RESEARCH ARTICLE
Instability of the faecal microbiota in diarrhoea-predominant
irritable bowel syndrome
n1, Juan J. Abella
n1, Nuria Jime
nez-Herna
ndez1, Alejandro Artacho1, Vicente Garrigues2,
Ana Durba
2
2
1,3
s Moya1,3
Vicente Ortiz , Julio Ponce , Amparo Latorre & Andre
n en Salud Pu
blica (CSISP) – Instituto Cavanilles de Biodiversidad y
Joint Research Unit on Genomics and Health Centro Superior de Investigacio
ecnic La Fe,
Biologıa Evolutiva (ICBiBE), Universitat de Valencia, Valencia, Spain; 2Digestive Functional Disorders Unit, Hospital Universitari i Polit
blica (CIBEResp), Madrid, Spain
Val
encia, Spain; and 3CIBER en Epidemiologıa y Salud Pu
1
Correspondence: Andres Moya, Centro
n en Salud Pu
blica
Superior de Investigacio
~a 21, 46010
(CSISP), Avenida de Catalun
Val
encia, Spain.
Tel.: +34 96 354 3480;
fax: +34 96 354 3670;
e-mail: andres.moya@uv.es
Received 28 February 2013; revised 20 June
2013; accepted 18 July 2013. Final version
published online 23 August 2013.
DOI: 10.1111/1574-6941.12184
MICROBIOLOGY ECOLOGY
Editor: Julian Marchesi
Keywords
irritable bowel syndrome; follow-up; faecal
microbiota; metagenomics;
metatranscriptomics.
Abstract
The irritable bowel syndrome (IBS) is a functional gastrointestinal disorder
with a largely unknown aetiology and a wide range of symptoms. Most
cross-sectional studies carried out so far suggest subtle alterations in the
structure of the intestinal microbiota that are barely reproduced, partly
because of the high inter-subject variation in the community composition
and disorder-specific features. We performed a longitudinal study to explore
the within-subject variation in the faecal microbiota in two patients with IBS
classified into the diarrhoea subtype and the healthy spouse of one of them.
Faecal communities were monitored over 6–8 weeks and analysed through
metagenomic and metatranscriptomic approaches. We found a higher temporal instability in the fraction of active microbiota related to the IBS condition
and fluctuating symptoms. Strong and quick shifts in the distribution of the
active microbiota and changes in the global pattern of gene expression were
detected in association with acute diarrhoea, whereas microbial composition
and encoded functions were more stable. The specific alterations in the microbiota were barely reproduced within and between patients. Further research
is needed to assess whether these changes are a consequence of the abnormal
gut function in acute diarrhoeic episodes and the potential usefulness of
tackling them.
Introduction
The irritable bowel syndrome (IBS) is the most common
functional gastrointestinal disorder in Western countries.
The main symptoms include abdominal pain or discomfort, bloating and alteration in bowel habits (Hungin
et al., 2005; Longstreth et al., 2006). Over the past decade, there has been an accumulation of evidence suggesting a role of the gut microbiota in IBS, mainly coming
from case–control studies based on molecular methods,
although no consensus has been reached regarding the
association of specific microorganisms with IBS (Salonen
et al., 2010; Simren et al., 2013). The detection of the
subtle alterations that seem to characterise microbial dysbiosis in IBS is hampered by the relatively small size of
the cohorts and the many sources of variability in the
FEMS Microbiol Ecol 86 (2013) 581–589
composition of the microbiota unrelated to the disorder.
Moreover, the detection of patterns may have been
further complicated by differences between patients
regarding physiopathology. Longitudinal studies in which
patients are followed over time may help to overcome
this.
There are few longitudinal studies on IBS, apart from
clinical trials targeting the GI microbiota that address the
improvement in symptoms (Moayyedi et al., 2010; Basseri
et al., 2011; Simren et al., 2013). One study reported a
higher long-term temporal variation in the predominant
faecal bacteria of patients with IBS when compared to
that of controls (M€att€
o et al., 2005). Later, the same
cohorts were re-analysed excluding patients who had
taken antibiotics (Maukonen et al., 2006). The authors
found a greater instability in patients with IBS in the
ª 2013 Federation of European Microbiological Societies.
Published by John Wiley & Sons Ltd. All rights reserved
A. Durb
an et al.
582
metabolically active clostridial populations and speculated
that instability might be due to variation in symptomatology between sampling days. In support of this, stabilisation of the faecal microbiota has been observed in
patients with IBS after a probiotic supplementation that
alleviated the symptoms (Kajander et al., 2008).
Besides, the functions of the microbiota are an essential
factor to consider in understanding the GI disorders.
