear y reorganización de las áreas corticales. Aunque sean precisos más estudios,
el implante coclear es un método efectivo para el tratamiento del acúfeno incapacitante en
pacientes con hipoacusia súbita severa-profunda unilateral.
© 2011 Elsevier España, S.L. Todos los derechos reservados.
Introduction
Tinnitus is defined as an auditory sensation without an external stimulus. It is a common symptom in patients who
are candidates for cochlear implant and has a prevalence
between 66% and 88%.1
Numerous studies have shown the suppression of tinnitus
by electrical stimulation of the acoustic pathway through
a cochlear implant, with a low risk of worsening after
implantation.2---4
A recent, innovative indication with promising results has
been the cochlear implant fundamentally to treat the tinnitus in patients with unilateral sensorineural hearing loss and
associated disabling tinnitus.5---8
The purpose of our study was to assess the effectiveness
of cochlear implantation in patients with sudden, unilateral, severe-profound hearing loss and associated disabling
tinnitus.
Methods
We performed a descriptive study with a design including
repeated measurements, in which each subject acted as
their own control. These subjects were 10 patients included
in the study according to the following criteria:
1. Ethical approval by the hospital and the Department of
Health.
2. Severe-profound sensorineural hearing loss in the ear to
be implanted; disyllabic tests <40% without lip reading
at 65 dB SPL.
3. Normal hearing or moderate hearing loss in contralateral
ear. Disyllabic tests >50% in silence at 65 dB SPL in the
best conditions, without the aid of lip reading.
4. Degree of disability in Tinnitus Handicap Inventory (THI)
>58%.
5. Tinnitus in the ear to be implanted. Onset after sudden
idiopathic hearing loss.
6. Failure of prior treatments.
7. Duration of hearing loss <10 years in the ear to be
implanted.
8. Duration of tinnitus <3 years.
9. No central source of tinnitus (diabetes, etc.).
Patients were assessed before the intervention using a
battery of medical, audiological and psychological tests to
determine correct treatment and to establish tinnitus and
speech perception ability. The assessment protocol used for
the study (Table 1) was based on a set of tests that investigated the involvement of 3 symptoms (tinnitus, hyperacusis
and hearing loss). With respect to tinnitus assessment,
we carried out a tinnitus test measuring 3 characteristics
(timbre, intensity and minimum masking level), along with
objective evaluation tests for tinnitus that included an initial evaluation questionnaire, a visual analogue scale9 (VAS)
and THI10,11 through 25 questions designed to measure the
disability caused by tinnitus.
As for quantifying the hyperacusis, we carried out the
hyperacusis test (HST),12---14 a numerical scale of discomfort
caused by sounds and a list of activities that the patient
could not perform secondarily.
The hearing assessment included a complete audiometry
with air conduction, bone conduction, logoaudiometry and
threshold of discomfort. This last test allowed us to assess
the association of tinnitus with hearing loss and thus regulate the prosthesis adequately. We also carried out a tonal
and verbal assessment of the prosthesis using headphones,
open field without hearing aids and open field with hearing
aids.
The study included a total of 10 patients, of which 4 were
male and 6 were female, with a mean age at implantation
of 42.7 years (range between 34 and 62 years). The mean
duration of hearing loss was 3.8 years (range between 1
and 5 years), while the mean duration of tinnitus was 1.5
years (range between 1 and 3 years). Patients presented
profound, unilateral sensorineural hearing loss with a mean
value of 90 dB (range between 83 and 110 dB); the right ear
was implanted in 5 patients and the left in the remaining 5.
We performed a follow-up period ranging between 3 and 18
months. All patients had been implanted and, depending on
the degree of their hearing loss, were carriers of a cochlear
implant model Freedom (4), Nucleus CI 512 (1) or Nucleus
Hybrid L24 (5) (Table 2).
With respect to the assessment of tinnitus
(Tables 3 and 4), 3 patients reported a holocranial
location, 4 a bilateral location and 3 a unilateral location.
Constant tinnitus was identified in all patients; frequencies
were low (250---1000 Hz) in 4 patients, high (≥5000 Hz) in
Documento descargado de http://www.elsevier.es el 01/10/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.
