S-T AND T-Q SEGMENT CHANGES DURING ISCHEMIA/Kleber et al.
Gesamt-Cholesterins im Serum. Z Klin Chem Klin Biochem 12: 403407, 1974
10. Eggstein M, Kreutz FH: Eine neue Bestimmung der Neutralfette im
Blutserum und Gewebe. Klin Wochenschr 44: 202-273, 1966
11. Morris JN, Adam C, Chave SPW, Sirey C, Epstein L: Vigorous
exercise in leisure time and the incidence of coronary heart disease.
Lancet 1: 333-339, 1973
12. Carlson LA, Bottiger LE: Ischaemic heart disease in relation to
fasting values of plasma triglycerides and cholesterol. Lancet 1: 865868, 1972
603
13. Heiberg A, Grieg A: Serum lipid and lipoprotein concentrations in a
Norwegian population sample. Acta Med Scand 196: 155-160, 1974
14. Aromaa A, Bjorksten F, Eriksson AW, Maatela J, Kirjarinta M,
Fellman J, Tamminen M: Serum cholesterol and triglyceride concentrations of Finns and Finnish Lapps. Acta Med Scand 198: 13-33,
1975
15. Dyerberg J, Hjorne N: Plasma lipid and lipoprotein levels in a Danish
population. Acta Med Scand 191: 413-421, 1972
16. Chong YH, Khoo KL: Serum lipid levels and the prevalence of
hyperlipidaemia in Malaysia. Clin Chim Acta 65: 143-148, 1975
Downloaded from http://circres.ahajournals.org/ by guest on October 1, 2016
Mechanism and Time Course of S-T and T-Q
Segment Changes during Acute Regional
Myocardial Ischemia in the Pig Heart Determined
by Extracellular and Intracellular Recordings
ANDRE G. KLEBER, MICHIEL J. JANSE, FRANS J.L.
VAN CAPELLE, AND DIRK DURRER
SUMMARY We recorded transmembrane potentials from subepicardial ventricular cells and local extracellular
DC electrograms in isolated perfused pig hearts before and after occlusion of the left anterior descending artery. The
first change was a decrease in the resting membrane potential, reflected by T-Q depression in the electrogram. After
3 minutes, action potentials shortened and their amplitude decreased, resulting in S-T elevation until, finally, cells in
the center of the ischemic zone became totally unresponsive at resting potentials of about —65 mV. This rendered
the extracellular complex monophasic. Determination of extracellular potential distribution at 150-250 epicardial
sites after 15-30 minutes of occlusion showed an increase of T-Q depression and S-T elevation toward a central area,
with maximum values of —15 and +35 mV, respectively. Comparison of amplitude and configuration of intramural
and epicardial potential profiles revealed that the potential distribution was homogeneous throughout ischemic parts
of the wall. Extracellular epicardial current originated, therefore, from the epicardial intracellular compartment.
Maximal current density during late systole was 1 /tA/mm 2 , flowing in the border zone towards normal myocardium.
After 1 hour of occlusion, there was a marked decrease of extracellular DC potentials which could be attributed to
transient recovery of electrical activity in the ischemic zone. After 2 hours, the zone of unresponsiveness was larger
than after 15 minutes of occlusion, and the overall amplitude of DC potentials had decreased further, possibly
because of healing over.
IN 1879, Burdon-Sanderson and Page1 described the
effects of injury to the surface of the frog heart and noted
that, during activity, the injured site became positive with
respect to the uninjured surface. Since then, many authors
have studied the effects of injury, including those of
ischemia, on local extracellular electrograms of the heart.
Gradually, it was established that S-T elevation as recorded with condenser-coupled amplifiers could be due to
both diastolic (T-Q) depression2':l and true S-T segment
elevation.:<~a The study of Samson and Scher9 provided
evidence that diastolic baseline depression in the extracellular electrogram was caused by loss of resting membrane
potential in ischemic cells, leading to a diastolic current of
From the Department of Cardiology and Clinical Physiology, University
Hospital Wilhelmina Gasthuis, Amsterdam, and the Interuniversity Cardiology Institute, Amsterdam, The Netherlands.
Supported by the Wynand M. Pon Foundation. Dr. A. G. Kleber
benefited from a grant of the "Schweizerische Stiftung ur MedizinischeBiologische Stipendien."
Address for reprints: Michiel J. Janse, M.D., Department of Cardiology
and Clinical Physiology, Wilhelmina Gasthuis, Eerste Helmersstraat 104,
Amsterdam, The Netherlands.
Received May 2, 1977; accepted for publication December 15, 1977.
injury between healthy cells and ischemic cells which
rendered the extracellular space in the ischemic area
negative with respect to the normal area. This was confirmed by the work of Prinzmetal et al.10 The mechanism
of S-T elevation, however, seems not quite as well established. Samson and Scher9 have stated that it is caused by
a shortening of the ischemic action potential. In the
absence of activation delay of the ischemic cells, a systolic
current of injury would be expected to flow between the
ischemic and normal areas, making the ischemic extracellular space positive with respect to the normal extracellular space. Samson and Scher found that "the injured area
produced near normal action potentials during depolarization" and they therefore stated that a lack of responsiveness in the injured area could not account for true S-T
elevation, as was originally suggested by the results of
Eyster et al.4 Recent studies from this laboratory" have
shown, however, that transmembrane action potentials
from ischemic cells can vary from "near normal" to
responses of very small amplitude, depending on localization and duration of ischemia.
604
CIRCULATION RESEARCH
Further knowledge of the relationship between transmembrane potentials and extracellular potentials in regional myocardial ischemia would be of help in interpreting results obtained by recording extracellular complexes.
Also, it would be interesting to obtain information about
the flow of injury current and its possible relationship to
the occurrence of ventricular arrhythmias. The purpose of
the present study was: (1) to measure the extracellular
potential distribution on the epicardium and at intramural
sites at different times after coronary artery occlusion and
to calculate from these data local current densities, and
(2) to compare the changes in extracellular potentials to
changes in transmembrane action potentials of the ischemic tissue.
