Medicine The American Journal of Sports P<P
advertisement

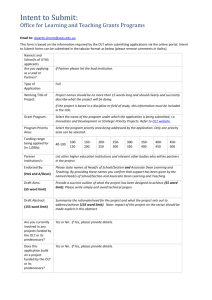
The American Journal of Sports Medicine http://ajs.sagepub.com/ Osteochondral Autologous Transplantation Is Superior to Repeat Arthroscopy for the Treatment of Osteochondral Lesions of the Talus After Failed Primary Arthroscopic Treatment Hang Seob Yoon, Yoo Jung Park, Moses Lee, Woo Jin Choi and Jin Woo Lee Am J Sports Med published online June 6, 2014 DOI: 10.1177/0363546514535186 The online version of this article can be found at: http://ajs.sagepub.com/content/early/2014/06/05/0363546514535186 Published by: http://www.sagepublications.com On behalf of: American Orthopaedic Society for Sports Medicine Additional services and information for The American Journal of Sports Medicine can be found at: P<P Published online June 6, 2014 in advance of the print journal. Email Alerts: http://ajs.sagepub.com/cgi/alerts Subscriptions: http://ajs.sagepub.com/subscriptions Reprints: http://www.sagepub.com/journalsReprints.nav Permissions: http://www.sagepub.com/journalsPermissions.nav >> OnlineFirst Version of Record - Jun 6, 2014 What is This? Downloaded from ajs.sagepub.com by MATTHEW MILEWSKI on June 10, 2014 AJSM PreView, published on June 6, 2014 as doi:10.1177/0363546514535186 Osteochondral Autologous Transplantation Is Superior to Repeat Arthroscopy for the Treatment of Osteochondral Lesions of the Talus After Failed Primary Arthroscopic Treatment Hang Seob Yoon,* MD, Yoo Jung Park,y MD, Moses Lee,y MD, Woo Jin Choi,y MD, PhD, and Jin Woo Lee,yz MD, PhD Investigation performed at Yonsei University College of Medicine, Seoul, Korea Background: Several studies have reported on the outcome of arthroscopic treatment or osteochondral autologous transplantation (OAT) for osteochondral lesions of the talus (OLT), with mixed results. None of these studies has compared the results of repeat arthroscopy and OAT after failed primary arthroscopic treatment. Purpose: To compare the outcomes of OAT and repeat arthroscopy for the treatment of OLT after primary arthroscopy Study Design: Cohort study; Level of evidence, 3. Methods: This study included 22 patients who underwent OAT (group A) and 22 patients who underwent repeat arthroscopy (group B) after failed treatment of OLT among 399 patients who received primary arthroscopic marrow stimulation at single institution between 2001 and 2009. All patients were evaluated clinically using the visual analog scale (VAS) for pain and American Orthopaedic Foot and Ankle Society (AOFAS) Ankle Hindfoot Scale. The cumulative success rates were compared by use of Kaplan-Meier life table analysis. Results: The patients’ demographic and clinical characteristics and indications for surgery were comparable between the groups. Both groups showed significantly improved (P \ .001) VAS and AOFAS scores 6 months after surgery. However, group B showed significant deterioration over a mean follow-up period of 50 months. Overall, 18 of 22 (81.8%) patients in group A and 7 of 22 (31.8%) patients in group B achieved an excellent or good (80) AOFAS score (P \ .001). No patient in group A and 14 of 22 (63.6%) in group B required further revisions. Conclusion: Osteochondral autologous transplantation was significantly superior to repeat arthroscopic treatment of OLT after a mean follow-up period of 48 months. Therefore, repeat arthroscopy should be used judiciously for the treatment of OLT after failed arthroscopic treatment. Keywords: ankle; osteochondral lesion; osteochondral autologous transplantation; repeat arthroscopy generally poor regenerative capacity and may be unable to self-repair depending on the size of the defect, its depth and location, and the patient’s age.13,25 When nonoperative treatment is unsuccessful, patients with symptomatic OLT may be treated by various surgical methods such as arthroscopic marrow stimulation techniques, osteochondral autologous transplantation (OAT), autologous chondrocyte implantation (ACI), and frozen osteochondral allograft.9,11,14 Arthroscopic marrow stimulation techniques, including debridement, microfracture, anterograde drilling, and retrograde drilling, have been the preferred initial surgical option for most OTL. Long-term follow-up has revealed good to excellent results for arthroscopic procedures in 65% to 90% of patients.2,4-6,28,34,36,38 However, several recent studies have reported less favorable outcomes of arthroscopic treatment in large and uncontained An osteochondral lesion of the talus (OLT) involves the talar articular cartilage and adjacent subchondral bone. Articular cartilage damaged by trauma or disease has z Address correspondence to Jin Woo Lee, MD, PhD, Department of Orthopaedic Surgery, Yonsei University College of Medicine, 50 Yonseiro, Seodaemun-gu, Seoul 120-752, Korea (e-mail: ljwos@yuhs.ac). *Department of Orthopaedic Surgery, Wooridul Hospital, Seoul, Korea. y Department of Orthopaedic Surgery, Yonsei University College of Medicine, Seoul, Korea. The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. The American Journal of Sports