Implant in Patients With Sudden Unilateral Sensorineural Hearing Loss and Associated Tinnitus
Table 1 Evaluation Protocol Used in the Study of Tinnitus:
Set of Tests That Evaluate the Implication of the 3 Symptoms
(Tinnitus, Hyperacusis and Hearing Loss).
Symptom
Measurement
Tinnitus
Intensity
Timbre
MML
Degree of
disability
Hyperacusis
Hearing loss
Presence
and degree
of symptom
Full audiological
exploration
Location of the
lesion
Functional gain
Test to Obtain Results
Tinnitus test
THI
Subjective discomfort
scale
VAS
Initial evaluation
questionnaire
HST
List of activities
Numerical scale
of discomfort
with sounds
Reduced dynamic
range
Tonal audiometry
Verbal audiometry
Open field with and
without hearing aid
HST: hyperacusis test; MML: minimum masking level; THI: tinnitus handicap inventory; VAS: visual analogue scale.
3, complete frequential in 2 patients and with a value of
2000 Hz in 1 patient. The mean intensity of the tinnitus was
4.5 dB (range between 4 and 5 dB).
Patient evaluation was carried out at 1, 3 and 6 months
after implant activation. After activation of the cochlear
implant, tinnitus retraining therapy (TRT) was applied in
those patients who did not show sufficient improvement in
tinnitus in the second evaluation after 3 months. This sound
therapy used habituation noises through the audio input of
the cochlear implant processor.
All participants were scheduled according to a specific
method based on tests and trials conducted during a pilot
study, in which a tinnitus test was used to calculate the
Table 2
17
frequency of tinnitus. The electrodes that corresponded to
the frequency determined by the tinnitus test were stimulated so as to identify which one was closest to the tinnitus.
Once the electrode was identified, the 4 collateral electrodes were given the same levels of T. These 5 electrodes
maintained their similar T as if they were acting as a single electrode, but with a greater bandwidth frequency. To
determine the C level of the tinnitus areas, we increased
the intensity until it equalled that of tinnitus. This C level
was also applied to the 4 collateral electrodes. The T and
C levels in other areas were determined according to the
programming of the standard cochlear implant. We created
4 maps and, after 10 days, 1 of them was maintained as
the reference map to start working on the implant programming. The processor configuration was modified on a
monthly basis to improve the acceptance of the device and
speech understanding.
Results
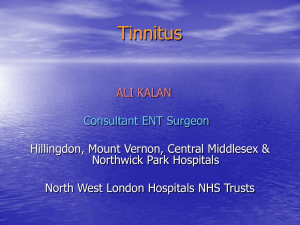
The mean score obtained in the preoperative THI was 72.1%.
After cochlear implantation, THI values at 1 and 3 months
fell to 27.4% and 14.3%, respectively (Fig. 1). In 2 of the 10
patients, we observed complete suppression of tinnitus; in
the remaining 8, we observed a significant decrease in its
perception.
In relation to the degree of disability according to the
THI score (absence of disability: 0%---16%, mild disability:
18%---36%, moderate disability, 38%---56%, severe disability: >58%), 10 patients presented a severe disability prior
to cochlear implantation. Three months after surgery, 8
patients presented no disability, 1 patient presented mild
disability and severe disability persisted in another patient
despite an improvement in THI score.
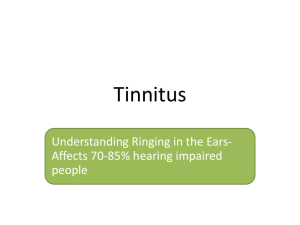
The VAS showed a reduction from 7.9 points preoperatively to 2.7 points at 3 months postoperatively
(Fig. 2).
As for the perception of tinnitus in percentage of hours
per day, there was a reduction from 100% (preoperative
value) to 11% (3 months postoperatively). It was observed
that the improvement in tinnitus perception remained even
when the implant was switched off.
In selected cases with residual hearing and in cases
with contralateral hearing loss, hybrid and bimodal
Comparison of the 10 Patients in the Study Through the Tinnitus Evaluation Protocol.
No.
