Psychometric evaluation of the Cognitive Appraisal
advertisement

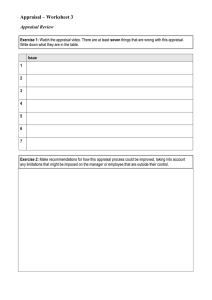
M E T H O D O L O G I C A L I S S UE S I N N U R S I N G R E S E A R C H Psychometric evaluation of the Cognitive Appraisal of Health Scale with patients with prostate cancer Muayyad M. Ahmad BSc MSc PhD Assistant Professor, Faculty of Nursing, University of Jordan, Amman, Jordan Submitted for publication 24 July 2003 Accepted for publication 7 May 2004 Correspondence: Muayyad Ahmad, Faculty of Nursing, University of Jordan, Amman, Jordan. E-mail: mma4@ju.edu.jo Journal of Advanced Nursing 49(1), 78–86 Psychometric evaluation of the Cognitive Appraisal of Health Scale with patients with prostate cancer Aim. This study was designed to investigate the psychometric properties of the Cognitive Appraisal of Health Scale, specifically with prostate cancer patients. Background. Measurement of appraisal is considered a relatively new area in the health studies literature. Cognitive appraisal of potentially stressful events becomes important when individuals face a crisis such as a change in their health status. So far, confirmatory factor analysis (CFA) has not been used to study the factor structure of the Cognitive Appraisal of Health Scale. Methods. The structure of the questionnaire was analysed by exploratory factor analysis, CFA using structural equation modelling and an Analysis of Moment Structure procedure with a sample of 133 patients with prostate cancer. Results. The results support the three-factor model for the Cognitive Appraisal of Health Scale because it has robust structure and excellent goodness-of-fit indices. Several of the 23 items were grouped into different factors from those in Kessler’s scale. Conclusion. The use of the reduced version of Cognitive Appraisal of Health Scale with men under health stress is recommended. AHMAD M.M. (2005) Keywords: Cognitive Appraisal of Health Scale, appraisal, prostate cancer, nursing, confirmatory factor analysis Introduction Cognitive appraisal Cognitive appraisal is the process by which an individual evaluates or judges a potentially stressful event for meaning and significance to their own well-being (Lazarus & Folkman 1984). Cognitive appraisal of potentially stressful events becomes important when people face crises such as a change in their health status; however, cognitive appraisal has not been well studied (Kessler 1998). In cognitive appraisal, a person evaluates the effect of an encounter with the environment on their well-being. Such an appraisal has three forms: (1) irrelevant, when the encounter with the environment has 78 no effect on well-being, (2) benign-positive, when the encounter with the environment is perceived as positive and (3) stressful. Additionally, there are three types of stress appraisal: (a) harm or loss, referring to damage already experienced, whether from an illness or damage to the self or social esteem; (b) threat, referring to harm or loss that has not yet occurred but is anticipated and (c) challenge, when the appraisal provides an opportunity for growth, mastery, or gain (Coyne et al. 1981, Lazarus & Folkman 1984, Lazarus 1998). Lazarus and Folkman (1984) described the meaning of stress in terms of appraisal; in their study, they asked whether the stress-inducing event was perceived as a harm/loss, threat, or challenge, and whether or not it was perceived as controllable. 2005 Blackwell Publishing Ltd Methodological issues in nursing research Psychometric evaluation of the CAHS When people face a potentially stressful situation, such as a cancer diagnosis, cognitive appraisal is carried out by the mental operations of thinking and reasoning (Lazarus & Folkman 1984). Several studies report that a cancer diagnosis is usually appraised as a stressful event that poses a threat greater than that of other serious diseases (Krause 1991, Lev 1992). In a study examining how cancer patients coped with their disease, Krause (1991) reported that 82 such patients (68%) described their feelings in response to the diagnosis as horror, shock, terror, surprise, anger, a sense of time standing still, emptiness, a sense of unreality, punishment and fate. In a study of patient strategies for adapting to a cancer diagnosis, Lev (1992) reported that this can be associated with pain, disfigurement, and death. Thus, patient reactions to a cancer diagnosis tend to be very intense, with profound psychological reactions such as shock, disbelief, denial, anger, sadness, depression and grief (Frank-Stromborg 1989, Fawzy 1995). However, these responses in previous studies need to be evaluated with appraisal measurements that are specific to the type of appraisal used in each situation., since