Tana et al. (2010) found higher levels of acetic and propionic acids in faecal samples of patients with IBS compared with those of controls, which correlate with worse
GI symptoms and quality of life and higher amounts of
Lactobacillus and Veillonella. Elevated levels of amino
acids and phenolic compounds (Ponnusamy et al., 2011)
or primary bile acids (Duboc et al., 2012) have also been
found in faeces of patients with IBS. Le Gall et al. (2011)
explored the metabolic activity of the faecal microbiota in
patients with IBS, patients with ulcerative colitis (UC)
and healthy controls. They found that specific metabolites
were associated with each group, but the IBS condition
could not be predicted from the metabolite profile, unlike
the UC or control conditions, similar to what happens at
the compositional level (Qin et al., 2010; Durban et al.,
2012). The functional impact of the gut microbiota on
the IBS condition and on the associated symptoms
warrants further investigation.
The objective of this study was to investigate the stability of the compositional and functional profiles of the
microbiota of patients with IBS over time and the specific
changes associated with acute diarrhoeic episodes. We followed two IBS patients with diarrhoea as predominant
bowel habit and a matched healthy control of one of
them over 6–8 weeks. Self-reported symptom diaries
allowed relating microbiological attributes to the presence
and severity of symptoms. The faecal microbiota were
analysed for the first time in IBS using metagenomics and
metatranscriptomics.
Materials and methods
The detailed study protocol is provided as Supplementary
Material.
Sampling
Two female IBS patients with diarrhoea subtype, according to the Rome III criteria (Longstreth et al., 2006), were
included in the study (Patients 1 and 2). The husband of
Patient 1 was included as an age-matched control who
shared her environment (Control 1). Participants gave
informed written consent to the study protocol, which
was approved by the Ethics Committee of La Fe University Hospital (Valencia, Spain). Relevant volunteers’
details are summarised in Table 1. Patients underwent
medical examination every 2 weeks and collected daily data
on symptoms (the presence of abdominal pain/discomfort, abdominal distension and/or defaecatory urgency, and
number and type of stools according to the Bristol scale)
(Lewis & Heaton, 1997). Faecal samples were collected in
the morning every 2 days the first week and once a week
thereafter. Additional samples were collected when patients
reported acute symptoms. A summary of the symptom diaries is shown in Supporting Information, Table S1. Faeces
were collected in tubes containing phosphate-buffered
saline and kept at 4 °C for 1–2 h before being stored at
80 °C. Volunteers kept their routine lifestyle habits
throughout.
Sequencing of metagenomes and
metatranscriptomes
Faecal suspensions were centrifuged at 3200 g to remove
big particles. Supernatants were centrifuged at 16100 g
to pellet cells. Nucleic acids were extracted using the
AllPrep DNA/RNA Mini Kit (QIAGEN). Total RNA was
Table 1. Characteristics of Control 1 (C1), Patient 1 (P1) and Patient 2 (P2)
Subject
C1
P1
P2
Group
Age
Sex
Body mass index
Nationality
Educational level
Physical activity
High fibre food intake
Alcohol consumption
Smoking
Antibiotics (last 3 months)
Medication intake at sampling time
Control
66
Male
31.7
Spanish
University/college
Moderate
Daily
Monthly
Ex-smoker
No
Hypertension, hyperlipidemia,
urinary tract disorders
IBS–diarrhoea
62
Female
27.5
Spanish
University/college
Moderate
Weekly
Never
Ex-smoker
No
Hypertension, arthrosis, osteoporosis
IBS–diarrhoea
21
Female
30.4
Spanish
High school
Moderate
Daily
Never
Smoker
No
Bowel spasms, contraceptives
ª 2013 Federation of European Microbiological Societies.
Published by John Wiley & Sons Ltd. All rights reserved
FEMS Microbiol Ecol 86 (2013) 581–589
583
Follow-up of faecal microbiota in IBS
incubated with DNase I (Ambion) and then linearly
amplified using the MessageAmp II-Bacteria Kit (Ambion). The resulting antisense RNA was converted to double-strand complementary DNA (cDNA) using random
hexamers. This cDNA and total DNA were sent for
pyrosequencing on a Genome Sequencer FLX system
using the GS FLX Titanium chemistry (454 Life Sciences,
Roche). The metatranscriptomes of all samples and the
metagenomes of some samples were analysed (1st and
3rd samples from Patient 1, 1st–5th samples from Patient
2). Table S2 provides characteristics of the obtained
libraries. The entire data set has been deposited in the
Sequence Read Archive of the European Bioinformatics
Institute under the accession number ERP001739.
and with analysis of similarities (ANOSIM). The variation
in symptom presence/absence and intensity was analysed
with principal components analysis (PCA). Chi-squared
tests were applied to assess the homogeneity in the relative abundance of each taxon between days with severe
and milder symptoms within each patient. The LEfSe
algorithm was applied to identify intermediate functional
categories in the KEGG pathway and the TIGRFAM hierarchies characterising the differences between patients and
between days with severe and mild/moderate symptoms
within each patient (Segata et al., 2011). Samples with
< 200 sequences with an assigned functional role were
discarded for analysis due to the great uncertainty in the
estimation of the functional profile.
