Voltage in Biopotential Amplifiers
advertisement

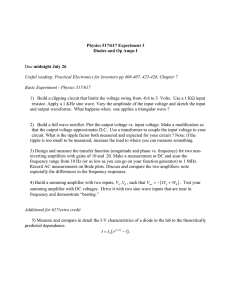
58 IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. BME-30, NO. 1, JANUARY 1983 Reductionl of Interference Due to Common Mode Voltage in Biopotential Amplifiers BRUCE B. WINTER, STUDENT MEMBER, IEEE, AND JOHN G. WEBSTER, SENIOR MEMBER, IEEE Abstract-We review how the nonideal properties of biopotential amplifiers can transform common mode voltage into interference. We then review several design approaches for two- and three-electrode amplifiers, both nonisolated and isolated, that reduce this interference. We consider the effects of static electricity on the various designs, and we show how to calculate the optimal values of the circuit components. INTRODUCTION BIOPOTENTIAL recordings such as the ECG, EEG, and EMG are frequently plagued with- interference originating from nearby power sources. There are four ways in which an electromagnetic source such as 60-Hz power lines can cause interference in a biopotential recording. 1) A magnetic field causes an induced voltage in the loop forned by the electrode leads. 2) An electric field induces into the electrode leads a displacement current which flows through the patient. This creates an interfering voltage drop across the electrode impedance. 3) An electric field induces into the patient a displacement current. This current may cause an interference voltage between the two recording electrodes as. it flows through the body impedance. 4) The current induced into the patient also creates a voltage between the two recording electrodes and the amplifier common. Since this voltage is common to both electrodes, it is referred to as the. common mode voltage v,. A portion of vu is transformed into an interfering differential voltage by the nonideal properties of the amplifier. Huhta and Webster [ 1 ] and Webster [2] present methods for reducing the interference from these four sources. Magnetic interference can be reduced by twisting the leads together to decrease the loop area, and thus the induced voltage. The effects of induced currents can be minimized by either shielding the cable or incorporating a buffer into the electrode. Careful electrode positioning avoids recording the voltage caused by displacement currents flowing through the body COMMON MODE VOLTAGE The common mode voltage on a body v, is composed of a static voltage component vU and a power-line-induced ac component va. Va is caused by a displacement current id which flows through the stray capacitances shown in Fig. 1. The sizes of these capacitances are determined by how close the patient is to power sources and grounded objects. va can be as small as a few millivolts if the patient is touching a grounded object or as large as 20 V if the patient grasps an insulated power cord. Typically, 6a is approximately 1 V. Fig. 1 shows typical values for the capacitances and displacement current. Static voltage vs is created by patient movement. Friction creates a charge that is stored in Cb, the capacitance between the body and ground. A nurse who is charged in this way can also induce a static voltage into the patient if he/she moves close to the patient [3]. Although most biopotential amplifiers filter out the dc component, a change in v5 will disrupt the baseline of the recording and may cause the amplifier to saturate [4]. EFFECTIVE COMMON MODE REJECTION RATIO Common mode voltage v. is transformed into an interfering differential voltage vi according to the following equation [1: .1st term 2nd term Vi = VC (1/CMRR + ZdlZc) (1) where Zd = difference between the two electrode impedances c= common mode impedance CMRR = differential gain/common mode gain. The ability of a differential amplifier to reject common mode voltages and to amplify differential voltages is defined as impedance. This paper addresses the reduction of the fourth source of its common mode rejection ratio (CMRR). Ideally,; the CMRR interference listed above. We first examine