Lazarus and Folkman (1984) reported that each type of appraisal is expected to stimulate different types of coping strategies. No reports were found in the literature about how prostate cancer patients appraise their diagnosis and its treatment consequences. addition to this setting limitation, the author did not establish validity of this scale. Mishel and Sorenson (1991) used the 15-item appraisal scale that was a part of the Ways of Coping Checklist (Folkman 1984). They collapsed the four appraisal subscales of threat, challenge, harm, and benign/irrelevant into two categories of danger and opportunity. These two scales limit the measurement of primary appraisal only to the emotional responses encountered in stressful events. Another scale, the Appraisal of Caregiving Scale (ACS) was developed by Oberst et al. (1989) to measure the extent to which cancer patient caregivers perceive the intensity of the illness/caregiving situation as a threat, challenge, harm/loss, or benign. The ACS reflects the construct of primary appraisal; however, its use is limited to studies of caregiver stress. The literature is inconsistent when it comes to assessing the necessity for coping in a situation appraised as irrelevant or benign positive. According to Lazarus and Folkman (1984), when an event is appraised as in this way, it does not require coping. When a diagnosis of cancer is appraised as stressful, it will evoke a number of responses (Menaghan 1982, Folkman & Lazarus 1988). On the contrary, Kessler (1998) considered that, even under non-stressful situations, coping occurs under benign/irrelevant appraisals. Therefore, the Cognitive Appraisal of Health Scale (CAHS) as developed by Kessler includes all types of appraisals and is arguably more comprehensive. Measurement of appraisal The instrument Measurement of appraisal is considered a relatively new area of study, as most of appraisal scales were developed only within the past 15 years. A number of researchers are responsible for defining the field of study. Gass (1988), in his study, used one question to assess appraisal of bereavement, and reported that this question was developed based on Lazarus and Folkman’s theoretical perspective because there were no other measures of appraisal available. However, evaluating individuals’ appraisal using a single category or item is not appropriate because primary appraisal is considered a multidimensional concept (Kessler 1998). Oberst et al. (1991) developed the Appraisal of Illness Scale (AIS) to study stress appraisal in cancer patients in relation to threat, loss, financial strain, and overall stressfulness; however, the validity and reliability of the AIS are not reported. In order to measure stress appraisal, Kammer (1994) has reviewed the work of Folkman and Lazarus to establish the Emotion Appraisal of Nursing Home Placement Tool (EANH). This was developed to assess how family members think about the nursing home placement of their elders. In The need for an instrument to measure appraisals by individuals with a variety of potentially stressful healthrelated events led to the construction of the CAHS (Kessler 1998). In the early development stages of the primary appraisal portion of the CAHS, the scale consisted of 27 items derived from theoretical literature on appraisal and from other existing instruments on appraisal. The 27-item cognitive appraisal was administered to a convenience sample of 201 women at 0Æ3–21 years after diagnosis with breast cancer (Kessler 1998). The ages of the participants ranged from 29 to 82 years. Participants were asked to respond to each item according to their appraisal of their health status. The 27 items with four separate scales measure the cognitive appraisal dimensions of threat, challenge, harm/loss and benign/irrelevant. All items are scored on a 5-point Likert scale from 1 (strongly disagree) to 5 (strongly agree). Higher scores indicate more agreement with the appraisal item or scale. Four out of five items in the CAHS were developed by Folkman et al. (1986); three of these four items represent the coping options associated with threat, challenge and harm/loss. Appraisals and cancer diagnosis 2005 Blackwell Publishing Ltd, Journal of Advanced Nursing, 49(1), 78–86 79 M.M. Ahmad The fourth item was added by Kessler (1998) to the instrument to represent the coping options associated with a benign/ irrelevant appraisal. However, the Benign/irrelevant appraisal showed no effect on the outcome variables (coping and health status) in a prostate cancer study (Bjorck et al. 1999). In addition, the CAHS as developed by Kessler (1998) is still considered a new instrument to measure cognitive appraisal; therefore, further