A randomized controlled trial of fetal endoscopic tracheal occlusion
advertisement

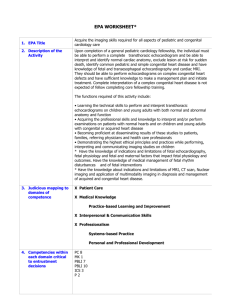
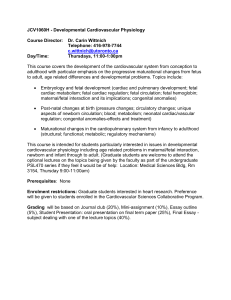
Ultrasound Obstet Gynecol 2012; 39: 20–27 Published online 14 December 2011 in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/uog.10142 A randomized controlled trial of fetal endoscopic tracheal occlusion versus postnatal management of severe isolated congenital diaphragmatic hernia R. RUANO*†, C. T. YOSHISAKI*, M. M. DA SILVA‡, M. E. J. CECCON§, M. S. GRASI§, U. TANNURI‡ and M. ZUGAIB* *Department of Obstetrics and Gynecology, Faculdade de Medicina, Universidade de São Paulo, São Paulo, Brazil; †Texas Children’s Fetal Center and the Department of Obstetrics and Gynecology, Baylor College of Medicine, Houston, TX, USA; ‡Department of Pediatric Surgery, Faculdade de Medicina, Universidade de São Paulo, São Paulo, Brazil; §Department of Neonatology, Faculdade de Medicina, Universidade de São Paulo, São Paulo, Brazil K E Y W O R D S: congenital diaphragmatic hernia; fetal abnormalities; fetal surgery; FETO; fetoscopy; prenatal diagnosis; pulmonary hypertension; pulmonary hypoplasia ABSTRACT Objective Severe pulmonary hypoplasia and pulmonary arterial hypertension are associated with reduced survival in congenital diaphragmatic hernia (CDH). We aimed to determine whether fetal endoscopic tracheal occlusion (FETO) improves survival in cases of severe isolated CDH. Methods Between May 2008 and July 2010, patients whose fetuses had severe isolated CDH (lung-to-head ratio < 1.0, liver herniation into the thoracic cavity and no other detectable anomalies) were assigned randomly to FETO or to no fetal intervention (controls). FETO was performed under maternal epidural anesthesia supplemented with fetal intramuscular anesthesia. Tracheal balloon placement was achieved with ultrasound guidance and fetoscopy between 26 and 30 weeks of gestation. All cases that underwent FETO were delivered by the EXIT procedure. Postnatal therapy was the same for both treated fetuses and controls. The primary outcome was survival to 6 months of age. Other maternal and neonatal outcomes were also evaluated. Results Twenty patients were enrolled randomly to FETO and 21 patients to standard postnatal management. The mean gestational age at randomization was similar in both groups (P = 0.83). Delivery occurred at 35.6 ± 2.4 weeks in the FETO group and at 37.4 ± 1.9 weeks in the controls (P < 0.01). In the intention-to-treat analysis, 10/20 (50.0%) infants in the FETO group survived, while 1/21 (4.8%) controls survived (relative risk (RR), 10.5 (95% CI, 1.5–74.7), P < 0.01). In the receivedtreatment analysis, 10/19 (52.6%) infants in the FETO group and 1/19 (5.3%) controls survived (RR, 10.0 (95% CI, 1.4–70.6) P < 0.01). Conclusion FETO improves neonatal survival in cases with isolated severe CDH. Copyright 2011 ISUOG. Published by John Wiley & Sons, Ltd. INTRODUCTION Congenital diaphragmatic hernia (CDH) can be diagnosed accurately by second-trimester ultrasound examination1 . Despite all efforts, morbidity and mortality in cases diagnosed prenatally remain high and are thought to be related to the severity of pulmonary hypoplasia and pulmonary arterial hypertension (PAH)2 . Many studies have shown that a complicated neonatal course and/or mortality are related to decreased fetal lung size observed on ultrasound or magnetic resonance imaging, the presence of herniated liver and decreased pulmonary vascularity3 – 12 . For severe forms, fetal tracheal occlusion has been suggested as a therapeutic option, since this procedure has been shown to stimulate fetal lung growth in both animal models and humans13 – 15 . Harrison et al.16 published a randomized study in human fetuses with CDH, in which fetal tracheal occlusion was performed, by means of maternal laparotomy followed by fetoscopy using standard laparoscopic instrumentation. Patients in the tracheal occlusion arm of the study experienced a high Correspondence to: Dr R. Ruano, Universidade de São Paulo, Faculdade de Medicina, Obstetrics Department, São Paulo, Brazil, Av. Dr. Enéias de Carvalho Aguiar, 255, 10◦ andar, Obstetrı́cia, São Paulo, Brazil, CEP 05403-900 (e-mail: rodrigoruano@usp.br) Accepted: 4 October 2011 Copyright 2011 ISUOG. Published by John Wiley & Sons, Ltd. RANDOMIZED CONTROLLED TRIAL Fetoscopic tracheal occlusion in severe CDH rate of preterm premature rupture of the membranes and preterm delivery, which probably influenced the lack of benefit reported. Furthermore, CDH cases of moderate severity were included in the trial, which may similarly have affected findings. More recently, a minimal access approach to tracheal occlusion was performed, with the introduction of a smaller diameter fetoscope placed percutaneously under ultrasound guidance, a procedure called ‘fetal endoscopic tracheal occlusion’ (FETO)13,16,17 . A European group published the results of