Methods
Downloaded from http://circres.ahajournals.org/ by guest on October 1, 2016
Pigs weighing 20-25 kg were anesthetized by an intravenous injection of sodium pentobarbital (20 mg/kg). The
thorax was opened by a midsternal incision. Approximately 1 liter of venous blood was taken from the pig and
mixed with modified Tyrode's solution yielding 2 liters of
perfusion fluid. The heart was removed rapidly and fixed
to the perfusion setup where it was perfused according to
the Langendorff method. The exact description of the
perfusion system and the composition of the perfusion
fluid are given elsewhere."
The heart was driven above the spontaneous frequency
of the sinus node by bipolar stimuli applied by means of a
pair of electrodes fixed to the right atrium. Ischemia in
the anterior wall and the septum was produced by clamping the anterior descending branch of the left coronary
artery, usually proximal to the origin of the first diagonal
branch.
Determination of the Extracellular Potentials
Extracellular DC potentials were measured by means of
a cotton wick (diameter, 0.5 mm) which emerged from a
polyethylene tube filled with isotonic saline. The saline
was in contact with a chlorided silver wire that was
connected to a high input impedance buffer amplifier. A
DC amplifier with differential input measured the potential at this electrode with respect to a relative zero
reference potential recorded through a second wick electrode fixed to the aortic root.
Prior to and after a series of 10-20 recordings at
different sites, the measuring wick was brought into
contact with the aortic root to check the level of zero
potential. Whenever the control revealed a shift of more
than 1 mV, the data were rejected. Epicardial potentials
were determined consecutively at different sites on the
anterior part of the right and the left ventricles. The
following technique was applied to achieve reproducible
measurements at different intervals after the occlusion at
distinct sites on the epicardial surface. A thin rubber
membrane was perforated to obtain a grid of holes 0.7
mm in diameter. The distance between the holes varied in
different experiments from 2 to 5 mm. Each hole in the
grid was identified by a letter giving its vertical position
and by a number indicating its horizontal position. Prior
to occlusion of the left anterior descending artery, the
membrane was sutured tightly to the anterolateral part of
VOL.
42, No. 5,
MAY
1978
the heart, covering the presumed future ischemic area and
an additional zone of the left ventricular anterolateral
wall. Potentials were measured by touching the epicardial
tissue underlying a hole lightly with the cotton wick. Thus,
in a typical experiment, epicardial potentials from 150 to
250 sites could be recorded within 15 minutes. By this
method, two adjacent points were connected electrically
only by the extracellular bridge under the rubber membrane, and the area of myocardium accessible to the
measuring electrode was the same at each site.
A polyethylene tube (diameter, 0.7 mm) of about 10
cm in length through which a fine cotton wick was pulled
served as the intramural wick electrode. A tiny hole in its
wall at a variable distance from the sealed end allowed
electrical contact between the wick and the intramural
extracellular space. The tube was driven through the
ventricular wall from the epicardial surface. The free end
of the tube emerged from the left ventricular cavity and
the mitral orifice. Measurements were taken by touching
the free end of the tube with the movable wick electrode
described above. The level of the zero potential was
determined in the same way as for the epicardial sites.
Measurements of Transmembrane Potentials
To determine transmembrane potentials, floating glass
microelectrodes12 filled with 3 M KC1 with resistances of
20-30 Mfl were used, together with conventional high
input impedance buffer preamplifiers and differential DC
amplifiers. The microelectrodes were brought into contact
with the extracellular space by advancing them carefully
through the holes in the rubber membrane attached to the
epicardium. Impalements were performed with a hydraulic micromanipulator. A second microelectrode with
a broken tip positioned in the same hole served as
extracellular reference. The determination of the value of
resting membrane potential on withdrawal of a microelectrode proved to be difficult, because of the great flexibility
of the microelectrode tips. Therefore, values of resting
membrane potentials will not be given for all transmembrane potentials shown in the Results section. The outputs
of the differential amplifiers were connected to an Ampex
multichannel instrumentation tape recorder. Signals were
printed out on an Elema multichannel inkwriter.
In Situ Experiments
In three control experiments, DC extracellular electrograms were measured from in situ hearts. Holes in a
rubber membrane 5 mm apart served as epicardial sites of
measurement. Cotton wick electrodes inserted from the
epicardium into the left ventricular wall recorded extracellular DC electrograms at a distance of 5-6 mm from the
epicardium.
Construction of Isopotential Maps and Computation of
Extracellular Current Densities and Laplacian Maps
Amplitudes of DC potentials at fixed intervals of the
cardiac cycle (taking the atrial stimulus as zero time) were
measured by hand from signals printed out at a sensitivity
of 1 mV/mm. From these data, isopotential maps were
constructed by hand or by using a computer program. This
program calculates the potential by linear interpolation
S-T AND T-Q SEGMENT CHANGES DURING ISCHEMIA/Kleber et al.
Downloaded from http://circres.ahajournals.org/ by guest on October 1, 2016
from the four neighboring points on the grid. The extracellular potential gradients which appear after coronary
occlusion during the T-Q and S-T segments are caused by
the flow of injury current through the extracellular compartment. This current is generated by the instantaneous
difference in transmembrane potential in adjacent myocardial tissue. The assessment of the epicardial and transmural potential distribution allowed us to (1) calculate the
extracellular current flowing between two measuring sites
and (2) determine the sources of this current, i.e., determine the net current which, at a certain measuring site,
flows between the intracellular and extracellular compartment and is added to or subtracted from the extracellular
current flowing at this site.
The principle of the technique is outlined briefly as
follows. Consider a point in the grid of holes in the rubber
membrane which is not at the border of the grid, for
example, F7. It is surrounded by F6, F8, E7, and G7.