examinations of the instrument were needed. The CAHS as developed by Kessler (1998) depended solely on exploratory factor analysis (EFA). However, EFA is primarily useful at the early stages of analysis (Tabachnick & Fidell 2001). Scales are developed from the items loading high together on the same factor while loading low on all other factors (Hair et al. 1998). In addition, exploratory factor models do not provide any explicit test statistics for assessing convergent and discriminant validity (O’LearyKelly & Vokurka 1998). Nothing was found in the literature about how prostate cancer patients appraise their diagnosis and its treatment consequences. The stability of a newly developed instrument, such as the CAHS, with different gender and different diagnosis merits further examination. Participants The convenience sample for the study was composed of 133 patients, recruited from two university-affiliated hospitals, where they were diagnosed with and treated for prostate cancer. The eligibility criteria were men of any age: (a) who had been diagnosed with prostate cancer and (b) with any stage of prostate cancer. Any patient with a cancer diagnosis other than prostate cancer, except where it was secondary to prostate cancer, was excluded. After obtaining informed consent, data were collected via mailed questionnaires. A total of 146 men completed and returned their packets, but 13 were excluded because they had other types of cancer. The demographic characteristics of the participants are shown in Table 1. Instrument The CAHS used in this study has 27 items, and responses are made using a 5-point Likert scale from 1 (strongly disagree) to 5 (strongly agree). Higher scores indicate more agreement with the appraisal item or scale. Confirmatory factor analysis Confirmatory factor analysis (CFA) is a relatively recent technique that is rapidly replacing the more traditional technique of EFA because it allows more precise testing of an instrument’s factor structure. CFA provides a theory-driven method for addressing construct validity by assigning the items in an instrument to their respective factors according to theoretical expectations (Aluja et al. 2003). Moreover, CFA enables the researcher to evaluate the reliability of the instrument in an approach that differs from traditional assessment of internal consistency (e.g. Cronbach’s alpha) through partialling out the measurement error (Munro 2001). CFA also enables the researcher to investigate the factor structures of the instrument across groups. For example, to examine gender differences between this study and the original study by Kessler (1998) in the factor structure of CAHS, CFA can be used to determine whether the structure changes or is invariant across groups. So far, CFA has not been used to study the factor structure of the CAHS as obtained by EFA. The study Purpose The purpose of this study was to use exploratory and CFA to evaluate the appropriateness of the CAHS in examining how prostate cancer patients appraise their diagnosis. 80 Ethical considerations Ethical approval was granted by the Research Ethics Committees of the study hospitals. The purpose, risks and benefits were explained to recruits before they decided to Table 1 Demographic Characteristics’ of the Participants (n ¼ 133) Characteristic Age Range Mean (SD ) Race White Non-white Marital status Married Single, divorced, widower, separated Education High school or less College graduate Graduate school Employment status Full-time Part-time Retired Income Inadequate Adequate Very adequate n (%) 47–91 66Æ3 (9Æ1) 115 (86Æ0) 18 (14Æ0) 107 (80Æ5) 26 (19Æ5) 46 (34Æ6) 61 (45Æ9) 26 (19Æ5) 49 (36Æ8) 8 (6Æ0) 76 (57Æ2) 13 (9Æ8) 85 (63Æ9) 35 (26Æ3) 2005 Blackwell Publishing Ltd, Journal of Advanced Nursing, 49(1), 78–86 Methodological issues in nursing research participate. They were assured that their participation was completely voluntary and that they could discontinue it at any time without affecting their current or future relationship with the treating hospital and/or physician. Results A principal components analysis with Varimax rotation for the prostate cancer patients’ cognitive appraisal was performed with the original 23 items of the CAHS as presented by Kessler (1998). Forcing a four-factors solution, 53Æ84% of the total variance was explained (Table 2). The bolded items under Factor 1, in comparison with Kessler’s (1998) model, include variables from benign/irrelevant appraisal (a15, a28, a23, a5), items from threat appraisal (a17, a18), and an item from harm/loss appraisal (a25). The bolded items under Factor 2 are close to the items loaded in Kessler’s scale under harm/loss appraisal beside the item (a25). The bolded items under