the first 210 cases of severe CDH that underwent FETO using a 1.2-mm fetoscope. Their findings suggested that this technique may be associated with a substantial improvement in perinatal survival, with a low rate of complications14 . Our group recently published a pilot study of 17 fetuses that underwent FETO using a 1.0-mm fetoscope, and described the feasibility and probable benefit of this fetal intervention for severe CDH18 . However, there has been no randomized trial that confirms the benefits of FETO for severe isolated CDH. In the present randomized trial, we investigated the efficacy of FETO for the treatment of severe isolated CDH. PATIENTS AND METHODS 21 Figure 1 Fetoscope insertion prior to fetal endoscopic tracheal occlusion. (a) Percutaneous insertion of the slightly curved 2.7-mm sheath into the amniotic cavity under ultrasound guidance. (b) Insertion of the 1.0-mm fetoscope inside the cannula after removing the trocar. Study design Between May 2008 and July 2010, a randomized controlled trial was conducted in a tertiary center at the University of São Paulo in São Paulo, Brazil. The protocol was approved by the Institutional Review Board of the University of São Paulo (CAPPesq 1087/07) and followed the CONSORT Statement19 . Women presenting with a singleton pregnancy between 22 and 26 weeks’ gestation and with fetal CDH were considered for the trial. Patients were evaluated with comprehensive fetal ultrasound, magnetic resonance imaging and echocardiography and underwent amniocentesis for karyotyping. Those meeting the following inclusion criteria were offered enrolment in the trial: no detectable fetal anomalies other than CDH; normal karyotype; fetal lung-to-head ratio (LHR) < 1.020,21 ; and at least one third of the fetal liver herniated into the thoracic cavity as estimated by ultrasound4,22,23 . Other fetal ultrasonographic characteristics recorded were: observed/expected LHR (o/e-LHR) < 0.2524 ; observed/expected total lung volume (o/e-TotFLV) < 0.3510 and contralateral pulmonary vascular index < 25%7 . All patients underwent extensive counseling, and those who met the inclusion criteria and agreed to participate provided written informed consent for both randomization and treatment. Patients who agreed to participate in the study were assigned randomly to receive FETO or prenatal expectant management in a ratio of 1 : 1 using a computer-generated randomization scheme. Fetal endoscopic tracheal occlusion (FETO) FETO was performed under maternal epidural anesthesia between 26 and 30 weeks’ gestation by one of three operators (R.R., C.T.Y., M.M.S.), following a well-established Copyright 2011 ISUOG. Published by John Wiley & Sons, Ltd. protocol. Adjunct fetal anesthesia involved fentanyl (15 µg/kg) and pancuronium (2 mg/kg) administration according to the sonographic estimated fetal weight. Medications were administered intramuscularly into the fetal arm using a 22-gauge needle under ultrasound guidance18 . A specially designed, slightly curved operating sheath, with a diameter of 2.7 mm, a working channel 1.3 mm in diameter and a lower channel 1.2 mm in diameter for the fetoscope, was introduced percutaneously into the amniotic cavity under guidance by conventional twodimensional ultrasound (Figure 1a). Inside the amniotic cavity, the trocar was withdrawn and the 1.0-mm fetoscope (11 510 A, Karl Storz, Tuttlingen, Germany) was inserted (Figure 1b)15 . The cannula with the fetoscope was advanced through the fetal mouth, over the epiglottis (Figure 2a) and finally through the vocal cords (Figure 2b) into the trachea. After identifying the carina, a catheter loaded with a detachable balloon (GOLDBALL 4, Balt Extrusion, Montmorency, France) was positioned just proximal to the bifurcation of the main stem bronchi (Figure 2c). The balloon was inflated with 0.8 mL saline solution and detached from the catheter (Figure 2d) and its position inside the fetal trachea was confirmed by ultrasonography. Prophylactic tocolysis in the form of intravenous Atosiban (Tractocile, Antocin, Ferring Pharmaceuticals, Malmo, Sweden) was administered according to our institution’s standard protocol: 6.75 mg (one ampule) was administered immediately before the procedure, over a 1-min period; followed by two ampules (13.50 mg) diluted in 90 mL saline solution administrated at a rate of 24 mL/h in the first 3 h, then 8 mL/h for 3.5 h25 . A prophylactic 2-g dose of intravenous cephalotin (a first-generation cephalosporin) was given to the patients Ultrasound Obstet Gynecol 2012; 39: 20–27. 