Medicine, Vol. XX, No. X DOI: 10.1177/0363546514535186 Ó 2014 The Author(s) 1 Downloaded from ajs.sagepub.com by MATTHEW MILEWSKI on June 10, 2014 2 Yoon et al The American Journal of Sports Medicine defects.4,6,7 Consequently, surgeons increasingly face the challenge of determining the most appropriate second-line surgical treatment strategy. Data are available from randomized studies comparing arthroscopic treatment with OAT for OLT and from more recent studies comparing arthroscopic treatment with ACI for cartilage defects of the knee.15,24 However, these studies have generally excluded patients previously treated arthroscopically, thus obscuring the relative efficacies of OAT and repeat arthroscopy in patients in whom previous arthroscopic treatment has failed. In a review of osteochondral lesions in the knee, osteochondral lesions for which prior microfracture therapy failed displayed subchondral changes such as a stiff and thickened subchondral plate, osseous overgrowth, and the formation of subchondral cysts.27,29 In the absence of similar studies evaluating OLT, these findings in the knee may provide useful and compelling information for clinical decision making in the treatment of ankle lesions because repeat arthroscopy has been associated with worse clinical outcomes due to these subchondral changes.27,29 Osteochondral autologous transplantation is a procedure in which viable hyaline cartilage and its underlying subchondral bone are harvested from the ipsilateral knee and transplanted to the site of the defect in the talus.11,14,30 This procedure has been used to treat large and cystic osteochondral lesions or after failed index surgery. Although OAT restores normal hyaline cartilage, it does have disadvantages, including considerable donor site morbidity, the formation of subchondral bone cysts, poor healing potential of the cartilage interface of the graft, the need for complex rehabilitation, and a long recovery time.30,37 No previously published study has compared the results of repeat arthroscopic treatment and OAT after failed arthroscopic treatment for OLT. The first aim of this study was to compare OAT with repeat arthroscopy for the treatment of OLT after failed primary arthroscopic treatment. The second aim was to evaluate the hypothesis that OAT is superior to arthroscopy in cases in which other modalities have failed. MATERIALS AND METHODS This study included 22 patients who underwent OAT (group A) and 22 patients who underwent repeat arthroscopy (group B) after failed treatment of OLT among 399 patients who received arthroscopic marrow stimulation at a single center between 2001 and 2009. All patients were informed of the potential risks, including nonunion of the osteotomy site and donor site morbidity after OAT, and of the benefits and possible complications of repeat arthroscopy. Selection of repeat arthroscopy versus OAT was made without any preference on the part of the clinician and was decided through discussion with the patient. The patients who elected to undergo repeat arthroscopy for failed OLT did so because they did not want to undergo surgery as aggressive as OAT. All arthroscopic and repeat surgical procedures were performed by the senior surgeon (J.W.L.). Institutional review board approval was obtained, and all patients provided informed consent. Inclusion and Exclusion Criteria The inclusion criteria were joint stability, absence of extensive joint degeneration (defined as radiographic changes of grade 2 or higher according to the grading system of Kellgren and Lawrence22), and osteochondral lesions for which previous arthroscopic treatment had not been successful. Patients with diffuse arthritic changes of the ankle joint on plain radiographs or diffuse fibrillated articular cartilage on arthroscopic examination of repeat surgery and those with axial malalignment or chronic ankle instability were excluded, as were those with OLT that had not been previously treated arthroscopically. Forty-eight consecutive patients who failed primary arthroscopic marrow stimulation underwent revision surgery during the study period. Of these 48 patients, 22 underwent OAT and 26 underwent repeat arthroscopy. Of the 26 patients who underwent repeat arthroscopy patients, 1 patient had chronic lateral ankle instability and 3 patients exhibited diffuse cartilage fibrillation considered as osteoarthritis on the talus in secondary arthroscopy. These 4 patients were excluded from this study. None of the patients were lost to follow-up during the study periods. All patients had previously undergone surgery on the same ankle, 22 for arthroscopic microfracture (13 in group A and 9 in group B) and 22 for removal of a loose osteochondral fragment and abrasion arthroplasty (9 in group A and 13 in group B). Clinical Analysis and Outcome Criteria All outcome assessments were collected by a blinded and independent examiner who was not involved in the clinical and surgical management of the patients. The clinical outcomes of all patients were analyzed using the visual analog scale (VAS) for pain and the American Orthopaedic Foot