The current flowing from any of these points to F7 is
proportional to the voltage difference between F7 and the
point in question. For example, the current density j E m
from E7 to F7, at time, t, in the cardiac cycle will be:
1
- VK7)[A/m2]
(1)
where p = the resistivity of the extracellular compartment
of the tissue, L = the distance between the measuring
points, and VE7 and VH-7 = the extracellular potentials at
the sites E7 and F7 at time, t, of the cardiac cycle. Now
consider a small cube of the subepicardial tissue sheet
oriented in parallel to the grid lines in such a way that site
F7 is the center of its top. Let the length of the edges be
L, the distance between the sampling points. The amount
of current entering this cube through a lateral face will be
the product of the current density and the area of the face.
The total amount of current entering or leaving the cube
through the lateral faces will thus be given by:
Ip7 =
L
' ( j K 7 F 7 ~*~ JK7G7
"*" JF6K7 ~*~ jK7Fn)
Introducing Equation 1 and dividing by the volume of the
cube yields:
lK7
=
p-U
(VE7 + VG7 + VK6
4VK7) [A/m 3 ]
(2)
where i is a scalar quantity representing an extra current
which cannot be accounted for by the two-dimensional
extracellular potential field measured on the grid. Indeed,
as long as the sheet of epicardial tissue behaves as a simple
passive resistance network, the total current flow to site
F7 is zero. This is equivalent to the condition that the
potential of the central point equals the numerical average
of the neighboring points. Exactly the same amount of
current then is flowing toward the central point as is
flowing away from it. As soon as iF7 in Equation 1 is not
zero, net current must either have been added to or
subtracted from the extracellular tissue at site F7. Two
biological explanations can be given in this case: (1) a
transmembrane current flowing locally between intra- and
extracellular compartments and (2) an extracellular current flowing between the epicardial and the underlying
605
intramural layer. As will be shown in the Results section,
during ischemia no important transmural gradients occurred in our experiments. Therefore, iF7 is the current
per unit volume of tissue flowing through the cell membranes at site F7. The term iK7 > 0 defines F7 as a current
source; iF7 < 0 defines F7 as a current sink. Equation 2 is
the discrete counterpart of the well known electroconduction field equation
i = div j = — • -AV,
P
where A represents the Laplacian operator. The current
source strength can be calculated for all the points on the
grid except those situated at the border and presented on
a map. For this map, the term "Laplacian map" will be
used in the remainder of the text. For actual calculations,
a slightly more elaborate version of Equation 2 was used,
which takes into account the potentials at eight instead of
four neighboring points.13 The relative weighing factors
for the potentials in Equation 2 may be conveniently
1
expressed in the computational molecule 1 - 4 1. The
1 4
1
1
form which was actually used was 4 - 2 0 4. For numerical
1 4 1
calculations, a value of 400 ohm cm was assumed for the
extracellular resistivity, p. The extracellular current density vector, j , will be expressed in /xA/mm2, the current
source strength, i, in nA/mm3.
Results
The Relationship between the Extracellular DC
Electrogram and the Transmembrane Potential during
Early Ischemia
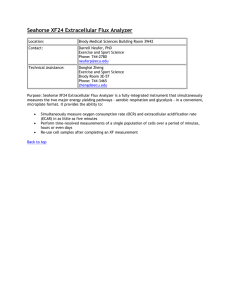
Figure 1 depicts the changes in the transmembrane
potential and local extracellular DC electrogram during
the first minutes after coronary artery occlusion. Each
panel is a superposition of the transmembrane potential
and the extracellular electrogram recorded at a single site
during the control situation and at various intervals during
ischemia. The first change to be observed is a shift of the
resting membrane potential to a more positive value and
a concomitant depression of the T-Q segment of the
extracellular potential. In the following minutes, the resting membrane potential decreases further and the upstroke velocity, amplitude, and duration of the action
potential diminish. These changes are reflected in the
extracellular signal by an increased T-Q depression and ST elevation, and by a decrease in magnitude and downstroke velocity of the electrogram spike. The decrease in
the resting transmembrane potential always was associated
with T-Q segment depression at every subepicardial site at
which it was measured. The nature of S-T elevation,
which, in Figure 1, is due to loss of action potential
amplitude and duration, is more complex. The onset of
local depolarization in Figure 1 was only slightly delayed
during ischemia with respect to the beginning of the
ventricular complex. As shown in Figure 2, from another
experiment, the onset of local depolarization in the ischemic zone can be markedly delayed. At these sites, the
CIRCULATION RESEARCH
606
2l&' occl.
4' OCCl.
20 mV
VOL.
42,
NO.
5,
MAY
1978
the nonischemic tissue causes an early and positive T
wave. Whenever repolarization of ischemic cells occurs
later than that of normal tissue, a negative T wave results.
The electrical alternation shown in Figure 2 is a typical
feature of the ischemic cells and occurs within the first
minutes of ischemia. In the center of the ischemic zone it
precedes the phase of unresponsiveness shown in Figure
3. The absence of local electrical activity is reflected in the
extracellular signal by a monophasic potential. At this
stage of ischemia, which begins some 7 minutes after
ligation, the extracellular complexes have their maximal
amplitude, the T-Q depression being about -15 mV and
the S-T elevation, about +35 mV. By withdrawing the
microelectrode from the unresponsive cell, an estimate
could be made of the membrane potential, which in this
case was - 6 5 mV.