how common is infinite, but because of nonlinearities and because compomode voltage is transformed into a differential voltage. We nents can never be exactly matched, typical CMRR's range then show how this interference can be minimized in noniso- from 60 to 120 dB. The second term in (1) is due to the voltage divider formed lated -and isolated amplifiers. We review both two- and threeby the electrode impedances and the amplifier's input impeelectrode amplifiers. dance as shown in Fig.. 2. If the electrode impedances Z1 and Z2 differ, then v, will be attenuated more at one of the differManuscript received January 18, 1982. B. B. Winter was with the Department of Electrical and Computer En- ential inputs than at the other: gineering, University of Wisconsin, Madison, WI 5 3706. He is now with the IBM Corporation, Rochester, MN 55901. J. G. Webster is with the Department of Electrical and Computer Engineering, University of Wisconsin, Madison, WI 53706. [Z2/(Z2 + Zc) - Z1/(Z 1 + ZA)] (2) Z. is the impedance to common presented by stray capaciUd - Ve 0018-9294/83/0100-0058$01.00 © 1983 IEEE Authorized licensed use limited to: UNIVERSITA MODENA. Downloaded on March 19,2010 at 10:36:16 EDT from IEEE Xplore. Restrictions apply. 59 WINTER AND WEBSTER: COMMON MODE VOLTAGE AND BIOPOTENTIAL AMPLIFIERS .sour.D Zi V L Fig. 1. The total common mode voltage on a body vC is composed of a static voltage component vs and a power-line-induced ac component Ua. va is typically 1 V and vs can be between zero and several thousand volts. DIFFERENTIAL R2 _ kl 1~~06 0 l_ ~~~~~~1 102 104 106 FREQUENCY, Hz (a) (b) Fig. 3. (a) Circuit diagram of a high-input-impedance bootstrap input buffer that provides input bias current to A4 through RI and R2. ul connects to the patient. v2 drives the rest of the amplifier. (b) Input impedance of the buffer as a function of frequency. Since a third electrode is not used, current cannot flow through it and the body to provide input bias current for the positive terminal of the op amp. The bootstrap input buffer of Fig. 3(a) supplies input bias current required by A4 through R1 and R2 and also provides the required high input impedance [4], [5]: Zi = R1/(I V3/vO) - Fig. 2. Common mode voltage can be transformed into a differential voltage if the. electrode impedances are imbalanced. tance and RF capacitors that are present at the input of the plifier. SinceZc is much greater than the electrode impedanc V3 = R2 [(V1 - V3)/R1 + (V2 - V3) Cl S] lGo + TaSlGo). Combining (5), (6), and (7), V2= v1/(l + [Rl (1 + 'rS) +R2](1 + I/Go +STaIGo) (5) (6) (7) (8) where Zd = Z2- Z1. i s2TTaIGo + s(7-1 + 'Ta)/Go + 1 + IlGo Thus, a low input impedance and a high electrode impeda where imbalance will transform vc into an interfering differen 'Ta = 1 /(27rfa), fa = corner frequency of op amp voltage according to (3). But a low input impedance; determi lowers vc. We will show that the optimum Zc is 'Ti =R2C1, Go = op amp's open-loop gain. by the degree of amplifier isolation from earth ground. A! Fig. 3(b) shows a typical frequency response of Zi. For frecommercially available amplifiers that have 50-200 pF cap below G0/(7-1 + Ta) and below [GoI'ria] 1/2, Z, bequencies tance from amplifier common to earth ground lower Zc haves as an inductance in series with a resistance: betw high frequencies by placing 100-500 pF capacitors each of the leads and amplifier common. Zi= RlR2CIs+R1 +R2(9) The second term of (1) has the same effect as the first te This derivation has neglected the common mode input impethey both determine how much of vc is transformed into indance Zcm of the op amp A4. Equation (9) holds as long as Re, terference. We lump the two terms together and call it CMR «Zm . With JFET op amps, this is no restriction because Zo<<Z the effective CMRR of the system: Zcm is very large. A bipolar op amp should not be used because CMRRe = 1/(I /CMRR + ZdIZc). (4) Zem may be low enough to cause a problem, and thus (9) would hold only for low