Annotation of sequences
Results
Genes and cDNAs of the 16S and 23S rRNA genes were
searched in metagenomes and metatranscriptomes as
described previously (Gosalbes et al., 2011). The taxonomic affiliation of 16S rRNA genes and cDNAs was determined using the Classifier tool of the Ribosomal Database
Project (RDP) II (Wang et al., 2007). Species-level phylotypes were defined at 97% of sequence identity for 16S
rRNA reads using the cluster tool of the USEARCH package,
version 5.0 (Edgar, 2010). Metagenomic reads were assembled using the runAssembly tool of the NEWBLER package,
version 2.6 (454 Life Sciences). Metatranscriptomic reads
not labelled as rRNA were aligned to the concatenated
metagenomic assembly of the corresponding volunteer
using the runMapping tool of the NEWBLER package, version
2.6. Putative coding regions were identified in the metagenomic assemblies from the coordinates of best hits in a
BLASTX search against the NCBI nonredundant protein
sequence database (Altschul et al., 1990). Additional
open reading frames were searched using GLIMMER, version
3.02 (Salzberg et al., 1998). Putative coding genes were
compared with the KEGG GENES and the TIGRFAM databases. The taxonomic assignment of the putative coding
regions identified from the BLASTX search was assessed
using the BLAST2LCA tool, version 0.02 (http://github.com/
emepyc/Blast2lca). Metatranscriptomic reads that aligned
to a genomic region adopted its annotations, while reads
not labelled as putative mRNAs were aligned against the
Rfam database. Table S2 shows the number of annotated
sequences per sample, which were the input for descriptive
and statistical analysis.
Statistical analyses
The similarity between samples according to their bacterial composition was assessed with correspondence analysis (CA) or detrended correspondence analysis (DCA)
FEMS Microbiol Ecol 86 (2013) 581–589
Classification of samples based on symptoms
Patients 1 and 2 differed in their symptomatology: Patient
1 complained about abdominal pain, abdominal distension and defaecatory urgency, whereas Patient 2 had a
high number of depositions with diarrhoea (Table S1). In
addition, Patient 1 remained rather stable over the follow-up, while Patient 2 went through several phases of
acute diarrhoea. Sampling days were classified based on
symptoms (Supporting Information, Fig. S1). Days with
milder symptoms were considered those with no pain–
distension–urgency (day 21 in Patient 1; days 1, 7 and 42
in Patient 2) and those with less stools–diarrhoea (days 1,
3 and 7 in Patient 1; day 35 in Patient 2). Days with
severe symptoms were considered those in which the
number of diarrhoeal stools was higher (days 14, 28, 37
and 42 in Patient 1; days 3 and 28 in Patient 2). Day 56
in Patient 2 was also classified as one with severe symptoms because the numbers of diarrhoeal stools in the
surrounding days were among the highest.
Dynamics of the microbial taxonomic profile
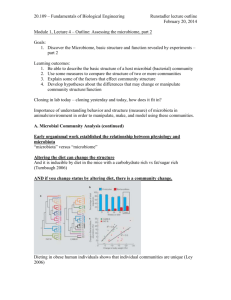
DCA of the distribution of microbial families estimated
from 16S rRNA genes separated samples of Patient 2
from samples of Patient 1 and Control 1, which were
mixed (Fig. 1). However, the last samples of Patient 1
(taken on days with more severe symptoms) were
slightly separated from the rest and closer to samples of
Patient 2. In Patient 2, the active microbiota on most
days with severe symptoms differed markedly from each
other and from those taken on days with mild/moderate
symptoms. Within each patient, samples taken on days
with milder symptoms were quite similar. These patterns
were similar to the ones observed from the taxonomic affiliation of mRNAs, although the bacterial distributions
ª 2013 Federation of European Microbiological Societies.
Published by John Wiley & Sons Ltd. All rights reserved
584
A. Durb
an et al.
to the active fraction of the predominant bacteria (Table
S4). Furthermore, when comparing the temporal variation
in metagenomes and metatranscriptomes over the first
5 days of the follow-up of Patient 2, it could be appreciated
that temporal dynamics was subtler at the metagenomic
level (Fig. 2).