Epicardial Potential Distribution during Early Ischemia
Downloaded from http://circres.ahajournals.org/ by guest on October 1, 2016
-
50 mV
200 msec
FIGURE 1 Local DC extracellular electrograms (top) and transmembrane potentials (bottom) recorded from a single subepicardial cell in the intact heart during control situation and 2.5, 4, 4.5,
and 7 minutes after occlusion (occl.) of the left anterior descending
artery. In each panel, the control signals are superimposed over
the signals recorded at the same site during ischemia. The solid line
in the extracellular electrogram indicates zero level.
delay in the onset of local activation seems mainly responsible for the local S-T elevation. The polarity of the local
T wave is dependent on both the duration of the ischemic
action potential and on the moment of activation. A short
action potential which repolarizes earlier than the cells in
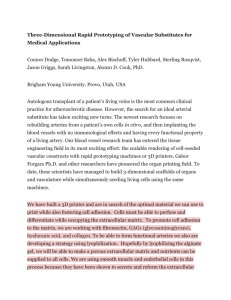
Figure 4 shows maps of isopotential lines constructed
from recordings taken between 15 and 30 minutes after
coronary artery occlusion at 240 epicardial sites, separated
by 3 mm, on the anterior wall of the heart. The upper
map shows the potential distribution during diastole; the
lower map shows that during early systole (250 msec after
the atrial stimulus). Both maps show an arrangement of
the isopotential lines around a central region with a
maximal T-Q depression of - 1 5 mV and a maximal S-T
elevation of +35 mV. In six other mapping experiments,
the results were comparable to those of Figure 4 with
respect to the arrangement of the isopotential lines and
amplitude of the potential changes. Complexes recorded
along a line where the potential gradient is steep show a
transition from completely monophasic potentials that
040rriV
50 mV
20 mV
control
« o msec
020 mV
-T\
control
7'occl.
0-65jwjL_^y--v-ri'(
5 min occl.
200 msec
FIGURE 2 Transmembrane potential and local DC electrogram
before (top) and 5 minutes after coronary occlusion (bottom).
Note alternation in action potential duration and amplitude. Delayed repolarization in ischemic area results in a negative T wave
in the electrogram.
\
withdraw microelectrode
FIGURE 3 Transmembrane potential and DC extracellular electrogram, before and 7 minutes after coronary occlusion. Local
unresponsiveness is reflected by a monophasic extracellular electrogram. Withdrawal of the microelectrode in lowest panel indicates
the level of membrane potential.
S-T AND T-Q SEGMENT CHANGES DURING ISCHEMIA//C/efcer el al.
607
Downloaded from http://circres.ahajournals.org/ by guest on October 1, 2016
FIGURE 4 Epicardial potential distribution in diastole (top) and early systole (bottom) after 15-25 minutes of occlusion of the left anterior
descending artery. Asterisks on the lowest electrogram indicate the moments during the cycle at which the potentials were measured. Signals
were recorded from the shadowed area on the anterior aspect of the heart shown in the inset, at sites 3 mm apart. The extracellular complexes
shown were recorded from sites along the line of steep potential gradients indicated. Square wave pulse indicates a 30-mV calibration.
Isopotential lines in both maps represent 4-mVsteps.
-10-
FIGURE 5 Comparison of epicardial DC potentials and intramural DC potentials recorded 3 mm below the epicardial surface. Inset shows
the arrangement of the measuring points: The epicardial sites (triangles) separated by 5 mm form a grid of 3 rows and 12 columns. The
intramural electrodes (crosses) are inserted at a distance of 1 mm from the epicardial measuring sites. The 3 pairs of graphs show the
potential distribution along the 3 rows during the T-Q segment (open circles) and the S-T segment (filled circles) before and 15 minutes after
occlusion. Intramural potentials are connected by an interrupted line; epicardial potentials, by a solid line. The time ofdiastolic and systolic
measurement is indicated by open and filled circles on two redrawn extracellular electrograms, one of which is in the ischemic zone and the
other in the normal tissue. Note that, during ischemia, intramural and epicardial potential profiles in the border zone are almost
superimposable.
CIRCULATION RESEARCH
608
indicate local unresponsiveness to normal extracellular
complexes that indicate normal intrinsic activity. In this
experiment, the shortest distance measured between areas
showing unresponsiveness and areas showing normal activity was 9 mm. Since the recording sites were separated
by 3 mm, the actual dimensions of this border zone could
be less.
Intramural Potential Distribution during Early Ischemia
Downloaded from http://circres.ahajournals.org/ by guest on October 1, 2016
To interpret the electrical changes on the epicardial
surface, we had to know whether the ischemic changes in
DC electrograms were uniform throughout the ventricular
wall or whether important differences existed between
intramural and corresponding surface sites. We therefore
performed several experiments, using intramural wick
electrodes to record DC potentials in the ventricular wall,
at various distances from the epicardial surface. In the
experiment shown in Figure 5, intramural wick electrodes
were inserted at 5-mm intervals in three parallel rows, and
intramural potentials were recorded 3 mm from the epicardial surface. Epicardial electrograms were recorded at
a site 1 mm from the insertion point of the intramural
electrode.
Potentials at fixed moments during diastole and systole
are depicted for the control condition and after 15 minutes
of ischemia. Although at certain sites during ischemia
there are slight differences in magnitude between intramural and epicardial potentials, it is evident that the
transitional zone where the potentials return to normal
has the same configuration and occurs at the same sites
both at the surface and in the wall. In another experiment
in which intramural potentials were recorded at different
VOL.
42, No. 5,
MAY
1978
depths, i.e., 3, 6, and 9 mm from the epicardial surface,
the potential profiles at the surface and in the wall also
were practically superimposable. We concluded therefore
that in the perfused pig heart the ischemic changes in
potential are uniform throughout the ventricular wall.
Consequently, the main orientation of the extracellular
current which causes the potential differences in the
epicardial extracellular space is directed parallel to the
surface.
Extracellular Epicardial Current Flow during Early
Ischemia
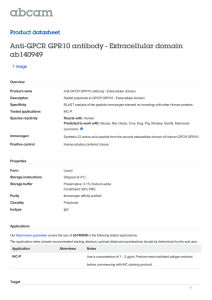
An isopotential map during the early S-T segment (250
msec after the atrial stimulus) and the corresponding
Laplacian map after 15 minutes of occlusion are shown in
Figure 6. The steepest potential gradients (left panel) are
situated in the border zone, and the potential distribution
in the center of the ischemic zone is more uniform. Since
the center of the ischemic zone is more positive with
respect to the normal area, currents must flow in a
centrifugal direction towards the nonischemic area. As
can be seen from the computed Laplacian map in the right
panel, the main sources of these currents are localized in
the borders of the ischemic area. At the site of the main
source maximum (point A), the current source has an
amplitude of 1.0 jiA/mra1. The current emerging from
point A spreads out into the adjacent sinks. The sinks are
distributed over a larger area than the sources and,
therefore, have smaller maximum amplitudes. At point B,
a current of 0.6 /xA/mm3 is disappearing from the epicardial layer. In the map of Figure 6, the greatest extracellular current density vector is located between A and B and
200 msec
FIGURE 6 Epicardial potential distribution (left panel) and computed Laplacian map (right panel) after 15 minutes of ischemia, at a
moment in the cardiac cycle indicated by the asterisks on redrawn extracellular electrograms recorded from sites A and B. Shaded area in
inset represents area recorded from. In the isopotential maps, lines indicate 4-mV steps. In the Laplacian maps, the shaded area represents
current sources; the unshaded area, current sinks. Lines indicate steps of extracellular current change of 200 nA/mm* extracellular space.