frequencies. INTERFERENCE REDUCTION IN NONISOLATED AMPLIFIEERS Fig. 4 shows the equivalent circuit of a body that is charged There are two ways to reduce the interference predictedI by with a static voltage and coupled with the circuit of Fig. 3. (1). With most two-electrode amplifiers, the approach is tc) in- For a step input, the output will oscillate with a decay time crease CMRRe so that vi will be within acceptable limits vvith constant 72: the largest expected vc. The second approach is to add a ti (10) T2 =2RR2C1/(R1 +R2). electrode in order to reduce v,. If 'T2 is too large, then any static voltage that appears on the A Two-Electrode Amplifier body may dissipate slowly, and thus saturate the amplifier or create unacceptable interference according to (1) [4]. If the Thakor and Webster [4] have presented the design consii ations for a two-electrode ECG amplifier. For a nonisol bootstrap circuit is designed for a short 'T2, however, static amplifier, a CMRR of 100 dB and a Zc of 1 G&2 are requi voltage conditions may be tolerable. Vd = VcZd/Zc Authorized licensed use limited to: UNIVERSITA MODENA. Downloaded on March 19,2010 at 10:36:16 EDT from IEEE Xplore. Restrictions apply. IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. BME-30, NO. 1, JANUARY 1983 60 RIGHT LEG L =R RI2C1 C~b B R= R+R2 EARTH GROUND - Fig. 4. Equivalent circuit of the buffer of Fig. 4 when it is coupled to a body that is charged to a static voltage. Cb is the body capacitance to earth ground. For Z1 = 1 GE at 60 Hz and r2 100 ms, we choose C1 = 1 pF. According to (9), RjR2 =2.6X 1012. (11) According to (10), EARTH GROUND Fig. 5. A simple grounding circuit that provides a low-impedance path to ground for currents less than 1 MiA and a high impedance to ground for currents greater than 1 AA. guarantee that less than 20 pA will flow if the patient acciden- R1+R2=52X 106 . There are two solutions to (1 1) and (12): 1)R =50Mn,R2 50kE2 2) R, = 50 kf R2 =50 ME. - or (12) tally touches a 120-V 60-Hz power source, the input circuit common must have less than 440 pF of stray capacitance to earth ground. Two-Electrode Isolated Amplifiers Fig. 6 shows that v, in isolated amplifiers is determined by Solution 2) yields a large r1. Equation (8) indicates that to the voltage divider formed by Zc and Z, where Z, is the commaximize the frequency range for which the circuit looks in- mon mode input impedance of the amplifier and Z, E the isoductive, we should minimize r1. Thus, we chose solution (1), lation impedance presented by the stray capacitance C,: which yielded the predicted time constant of 100 ins. (13) UC = Vb [Zc/(Zs + Z)I -VbZclZs Three-Electrode Amplifiers Ub = body voltage with respect to earth ground. The other approach to reducing interference due to common mode voltage is to reduce vc. This is done by placing a third electrode on the patient, which provides a low-impedance Equation (13) shows that we can reduce the v. in isolated path to ground for the displacement current id. This electrode systems to low values by decreasing Z,. The lower limit for cannot be connected directly to ground, however, because the ZC is dictated by the voltage divider effect of Zc and the elecpatient must be protected from currents of greater than 20 pA trode impedance Z. The measured differential voltage is [71. lower than the true voltage by a factor equal to Zcl(Zc + Ze). One simple way to do this is with the circuit shown in Fig. 5 In order to maintain a 20 percent calibration under worst case [8] , which makes point c a virtual ground. For currents below conditions (Ze = 100 k2), Zc should not be reduced below 1 pA, diodes D1 and D4 conduct and clamp points a and b 500 k92. near ground. The impedance from the point c to ground is Reducing the common mode impedance is not a total soluthen the forward bias resistance of diodes D2 and D3 plus the tion, however. The interference due to impedance imbalance forward bias resistance of D1 and D4. This is typically around of the electrodes [the