22 Ruano et al. Figure 2 Fetal endoscopic tracheal occlusion. Advancement of the cannula with the fetoscope over the epiglottis (a) and the vocal cords (b) to the fetal trachea and positioning of the balloon just proximal to the bifurcation of the main stem bronchi (c). (d) Balloon inflation inside the fetal trachea. This is followed by confirmation of its location by ultrasonography. every 6 h for 24 h. All patients stayed in the city for further monitoring until the time of delivery. Ultrasound examination was performed every 2 weeks until delivery. Perinatal management All fetuses in the FETO group were delivered by EXIT (ex-utero intrapartum therapy) procedure to allow for the controlled removal of the tracheal balloon at a planned gestational age of 38 weeks. Briefly, maternal general anesthesia was initiated and a hysterotomy was performed, taking care to minimize maternal bleeding. After delivery of the fetal head and while the fetus remained on placental bypass, bronchoscopy was performed to remove the balloon and to insert an endotracheal tube. The umbilical cord was then cut. Controls were delivered by planned Cesarean section at 38 weeks’ gestation in order to avoid bias from the method of delivery, which could interfere with neonatal outcome. All neonates were treated according to the same protocol26,27 . Briefly, in the delivery room they were intubated immediately, with placement of a nasogastric tube, and then admitted to the neonatal intensive care unit. Immediate ventilator support was started, with Copyright 2011 ISUOG. Published by John Wiley & Sons, Ltd. the fraction of inspired oxygen (FiO2 ) progressively adjusted to achieve a preductal saturation > 80%. Central venous access was obtained in all cases. Sedation was not used routinely. High-frequency oscillatory ventilation was started if persistent hypoxemia and hypercapnia were observed on conventional ventilation. The treatment protocol did not include extracorporeal membrane oxygenation (ECMO), either pre- or postoperatively, as this treatment modality is not available at our institution. Surfactant was not used routinely. Inhaled nitric oxide (iNO) was administered in cases of PAH verified by a pre- to postductal saturation difference > 10% and confirmed by echocardiography. Hemodynamic support was achieved by volume expansion and administration of dobutamine (10–20 µg/kg/min) and norepinephrine, when necessary (0.5–2 µg/kg/min). CDH repair was only performed after preoperative respiratory and hemodynamic stabilization. Stabilization was defined by the following criteria: (a) normal hemodynamic variables (mean blood pressure > 40 mmHg, urine output > 2 mL/kg/h), without inotropic agents; (b) absence of pre- to postductal saturation difference and signs of PAH during echocardiography, without iNO; and (c) a switch to conventional mechanical ventilation that was well-tolerated, with moderate values of peak inspiratory Ultrasound Obstet Gynecol 2012; 39: 20–27. Fetoscopic tracheal occlusion in severe CDH 23 pressure (15–20 cmH2 O) and adequate oxygenation, achieved with FiO2 ≤ 40%. 57 patients referred for evaluation 14 not eligible 2 did not provide consent Outcomes and statistical analysis The primary outcome was survival to 6 months of age. Additional outcomes were maternal complications, the presence of postnatal severe PAH and length of time to surgical repair of the diaphragmatic defect. Severe PAH was defined when elevated pulmonary pressure (judged by right to left or bidirectional shunting) was verified by echocardiography or a there was a persistent difference in pre- to postductal saturation gradient > 20%28,29 . The sample size for the study was calculated considering the primary outcome (infant survival rate) based on our pilot study18 . An infant survival rate of 5–10% in cases with severe CDH receiving standard neonatal care and an infant survival rate of 40–60% in cases with severe CDH treated with FETO were used for this calculation. A twotailed type I error of 5% and a power of 90% were used to determine that a sample size of 19 fetuses per group would be necessary. The trial was monitored regularly after delivery of each case by an independent data safety committee. Since we had performed a previous pilot study, no interim analysis was planned during the trial due to the small sample size. Analyses were performed using the intention-to-treat principle. The data were analyzed using Student’s t, Mann–Whitney U, chi-square and Fisher’s exact tests and Kaplan–Meier survival analysis with Cox proportional hazard model. Relative risks (RR) were also calculated. Differences were considered to be statistically significant when P < 0.05. RE SULTS During the study period, a total of 57 women with fetal CDH were referred for evaluation, of whom 41 met the inclusion criteria and gave written informed consent (Figure 3). Twenty patients were assigned randomly to the FETO group and 21 to postnatal care alone. Three 41 underwent randomization 20 assigned to FETO (intention-to-treat analysis) 21 assigned to no fetal intervention (intention-to-treat analysis) 1 declined planned treatment based on randomization 19 included in FETO group (received-treatment analysis) 2 declined planned treatment based on randomization 19 included in no fetal intervention group (received-treatment