Since the Laplacian values of sites at the border of the area recorded from cannot be calculated, the Laplacian map is smaller than the
isopotential map.
S-T AND T-Q SEGMENT CHANGES DURING ISCHEMIA/Kleber et al.
609
Downloaded from http://circres.ahajournals.org/ by guest on October 1, 2016
FIGURE 7 Epicardial isopotential maps during
diastole (top) and systole (middle) after 15 minutes, 1 hour, and 2 hours of occlusion. Moments
of measurements are indicated by asterisks on the
extracellular electrogram recorded from a site in
the ischemic area. Isopotential lines indicate 4mV steps. Area recorded from is shown in- the
inset. In the lowest panels, the shaded areas
represent zones of absent local electrical activity.
has an amplitude of 1 /iA/mm!. The localization of
current sources and sinks at this time of the cardiac cycle
was similar in all other experiments; a maximal extracellular current density in the order of 1 /xA/mm2 was
present in the border zone.
A similar distribution of current sources and sinks was
present at a later instant during systole, when cells which
are already repolarized show a positive T wave in the local
extracellular electrogram, whereas cells which are still
depolarized show a flat S-T segment.
During diastole, extracellular current flows into the
negative ischemic area. The potential changes occur more
gradually toward the center, and the absolute magnitudes
of the potentials are less than during the S-T segment
(Fig. 4). The extracellular current is therefore more
regularly distributed over the ischemic area and flows in
the opposite direction than during the S-T segment.
Maximal values are in the order of 0.3 ju.A/mm2.
Time Course of Extracellular Potential Distribution
within the First 2.5 Hours Following Coronary Artery
Occlusion
The use of a rubber membrane pierced with holes
enabled us to record extracellular potentials at the same
sites over a period of a few hours. Figure 7 shows diastolic
and systolic isopotential maps determined at 15-30 minutes, 60-75 minutes, and 120-135 minutes after coronary
artery occlusion. It is evident that the magnitude of the TQ depression and S-T elevation are greatest 15 minutes
after occlusion. After 2 hours of ischemia, the T-Q
depression has moderately decreased to values between
- 2 and —6 mV, while S-T elevation shows a marked
decrease to about +10 mV throughout the injured area.
The overall amplitudes of the monophasic extracellular
potentials indicating local unresponsiveness 2 hours after
occlusion were 25% of the amplitude measured between
10 and 15 minutes after occlusion. This decrease in
amplitude of the extracellular DC potentials was present
in all experiments, and the potential distribution after 2
hours was always very similar to that shown in Figure 7.
The initial fast transition from normal electrical activity to
unresponsiveness, already demonstrated by intracellular
measurements in Figures 1-3, results in two large zones of
absent electrical activity, as shown in the left lower panel
of Figure 7. Between approximately 30-45 minutes after
occlusion, most of the cells in this area regain their
excitability. In the experiment shown in Figure 7, only
three small areas of unresponsiveness were present after 1
hour. After 2 hours of occlusion, activity had again
disappeared from a large zone which exceeded the area of
unresponsiveness present after 15 minutes of occlusion.
Transmembrane potentials which were measured from
nonischemic sites within 2.5 hours of coronary occlusion
showed the same amplitude and configuration as the
control values before occlusion. At this stage, no electrical
activity could be restored by reperfusion. The transient
return of electrical activity in previously unresponsive cells
was found in every experiment. Its onset occurred at
intervals varying from 30 to 45 minutes after occlusion,
and unresponsiveness gradually returned between 1 hour
and 1.5 hours after occlusion.
Intracellular recordings at different stages of occlusion
are shown in Figure 8. In the left panel, a cell in the center
of the ischemic area has become unresponsive after 7.5
minutes of occlusion. After 42 minutes, activity has returned. The transmembrane action potential at this stage
is of low amplitude and short duration and shows a loss of
CIRCULATION RESEARCH
610
o-
control
14'0CCl.
VOL.
42, No. 5,
MAY
1978
of occlusion, the decrease in T-Q depression and S-T
elevation is marked at both epicardial and intramural sites
and follows the same time course. The border of the
potential changes does not change its site between 15
minutes and 2 hours of occlusion. Similar results were
obtained when intramural recordings 3 and 9 mm from
the epicardium were compared with corresponding surface
recordings. In Figure 9 it can be seen that site A is
unresponsive at 15 minutes of ischemia but that intrinsic
activity reappears after 30 minutes, while, even after 1
hour, the small downstroke indicates the presence of a
small transmembrane action potential. Site B shows activity throughout the first hour. After 2 hours, no intrinsic
activity is seen at either site.
Control Experiments in Situ
Ihour
Downloaded from http://circres.ahajournals.org/ by guest on October 1, 2016
FIGURE 8 The panel on the left shows the transmembrane
potentials (top tracings) and the corresponding DC extracellular
electrogram (lower tracings) of one cell in the ischemic area before,
and 7.5 and 42 minutes after occlusion of the left anterior
descending artery. Note return of electrical activity after 42 minutes. The panel on the right shows transmembrane potentials (top
tracings) and DC electrograms (lower tracings) in the border zone
at different times after coronary occlusion (in lowest panel, the
atria were not stimulated).
plateau. The onset of depolarization is markedly delayed.