and Ankle Society (AOFAS) Ankle Hindfoot Scale.23 All patients were evaluated before operation and were reviewed after 6, 12, and 24 months and then yearly thereafter. The overall clinical results were categorized according to the criteria suggested by other clinical studies using the AOFAS score (excellent, 90-100; good, 80-89; fair, 70-79; and poor, \70).5,6,28,33 Treatment failure was defined as persistent or recurrent symptoms, additional surgical treatment, or an AOFAS score lower than 80.5,6,33 The time to treatment failure was the time between the end of the primary surgical procedure and the date of repeat intervention. At the time of our initial examination, standard radiography and magnetic resonance imaging (MRI) were performed on all 44 patients and revealed no arthritic changes in any patient in either group. The size of each OLT was measured from the preoperative MRI as described in a previous study (calculated from the coronal and sagittal length using the ellipse formula),6 and the lesion was classified as small (\150 mm2) or large (150 mm2). To avoid potential bias, an independent observer who was not involved in the care of the patients and was blinded to the intention of this study evaluated the MRIs. Downloaded from ajs.sagepub.com by MATTHEW MILEWSKI on June 10, 2014 Vol. XX, No. X, XXXX OLT After Failed Primary Arthroscopic Treatment 3 Figure 1. (A) Primary arthroscopic debridement and abrasion of a full-thickness articular cartilage defect in the medial dome of the talus. (B) Repeat arthroscopy 3 years after primary treatment showed surface irregularity with fibrillation that clearly differs from the surrounding normal articular cartilage. Figure 2. Osteochondral autologous transplantation (OAT) via osteotomy of the medial malleolus. (A) An area of fibrocartilage that was of poor quality, partially loose, and not fully healed after primary arthroscopic treatment in the medial dome of the talus. (B) After the removal of fibrotic tissue, the defect was filled with an osteochondral plug 10 mm in diameter that was harvested from the nonweightbearing zone of the lateral femoral condyle. Surgical Technique Repeat Arthroscopic Marrow Stimulation Procedure. Primary and repeat arthroscopies were performed by the senior author using identical techniques. We used only 2 anterior portals (anteromedial and anterolateral) for the arthroscope and working instrument. Noninvasive traction (15 pounds) was applied by use of a foot strap to provide gentle ankle distraction. First, the joint was examined arthroscopically by use of previous arthroscopic portals. No filling of the defect with fibrocartilage or loosening of the reparative fibrocartilage from the defect site was found in any of the 22 patients, and 4 patients had total degeneration of the microfracture area (Figure 1). This was removed with a ring-shaped or curved curette and a power shaver with a small blade. After this preparation of the lesion, multiple holes were made in the exposed subchondral bone plate by use of an arthroscopic awl. In areas affected by loss of subchondral bone, abrasion arthroplasty was performed by trimming the damaged cartilage with a power shaver to create a smooth, stable articular surface. Once the microfracture or abrasion arthroplasty was completed, the tourniquet was released to visualize the release of fat droplets and blood from the microfracture holes into the ankle. Additional arthroscopic findings included soft tissue impingement with a fibrotic scar in 12 patients (54.5%) and loose body in 9 patients (40.9%). We treated these lesions with arthroscopic debridement and bone Downloaded from ajs.sagepub.com by MATTHEW MILEWSKI on June 10, 2014 4 Yoon et al The American Journal of Sports Medicine TABLE 1 Demographic and Clinical Characteristics: Osteochondral Autologous Transplantation (Group A) Versus Repeat Arthroscopy (Group B)a Characteristic Group A (n = 22) Mean age, y Age 35 y Male Body mass index, kg/m2 Duration of symptoms, mo History of trauma Type of defect Contained Uncontained Mean defect size, mm2 \150 mm2 150 mm2 Location of defect Medial/lateral Anterior/middle/posterior Arthroscopic procedure Microfracture Abrasion arthroplasty Group B (n = 22) 37.1 11 15 25.6 59.9 12 6 13.6 (50) (68) 6 3.0 6 39.3 (55) 41.6 15 18 25.3 82.2 14 6 13.2 (68) (82) 6 3.0 6 44.6 (64) 3 19 152.9 14 8 (14) (86) 6 76.5 (64) (36) 3 19 138.5 15 7 (14) (86) 6 60.0 (68) (32) 19/3 (86/14) 3/10/9 (14/45/41) 18/4 (82/18) 6/8/8 (27/36/36) 13 (59) 9 (31) P .234 .220 .296 .622 .104 .833 .668 .760 .750 .680 .527 .183 9 (41) 13 (59) a The age, body mass index, duration of symptoms, and defect size are given as the mean 6 standard deviation and compared between the groups by use of the Mann-Whitney U test. The categorical variables are presented as the number (%) of patients and compared between the groups using the Pearson x2 test. TABLE 2 Type of Intra-Articular Lesions in Both Groupsa Group A (n = 22) Group B (n = 22) Pb Subchondral cyst Tibial chondral lesion Soft tissue impingement Ossicle Loose body 13 1 12 4 9 (59) (5) (55) (18) (41) 14(64) 3 (14) 14 (64) 0 (0) 10 (45) .760 .300 .544 .038 .764 a Values are expressed as n (%). Mann-Whitney U test. b marrow stimulation. After surgery, the patients were restricted to partial weightbearing for 4 weeks and were prescribed physical therapy for range of motion and strengthening. No impact activities were allowed for a minimum of 12 weeks. Osteochondral Autologous Transplantation. After arthroscopic inspection and debridement of the ankle joint, the lesion was approached through a small longitudinal incision in the joint capsule. Remnants of residual fibrotic tissue were removed from the subchondral bone of the defect. The osteochondral grafts (6 and 8 mm) were harvested from the nonweightbearing zone of the lateral femoral condyle using a special chisel (OATS; Arthrex, Naples, Florida, USA). The recipient lesions were debrided and prepared for the grafts. The donor cylinders were implanted by use of a press-fit technique (Figure 2). A mean of 2.1 osteochondral plugs (range, 1-3 plugs) were used in each patient. In patients with medial OLT, osteotomy of the medial malleolus was necessary for appropriate exposure of the talus lesion. For osteotomy of the medial ankle, 4 drill holes were made and oblique osteotomy was performed at the transition between the pilon and the medial malleolar joint surface. After OAT, the medial ankle was fixed with four 4.0-mm screws. Postoperatively, passive exercise of the ankle with limited range of motion and active isometric training were initiated immediately. Toe-touch ambulation with crutches was permitted, and physical therapy was prescribed. Gradual progression from partial to full weightbearing activity was allowed beginning 6 weeks after surgery after follow-up radiographs confirmed good incorporation of the osteochondral graft.16,26 Statistical Analysis The clinical data were compared using the nonparametric Wilcoxon signed rank test for paired samples (preoperative and postoperative scores). Differences between groups were analyzed using the Mann-Whitney U test for continuous variables and the chi-square test or Fisher’s exact test (used when the expected frequency count in a cell was \5), as appropriate, for categorical variables. Bivariate analysis was performed using Spearman’s correlation coefficient for correlations between preoperative variables (age, sex, body mass index [BMI], symptom duration, time interval between the procedures, type of defect, and defect size) and all final clinical outcomes. The estimated probabilities of clinical failure were calculated using the Kaplan-Meier method.21 A P value less than .05 was considered indicative of significance. The data were analyzed using the Statistical Package for Social Sciences (v 18.0; SPSS Inc, Chicago, Illinois, USA). Downloaded from ajs.sagepub.com by MATTHEW MILEWSKI on June 10, 2014 Vol. XX, No. X, XXXX OLT After Failed Primary Arthroscopic Treatment TABLE 3 Comparison of Clinical Outcomes Between the Osteochondral Autograft Transplantation (Group A) and Repeat Arthroscopic Treatment (Group B)a TABLE 4 Correlations Between Preoperative Variables and Clinical Outcome Group A (n = 22) Group A (n = 22) VAS score, mean 6 SD Preoperative 6 months 12 months 24 months Last follow-up AOFAS score, mean 6 SD Preoperative 6 months 12 months 24 months Last follow-up Clinical outcome at last follow-up, No. (%)1-3,b Excellent Good Fair Poor Group B (n = 22) P 6.14 2.95 2.45 1.95 1.91 6 6 6 6 6 1.32 1.09 1.14 0.89 1.54 5.86 3.18 2.68 3.41 5.27 6 6 6 6 6 1.55 .708 1.05 .508 0.84 .324 1.22 \.001 1.72 \.001 50.40 82.81 86.22 85.90 85.27 6 6 6 6 6 7.66 6.58 5.56 4.15 5.75 50.41 83.73 79.77 71.77 69.64 6 6 6 6 6 11.40 .144 2.65 .056 4.09 \.001 10.00 \.001 10.59 \.001 \.001 6 (27.3) 12 (54.5) 4 (18.2) 0 0 7 (31.8) 5 (22.7) 10 (45.5) a Boldface type indicates statistical significance (P \ .05). AOFAS, American Orthopaedic Foot and Ankle Society Ankle Hindfoot Scale; SD, standard deviation; VAS, visual analog scale. b Clinical results at final follow-up were graded according to the AOFAS scores (excellent; 90-100, good; 80-89, fair; 70-79, and poor; \70). 5 Age Male sex Body mass index Duration of symptoms Time interval between the procedures Type of defect (uncontained) Defect size Spearman Correlation Coefficient Group B (n = 22) P Spearman Correlation Coefficient P –0.325 0.224 0.086 0.091 0.131 .140 .159 .702 .425 .641 0.085 0.329 –0.085 0.525 –0.223 .706 .621 .708 .411 .317 –0.082 .095 –0.052 .059 0.417 .053 –0.462 .030 RESULTS Baseline Characteristics The 2 groups did not differ significantly in age, gender ratio, BMI, duration of symptoms, defect size, or primary arthroscopic procedure (all P . .05) (Table 1). The mean duration of follow-up was 48 months overall, 45 months (range, 24-101 months) in group A and 50 months (range, 24-116 months) in group B. Comparison of the primary arthroscopic data showed that the groups were similar with respect to the types, sizes, and grades of their lesions. Overall, the cartilage defects of patients in this study were predominantly large (mean total defect size, 152.9 mm2 in group A and 138.5 