analysis) Figure 3 Flow diagram of patients with severe isolated congenital diaphragmatic hernia enrolled into the study. FETO, fetal endoscopic tracheal occlusion. patients (one in the FETO group and two in the standard neonatal treatment group) declined planned treatment based on randomization. These three patients did not receive the same antenatal and neonatal management as the remaining patients in the trial. They had limited follow-up, including infant survival – all three died in the neonatal period. Thus, 19 fetuses with severe CDH successfully underwent FETO and 19 fetuses received the standard care (controls). For the intention-to-treat analysis, in the FETO group there were 15 left-sided CDH cases and five right-sided cases; in the control group there were 15 left-sided and six right-sided cases. The two groups did not differ in this or any other characteristic (Tables 1 and S1). In this series, the mean duration of the FETO procedure was 17.3 ± 8.3 min, which was significantly shorter than that of our previous series18 (27.7 ± 8.3 min; P < 0.01). Table 1 Sample characteristics of study groups: fetuses with severe isolated congenital diaphragmatic hernia randomized to receive fetal endoscopic tracheal occlusion (FETO) or to no prenatal intervention (controls) in the intention-to-treat analysis Characteristic GA at randomization (weeks) Maternal age (years) Parity Nulliparous Parous LHR o/e-LHR o/e-TotFLV Contralateral VI (%) Laterality of diaphragmatic defect Left-sided Right-sided FETO group (n = 20) Controls (n = 21) P 25.3 ± 3.8 (21–26) 29.5 ± 6.6 (18–41) 25.5 ± 3.5 (21–26) 30.3 ± 6.4 (20–38) 0.83 0.85 0.76 12 (60.0) 8 (40.0) 0.80 ± 0.11 0.18 ± 0.02 0.26 ± 0.05 11.3 ± 4.5 12 (57.1) 9 (42.9) 0.79 ± 0.10 0.17 ± 0.06 0.27 ± 0.04 12.3 ± 4.5 15 (75.0) 5 (25.0) 15 (71.4) 6 (28.6) 0.77 0.85 0.39 0.60 0.99 Data given as mean ± SD (range), mean ± SD or n (%). GA, gestational age; LHR, lung-to-head ratio; o/e, observed/expected; TotFLV, total fetal lung volume; VI, pulmonary vascular index. Copyright 2011 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2012; 39: 20–27. Ruano et al. 24 Table 2 Obstetric outcomes in fetuses with severe isolated congenital diaphragmatic hernia randomized to receive fetal endoscopic tracheal occlusion (FETO) or to no prenatal intervention (controls) in the intention-to-treat analysis Obstetric outcome Maternal death Maternal blood transfusion Abruption Maternal infection PPROM < 37 weeks PPROM < 32 weeks Preterm delivery < 37 weeks Preterm delivery < 32 weeks GA at delivery (weeks) FETO group (n = 20) Controls (n = 21) 0 0 0 1 (5.0)* 7 (35.5) 4 (20.0) 10 (50.0) 3 (15.0) 35.6 ± 2.4 (31–38) 0 0 0 0 5 (23.8) 2 (9.5) 6 (28.6) 0 37.4 ± 1.9 (33–40) P — — — — 0.51 0.41 0.21 0.11 < 0.01 Data given as n (%) or mean ± SD (range). *Chorioamnionitis after preterm premature rupture of membranes (PPROM). Table 3 Infant outcome in cases of severe isolated congenital diaphragmatic hernia which as fetuses were randomized to receive fetal endoscopic tracheal occlusion (FETO) or to no prenatal intervention (controls) in the intention-to-treat analysis Infant survival to 6 months Severe pulmonary arterial hypertension FETO group (n = 20) (n (%)) Controls (n = 21) (n (%)) P Relative risk (95% CI) 10 (50.0) 10 (50.0) 1 (4.8) 18 (85.7) < 0.01 0.02 10.5 (1.5–74.7) 0.6 (0.4–0.9) The balloon was initially placed successfully inside the fetal trachea using a single entry into the uterus in all cases, including the seven patients with anterior placenta, which did not require a transplacental fetoscopic entry. Correct placement was confirmed by ultrasound examination. In two cases, the balloon ruptured after introducing it into the fetal trachea and a second balloon was placed correctly through the fetoscope without additional entry into the uterus. Since our cannula had an independent working channel, the balloon could be replaced without removing the cannula from its position inside the fetal trachea. The balloon was identified 6 weeks after FETO in all 16 cases that delivered more than 6 weeks after the procedure. The balloon was removed in all infants during EXIT procedure; in two of these cases reduced inflation was noted (13.3%). There were no immediate intraoperative complications. Obstetric outcomes are shown in Tables 2 and S2. Preterm premature rupture of the membranes < 32 weeks and < 37 weeks were not significantly different between FETO and control groups. Patients delivered at an earlier mean gestational age in the FETO group compared with controls (P < 0.01); however, the frequencies of prematurity (delivery < 37 weeks) and extreme prematurity (delivery < 32 weeks) were not significantly different between the two groups. All cases in the FETO group (received-treatment analysis) were delivered by EXIT procedure; 14 (73.7%) cases were planned procedures (10 at 37–38 weeks and four at 34–36 weeks after PROM) and five (26.3%) cases were