In the panel on the right, the transmembrane action
potential from a border site is shown. Although the
transmembrane potentials remain virtually the same after
14, 30, and 60 minutes of occlusion, the concomitant
extracellular electrogram clearly diminishes in size.
In Figure 9 the time course of potential changes on the
epicardium is compared to that at corresponding intramural sites 6 mm from the epicardial surface. Although
minor transmural gradients existed during different stages
The in situ control experiments did not allow the
measurement of potentials from extracellular sites separated by less than 5 mm, a limit which is needed to obtain
accurate information about epicardial extracellular current
flow. The distribution and amplitude of both epicardial
and intramural DC potentials was similar to that found for
the isolated hearts. The only difference was the time
course of the changes. Initially, unresponsiveness in the
center of the ischemic zone occurred between 5 and 7
minutes after occlusion. Transient improvement of electrical activity in the ischemic zone occurred between 10 and
20 minutes of occlusion. After 1 hour, a large zone of
unresponsiveness was present, and the overall amplitude
of the extracellular monophasic complexes had decreased
to 25% of the values recorded during the initial stage.
This corresponds to the amplitudes found in the isolated
hearts 2 hours after ligation.
Discussion
Our results confirm previous findings9"" that cells in the
ischemic myocardium undergo depolarization after coronary artery occlusion. The transmembrane action poten-
FIGURE 9 Epicardial DC potentials (solid lines)
and intramural DC potentials recorded 6 mm below
the epicardial surface (broken lines) at sites indicated
in the inset, at 3, 15, 30, 60, and 150 minutes after
coronary artery ligation. Redrawn extracellular electrograms from sites A, B, and C are shown for each
period of measurement. Open and filled circles
indicate moments during cardiac cycle at which
potentials have been measured.
S-T AND T-Q SEGMENT CHANGES DURING ISCHEMIA/Kleber et al.
Downloaded from http://circres.ahajournals.org/ by guest on October 1, 2016
tials show a progressive decrease in amplitude and upstroke velocity and a decrease in duration, until, between
7 and 10 minutes after ligation, no action potentials can
be evoked by excitation propagating from normal myocardium." Membrane potentials recorded from unresponsive
cells (Fig. 3) indicate that the critical level at which
unresponsiveness occurs is identical to the threshold for
the rapid inward sodium current.H
Our recordings of DC extracellular electrograms obtained simultaneously with the recording of transmembrane potentials show that loss of resting membrane
potential is associated with T-Q depression9'10 and that
loss of action potential amplitude, action potential
shortening, and delayed activation are associated with S-T
elevation (Figs. 1 and 2). Complete unresponsiveness
results in a monophasic extracellular potential" (Fig. 3),
the amplitude of which is comparable to the monophasic
potential recorded after mechanical injury.15
The ischemic changes in the experiments on in situ
hearts were comparable to the changes in the isolated
heart with respect to the magnitude of the T-Q and S-T
segment changes and their distribution. The faster time
course of their development may reflect the fact that the
oxygen demand in the Langendorff-perfused heart is
smaller than in a heart working against an external load
and, consequently, changes in intracellular metabolism
occur more slowly after coronary occlusion in the isolated
heart.
The determination of the intramural extracellular potential distribution showed that no major transmural potential gradients were present in the pig heart during
ischemia. This is in agreement with the finding that
occlusion of the left anterior descending artery in the pig
heart results in a transmural infarct, whereas, in the dog
heart, the ischemic area is predominantly in the subendocardium.16 The absence of transmural potential gradients
means that extracellular current flow during the T-Q and
S-T segments is directed tangentially to the ventricular
wall and generated at any layer of tissue by the intracellular compartment of this layer. Extracellular epicardial
current flow then is the consequence of intracellular
current of opposite direction in the epicardial cellular
sheet. The electrical driving force for this current is the
instantaneous difference in transmembrane potentials between ischemic and nonischemic cells, as illustrated in
Figure 1. This relationship between transmembrane potential and the extracellular DC electrogram already has
been shown hypothetically in electrical models of regional
myocardial ischemia16'17 and experimentally in isolated
perfused rabbit hearts.18
To quantify the direction, localization, and magnitude
of extracellular currents, isopotential maps were constructed from the epicardial surface. An ideal map would
be constructed from simultaneous recordings. Several
observations showed that the error introduced by sequential recording at different sites did not influence the main
conclusions drawn from our data. (1) Although extracellular potentials changed rapidly during the first minutes
of ischemia, after 10-15 minutes, potentials remained
stable for some 20 minutes, as shown by repeated mapping
during this period. The decline in potential amplitude in
later stages occurred very gradually. (2) Maps from differ-
611
ent experiments made after 15 minutes of ischemia at
similar periods showed essentially the same configuration
and amplitudes, although the sequence of measurement
was different in different experiments. (3) The area covered by points necessary to calculate one value of the
Laplacian operator was recorded within 3 minutes or less.
The Laplacian maps provide a two-dimensional representation of the origin of the extracellular currents. During
the early stage of the S-T segment, and during its later
stages, when some fibers have already repolarized, the
distribution of current sources and sinks is similar and is
localized in the border zone. The maximal strength of the
current sources was of the order of 1.0 /xA/mm3 extracellular space. This current is dispersed into sinks localized
toward the normal myocardium. Maximal extracellular
current densities are found in the border zone and are of
the order of 1 /iA|mm!. In diastole, the current flows in
the opposite direction, is more dispersed over the ischemic
area, and has a maximal amplitude of 0.3 /nA/mm2. These
current strengths are scaled by the value we chose for
resistivity of the tissue. Values found in the literature
range from 800 to 160 ohm-cm.1*"21 We used the value of
400 ohm-cm, which might be on the low side. Consequently, we might have underestimated the actual current
strength. Also, the fact that the muscle resistivity may be
anisotropic21 has not been taken into account. Finally,
since the Laplacian represents a second difference quotient of the measured values and no smoothing of the data
was done, the Laplacian maps are more sensitive for noise
than the potential maps. Therefore the Laplacian maps
should be interpreted mainly as an indication of the order
of magnitude and of the localization of the current sources
and sinks.