The alterations detected in association with worsening
of symptoms were barely consistent between patients and
within a single patient (Table S5). In Patient 2, the
morning sample of day 3 had the highest level of activity
of Alphaproteobacteria of all samples; the afternoon sample, the highest level of total Bacteroidia and Porphyromonadaceae; and sample of day 56, the highest level of
Streptococcaceae, Clostridiaceae, Betaproteobacteria and
Gammaproteobacteria. In Patient 1, sample of day 14 had
an increase in Verrucomicrobia, while samples of days 28,
37 and 42, an increase in unknown members of Alphaproteobacteria and Proteobacteria, although this trend was
shared with Control 1, which might reflect common environmental factors affecting the microbiota. The increases
in the relative abundance of Proteobacteria were not due
to a single or a few species, as demonstrated by the detection of multiple phylotypes defined at 97% of sequence
identity mapped along reference 16S rRNA genes.
Fig. 1. DCA of the distribution of microbial families in samples of
Control 1, Patient 1 and Patient 2. Data were generated by
taxonomic annotation of 16S rRNA genes in metatranscriptomes.
Percentages correspond to the fraction of inertia explained by each
axis. Samples are labelled with the code of the volunteer (C1, P1 and
P2) and the sampling day over the follow-up. When there are two
samples from a given individual in the same day, these are numbered
after the day (e.g. P2.3.2 refers to the 2nd sample taken on day 3
from Patient 2). Days with milder and severe symptoms are circled in
green and red, respectively.
Dynamics of the microbial functional profile
obtained with both procedures differed significantly (Figs
S2 and S3).
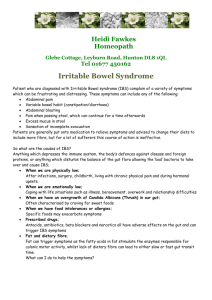
The major groups of active bacteria were similar and
remained quite constant in faeces of Control 1 and
Patient 1 (Fig. 2, Table S3a). The Clostridia and Bacteroidia classes accounted for the largest number of sequences
all days in the communities of these subjects. Conversely,
the faecal microbiota of Patient 2 was characterised by
great temporal variation in the distribution of active
bacteria (Fig. 2, Table S3b). For example, the Firmicutes/
Bacteroidetes ratio and the proportion of Proteobacteria
varied widely over time (from 0.26 to 4.10 and from 3%
to 88%, respectively). Also, the fraction of each bacterial
family experienced greater variation than in Control 1
and Patient 1 (see, for example, the fluctuations in the
amount of Clostridiaceae or Rikenellaceae over the followup). ANOSIM at the family level revealed that the median
rank of distances between samples of Patient 1 was four
times that of Control 1, and half of that found within
Patient 2. Thus, temporal instability in the microbiota was
associated with the IBS condition (greater in Patients than
in Control 1) and with severe diarrhoea (greater in Patient
2 than in Patient 1). The discrepancies between the taxonomic composition estimated from metagenomes and
from metatranscriptomes indicated a different contribution
Figure 3 shows the distribution of broad categories in the
KEGG pathway hierarchy. The encoded functions were
highly conserved between subjects and over time (within
a few days) within each subject. Temporal variation was
higher at the gene expression level, but lower than variation in the distribution of active microorganisms. Given
the different community assemblies found in each sample,
it supports the concept of functional redundancy among
faecal microorganisms. CA of the distribution of intermediate categories in the TIGRFAM and the KEGG pathway
hierarchies separated the metagenomic samples of Patient
1 and Patient 2, while plots of metatranscriptomic samples gave a picture similar to that found with the distribution of active bacteria (Fig. S4). It should be noted that
only a small number of sequences had a functional annotation in metatranscriptomes, so these results should be
interpreted with caution.
Although statistically significant, the few differentially
abundant functional features between and within patients
detected with LEfSe analysis are difficult to interpret considering the limited number of samples per group and
the rather low number of sequences per sample, which
also complicate the detection of significant changes (Table
S6). These limitations are more evident when we focus
on specific taxa, because the number of sequences within
each taxon was small.
ª 2013 Federation of European Microbiological Societies.
Published by John Wiley & Sons Ltd. All rights reserved
FEMS Microbiol Ecol 86 (2013) 581–589
Follow-up of faecal microbiota in IBS
585
Fig. 2. Relative abundance of microbial families in samples of Control 1, Patient 1 and Patient 2. Data were generated by taxonomic annotation
of 16S rRNA genes and transcripts. The sampling day is indicated below each column. When there are two samples from a given individual in
the same day, these are numbered after the day.