second term in (1)] is not reduced be150 k92. For currents above 1 MA, however, diodes D1 and cause it is inversely proportional to Zc. According to (1) and D3 are reverse biased, and the impedance to ground increases (13), to 20 MQ. The most common and most effective way of utilizing the vi= (vbZclZs)(1/CMRR + ZdlZc) third electrode is with the driven-right-leg circuit where vc is (14) vi= (vb/ZS)(ZC/CMRR + Zd). actively driven to a few tenths of a millivolt. The driven-rightleg circuit reduces the effective impedance of the third elecWe can reduce both interference terms in (14) by increasing trode [9]. Z, (decreasing C). If Z, is large enough, as in biotelemetry, INTERFERENCE REDUCTION IN ISOLATED AMPLIFIERS then UC is small enough so that a third electrode is not required. In order to protect the patient from dangerous current flow, For example, (14) shows that if Vb = 1 V and if vi is to be kept most modern biopotential amplifiers feature an electrical isola- below 10 MV with a 100-k92 imbalance, then Z4 must be tion barrier between the input circuitry and earth ground. To greater than 10 G12 (Cs < 0.3 pF at 60 Hz). Authorized licensed use limited to: UNIVERSITA MODENA. Downloaded on March 19,2010 at 10:36:16 EDT from IEEE Xplore. Restrictions apply. WINTER AND WEBSTER: COMMON MODE VOLTAGE AND BIOPOTENTIAL AMPLIFIERS DIFFERENTIAL Id Zc Vc Vb \ 61 ICb I ISOLATED COMMON T EARTH GROUND Cs - Fig. 6. The common mode voltage in isolated amplifiers can be reduced by reducing Rc or by increasing Zs. Three-Electrode Isolated Amplifiers EARTH GROUND * ISOLATED +_ COMMON OF A3 In most line-powered instruments, however, such isolation is 7. A two-electrode bootstrapped common amplifier. A 3 drives the not easily achieved. - Stray capacitances between the amplifier Fig. isolated common of the input circuitry to the common mode voltage and ground can be reduced with a negative capacity amplifier of the patient. [10], but a few picofarads are typically the limit. Thus, the third electrode is used to further reduce v,. The supply voltage of A3 must be large enough to accomThe simplest approach would be to connect the third elec- modate the largest expected common mode voltage according trode directly to the isolated common. Fig. 6 shows that a to the following equation [11 ]: small resistance between the patient and the isolated common Vp >vc(Zs+Rr)IZs (15) results in a small v, Since the electrode resistance Ze can be as large as 100 kQ, the driven-right-leg circuit is usually used Rr should have a resistance of at least 10 Mi2 to isolate the to reduce its effective impedance by a factor of 100 [9]. patient from earth ground. For a stray impedance of 10 MQ (Cs = 200 pF), (15) shows that the voltage supply to A3 would A Two-Electrode Bootstrapped Common Circuit have to be greater than twice the largest common mode voltThe preceding analyses show that we can reduce vC in isolated age expected. amplifiers by: 1) increasing the isolation so that most of vb is dropped across the isolation impedance, or 2) by adding a third CONCLUSIONS electrode that passively or actively provides a low-impedance The reduction of interference due to common mode voltage path from the body to the amplifier common. We will review is accomplished in one of two ways. 1) The amplifier's effecone last approach that combines the convenience of two elec- tive common mode rejection ratio is improved so that only an trodes and the low common mode voltage of a driven-right-leg acceptable amount of is v, transformed into interference. 