The onset of local depolarization in the ischemic area
can be markedly delayed."'22"25 This delay may influence
the direction of current flow during repolarization, because repolarization in the ischemic area may outlast
repolarization in the normal area and produce a negative
T wave in the electrogram, as shown in Figure 2. This
occurs especially in the transient phase during which
ischemic action potentials alternate with respect to amplitude and duration." Because of the transient nature of
this phase, maps which would have allowed calculations of
current flow could not be made. The occurrence of
arrhythmias during the first minutes of ischemia coincides
with the period of maximal T-Q depression and S-T
elevation, and with the phase of electrical alternans." One
might therefore ask whether the extracellular current flow
does play a role in the genesis of ectopic ventricular
rhythms. Figure 10 shows in diagrammatic form the
relationship between local electrical activity and current
flow during repolarization at the time alternation occurs
in the ischemic area. In the upper panel, current flows
during the repolarization of the normal action potential
intracellularly into ischemic cells which have already repolarized. The maximal electrotonic effect of this depolarizing current is exerted at sites where the transmembrane
current is greatest (maximal source in the Laplacian map).
Since, at this stage, excitability of the ischemic zone is
depressed and the refractory period is longer than the
action potential duration," it is unlikely that local ectopic
excitation occurs. However, as indicated in the lower
612
CIRCULATION RESEARCH
OITW,
-15mV
extracellular
+ 5 n W
_
75mV
Downloaded from http://circres.ahajournals.org/ by guest on October 1, 2016
FIGURE 10 Relationship between transmembrane potential and
DC extracellular electrogram during electrical alternans. The signals of Figure 2 are superimposed so that potential differences
between ischemic and nonischemic potentials can be estimated. In
the diagram, the relationship is given between transmembrane
potential, extracellular potential, and current flow at a time indicated by the arrows in the superimposed potentials. In the upper
panel, electrotonic current has a depolarizing effect on the ischemic
cells; in the lower panel, the electrotonic current exerts a depolarizing effect on the normal cells.
panel, in the subsequent beat, when repolarization in the
ischemic area occurs later than repolarization in the
normal zone, current flows in the opposite direction
toward the normal zone, where it exerts a depolarizing
effect. At that moment in the cardiac cycle, excitability in
the normal myocardium has recovered, and the current
requirement for excitation at that moment may even be
slightly less than later in diastole.26 In a previous paper it
was shown that during the phase of alternation, the
conditions required for reentry were present." In view of
the above considerations, we should add that reexcitation
causd by "currents of injury" may also be a factor in the
genesis of arrhythmias. This reexcitation would occur
when, primarily because of delayed activation within the
ischemic zone, repolarization in the ischemic area outlasts
repolarization in the normal zone. This condition is apparent from the configuration of the extracellular electrogram
and is represented by a negative T wave.
VOL.
42, No. 5,
MAY
1978
dial cells in vitro27 and are partially responsible for the
early occurrence of inexcitability in the ischemic area."
After 90 minutes of ischemia, excitability has again disappeared from a region which, at many sites, exceeds the
initial area of unresponsiveness. At 120 minutes, the T-Q
depression has about the same amplitude as the S-T
elevation, whereas the ratio of S-T elevation to T-Q
depression after 15 minutes is about 2.5. This shift can be
explained by the loss of polarization of the ischemic cells.
When the membrane potential of ischemic cells gradually
shifts toward zero, the electrical gradient between ischemic and nonischemic cells increases during diastole
and decreases during activity of the normal zone. The
overall decrease in extracellular potential at all epicardial
and intramural sites within the ischemic area during the
first 2 hours after coronary artery ligation can be due
either to a decrease in tissue resistivity through which the
current is flowing or to a decrease in the amount of
current. Extracellular edema' may lead to a decrease in
extracellular resistivity, and this could occur in the ischemic zone and partially account for our results. It
would, however, lead to an increase in conduction velocity, and the marked delays in onset of local depolarization
in the border zone where local activity is only moderately
impaired would not be expected. A gradual electrical
uncoupling of the ischemic cells may be the major reason
for the decrease in amplitude of the extracellular potentials.
Wojtczak28 has shown that the internal longitudinal
resistance of bovine myocardial trabeculae increases rapidly when the fibers are immersed in hypoxic, glucose-free
medium, and that this increase is related to an increase in
intracellular Ca2+ concentration. This process may be
similar to the "healing over" observed after mechanical
injury of cardiac tissue, which is dependent on the presence of Ca ions at the low resistance intercellular connections.29'30
The decrease in amplitude of S-T elevation and T-Q
depression after the initial stage of coronary occlusion
thus can be due either to a reappearance of electrical
activity in the ischemic area or to electrical uncoupling of
damaged cells.
Acknowledgments
We thank Wim ter Smitte for excellent technical assistance.
Time Course of T-Q and S-T Segment Potential Changes
References
Several factors could account for the gradual decrease
in T-Q depression and S-T elevation which begins 30
minutes after ligation. Between 30 and 45 minutes of
ischemia, action potentials reappear in previously unresponsive cells, and this may lead to a decline in T-Q
depression and S-T elevation. We do not know the reason
for this transient improvement of electrical activity, which
has been noted before, both in the pig heart" and in the
dog heart.23 One might speculate about a delayed increase
of collateral flow into the ischemic area. Alternatively, it
is possible that, due to diffusion through the extracellular
space, the extracellular concentration of substances which
leaked out from ischemic cells may diminish with time.