mm2 in group B) and full thickness (Ferkel and Cheng10 staging system, grades D-F) and were located mainly on the medial talar dome. The groups had similar proportions of associated intra-articular lesions, including subchondral cysts, tibial chondral lesions, soft tissue impingement, ossicles, and loose bodies (P . .05) (Table 2). Clinical Outcomes Figure 3. Kaplan-Meier survival curve showing the cumulative rate of clinical failure in patients treated with osteochondral autologous transplantation (OAT) versus repeat arthroscopy. Patients treated with repeat arthroscopy showed significantly greater clinical failure (defined as persistent pain or recurrent symptoms, additional surgical treatment, or AOFAS score \80) than did those treated with OAT (P \ .001) Both groups demonstrated significant clinical improvement (P \ .05) after 1 year, and comparison of the clinical outcome criteria5,6,28,33 showed that the AOFAS scores were excellent or good (80) in 19 of 22 (86.4%) patients in group A versus 12 of 22 (54.5%) in group B (P = .021). Group B showed significant deterioration at the 1-year follow-up assessment but had still achieved significant clinical improvement relative to the patients’ preoperative evaluations (P \ .001). As of the last follow-up, 18 of 22 (81.8%) patients in group A but only 7 of 22 (31.8%) in group B maintained excellent or good results (P \ .001) (Table 3). The pattern of lower postoperative AOFAS scores in the patients treated with repeat arthroscopy persisted, and the cumulative clinical failure rate was significantly higher in the patients treated with repeat arthroscopy compared with those treated with OAT Downloaded from ajs.sagepub.com by MATTHEW MILEWSKI on June 10, 2014 6 Yoon et al The American Journal of Sports Medicine (P \ .001) (Figure 3). Similar trends were also observed for the VAS score. In group A, 4 patients reported continued ankle pain and swelling even after appropriate rehabilitation and were not completely satisfied with the statuses of their ankles. Therefore, we performed second-look arthroscopy in each of these patients at a mean of 21.4 months (range, 14-36 months) after their index operations. The second-look arthroscopies revealed fibrillation of the graft surface and soft tissue between the grafts on probing relative to the surrounding cartilage, which required debridement. Six months after debridement and chondroplasty, these patients were painfree and began engaging in sports activities. In group B, 14 of 15 patients with failure underwent revision OAT. The single patient who experienced clinical failure but refused to undergo more aggressive surgery was managed with nonsurgical measures, including rest, immobilization, anti-inflammatory medication, and physical therapy. We attempted to identify factors associated with the final results in both groups but found no associations between several preoperative variables and clinical outcomes as of the last follow-up evaluation in group A (Table 4). In group B, poorer clinical outcomes were associated with patients who had larger defect (r = –0.462, P = .030). In group A, the rate of clinical failure was higher in patients with large defects (25.0%, 2/8) than in those with small defects (14.3%, 2/14). However, this difference did not reach statistical significance (P = .393). In group B, clinical failure occurred within 50 months in 8 of 15 patients (53.3%) with small defects versus in all (100%, 7/7) of the patients with large defects (P \ .001). In group A, 4 of 22 (18%) patients and 2 of 22 (9%) patients reported mild knee pain and crepitation, respectively. These complaints resolved successfully within 3 months of nonoperative treatment. One patient developed a superficial wound infection, which had resolved after oral antibiotic therapy. In group B, there were no intraoperative or perioperative complications, including wound infection and neural injury. DISCUSSION A number of promising surgical interventions for OLT have been established in recent years. These can be either reparative, as are marrow stimulation techniques, or restorative, for which OAT and ACI have become wellestablished techniques.11,37 The clinical results and outcomes of reparative and restorative techniques have been carefully investigated, and various predictors and factors influencing the success rates of these techniques have been established. Several authorities advocate the preferential use of arthroscopic treatment in patients with OLT, claiming good clinical results equal to those of cartilage replantation techniques such as OAT and ACI.7,14,33 In our study, 88% of 399 patients who underwent primary arthroscopic marrow stimulation did not require revision surgery. Our results are consistent with those reported by Choi et al,6 who found that 8 of 120 ankles (6.7%) required revision surgery after arthroscopic marrow stimulation, with good to excellent results in 81.6% ankles at the average 35.6 months follow-up. Lee et al,28 in a study of 20 ankles treated with arthroscopic treatment, reported that overall 90% of ankles achieved good to excellent