2) system. is or actively passively reduced before it is transformed into v, Fig. 7 shows the principle of a bootstrap circuit that is interference. The second approach can be done by 1) increaspatented by the Hewlett-Packard Corporation [I1]. It drives ing the isolation of the amplifier, 2) using the third electrode the isolated common of the input amplifier to the body volt- to equalize the voltage between the patient and the amplifier, age. Unlike the driven-right-leg circuit, the third electrode is or earth 3) using ground as a reference to drive the voltage of not needed to drive the body potential. This circuit is similar the amplifier's isolated common to the voltage on the patient. to the circuit shown in Fig. 3(a). The common mode voltage We have reviewed the equations and circuits used to impleis buffered by a unity gain amplifier A3 and fed back to the ment these approaches. isolated common end of the input impedance so that the voltage on both ends of the input impedance is nearly the same. REFERENCES This simulates a high input impedance according to (9), and [1] J. C. Huhta and J. G. Webster, "60-Hz interference in electrocarthus reduces the interference due to the second term of (1). diography," IEEE Trans. Biomed. Eng., vol. BME-20, pp. 91-101, In addition, since the circuit of Fig. 7 also drives the isolated Mar. 1973. common of the differential amplifier, the amplifier will see [2] J. G. Webster, "Interference and motion artifact in biopotentials," in IEEE Region 6 Conf. Rec., 1977, pp. 53-64. very little common mode voltage. This reduces the effect of [31 D. H. Gordon, "Triboelectric- interference in the ECG," IEEE the first term of (1). Trans. Biomed. Eng., vol. BME-22, pp. 252-255, May 1975. [4] N. V. Thakor and J. G. Webster, "Ground-free ECG recording A second isolated power supply powers A3, which drives the with two electrodes," IEEE Trans. Biomed. Eng., vol. BME-27, isolated common through C1. C1 blocks the dc offset voltages pp. 699-704, Dec. 1980. of the op amps so that the positive feedback will not saturate [51 R. P. Betts and B. H. Brown, "Method for recording electrocardiograms with dry electrodes applied to unprepared skin," Med. the op amps. R3 is included so that static voltages will be disEng., vol. 14, pp. 313-315, 1976. charged through the R, -R3J-Rr impedance path with a time [6] BioL M. R. Neuman, "Biopotential amplifiers," in Medical Instrumen= constant given by (1 1) where R2 Rr + R3. As before, we use tation: Application and Design, J. G. Webster, Ed. Boston, MA: Houghton Mifflin, 1978. (9) and (10) to calculate the values of R1, R2, and C1. Authorized licensed use limited to: UNIVERSITA MODENA. Downloaded on March 19,2010 at 10:36:16 EDT from IEEE Xplore. Restrictions apply. IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. BME-30, NO. 1, 62 "Electricity in patient care areas of hospitals," Nat. Fire Protection Ass., Quincy, MA, NFPA-76B, 1980. 8811A Bioelectric Amplifier Service Manual, Med. Electron. Div., Hewlett-Packard Corp., Waltham, MA, 1971, p. 5. B. B. Winter and J. G. Webster, "Driven-right-leg circuit design," this issue, pp. 62-66. 78213 Neonatal Heart Rate Module Service Manual, Med. Electron. Div., Hewlett-Packard Corp., Waltham, MA, 1977, p. 3.2. A. Miller, "Coupling circuit with driven guard," U.S. Patent 4 191 195, 1978. 0 X B. Winter (S'80) was born on July 8, lBruce 1958. He received the B.S. degree in electrical engineering from Montana State University, Bozeman, in 1980, and the M.S.E.E. degree k a from the University of Wisconsin, Madison, in 1981. While at the University of Wisconsin, he was a Fellow and Teaching Assistant in instrumentation and logic design. Presently, he is working with large-scale integration at the IBM Corpora- tion, Rochester, MN. JANUARY 1983 John G. Webster (M'59-SM'69) received the B.E.E. degree from Cornell University, Ithaca, NY, in 1953, and the M.S.E.E. and Ph.D. degrees from the University of Rochester, Rochester, NY, in 1965 and 1967, respectively. He is a Professor of Electrical and Computer Engineerig at the University of Wisconsin, Madison. In the field of medical instrumentation, he teaches undergraduate, graduate, and short courses, and does research on electrodes, impedance plethysmography, and portable arrhythmia monitors. Dr. Webster is Associate Editor, Medical Instrumentation, of the IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, and is a member of IEEE-EMBS Administrative