Such substances produce inexcitability of normal myocar-
1. Burdon-Sanderson J, Page FJM: On the time relation of the excitatory
process in the ventricle of the heart of the frog. J Physiol (Lond) 2:
384-429, 1879
2. de Waart A, Storm CJ, Koumans AKJ: Ligation of the coronary
arteries in Javanese monkeys. III. Further theoretical considerations
of the changes in the ventricular electrocardiogram, with illustrative
experiments. Am Heart J 12: 184-205, 1936
3. Nahum LH, Hamilton WF, Hoff HE: The injury current in the
electrogram. Am J Physiol 139: 202-207, 1945
4. Eyster JAE, Meek WJ, Goldberg H, Gilson WE: Potential changes in
an injured region of cardiac muscle. Am J Physiol 124: 717-728,
1938
5. Sugarman H, Katz LN, Sanders A, Jochim K: Observations on the
genesis of the electrical currents established by injury to the heart.
Am J Physiol 130: 130-140, 1940
6. Katcher AH, Peirce G, Sayen JJ: Effects of experimental regional
ischemia and levarterenol on the RS-T segment and baseline of
ventricular surface electrograms obtained by direct-coupled amplification. Circ Res 8: 29-43, 1960
S-T AND T-Q SEGMENT CHANGES DURING ISCHEMIA/Kleber et al.
Downloaded from http://circres.ahajournals.org/ by guest on October 1, 2016
7. Bruyneel KJJ: Use of moving epicardial electrodes in defining STsegment changes after acute coronary occlusion in the baboon. Relation to primary ventricular fibrillation. Am Heart J 89: 731-741,
1975
8. Cohen D, Kaufman LA: Magnetic determination of the relationship
between the ST-segment shift and the injury current produced by
coronary artery occlusion. Circ Res 36: 414-424, 1974
9. Samson WE, Scher AM: Mechanism of ST-segment alteration during
acute myocardial injury. Circ Res 8: 780-787, 1960
10. Prinzmetal M, Toyoshima H, Ekmekci A, Mizumo Y, Nagaya T:
Myocardial ischemia. Nature of ischemic electrocardiograph^ patterns
in the mammalian ventricles as determined by intracellular electrographic and metabolic changes. Am J Cardiol 8: 493-503, 1961
11. Downar E, Janse MJ, Durrer D: The effect of acute coronary artery
occlusion on subepicardial transmembrane potentials in the intact
porcine heart. Circulation 56: 217-224, 1977
12. Woodbury JW, Brady AJ: Intracellular recording from moving tissue
with a flexibly mounted ultra microelectrode. Science 123: 100-101,
1956
13. Bickley WG: Finite difference formulae for the square lattice.
14. Beeler GW, Reuter H: Voltage clamp experiments on ventricular
myocardial fibers. J Physiol (Lond) 207: 165-190, 1970
15. Hoffman BF, Cranefield PF, Lepeschkin E, Surawicz B, Herrlich H:
Comparison of cardiac monophasic action potentials recorded by
intracellular and suction electrodes. Am J Physiol 196: 1297-1301,
1959
16. Holland RP, Brooks H: Precordial and epicardial surface potentials
during myocardial ischemia in the pig. A theoretical and experimental
analysis of the TO and ST segments. Circ Res 37: 471-479, 1975
17. Fozzard HA, Das Gupta DS: ST-segment potentials and mapping.
Theory and experiments. Circulation 54: 533-537, 1976
18. Wittig JH, Vaughan Williams EM: Mechanism of decrease of STelevation by propranolol in ischemic myocardium (abstr). Circulation
54(suppl II): 15, 1976
613
19. Schwarz HP, Kay CJ: Specific resistance of body tissue. Circ Res 4:
665-670, 1956
20. Thalen HJTh: The artificial cardiac pacemaker. M.D. Thesis, University of Groningen, 1969
21. Rush S, Abildskov JA, McFee R: Resistivity of body tissues at low
frequencies. Circ Res 12: 40-50, 1963
22. Durrer D, Formijne P, van Dam RTh, Biiller J, van Lier AAW,
Meijler FL: The electrocardiogram in normal and some abnormal
conditions. In revived human fetal hearts and in acute and chronic
coronary occlusion. Am Heart J 61: 303-314, 1961
23. Scherlag BJ, El-Sherif N, Hope R, Lazzara R: Characterization and
localization of ventricular arrhythmias resulting from myocardial ischemia and infarction. Circ Res 35: 372-383, 1974
24. Boineau JP, Cox JL: Slow ventricular activation in acute myocardial
infarction. A source of re-entrant premature ventricular contraction.
Circulation 48: 702-713, 1973
25. Waldo AL, Kaiser GA: A study of ventricular arrhythmias associated
with acute myocardial infarction in the canine heart. Circulation 47:
1222-1228, 1973
26. Weidmann S: Effects of calcium ions and local anaesthetics on
electrical properties of Purkinje fibers. J Physiol (Lond) 129: 568582,1955
27. Downar E, Janse MJ, Durrer D: The effect of "ischemic" blood on
transmembrane potentials of normal porcine ventricular myocardium.
Circulation 55: 455-462, 1977
28. Wojtczak J: Hypoxia-induced electrical uncoupling and contractures
of cardiac cells. In Proceedings of the 7th European Congress of
Cardiology, Amsterdam, Holland Organizing Center, 1976, p 143
29. Deleze J: The recovery of resting potential and input resistance in
sheep heart injured by knife and laser. J Physiol (Lond) 208: 547562,1970
30. de Mello WC: Effect of intracellular injection of calcium and strontium on cell communication in heart. J Physiol (Lond) 250: 231-245,
1975
Mechanism and time course of S-T and T-Q segment changes during acute regional
myocardial ischemia in the pig heart determined by extracellular and intracellular
recordings.
A G Kléber, M J Janse, F J van Capelle and D Durrer
Downloaded from http://circres.ahajournals.org/ by guest on October 1, 2016
Circ Res. 1978;42:603-613
doi: 10.1161/01.RES.42.5.603
Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1978 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7330. Online ISSN: 1524-4571
The online version of this article, along with updated information and services, is located on the
World Wide Web at:
http://circres.ahajournals.org/content/42/5/603.citation
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in
Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the
Editorial Office. Once the online version of the published article for which permission is being requested is
located, click Request Permissions in the middle column of the Web page under Services. Further information
about this process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation Research is online at:
http://circres.ahajournals.org//subscriptions/