results. Therefore, arthroscopic marrow stimulation is currently the primary technique used to treat symptomatic OLT. Arthroscopic treatment has been reported to provide effective improvement in ankle function when used to treat small OLT, but favorable long-term results have been less predictable for large OLT.1,12 In cases in which primary arthroscopic treatment fails, the decision of which subsequent technique to choose has become increasingly difficult, as such patients may be unlikely to have good clinical outcomes irrespective of the surgical technique used. In the last 10 to 15 years, there have been many attempts to identify the most appropriate method for treating lesions in which primary arthroscopy has failed. The techniques examined have included repeat arthroscopy, open reconstructive procedures including OAT, ACI, and structural osteochondral allograft.16,20,26,32,37 Kreuz et al26 used OAT to treat recurrent OLT after failed primary arthroscopic treatment and achieved good clinical results. Savva et al32 reported that repeat arthroscopic debridement is an acceptable option for treatment of small to medium-sized OLT for which primary debridement failed. However, there have been no studies comparing OAT and repeat arthroscopy, and only level 4 studies for each technique are available in the literature.16,17,31,32,39 The present study is, to our knowledge, the first to compare OAT with repeat arthroscopy for treatment of OLT in which prior arthroscopic treatment failed. We have shown that both OAT and repeat arthroscopy give encouraging clinical results for the first year of follow-up but that OAT is significantly superior to repeat arthroscopy after follow-up for a mean of 4 years. The size of the OLT influences the choice and results of its treatment. Arthroscopic marrow stimulation procedures have been proposed as an easy, rapid, and inexpensive way to restore cartilage injuries, but these procedures may restore cartilage defects by inducing the formation of fibrocartilage. For smaller lesions, this substitution of fibrocartilage may suffice; however, for larger lesions, fibrocartilage may not be adequate for longevity of the joint.6,7,14 In contrast, several studies have suggested that the results of OAT remain more durable over the long term, especially in large OLT, because of the ability of OAT to provide mechanically stable hyaline cartilage.9,11,14,16,18 When size-dependent repair is discussed in the literature, OAT is generally recommended for larger cartilage defects.9,14 Hangody et al19 reported the treatment of 36 patients with osteochondral defects larger than 10 mm using OAT and achieved excellent results in 34 patients (94%) after a mean follow-up period of 4.2 years. The cited reports are in agreement with our finding. In our study, the size of the osteochondral lesions was comparable between the groups. One of the notable features of the present study is that we analyzed the clinical outcomes relative to the preoperative variables and were thus able to show that the size of the cartilage defect was the strongest predictor of poor Downloaded from ajs.sagepub.com by MATTHEW MILEWSKI on June 10, 2014 Vol. XX, No. X, XXXX OLT After Failed Primary Arthroscopic Treatment clinical outcome in group B but did not affect the clinical results in group A. Among patients with larger osteochondral defects (150 mm2), only 2 of 8 (25.0%) in group A versus all (100%, 7/7) in group B exhibited clinical failure. The higher failure rate of repeat arthroscopy for treatment of large osteochondral defects could account in part for the major difference in clinical outcomes between the OAT group and the repeat arthroscopy group. The prognostic significance of the containment of OLT has recently garnered renewed attention in the field of arthroscopic marrow stimulation treatment.4,8 Intact cartilage walls provide an enclosed space in which marrow clot can form; however, the ‘‘superclot’’ that facilitates fibrocartilage formation might not form in uncontained lesions.29 Choi et al4 found that patients with uncontained OLT had substantially worse clinical results than those with contained OLT after follow-up for 74 months. Although the containment of the OLT has not been reported to affect the clinical outcome after OAT, OAT with perpendicular access can be used to reconstruct the articular surface of the talar dome.9 Most of the patients in our present series had uncontained OLT, which may have contributed to the difference in long-term results between the 2 groups. As our understanding of its underlying pathophysiological process has increased, osteoarthritis has come to be considered a disease of the entire osteochondral unit rather than being limited to the articular cartilage.3 In a review of osteochondral lesions in the knee, osteochondral lesions for which microfracture therapy failed resembled chronic chondral lesions and displayed subchondral changes such as a stiff and thickened subchondral plate, osseous overgrowth, and the formation of subchondral cysts.27,29 In the absence of similar studies evaluating