Discussion
Temporal variation in the structure and function of the
faecal microbiota was associated with the presence and
intensity of IBS symptoms. Relapse and remission of acute
diarrhoea occurred within short intervals and were associated with strong and quick changes in the microbiota of
Patient 2. The increased instability in the patients with IBS
could be reflecting the inability of the gut microbiota itself
to maintain its structure, which might contribute to symptom development, or the microbial alterations produced
by diarrhoea with the associated changes in motility and
luminal contents. Moreover, a high degree of temporal
variation is typical of re-establishing communities after
disturbance, as seen in the faecal microbiota of subjects
treated with antibiotics or dietary interventions or in
patients with recurrent Clostridium difficile–associated
FEMS Microbiol Ecol 86 (2013) 581–589
diarrhoea (Chang et al., 2008; Dethlefsen & Relman, 2011;
Wu et al., 2011).
We focused on the study of microbial activity at the
level of gene expression because there are few functional
studies on IBS and because we found greater variation
between and within subjects at this level than at the genomic level. Compositional shifts in the active fraction
of the microbiota characterised days with acute diarrhoea. Similarly, changes in the pattern of gene expression
were associated with worsening of symptoms. Unfortunately, we had a relatively small number of sequences
with a functional annotation in metatranscriptomes due
to methodological limitations (the difficulty to enrich
mRNAs prior to sequencing and the small length of nonrRNA sequences that makes difficult a confident assignment in homology searches). This leads to higher
uncertainty in the estimated distributions of functional
ª 2013 Federation of European Microbiological Societies.
Published by John Wiley & Sons Ltd. All rights reserved
586
A. Durb
an et al.
Fig. 3. Relative abundance of functional categories in the KEGG pathway hierarchy in samples of Control 1, Patient 1 and Patient 2. Data were
generated by functional annotation of protein coding genes and mRNAs. The sampling day is indicated below each column. When there are two
samples from a given individual in the same day, these are numbered after the day. Samples with < 200 sequences with an assigned functional
role are not shown.
categories, so these results should be interpreted with
caution.
Quantitatively, it is difficult to assess the influence of the
difference in the number of sequences per sample on the
analysis of similarities between samples. However, we
expect that it has little effect on our analyses based on relative abundances. Although the number of sequences is
important for the estimation of OTU richness, the estimation of relative abundances is in general less sensitive to
it (although the associated standard errors are obviously
larger for smaller samples). The smallest samples in metatranscriptomes (P1.3 in Patient 1 and P2.42 in Patient 2)
were quite similar according to the distribution of microbial families to the other samples taken on days with similar symptoms. Therefore, undersampling did not appear to
lead to a significant overestimation of dissimilarities.
ª 2013 Federation of European Microbiological Societies.
Published by John Wiley & Sons Ltd. All rights reserved
Diarrhoea per se may result in the alterations detected
in Patient 1 and Patient 2 on days with worse symptoms.
The high rate of purging may disrupt the anaerobic environment in the gut, leading to the displacement of commensal anaerobes, and wash down more bacteria from
the proximal regions of the gut, which have higher proportions of aerobes and facultative anaerobes than distal
regions (Hayashi et al., 2005). Previous analyses of the
faecal microbiota in sufferers from cholera and acute
diarrhoea have shown reduced levels of obligate anaerobes
and increases in facultative anaerobes (both commensal
and pathogenic bacteria) (Albert et al., 1978; Balamurugan et al., 2008; Monira et al., 2013). Accordingly, we
detected an overrepresentation of facultative anaerobes
within Proteobacteria and Streptococcaceae on days with
acute diarrhoea. However, it is important to note that we
FEMS Microbiol Ecol 86 (2013) 581–589
587
Follow-up of faecal microbiota in IBS
assessed the change in relative abundances of taxa comparing different samples, which does not necessarily
translate into absolute changes. Diarrhoea may also
increase the washout of mucosa-associated bacteria in the
colon. The Proteobacteria, Streptococcaceae, Clostridiaceae
and Verrucomicrobia detected in our surveys on days with
worse symptoms could represent at least in part bacteria
detached from the colonic mucosa, because the prevalence of these taxa seems to be higher in the colonic
mucosa than in faeces (Durban et al., 2011, 2012).
Besides, it has been repeatedly demonstrated an expansion of Enterobacteriaceae in unsubtyped IBS and diarrhoea-predominant IBS (Si et al., 2004; Krogius-Kurikka
et al., 2009; Carroll et al., 2012). We did not detect this
abnormality in our patients with IBS, but the levels of
unknown members of Alphaproteobacteria and Proteobacteria were unusually high. Interestingly, an enrichment in
Alphaproteobacteria in diarrhoea-predominant IBS sufferers compared with healthy controls has been reported
previously (Krogius-Kurikka et al., 2009).