MAT Right Ear
MAT Left Ear
Implant Side
Contralateral Side
Cochlear Implant Type
1
2
3
4
5
6
7
8
9
10
86.67
83.33
93.33
43.33
98.33
16.67
13.33
25
38
Deafness
51.67
70
83.33
86.67
61.67
85
105
80
82
25
Right
Right
Right
Left
Right
Left
Left
Left
Left
Right
Hearing
Hearing
Hearing
Hearing
Hearing
CI24REH L
CI24RE (CA)
CI24RE (CA)
CI24REH L
CI24RE (CA)
CI24REH L
CI512
CI24REH L
CI24REH L
CI24RE (CA)
MAT: mean auditory threshold at 0.5, 1, 2 and 4 kHz.
aid
aid
aid
aid
aid
Documento descargado de http://www.elsevier.es el 01/10/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.
18
Á. Ramos et al.
Characteristics of Tinnitus Regarding Location, Type, Frequency and Intensity.
Table 3
Type of Implant
Location
Type
Frequency
Intensity
Hybrid 1
Hybrid 2
Hybrid 3
Hybrid 4
Unilateral
Constant
250---5000 Hz
5 dB
Bilateral
Constant
250 Hz
5 dB
Holocranial
Constant
6000 Hz
4 dB
Holocranial
Constant
250---1000 Hz
5 dB
Hybrid 5
Unilateral
Constant
250---5000 Hz
5 dB
Characteristics of Tinnitus (Location, Type, Frequency and Intensity).
Table 4
Type of Implant
CI24Re(CA)1
CI24Re(CA)2
CI24Re(CA)3
CI24Re(CA)4
CI512
Location
Type
Frequency
Intensity
Bilateral
Constant
5000 Hz
5 dB
Bilateral
Constant
2000 Hz
4 dB
Unilateral
Constant
6000 Hz
5 dB
Holocranial
Constant
250---1000 Hz
5 dB
Bilateral
Constant
250---1000 Hz
4 dB
THI
100
90
90
82
78
80
70
68
68
63
73
72
65
58
59
60
72.1
68
Preoperative THI
48
50
Postoperative THI (1 month)
40
40
30
28
30
Postoperative THI (3 months)
31
28
27.4
10
14.3
10
1010
1
10
4
2
4
2
0
0
Figure 1
tion.
19
18
20
2
3
4
5
6
0
7
8
9
10 Mean
Graph showing Tinnitus Handicap Inventory (THI) values preoperatively, 1 month and 3 months after cochlear implanta-
10
10
10
10
9
9
9
8
7.9
8
7
7
6
6
5
5
5
5
Preoperative
4
4
Postoperative
4
3
3
3
3
3
2.7
2
1
1
1
0
0
Figure 2
1
2
3
4
5
6
7
8
9
10 Mean
Visual analogue scale (VAS) for the evaluation of tinnitus preoperatively and after cochlear implantation.
Documento descargado de http://www.elsevier.es el 01/10/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.
Implant in Patients With Sudden Unilateral Sensorineural Hearing Loss and Associated Tinnitus
100
92
76
75
80
65
88
74
82
64
60
CI alone
52 52
42
HA
40
22
CI + HA
20
0
Bi Hy1
Bi Hy2
Bi CA1
Bi CA2
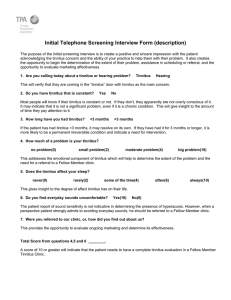
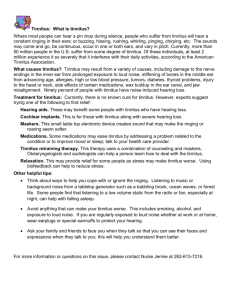
Figure 3 Disyllabic test at 12 months after cochlear implantation, in patients with contralateral hearing aid (results
with cochlear implants [CI], hearing aids [HA] and cochlear
implant + hearing aid). The first 2 patients were carriers of a
hybrid Nucleus L24 and the other 2 patients of a Nucleus CI512.
stimulation, respectively, showed good results regarding
hearing (Figs. 3 and 4) and tinnitus control.