arthroscopic treatment of the talus, these previous studies of the knee indicate that changes of the osteochondral unit may provide useful insight into the limitations of repeat arthroscopic treatment.27,29 The alteration to the osteochondral unit can be theorized to be responsible for the worse outcomes after repeat arthroscopy versus OAT because the latter replaces the cartilage lesions with an intact and integrated bone–hyaline cartilage unit loaded with viable cells. Osteochondral autologous transplantation has become an accepted surgical procedure for the treatment of OTL of large size9 and those associated with expansive subchondral cysts.35 However, clinical outcomes and success rates of OAT as a revision technique after failure of marrow stimulation in the same location remain controversial. Imhoff et al20 found that patients in whom OAT was the second surgical procedure after arthroscopic drilling for a talar defect had worse clinical outcomes than did those in whom OAT was the first surgical procedure. In contrast, Haasper et al16 reported equally favorable outcomes in patients undergoing secondary OAT relative to patients undergoing primary OAT after follow-up for a median of 24 months. Kreuz et al26 described good clinical outcomes after a mean follow-up period of 49 months in their 35 patients treated with OAT after failed primary arthroscopic management. Despite the general baseline severity of the lesions treated with OAT in the present study, 81.8% of the patients had excellent or good AOFAS scores 7 (80 points) after follow-up for a mean of 45 months. Although our study did not examine primary OAT and therefore cannot determine whether the results of revision OAT after failed arthroscopic microfracture are better or worse, it does demonstrate that OAT is an effective option for the treatment of symptomatic OLT in which arthroscopic treatment has failed. The limitations of our study include its retrospective nonrandomized nature, although we did use data gathered preoperatively. We also examined a relatively small number of patients, which limits our statistical power. Furthermore, it remains questionable whether the AOFAS score is the best evaluation to assess the clinical outcome for the treatment of OLT. However, given that no previously published study has compared the results of repeat arthroscopic treatment with those of OAT for the treatment of OLT for which primary arthroscopic treatment has failed, we believe that our data may aid orthopaedic surgeons in the selection of the most appropriate revision technique in such cases. Arthroscopic treatment plays an important role in the treatment of OLT. However, the management of OLT in which arthroscopic treatment has failed is challenging given the poor potential of these lesions for healing. In our study, OAT showed significant superiority over repeat arthroscopic treatment of OLT in the ankle after follow-up for a mean of 48 months. Therefore, repeat arthroscopy should be used judiciously for the treatment of OLT in which arthroscopic treatment has failed. REFERENCES 1. Angermann P, Jensen P. Osteochondritis dissecans of the talus: long-term results of surgical treatment. Foot Ankle. 1989;10:161-163. 2. Barnes CJ, Ferkel RD. Arthroscopic debridement and drilling of osteochondral lesions of the talus. Foot Ankle Clin. 2003;8:243-257. 3. Brandt KD, Radin EL, Dieppe PA, van de Putte L. Yet more evidence that osteoarthritis is not a cartilage disease. Ann Rheum Dis. 2006;65:1261-1264. 4. Choi WJ, Choi GW, Kim JS, Lee JW. Prognostic significance of the containment and location of osteochondral lesions of the talus: independent adverse outcomes associated with uncontained lesions of the talar shoulder. Am J Sports Med. 2013;41:126-133. 5. Choi WJ, Kim BS, Lee JW. Osteochondral lesion of the talus: could age be an indication for arthroscopic treatment? Am J Sports Med. 2012;40:419-424. 6. Choi WJ, Park KK, Kim BS, Lee JW. Osteochondral lesion of the talus: is there a critical defect size for poor outcome? Am J Sports Med. 2009;37:1974-1980. 7. Chuckpaiwong B, Berkson EM, Theodore GH. Microfracture for osteochondral lesions of the ankle: outcome analysis and outcome predictors of 105 cases. Arthroscopy. 2008;24:106-112. 8. Cuttica DJ, Smith WB, Hyer CF, Philbin TM, Berlet GC. Osteochondral lesions of the talus: predictors of clinical outcome. Foot Ankle Int. 2011;32:1045-1051. 9. Easley ME, Latt LD, Santangelo JR, Merian-Genast M, Nunley JA. Surgical techniques: osteochondral lesions of the talus. J Am Acad Orthop Surg. 2010;18:616-630. 10. Ferkel RD, Cheng JC. Ankle and subtalar arthroscopy. In: Kelikian A, ed. Operative Treatment of the Foot and Ankle. New York: Appleton-Croft; 1999:321-350. 11. Ferkel RD, Scranton PE Jr, Stone JW, Kern BS. Surgical treatment of osteochondral lesions of the talus. Instr Course Lect. 2010;59:387-404. Downloaded from ajs.sagepub.com by MATTHEW MILEWSKI on June 10, 2014 8 Yoon et al The American Journal of Sports Medicine 12. Ferkel RD, Zanotti RM, Komenda GA, et al. Arthroscopic treatment of chronic osteochondral lesions of the talus: long-term results. Am J Sports Med. 2008;36:1750-1762. 