In this study, the global distribution of active bacteria
discriminated Patient 2 from Control 1 and Patient 1.
The last two were of similar age and shared environmental factors, which most probably contributed to their differentiation from Patient 2. However, the mild symptoms
experienced by Patient 1 compared with Patient 2,
together with the large alterations in the microbiota of
Patient 2 concomitant with changes in symptom intensity, support that the singularities of Patient 2 were also
related to the disorder. The inclusion of single samples
from patients that were fairly asymptomatic at the time
of sampling might partly explain the failure of most of
the previous studies to discriminate IBS cases from controls on the basis of the global distribution of gut bacteria
(Salonen et al., 2010; Durban et al., 2012; Simren et al.,
2013). Besides, the analysis of the microbial activity
instead of the microbial composition may have helped to
differentiate our study subjects. Further studies should
follow more patients and over longer periods to increase
the chance of collecting samples that cover changes in
bowel symptoms and relapse and remission of acute disease. Moreover, it would be helpful to have a finer classification of patients based on the pattern of symptoms,
which can vary widely between patients and over time.
Cross-sectional studies on IBS to date have not found
consistent alterations in the gut microbiota and are sometimes contradictory (Salonen et al., 2010; Simren et al.,
2013). Similarly, the alterations we found associated with
acute symptoms are not systematic within a single patient.
Although our results need to be interpreted with caution
because of the limited sample size and they may also not be
extrapolated to IBS patients with other symptom patterns,
we consider it unlikely that dysbiosis is the underlying
FEMS Microbiol Ecol 86 (2013) 581–589
cause of the development of IBS symptoms. Other mechanisms may trigger the acute phases, for example stress. Animal studies suggest that psychological stress can change the
composition of the microbiota via perturbation of the normal gastrointestinal habitat (Collins & Bercik, 2009).
Besides, IBS sufferers tend to have a low threshold for coping with stressful situations and a high incidence of psychiatric comorbidity (Drossman, 1999; Hungin et al., 2005).
Thus, stress may promote the alterations in the gut function observed in IBS and, subsequently, the alterations in
the gut microbiota. We have proved that IBS is associated
with a decrease in the stability (this study) and a decrease
in the biodiversity of the gut microbiota (Durban et al.,
2012). Regardless of whether the community imbalances
are a cause or a consequence of the development of symptoms (a topic that warrants further research), treatments
that potentially counteract these attributes of the microbiota could be helpful in IBS.
Acknowledgements
This work was funded by Grants BFU2009-04501-E,
SAF2009-13032-C02-01 and SAF2012-31187 from Ministerio de Economıa y Competitividad, Spain, and Prometeo/2009/092 from Generalitat Valenciana to A.M. A.D. is
recipient of a fellowship from Instituto de Salud Carlos
III, Spain.
Authors’ contribution
A.L. and A.M. contributed equally to this work.
References
Albert MJ, Bhat P, Rajan D, Maiya PP, Pereira SM & Baker SJ
(1978) Faecal flora of south indian infants and young
children in health and with acute gastroenteritis. J Med
Microbiol 11: 137–143.
Altschul SF, Gish W, Miller W, Myers EW & Lipman DJ
(1990) Basic local alignment search tool. J Mol Biol 215:
403–410.
Balamurugan R, Janardhan HP, George S, Raghava MV,
Muliyil J & Ramakrishna BS (2008) Molecular studies
of fecal anaerobic commensal bacteria in acute diarrhea
in children. J Pediatr Gastroenterol Nutr 46: 514–519.
Basseri RJ, Weitsman S, Barlow GM & Pimentel M (2011)
Antibiotics for the treatment of irritable bowel syndrome.
Gastroenterol Hepatol 7: 455–493.
Carroll IM, Ringel-Kulka T, Siddle JP & Ringel Y (2012)
Alterations in composition and diversity of the intestinal
microbiota in patients with diarrhea-predominant irritable
bowel syndrome. Neurogastroenterol Motil 24: 521–530.
Chang JY, Antonopoulos DA, Kalra A, Tonelli A, Khalife WT,
Schmidt TM & Young VB (2008) Decreased diversity of the
ª 2013 Federation of European Microbiological Societies.
Published by John Wiley & Sons Ltd. All rights reserved
588
fecal microbiome in recurrent Clostridium difficile-associated
diarrhea. J Infect Dis 197: 435–438.