Discussion
According to Bauer,15 the estimated prevalence of adults
with chronic tinnitus varies between 6% and 20%. Of these,
between 1% and 3% suffer disabling tinnitus that interferes
with their quality of life. The genesis of tinnitus is explained
as a negative consequence of neural plasticity of the central
nervous system after a peripheral aggression.
Scientific evidence has shown that reorganisation processes take place in the auditory cortex after suffering
tinnitus associated to sensorineural hearing loss, as well as
an overstimulation of certain tonotopic cortical areas. Herraiz et al.16 found that acoustic rehabilitation reduced the
impact of this reorganisation and improved tinnitus.
Numerous studies support the suppression or improvement of tinnitus after cochlear implantation.2---4,17---19 On
average, between 60% and 90% of tinnitus cases in implanted
patients with hearing loss show an improvement in perception, which sometimes even reaches its disappearance. This
effect may persist for a certain time after switching off the
processor, probably in relation to residual inhibition.20 Moreover, in some patients electrical stimulation of the auditory
pathway succeeds in improving or even suppressing contralateral tinnitus.19,21
100
96
100
100
100
80
52
60
40
22
20
0
CI alone
Normal hearing
34
Asy Hy1
Asy Hy2
In our study, we observed a suppression of tinnitus in 2
patients (20%), whereas 8 experienced an improvement in
its perception (80%). In connection with the score obtained
on the THI, there was a reduction from 72.1% in the preoperative period to 14.3% in the 3 postoperative months.
Bovo et al.19 conducted a study on 51 patients with
profound, bilateral sensorineural hearing loss, who were
candidates for cochlear implantation. The study cohort for
tinnitus and cochlear implant was reduced to 36 patients;
in 11 patients (30.5%), there was a suppression of tinnitus;
in 16 (44.4%), its perception decreased; in 5 (13.9%), there
was no change and in 4 patients (11.1%), there was a worsening. In connection with THI, there was an improvement in
72.2% of patients, no change in 2.8% and a worsening in 25%
of cases. Of the 36 patients, 27 presented bilateral tinnitus
and there was an improvement of contralateral tinnitus in
10 of them (45%).
Di Nardo et al.18 established 2 study groups: group A,
composed of 20 patients with preimplantation tinnitus, and
group B, composed of 10 patients without preimplantation
tinnitus. No patient in group B presented postimplantation
tinnitus. In group A, there was a suppression of tinnitus
in 8 patients (40%), its perception decreased in 6 (30%), 5
patients (25%) did not experience any changes and 1 patient
(5%) reported a worsening of tinnitus.
In recent years, cochlear implants have been used in
a novel way in patients with unilateral, severe-profound
sensorineural hearing loss with associated disabling tinnitus
and normal contralateral hearing with good results.5,6,8 The
largest series studied to date includes 5 patients. Of these,
tinnitus was suppressed in 3 and its perception improved in
2.5
Our study results are encouraging, but we must be cautious in their interpretation. Undoubtedly, further work with
a larger patient cohort is needed to refine the selection
criteria in these cases.
Conclusions
Cochlear implants can reduce or suppress incapacitating
tinnitus in patients with unilateral, severe-profound sensorineural hearing loss and normal contralateral hearing.
It is a valid and effective therapy when other treatments
have failed. In selected cases with residual hearing and
in cases suffering contralateral hearing loss, hybrid and
bimodal stimulation, respectively, have shown good results
in hearing and in the control of tinnitus.
The reduction of tinnitus after cochlear implantation may
be due to several mechanisms, such as habituation, acoustic masking, direct stimulation of the cochlear nerve and
reorganisation of cortical areas.
Conflict of Interests
16
Asy Hy3
19
Asy CA1
Figure 4 Disyllabic test at 12 months after cochlear implantation, in patients with normal contralateral hearing. The first
3 patients were carriers of a hybrid Nucleus L24 and the other
patient of a Nucleus CI512.
The authors have no conflicts of interest to declare.
References
1. Quaranta N, Wagsta VS, Baguley D. Tinnitus and cochlear
implantation. Int J Audiol. 2004;43:245---51.
Documento descargado de http://www.elsevier.es el 01/10/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.
20
2. Miyamoto RT, Bicheley BG. Cochlear implantation for tinnitus suppression. Otolaryngol Clin North Am. 2003;36:
345---52.