13. Giannini S, Buda R, Faldini C, et al. Surgical treatment of osteochondral lesions of the talus in young active patients. J Bone Joint Surg Am. 2005;87(suppl 2):28-41. 14. Giannini S, Vannini F. Operative treatment of osteochondral lesions of the talar dome: current concepts review. Foot Ankle Int. 2004;25:168-175. 15. Gobbi A, Francisco RA, Lubowitz JH, Allegra F, Canata G. Osteochondral lesions of the talus: randomized controlled trial comparing chondroplasty, microfracture, and osteochondral autograft transplantation. Arthroscopy. 2006;22:1085-1092. 16. Haasper C, Zelle BA, Knobloch K, et al. No mid-term difference in mosaicplasty in previously treated versus previously untreated patients with osteochondral lesions of the talus. Arch Orthop Trauma Surg. 2008;128:499-504. 17. Hangody L. The mosaicplasty technique for osteochondral lesions of the talus. Foot Ankle Clin. 2003;8:259-273. 18. Hangody L, Fules P. Autologous osteochondral mosaicplasty for the treatment of full-thickness defects of weight-bearing joints: ten years of experimental and clinical experience. J Bone Joint Surg Am. 2003;85(suppl 2):25-32. 19. Hangody L, Kish G, Modis L, et al. Mosaicplasty for the treatment of osteochondritis dissecans of the talus: two to seven year results in 36 patients. Foot Ankle Int. 2001;22:552-558. 20. Imhoff AB, Paul J, Ottinger B, et al. Osteochondral transplantation of the talus: long-term clinical and magnetic resonance imaging evaluation. Am J Sports Med. 2011;39:1487-1493. 21. Kaplan EL, Meier P. Non-parametric estimation from incomplete observation. J Am Stat Assoc. 1958;53:457-481. 22. Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957;16:494-502. 23. Kitaoka HB, Alexander I, Adelaar RS, Nunley JA, Myerson MS, Sanders M. Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int. 1994;15:349-353. 24. Knutsen G, Engebretsen L, Ludvigsen TC, et al. Autologous chondrocyte implantation compared with microfracture in the knee: a randomized trial. J Bone Joint Surg Am. 2004;86:455-464. 25. Kono M, Takao M, Naito K, Uchio Y, Ochi M. Retrograde drilling for osteochondral lesions of the talar dome. Am J Sports Med. 2006;34:1450-1456. 26. Kreuz PC, Steinwachs M, Erggelet C, Lahm A, Henle P, Niemeyer P. Mosaicplasty with autogenous talar autograft for osteochondral lesions 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. of the talus after failed primary arthroscopic management: a prospective study with a 4-year follow-up. Am J Sports Med. 2006;34:55-63. Kreuz PC, Steinwachs MR, Erggelet C, et al. Results after microfracture of full-thickness chondral defects in different compartments in the knee. Osteoarthritis Cartilage. 2006;14:1119-1125. Lee KB, Bai LB, Yoon TR, Jung ST, Seon JK. Second-look arthroscopic findings and clinical outcomes after microfracture for osteochondral lesions of the talus. Am J Sports Med. 2009;37(suppl 1):63S-70S. Mithoefer K, Williams RJ III, Warren RF, et al. The microfracture technique for the treatment of articular cartilage lesions in the knee: a prospective cohort study. J Bone Joint Surg Am. 2005;87:1911-1920. Murawski CD, Foo LF, Kennedy JG. A review of arthroscopic bone marrow stimulation techniques of the talus: the good, the bad, and the causes for concern. Cartilage. 2010;1:137-144. Ogilvie-Harris DJ, Sarrosa EA. Arthroscopic treatment after previous failed open surgery for osteochondritis dissecans of the talus. Arthroscopy. 1999;15:809-812. Savva N, Jabur M, Davies M, Saxby T. Osteochondral lesions of the talus: results of repeat arthroscopic debridement. Foot Ankle Int. 2007;28:669-673. Saxena A, Eakin C. Articular talar injuries in athletes: results of microfracture and autologous bone graft. Am J Sport Med. 2007;35:16801687. Schuman L, Struijs PA, van Dijk CN. Arthroscopic treatment for osteochondral defects of the talus: results at follow-up at 2 to 11 years. J Bone Joint Surg Br. 2002;84:364-368. Scranton PE Jr, Frey CC, Feder KS. Outcome of osteochondral autograft transplantation for type-V cystic osteochondral lesions of the talus. J Bone Joint Surg Br. 2006;88:614-619. Tol JL, Struijs PA, Bossuyt PM, Verhagen RA, van Dijk CN. Treatment strategies in osteochondral defects of the talar dome: a systematic review. Foot Ankle Int. 2000;21:119-126. Valderrabano V, Leumann A, Rasch H, Egelhof T, Hintermann B, Pagenstert G. Knee-to-ankle mosaicplasty for the treatment of osteochondral lesions of the ankle joint. Am J Sports Med. 2009;37(suppl 1):105S-111S. van Bergen CJ, Kox LS, Maas M, Sierevelt IN, Kerkhoffs GM, van Dijk CN. Arthroscopic treatment of osteochondral defects of the talus: outcomes at eight to twenty years of follow-up. J Bone Joint Surg Am. 2013;95:519-525. van Bergen CJ, Tuijthof GJ, Sierevelt IN, van Dijk CN. Direction of the oblique medial malleolar osteotomy for exposure of the talus. Arch Orthop Trauma Surg. 2011;131:893-901. For reprints and permission queries, please visit SAGE’s Web site at http://www.sagepub.com/journalsPermissions.nav Downloaded from ajs.sagepub.com by MATTHEW MILEWSKI on June 10, 2014