emergency EXIT procedures due to the onset of preterm contractions. In the control group, all patients were delivered by Cesarean section; 15 Copyright 2011 ISUOG. Published by John Wiley & Sons, Ltd. Cumulative proportion surviving Infant outcome 1.0 0.8 0.6 0.4 0.2 0.0 0 20 40 60 80 100 120 140 160 180 Days of age Figure 4 Kaplan–Meier survival plot for intention-to-treat analysis, showing cumulative proportion surviving from birth, in infants which had undergone fetal endoscopic tracheal occlusion for severe , n = 20) isolated congenital diaphragmatic hernia ( compared with controls which received no prenatal intervention , n = 21) (P < 0.01). ( (78.9%) cases were planned deliveries and four (21.1%) cases were emergency sections (P = 0.70). In the intention-to-treat analysis, 10 of 20 (50.0%) infants in the FETO group survived, while 1/21 (4.8%) controls survived (P < 0.01; RR, 10.5 (95% CI, 1.5–74.7)) (Table 3 and Figure 4). The frequency of severe PAH was significantly lower in the FETO group compared with controls (50.0% vs. 85.7%, P = 0.02). In the received-treatment analysis (Table S3), among the neonates that had postnatal surgical repair (12 in the FETO group and four in the control group, P = 0.02), hemodynamic stabilization occurred earlier in the FETO group than it did in controls (P < 0.01). A prosthetic Ultrasound Obstet Gynecol 2012; 39: 20–27. Fetoscopic tracheal occlusion in severe CDH patch was used in 13 of the 16 (81.3%) infants that underwent postnatal repair. In the control group, two infants died after surgery secondary to heart failure related to severe pulmonary hypertension and another died secondary to pneumonia. The sole surviving infant in the control group was discharged home without needing any respiratory support. In the FETO group, one infant died after postnatal surgical repair due to heart failure caused by severe pulmonary hypertension. Another infant died due to aspiration pneumonia secondary to megaesophagus caused by severe esophageal reflux. None of the survivors in the FETO group needed respiratory support after discharge. In one case, fundoplication was performed before discharge due to severe esophageal reflux. The mean age at hospital discharge among the survivors in the FETO group was 34.7 ± 5.7 (range, 28–48) days. The laterality of the CDH lesion was not associated statistically with outcome. The overall infant survival rates among the left-sided CDH and right-sided CDH cases in the FETO group were 8/15 (53.3%) and 2/5 (40.0%), respectively (P = 0.38, intention-to-treat analysis). In cases of left-sided CDH, the survival rate in the FETO group was better than that of the controls (53.3% vs 6.7%, P < 0.01; RR, 8.0 (95% CI, 1.1–56.3)). In cases of right-sided CDH, FETO again appeared to be associated with an increased chance of survival compared with controls although this difference was not statistically significant (40.0% vs 0%, P = 0.08; RR, 5.8 (95% CI, 0.3–99.2)). DISCUSSION We found that FETO improved survival for fetuses with severe isolated CDH compared with cases that received only postnatal intensive care that is standard in our country (50% vs 4.8%). However, the survival rates in our present series for both antenatally treated and non-treated groups were considerably lower when compared to a previous randomized study16 . This difference could be explained by the more rigorous criteria of CDH severity used in the present study. In the previous randomized study16 , inclusion criteria were LHR < 1.4 and liver herniation, while in our study only fetuses with LHR < 1.0 and liver herniation were included. Our results are very similar to those of a European cohort, which reported a 50% rate of neonatal survival after FETO13,14 . The inclusion criteria in that study were similar to those in our current investigation. Our previous pilot study18 demonstrated that FETO was feasible using a fetoscope of smaller diameter (1 mm) than has been reported previously. In that earlier series, placental abruption occurred in one case following FETO and hemorrhage into the amniotic cavity occurred in another. Both complications occurred in patients in which there was inadvertent transplacental placement of the trocar. In our current randomized study, we avoided inserting the trocar through or near the placenta. The duration of the fetal procedure was significantly reduced compared Copyright 2011 ISUOG. Published by John Wiley & Sons, Ltd. 25 with our initial series18 . These findings demonstrate a clear learning curve for the procedure. However, despite the use of a small-diameter fetoscope and a reduced size of the trocar, FETO was still associated with a high incidence of prematurity (50.0%), extreme prematurity (15.0%) and preterm premature rupture of the membranes (35.0%). The incidence of these complications was significantly lower compared with a previously published randomized trial that used maternal laparotomy and 5.0-mm