3. Ruckenstein MJ, Hedgepeth C, Rafter KO, Montes ML,
Bigelow DC. Tinnitus suppression in patients with cochlear
implants. Otol Neurotol. 2001;22:200---4.
4. Ito J. Tinnitus suppression in cochlear implant patients. Otolaryngol Head Neck Surg. 1997;117:701---3.
5. Buechner A, Brendel M, Lesinski-Schiedat A, Wenzel G,
Frohne-Buechner C, Jaeger B, et al. Cochlear implantation in
unilateral deaf subjects associated with ipsilateral tinnitus.
Otol Neurotol. 2010;31:1381---5.
6. Kleinjung T, Steffens T, Strutz J, Langguth B. Curing tinnitus with
a Cochlear Implant in a patient with unilateral sudden deafness:
a case report. Cases J. 2009;2:7462.
7. Van de Heyning P, Vermeire K, Diebl M, Nopp P, Anderson I,
De Ridder D. Incapacitating unilateral tinnitus in single-sided
deafness treated by cochlear implantation. Ann Otol Rhinol
Laryngol. 2008;117:645---52.
8. Masgoret E, Meran J, Moreno C, Falcón JC, Artiles O, Ramos A.
Acúfeno e implante coclear. Experiencia preliminar. Acta Otorrinolaringol Esp. 2010;61:405---11.
9. Miller MD, Ferris DG. Measurement of subjective phenomena in
primary care research: the Visual Analogue Scale. Fam Pract Res
J. 1993;13:15---24.
10. Newman CW, Jacobson GP, Spitzer J. Development of Tinnitus Handicap Inventory. Arch Otolaryngol Head Neck Surg.
1996;122:143---8.
11. Herráiz C, Hernández Calvín J, Plaza G, Tapia MC, de los Santos
G. Evaluación de la incapacidad en pacientes con acúfenos. Acta
Otorrinolaringol Esp. 2001;52:534---8.
Á. Ramos et al.
12. Nelting M, Rienhoff NK, Hesse G, Lamparter U. Die Erfassung
des subjektiven Leidens unter Hyperakusis mit einem Selbstbeurteilungsbogen zur Geräuschüberempfindlichkeit (GÜF).
Laryngo-Rhino-Otol. 2002;81:327---34.
13. Herráiz C, de los Santos G, Diges I, Díez R, Aparicio JM. Evaluación de la hiperacusia: test de hipersensibilidad al sonido. Acta
Otorrinolaringol Esp. 2006;57:303---6.
14. Dauman R, Bouscau-Faure F. Assessment and amelioration of
hyperacusis in tinnitus patients. Acta Otolaryngol (Stockh).
2005;125:503---8.
15. Bauer CA. Mechanisms of tinnitus generation. Curr Opin Otolaryngol Head Neck Surg. 2004;12:413---7.
16. Herráiz C. Mecanismos fisiopatológicos en la génesis y cronificación del acúfeno. Acta Otorrinolaringol Esp. 2005;56:335---42.
17. Tyler RS, Rubinstein J, Pan T, Chang SA, Gogel SA, Gehringer A,
et al. Electrical stimulation of the cochlea to reduce tinnitus.
Semin Hear. 2008;29:326---32.
18. Di Nardo W, Cantore I, Cianfrone F, Melillo P, Scorpecci A,
Paludetti G. Tinnitus modificacions after cochlear implantation.
Eur Arch Otorhinolaryngol. 2007;264:1145---9.
19. Bovo R, Ciorba A, Martini A. Tinnitus and cochlear implants.
Auris Nasus Larynx. 2011;38:14---20.
20. Souliere Jr CR, Kileny PR, Zwolan TA, Kemink JL. Tinnitus suppression following cochlear implantation. A multifactorial investigation. Arch Otolaryngol Head Neck Surg.
1992;118:1291---7.
21. Zwolan TA, Kileny RP, Souliere CR, Kemink JL. Tinnitus suppression following cochlear implantation. In: Aran JM, Dauman R,
editors. Tinnitus 91: proceedings of the fourth international
tinnitus seminar Amsterdam. The Netherlands: Kugler; 1992.
p. 423---6.