Committee. He is coauthor, with B. Jacobson, of Medicine and Clinical Engineering (Englewood Cliffs, NJ: Prentice-Hall, 1977). He is Editor ofMedical Instrumentation: Application and Design (Boston, MA: Houghton Mifflin, 1978). He is coeditor, with A. M. Cook, of Clinical Engineering: Principles and Practices (Englewood Cliffs, NJ: Prentice-Hall, 1979), with W. J. Tompkins, of Design of Microcomputer-Based Medical Instrumentation (Englewood Cliffs, NJ: Prentice-Hall, 1981) and, with A. M. Cook, of Therapeutic Medical Devices: Application and Design (Englewood Cliffs, NJ: Prentice-Hall, 1982). Driven-Right-Leg Circuit Design BRUCE B. WINTER, STUDENT MEMBER, IEEE, AND Abstract-The driven-right-eg circuit is often used with biopotential differential amplifiers to reduce common mode voltage. We analyze this circuit and show that high loop gains can cause instability. We present equations that can be used to design circuits that minimize common mode voltage without instability. We also show that it is important to consider the reduction of high-frequency interference from fluorescent lights when determining the bandwidth of the drivenright-leg circuit. INTRODUCTION Wa rHEN a differential amplifier records biopotentials, the voltage of the patient with respect to the amplifier's common is called the common mode voltage vc. Since v, can be transformed by the amplifier into an interfering differential signal [1], it is desirable to minimize Vc by attaching a third electrode to the patient. This electrode provides a low-impedance path between the patient and the amplifier common so that v, is small. Connecting the electrode directly to the common is undesirable for two reasons. 1) If the circuit is not isolated, dangerous currents could flow through the third electrode. 2) A poor electrode contact may present up to 100 k92 of resistance between the patient and the common. The most common and effective use of the third electrode W Manuscript received January 18, 1982; revised July 23, 1982. B. B. Winter was with the Department of Electrical and Computer Engineering, University of Wisconsin, Madison, WI 53706. He is now with the IBM Corporation, Rochester, MN 55901. J. G. Webster is with the Department of Electrical and Computer Engineering, University of Wisconsin, Madison, WI 53706. JOHN G. WEBSTER, SENIOR MEMBER, IEEE is to connect it to a driven-right-leg circuit [2], [3]. This circuit overcomes both of the problems listed above. It reduces the effective electrode resistance by several orders of magnitude, and it allows only a safe amount of current to flow through the third electrode. Although the circuit is used extensively in modern biopotential amplifiers [4]-[6], little has been written on optimal design technique. We present a design approach that results in the minimization of v,. However, a nonoptimal driven-right-leg circuit may seem to work as well as one that minimizes vc because: 1) the nonoptimal circuit reduces the interference to a level that is below the sensitivity of the recorder, or 2) other sources create more interference than vc [7], [8]. CIRCUIT DESCRIPTION Fig. I shows the components of the driven-right-leg circuit. Resistors Ra and Ra average the voltage of the differential electrode pair to sense vc. A3 amplifies and inverts this voltage and feeds it back to the body via the third electrode. For ECG systems, the third electrode is commonly applied to the right leg; hence, we have the name driven-right-leg circuit. Fig. 2 shows an equivalent circuit of the system shown in Fig. 1. The displacement current id that flows into the body via stray capacitances to nearby power lines divides between the current that flows directly to ground id, and the current that flows back to ground through the driven-right-leg circuit 1d2: 'd2 = idCsl(CS + Cb). 0018-9294/83/0100-0062$01.00 1983 IEEE Authorized licensed use limited to: UNIVERSITA MODENA. Downloaded on March 19,2010 at 10:36:16 EDT from IEEE Xplore. Restrictions apply. (1)