diameter trocars, in which the incidence of prematurity was 73% and that of preterm rupture of the membranes was 100%16 . On the other hand, our incidence of premature complications was very similar to those reported in the European cohort of 210 cases that underwent FETO using a 1.2-mm fetoscope and a 3.2-mm trocar. In that series, the median gestational age at delivery was 35 weeks, the incidence of extreme prematurity was 17.1% and that of preterm premature rupture of the membranes was 47.1%14 . In our present study we used a larger balloon (GOLDBALL 4) in comparison to our previous pilot study18 , in which we used the GOLDBALL 2. The main difference between these two balloons is the diameter after inflation. The GOLDBALL 2 should be inflated with 0.6 mL saline solution to reach an inflated diameter and length of 7 mm and 20 mm, respectively. The GOLDBALL 4 can be inflated with a maximum 0.8 mL volume, leading to an inflated diameter and length of 9 mm and 16 mm, respectively. We changed to the largerdiameter balloon after our pilot study based on our experience with frequent rupture of the smaller-diameter balloon during inflation as well as a reduced rate of retention of the inflated balloon after placement. We noted in our pilot study that the balloon was no longer inflated after 5–6 weeks in almost two thirds of cases and hypothesized that a larger balloon would result in a more occlusive effect and a greater incidence of retention. This hypothesis was confirmed by our current finding that, after the prescribed 6-week period of retention, the balloon was identified in all 16 fetuses that had not already delivered. The FETO procedure apparently improves survival by enhancing pulmonary growth as a consequence of fetal tracheal occlusion30,31 . Some experimental studies suggest that fetal tracheal occlusion may also improve pulmonary vascularity32 , which may reduce the risk of severe PAH. In our present study, the frequency of severe PAH was significantly lower in cases that underwent FETO. However, further studies are necessary to demonstrate conclusively the beneficial effects of FETO on pulmonary growth and vasculature response. One criticism of this study is related to the fact that the balloon was removed at the time of delivery through an EXIT procedure. Other groups have recommended removal of the balloon prior to delivery to improve neonatal outcome30 . Experimental research in a sheep model for CDH has revealed that reversal of tracheal occlusion prior to delivery allows recovery of type II pneumocytes33,34 . Current guidelines for FETO include placement between 26 and 30 weeks’ gestation, with removal 6 weeks later13 . Ultrasound Obstet Gynecol 2012; 39: 20–27. Ruano et al. 26 A recent study suggested that the release of tracheal occlusion at least 24 h before delivery was associated with improved neonatal outcome30 . However, there are insufficient data that provide information on the optimal duration of tracheal occlusion in humans. Perhaps the main advantage of removing the tracheal balloon before delivery is avoidance of the need for an emergency EXIT procedure, which occurred in 26% of our cases. Another possible criticism is that our cases were not managed after birth with ECMO. The use of ECMO in the management of CDH is controversial and its true benefits have not been proven conclusively35 – 38 . One systematic review including 21 retrospective studies and three randomized controlled trials indicated that ECMO improves short-term neonatal survival (RR, 0.73 (95% CI, 0.54–0.98), P = 0.04), but not long-term survival (RR, 0.83 (95% CI, 0.66–1.05), P = 0.12)37 . A more recent Cochrane review found that ECMO improved shortterm neonatal survival (RR, 0.73 (95% CI, 0.55–0.99), P = 0.03), but not long-term survival (RR, 0.84 (95% CI, 0.67–1.10), P = 0.13)38 . In our study, all infants that survived to discharge were alive at 6 months of age. ECMO has been associated with other long-term morbidities, including neurological and respiratory complications37,38 . Larger studies in centers that provide ECMO are needed to determine if FETO can reduce the need for ECMO and its associated morbidities. We did not use laterality of the diaphragmatic defect to stratify patients before randomization. In general, right sided-CDH is considered more severe because these cases have a greater amount of herniated liver and smaller lung volumes. However, in our series, the laterality of the CDH did not appear to influence the survival rate after FETO. In conclusion, FETO improves infant survival in isolated severe CDH. However, the risk of prematurity and preterm premature rupture of membranes was high, despite the use of small-diameter fetoscopes. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. ACKNOWLEDGMENTS We thank Dr Kenneth Moise Jr. for his great contribution to the revision and analysis of the data as well as editing of the English text. We also thank Dr Michael A. Belfort for revision and editing of the manuscript. The present study was funded by the CNPq (Conselho Nacional de Desenvolvimento de Pesquisa e Tecnologia do Brasil). SISNEP CAAE - 0926.0.015.000-07 (April 2008) ClinicalTrials.gov Identifier: NCT01302977 (Feb 2011). 13. 14. 15. RE FERENCES 1. Bétrémieux P, Lionnais S, Beuchée A, Pladys P, Le Bouar G, Pasquier L, Loeuillet-Olivo L, Azzis O, Milon J, Wodey E, Frémond B, Odent S, Poulain P. Perinatal management and outcome of prenatally diagnosed congenital diaphragmatic hernia: a 1995–2000 series in Rennes University Hospital. Prenat Diagn 2002; 22: 988–994. 2. Beck C, Alkasi O, Nikischin W, Engler S, Caliebe A, Leuschner I, von Kaisenberg CS. Congenital diaphragmatic hernia, etiology Copyright 2011 ISUOG. Published by John Wiley & Sons, Ltd. 16. 17. and management, a 10-year analysis of a single center. Arch Gynecol Obstet 2008; 277: 55–63. Balassy C, Kasprian G, Brugger PC, Weber M, Csapo B, Herold C, Prayer D. Assessment of lung development in isolated congenital diaphragmatic hernia using signal intensity ratios on fetal MR imaging. Eur Radiol 2010; 20: 829–837. Cannie M, Jani J, Chaffiotte C, Vaast P, Deruelle P, HoufflinDebarge V, Dymarkowski S, Deprest J. Quantification of intrathoracic liver herniation by magnetic resonance imaging and prediction of postnatal survival in fetuses with congenital diaphragmatic hernia. Ultrasound Obstet Gynecol 2008; 32: 627–632. Jani JC, Peralta CF, Ruano R, Benachi A, Done E, Nicolaides KH, Deprest JA. Comparison of fetal lung area to head circumference ratio with lung volume in the prediction of postnatal outcome in diaphragmatic hernia. Ultrasound Obstet Gynecol 2007; 30: 850–854. Mahieu-Caputo D, Sonigo P, Dommergues M, Fournet JC, Thalabard JC, Abarca C, Benachi A, Brunelle F, Dumez Y. Fetal lung volume measurement by magnetic resonance imaging in congenital diaphragmatic hernia. BJOG 2001; 108: 863–868. Ruano R, Aubry MC, Barthe B, Mitanchez D, Dumez Y, Benachi A. Quantitative analysis of fetal pulmonary vasculature by 3-dimensional power Doppler ultrasonography in isolated congenital diaphragmatic hernia. Am J Obstet Gynecol 2006; 195: 1720–1728. Ruano R, Aubry MC, Barthe B, Mitanchez D, Dumez Y, Benachi A. Predicting perinatal outcome in isolated congenital diaphragmatic hernia using fetal pulmonary artery diameters. J Pediatr Surg 2008; 43: 606–611. Ruano R, Aubry MC, Dumez Y, Zugaib M, Benachi A. Predicting neonatal deaths and pulmonary hypoplasia in isolated congenital diaphragmatic hernia using the sonographic fetal lung volume-body weight ratio. AJR Am J Roentgenol 2008; 190: 1216–1219. Ruano R, Benachi A, Joubin L, Aubry MC, Thalabard JC, Dumez Y, Dommergues M. Three-dimensional ultrasonographic assessment of fetal lung volume as prognostic factor in isolated congenital diaphragmatic hernia. BJOG 2004; 111: 423–429. Ruano R, Bunduki V, Silva MM, Yoshizaki CT, Tanuri U, Macksoud JG, Zugaib M. Prenatal diagnosis and perinatal outcome of 38 cases with congenital diaphragmatic hernia: 8-year experience of a tertiary Brazilian center. Clinics (Sao Paulo) 2006; 61: 197–202. Cruz-Martinez R, Moreno-Alvarez O, Hernandez-Andrade E, Castañon M, Done E, Martinez JM, Puerto B, Deprest J, Gratacos E. Contribution of intrapulmonary artery Doppler to improve prediction of survival in fetuses with congenital diaphragmatic hernia treated with fetal endoscopic tracheal occlusion. Ultrasound Obstet Gynecol 2010; 35: 572–577. Deprest J, Gratacos E, Nicolaides KH. Fetoscopic tracheal occlusion (FETO) for severe congenital diaphragmatic hernia: evolution of a technique and preliminary results. Ultrasound Obstet Gynecol 2004; 24: 121–126. Jani JC, Nicolaides KH, Gratacós E, Valencia CM, Doné E, Martinez JM, Gucciardo L, Cruz R, Deprest JA. Severe diaphragmatic hernia treated by fetal endoscopic tracheal occlusion. Ultrasound Obstet Gynecol 2009; 34: 304–310. Ruano R, Okumura M, Zugaib M. Four-dimensional ultrasonographic guidance of fetal tracheal occlusion in a congenital diaphragmatic hernia. J Ultrasound Med 2007; 26: 105–109. Harrison MR, Keller RL, Hawgood SB, Kitterman JA, Sandberg PL, Farmer DL, Lee H, Filly RA, Farrell JA, Albanese CT. A randomized trial of fetal endoscopic tracheal occlusion for severe fetal congenital diaphragmatic hernia. N Engl J Med 2003; 349: 1916–1924. Deprest J, Breysem L, Gratacos E, Nicolaides K, Claus F, Debeer A, Smet MH, Proesmans M, Fayoux P, Storme L. Tracheal side effects following fetal endoscopic tracheal occlusion Ultrasound Obstet Gynecol 2012; 39: 20–27. Fetoscopic tracheal occlusion in severe CDH 18. 19. 20. 21. 22. 23. 24. 25. 26. for severe congenital diaphragmatic hernia. Pediatr Radiol 2010; 40: 670–673. Ruano R, Duarte SA, Pimenta EJ, Takashi E, da Silva MM, Tannuri U, Zugaib M. Comparison between fetal endoscopic tracheal occlusion using a 1.0-mm fetoscope and prenatal expectant management in severe congenital diaphragmatic hernia. Fetal Diagn Ther 2011; 29: 64–70. Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. J Pharmacol Pharmacother 2010; 1: 100–107. Lipshutz GS, Albanese CT, Feldstein VA, Jennings RW, Housley HT, Beech R, Farrell JA, Harrison MR. Prospective analysis of lung-to-head ratio predicts survival for patients with prenatally diagnosed congenital diaphragmatic hernia. J Pediatr Surg 1997; 32: 1634–1636. Metkus AP, Filly RA, Stringer MD, Harrison MR, Adzick NS. Sonographic predictors of survival in fetal diaphragmatic hernia. J Pediatr Surg 1996; 31: 148–151; discussion 51–52. Bretelle F, Mazouni C, D’Ercole C, Chaumoitre K, Chau C, Desbrieres R. Fetal lung-head ratio measurement in the evaluation of congenital diaphragmatic hernia. J Pediatr Surg 2007; 42: 1312–1313; author reply 3–4. Hedrick HL, Danzer E, Merchant A, Bebbington MW, Zhao H, Flake AW, Johnson MP, Liechty KW, Howell LJ, Wilson RD, Adzick NS. Liver position and lung-to-head ratio for prediction of extracorporeal membrane oxygenation and survival in isolated left congenital diaphragmatic hernia. Am J Obstet Gynecol 2007; 197: 422.e1–4. Jani J, Nicolaides KH, Keller RL, Benachi A, Peralta CF, Favre R, Moreno O, Tibboel D, Lipitz S, Eggink A, Vaast P, Allegaert K, Harrison M, Deprest J; Antenatal-CDH-Registry Group. Observed to expected lung area to head circumference ratio in the prediction of survival in fetuses with isolated diaphragmatic hernia. Ultrasound Obstet Gynecol 2007; 30: 67–71. Cabar FR, Bittar RE, Gomes CM, Zugaib M. [Atosiban as a tocolytic agent: a new proposal of a therapeutic approach]. Rev Bras Ginecol Obstet 2008; 30: 87–92. Datin-Dorriere V, Walter-Nicolet E, Rousseau V, Taupin P, Benachi A, Parat S, Hubert P, Revillon Y, Mitanchez D. Experience in the management of eighty-two newborns with congenital diaphragmatic hernia treated with high-frequency oscillatory ventilation and delayed surgery without the use of extracorporeal membrane oxygenation. J Intensive Care Med 2008; 23: 128–135. 27 27. Mitanchez D. [Antenatal treatment of congenital diaphragmatic hernia: an update]. Arch Pediatr 2008; 15: 1320–1325. 28. Greenough A, Khetriwal B. Pulmonary hypertension in the newborn. Paediatr Respir Rev 2005; 6: 111–116. 29. Roofthooft MT, Bergman KA, Waterbolk TW, Ebels T, Bartelds B, Berger RM. Persistent pulmonary hypertension of the newborn with transposition of the great arteries. Ann Thorac Surg 2007; 83: 1446–1450. 30. Cannie MM, Jani JC, De Keyzer F, Allegaert K, Dymarkowski S, Deprest J. Evidence and patterns in lung response after fetal tracheal occlusion: clinical controlled study. Radiology 2009; 252: 526–533. 31. Peralta CF, Jani JC, Van Schoubroeck D, Nicolaides KH, Deprest JA. Fetal lung volume after endoscopic tracheal occlusion in the prediction of postnatal outcome. Am J Obstet Gynecol 2008; 198: 60.e1–5. 32. Cruz-Martinez R, Moreno-Alvarez O, Prat J, Krauel L, Tarrado X, Castañón M, Hernandez-Andrade E, Albert A, Gratacos E. Lung tissue blood perfusion changes induced by in utero tracheal occlusion in a rabbit model of congenital diaphragmatic hernia. Fetal Diagn Ther 2009; 26: 137–142. 33. Benachi A, Dommergues M, Delezoide AL, Bourbon J, Dumez Y, Brunnelle F. Tracheal obstruction in experimental diaphragmatic hernia: an endoscopic approach in the fetal lamb. Prenat Diagn 1997; 17: 629–634. 34. Bratu I, Flageole H, Laberge JM, Chen MF, Piedboeuf B. Pulmonary structural maturation and pulmonary artery remodeling after reversible fetal ovine tracheal occlusion in diaphragmatic hernia. J Pediatr Surg 2001; 36: 739–744. 35. Reiss I, Schaible T, van den Hout L, Capolupo I, Allegaert K, van Heijst A, Gorett Silva M, Greenough A, Tibboel D; CDH EURO Consortium. Standardized postnatal management of infants with congenital diaphragmatic hernia in Europe: the CDH EURO Consortium consensus. Neonatology 2010; 98: 354–364. 36. Mitchell IC, Garcia NM, Barber R, Ahmad N, Hicks BA, Fischer AC. Permacol: a potential biologic patch alternative in congenital diaphragmatic hernia repair. J Pediatr Surg 2008; 43: 2161–2164. 37. Morini F, Goldman A, Pierro A. Extracorporeal membrane oxygenation in infants with congenital diaphragmatic hernia: a systematic review of the evidence. Eur J Pediatr Surg 2006; 16: 385–391. 38. Mugford M, Elbourne D, Field D. Extracorporeal membrane oxygenation for severe respiratory failure in newborn infants. Cochrane Database Syst Rev 2008; CD001340. SUPPORTING INFORMATION ON THE INTERNET The following supporting information may be found in the online version of this article: Tables S1–S3 Sample characteristics (Table S1), obstetric outcome (Table S2) and infant outcome (Table S3) in fetuses with severe isolated congenital diaphragmatic hernia randomized to receive fetal endoscopic tracheal occlusion (FETO) or to no prenatal intervention (controls) in the received-treatment analysis. Copyright 2011 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2012; 39: 20–27.