Collins SM & Bercik P (2009) The relationship between
intestinal microbiota and the central nervous system in
normal gastrointestinal function and disease.
Gastroenterology 136: 2003–2014.
Dethlefsen L & Relman DA (2011) Incomplete recovery and
individualized responses of the human distal gut microbiota
to repeated antibiotic perturbation. P Natl Acad Sci USA
108(suppl 1): 4554–4561.
Drossman DA (1999) Do psychosocial factors define symptom
severity and patient status in irritable bowel syndrome? Am
J Med 107: 41S–50S.
Duboc H, Rainteau D, Rajca S et al. (2012) Increase in fecal
primary bile acids and dysbiosis in patients with
diarrhea-predominant irritable bowel syndrome.
Neurogastroenterol Motil 24: 513–520.
Durban A, Abellan JJ, Jimenez-Hernandez N, Ponce M, Ponce
J, Sala T, D’Auria G, Latorre A & Moya A (2011) Assessing
gut microbial diversity from feces and rectal mucosa. Microb
Ecol 61: 123–133.
Durban A, Abellan JJ, Jimenez-Hernandez N, Salgado P, Ponce
M, Ponce J, Garrigues V, Latorre A & Moya A (2012)
Structural alterations of faecal and mucosa-associated
bacterial communities in irritable bowel syndrome. Environ
Microbiol Rep 4: 242–247.
Edgar RC (2010) Search and clustering orders of magnitude
faster than BLAST. Bioinformatics 26: 2460–2461.
Gosalbes MJ, Durban A, Pignatelli M, Abellan JJ,
Jimenez-Hernandez N, Perez-Cobas AE, Latorre A & Moya
A (2011) Metatranscriptomic approach to analyze the
functional human gut microbiota. PLoS One 6: e17447.
Hayashi H, Takahashi R, Nishi T, Sakamoto M & Benno Y
(2005) Molecular analysis of jejunal, ileal, caecal and
recto-sigmoidal human colonic microbiota using 16S rRNA
gene libraries and terminal restriction fragment length
polymorphism. J Med Microbiol 54: 1093–1101.
Hungin AP, Chang L, Locke GR, Dennis EH & Barghout V
(2005) Irritable bowel syndrome in the United States:
prevalence, symptom patterns and impact. Aliment
Pharmacol Ther 21: 1365–1375.
Kajander K, Myllyluoma E, Rajilic-Stojanovic M, Kyr€
onpalo S,
Rasmussen M, J€arvenp€a€a S, Zoetendal EG, de Vos WM,
Vapaatalo H & Korpela R (2008) Clinical trial: multispecies
probiotic supplementation alleviates the symptoms of
irritable bowel syndrome and stabilizes intestinal
microbiota. Aliment Pharmacol Ther 27: 48–57.
Krogius-Kurikka L, Lyra A, Malinen E, Aarnikunnas J,
Tuimala J, Paulin L, M€akivuokko H, Kajander K &
Palva A (2009) Microbial community analysis reveals
high level phylogenetic alterations in the overall
gastrointestinal microbiota of diarrhoea-predominant
irritable bowel syndrome sufferers. BMC Gastroenterol 9: 95.
Le Gall G, Noor SO, Ridgway K, Scovell L, Jamieson C,
Johnson IT, Colquhoun IJ, Kemsley EK & Narbad A
(2011) Metabolomics of fecal extracts detects altered
ª 2013 Federation of European Microbiological Societies.
Published by John Wiley & Sons Ltd. All rights reserved
A. Durb
an et al.
metabolic activity of gut microbiota in ulcerative
colitis and irritable bowel syndrome. J Proteome Res 10:
4208–4218.
Lewis SJ & Heaton KW (1997) Stool form scale as a useful
guide to intestinal transit time. Scand J Gastroenterol 32:
920–924.
Longstreth GF, Thompson WG, Chey WD, Houghton LA,
Mearin F & Spiller RC (2006) Functional bowel disorders.
Gastroenterology 130: 1480–1491.
M€att€
o J, Maunuksela L, Kajander K, Palva A, Korpela R,
Kassinen A & Saarela M (2005) Composition and temporal
stability of gastrointestinal microbiota in irritable bowel
syndrome - a longitudinal study in IBS and control subjects.
FEMS Immunol Med Microbiol 43: 213–222.
Maukonen J, Satokari R, M€att€
o J, S€
oderlund H,
Mattila-Sandholm T & Saarela M (2006) Prevalence and
temporal stability of selected clostridial groups in irritable
bowel syndrome in relation to predominant faecal bacteria.
J Med Microbiol 55: 625–633.
Moayyedi P, Ford AC, Talley NJ, Cremonini F, Foxx-Orenstein
AE, Brandt LJ & Quigley EM (2010) The efficacy of
probiotics in the treatment of irritable bowel syndrome: a
systematic review. Gut 59: 325–332.
Monira S, Nakamura S, Gotoh K et al. (2013) Metagenomic
profile of gut microbiota in children during cholera and
recovery. Gut Pathog 5: 1.
Ponnusamy K, Choi JN, Kim J, Lee SY & Lee CH (2011)
Microbial community and metabolomic comparison of
irritable bowel syndrome faeces. J Med Microbiol 60: 817–827.
Qin J, Li R, Raes J et al. (2010) A human gut microbial gene
catalogue established by metagenomic sequencing. Nature
464: 59–65.
Salonen A, de Vos WM & Palva A (2010) Gastrointestinal
microbiota in irritable bowel syndrome: present state and
perspectives. Microbiology 156: 3205–3215.
Salzberg SL, Delcher AL, Kasif S & White O (1998) Microbial
gene identification using interpolated Markov models.
Nucleic Acids Res 26: 544–548.
Segata N, Izard J, Waldron L, Gevers D, Miropolsky L, Garrett
WS & Huttenhower C (2011) Metagenomic biomarker
discovery and explanation. Genome Biol 12: R60.
Si JM, Yu YC, Fan YJ & Chen SJ (2004) Intestinal
microecology and quality of life in irritable bowel syndrome
patients. World J Gastroenterol 10: 1802–1805.
Simren M, Barbara G, Flint HJ, Spiegel BM, Spiller RC, Vanner
S, Verdu EF, Whorwell PJ, Zoetendal EG & Rome Foundation
Committee (2013) Intestinal microbiota in functional bowel
disorders: a Rome foundation report. Gut 62: 159–176.
Tana C, Umesaki Y, Imaoka A, Handa T, Kanazawa M &
Fukudo S (2010) Altered profiles of intestinal microbiota
and organic acids may be the origin of symptoms in irritable
bowel syndrome. Neurogastroenterol Motil 22: 512–519.
Wang Q, Garrity GM, Tiedje JM & Cole JR (2007) Naive
Bayesian classifier for rapid assignment of rRNA sequences
into the new bacterial taxonomy. Appl Environ Microbiol 73:
5261–5267.
FEMS Microbiol Ecol 86 (2013) 581–589
Follow-up of faecal microbiota in IBS
Wu GD, Chen J, Hoffmann C et al. (2011) Linking long-term
dietary patterns with gut microbial enterotypes. Science 334:
105–108.
Supporting Information
Additional Supporting Information may be found in the
online version of this article:
Fig. S1. PCA based on the symptoms on sampling days.
Fig. S2. DCA of the distribution of microbial families
estimated from the taxonomic affiliation of mRNAs in
the metatranscriptomes of Control 1, Patient 1, and
Patient 2.
Fig. S3. Relative abundance of microbial families in samples of Control 1, Patient 1, and Patient 2. Data were
generated by taxonomic annotation of protein coding
genes and mRNAs.
Fig. S4. CA of the distribution of KEGG metabolic pathways (a,c) and TIGRFAM functional roles (b,d) in the
metagenomes (a,b) and metatranscriptomes (c,d) of
Control 1, Patient 1, and Patient 2.
FEMS Microbiol Ecol 86 (2013) 581–589
589
Table S1. Intestinal symptons of Patient 1 (P1) and
Patient 2 (P2) in the days of sampling, the previous days,
and the subsequent ones.
Table S2. Characteristics of the metagenomic (DNA) and
metatranscriptomic (cDNA) libraries from the faecal
microbial communities analysed in this study.
Table S3. Relative abundance of microbial families in
samples of Control 1 and Patient 1 (a), and Patient 2 (b).
Table S4. Odds ratios (OR) for the significant differences
detected in chi-square tests in the relative abundance
of bacterial families between metatranscriptomes and
metagenomes sampled on the same day.
Table S5. Odds ratios (OR) for the significant differences
detected in chi-square tests in the relative abundance of
bacterial families between the metatranscriptomes of
Patient 1 (P1) or Patient 2 (P2) on days with severe
symptoms and days with milder symptoms.
Table S6. Significant differences detected in LEfSe analyses
in the relative abundance of functional categories between
the metatransciptomes of Patient 1 (P1) and Patient 2
(P2), and between the metatranscriptomes of Patient 2 on
days with severe and mild/moderate symptoms.
ª 2013 Federation of European Microbiological Societies.
Published by John Wiley & Sons Ltd. All rights reserved