Factor 3, in comparison with Kessler’s model, refer to threat appraisal (a6, a7) and challenge Psychometric evaluation of the CAHS appraisal (a2). The bolded items under Factor 4 refer to challenge appraisal in Kessler’s model in addition to item (a2). Determining the number of factors to be extracted depends on how strongly and cleanly the variables load on the factors, so the analyst may decrease or increase the number of factors (Youngblut 1993). The variable will load strongly in a particular factor if loading ‡0Æ40, and is considered clean if the absolute difference between the loading is more than 0Æ20 (Nunnally & Bernstein 1994). It is obvious that many items had non-clean loading (a25, a5, a9, a10, a14). Consistent with the Lazarus and Folkman (1984) theoretical model from which the CAHS was drawn, the benign/ irrelevant factor was deleted and further exploratory factor analyses were conducted on a three-factor model. Accordingly, non-clean loading items were deleted from the model (a7, a6, a2, a28, a25, a14), and other items were re-allocated to other factors to fit the theoretical meaning (a5, a23), as scores were reversed. In addition, one item (a15) was deleted because of its redundancy with another item (a17), leaving the model with 16 items. Table 2 Exploratory factor analysis of the CAHS four-factor model, 23 items with patients with prostate cancer Principal components with Varimax rotation Items Factor 1 Factor 2 Factor 3 Factor 4 a17. I have a lot to lose because of this health problem a15. I have nothing to lose because of this health problem a18. I worry about what will happen to me a28. This health problem doesn’t affect my life a23. I don’t think much about this health problem a4. The health problem is frightening to me a25. I have been hurt by this health problem a5. This health problem isn’t stressful to me a13. I have a sense of loss over the things I can no longer do a9. I have lost interest in the things around me a8. This health problem has damaged my life a3. I have not been able to do what I want to do because of this health problem a19. Relationships with my family and friends have suffered a21. I have been harmed in some way by this health problem a10. I have had to give up a great deal because of this health problem a6. Things will only get worse because of this health problem a7. This health problem will not go well a2. This health problem won’t get me down a26. There is a lot I can do to overcome this health problem a11. I can beat this health problem despite the difficulties a24. This health problem has caused me to learn more about myself a1. I can control what will happen to me a14. I feel I can handle this health problem % Variance* Cumulative variance 0Æ70 0Æ68 0Æ67 0Æ66 0Æ66 0Æ57 0Æ55 0Æ45 0Æ27 0Æ16 0Æ26 0Æ16 0Æ12 0Æ32 0Æ14 0Æ16 0Æ19 0Æ31 0Æ20 0Æ15 0Æ19 0Æ10 0Æ16 0Æ17 0Æ13 0Æ26 0Æ31 0Æ17 0Æ29 0Æ18 0Æ12 0Æ10 0Æ54 0Æ15 0Æ74 0Æ65 0Æ69 0Æ68 0Æ62 0Æ60 0Æ51 0Æ21 0Æ10 0Æ26 0Æ13 0Æ23 0Æ21 15Æ94 15Æ94 0Æ11 15Æ76 31Æ70 0Æ30 0Æ17 0Æ46 0Æ18 0Æ28 0Æ12 0Æ51 0Æ70 0Æ67 0Æ67 0Æ17 0Æ25 0Æ36 0Æ21 0Æ35 0Æ41 11Æ70 43Æ40 0Æ13 0Æ18 0Æ77 0Æ71 0Æ61 0Æ52 0Æ51 10Æ45 53Æ85 *Percentage of the variance accounted for each factor. Rotation Sums of Squared Loadings. items load < 0Æ10. Loading not clean. 2005 Blackwell Publishing Ltd, Journal of Advanced Nursing, 49(1), 78–86 81 M.M. Ahmad Confirmatory factor analysis is a special application of structural equation modelling (SEM), making it important to screen data for multivariate normality when performing CFA (Hair et al. 1998). The multivariate normality of the data was examined by conducting normality checks by using Analysis of Moment Structure (AMOS 5.0) software (Arbuckle 2003). Normality is usually rejected if the ratio of kurtosis is higher than ±2 and/or skewness is higher than ±1, which indicates a distribution that departs significantly from normality (Nunnally & Bernstein 1994). The skewness for items a9, a10, and a24 were 1Æ68, 3Æ49 and 1Æ02 respectively. Kurtosis for item a9 was 2Æ78 and for item a10 was 20Æ32. Thus, three items (a9, a10, a24) were dropped from the model. Table 3 shows the most interpretable form of the factor analysis that was performed with the remaining 13 items and three factors that have the maximum variance accounted for (55Æ48%). Table 3 Exploratory factor analysis of the three-factor model of the Cognitive Appraisal of Health Scale 13 items Principal components with Varimax rotation Items a13 a3 a8 a21 a19 a23 a18 a4 a17 a5 a11 a1 a26 % Variance* Cumulative variance Harm/loss Threat 0Æ82 0Æ76 0Æ65 0Æ63 0Æ60 0Æ18 0Æ22 0Æ14 0Æ18 0Æ21 0Æ32 0Æ17 0Æ22 0Æ73 0Æ72 0Æ68 0Æ67 0Æ55 34 20Æ80 20Æ80 Challenge 13 25 23 14 14 0Æ82 0Æ77 0Æ73 15Æ14 55Æ48 -0Æ21 19Æ54 41Æ34 *Percentage of the variance accounted for each factor. Rotation Sums of Squared Loadings. Items load < 0Æ10. The Kaiser–Meyer–Oklin (KMO) is a measure that provides an approach to comparing the zero-order correlations to the partial correlations between pairs of variables (Munro 2001). The KMO in the 13-item three factors model is 0Æ82; Kaiser (1974) stated that if KMO is >0Æ50 it is acceptable. The closer the KMO to one, the better the correlations between pairs of variables that can be explained by the other variables (Norusis 1998). Bartlett’s Test of Sphericity evaluates all factors together and each factor separately against a hypothesis stating that there are no factors (Tabachnick & Fidell 2001). The Bartlett’s Test in this study is significant (P < 0Æ001), indicating that enough shared variance is present. Item-total correlation refers to a correlation of an item or indicator with the composite score (total) of all the items forming the same construct. Items from a given scale exhibiting item-total correlations <0Æ50 are usually candidates for deletion (Hair et al. 1998). All items in the three subscales of CAHS demonstrated item-total correlations between 0Æ62 and 0Æ82. Confirmatory factor analysis was carried out over the variance–covariance matrix for the 23-item, 16-item and 13item three-factor models through the AMOS 5.0 statistical package (Arbuckle 2003). The estimation method was the Maximum Likelihood. In order to achieve model identification, regression coefficients of the error terms over the endogenous variables were fixed to 1. The CFA was performed in order to determine whether the hypothesized statistical model fitted the actual data set, and a number of ‘goodness-of-fit’ statistics were used on the three factor models derived by means of EFA (Table 4). A non-significant chi-square result is an indication of fit because the researcher seeks to confirm the null hypothesis (i.e. the model fits the data well) (Byrne 1994). However, the chi-square goodness of fit is inadvisable because it is greatly influenced by sample size and violation of multivariate normality (Joreskog & Sorbom 1993, Wang et al. 1996). Therefore, chi-square statistics should not be the only method used for drawing conclusions about data-model fit (Bollen & Long 1993). Other commonly used fit statistics include the goodness of fit index (GFI), comparative fit index (CFI), and Models v2 d.f. P v2/d.f. GFI AGFI CFI IFI RMSEA M1 M2 M3 476Æ51 154Æ04 64Æ26 224 101 62 <0Æ01 <0Æ01 0Æ40 2Æ13 1Æ53 1Æ03 0Æ75 0Æ87 0Æ93 0Æ69 0Æ83 0Æ90 0Æ76 0Æ90 0Æ99 0Æ76 0Æ91 0Æ99 0Æ09 0Æ06 0Æ02 Table 4 Goodness-of-Fit Indices for three models in the prostate cancer patients sample v2/d.f., relative chi-square; GFI, goodness of fit index; AGFI, adjusted GFI; CFI, comparative fit index; IFI, increment fit index; RMSEA, root mean square error of approximation; M1, four factors (23 items); M2, three factors (16 items); M3, three factors (13 items). 82 2005 Blackwell Publishing Ltd, Journal of Advanced Nursing, 49(1), 78–86 Methodological issues in nursing research incremental fit index (IFI), all with a range 0–1 and with values >0Æ90 indicating a good fit. CFI is recommended over GFI because it is less influenced by sample size (Wang et al. 1996). The root mean square of approximation (RMSEA) of 0Æ05 or less indicates a ‘close fit’, while values of more than 0Æ1 justify rejecting the model (Browne & Cudeck 1989). Therefore, it is best to consider a variety of fit indices so that the weaknesses of a particular index are counteracted by the strength of another (March et al. 1996). The goodness-of-fit indices of the 23-item model were very poor in general terms (Table 4). The 16-item model obtained from the second EFA (includes item a9, a10 and a24) yielded fit indices slightly better than the previous model. According to chi square results, both of these models were rejected. The 13-item model yielded highly acceptable indices in all respects. Therefore, the goodness-of-fit indicators support the three factors 13-item model to measure the cognitive appraisal. Confirmatory factor analysis involves the specification and estimation of one or more hypothesized models of factors structure, each of which proposes a set of factors (latent variables) to account for covariance among a set of observed variables. SEM can be used to test the fit of a hypothesized model against the sample data. Using CFA to evaluate the appropriateness of the CAHS in examining how patients with prostate cancer appraise their diagnosis provides construct validity for the instrument by assigning the items to their respective factors according to theoretical expectations. Following the convention of AMOS analysis (Arbuckle 2003), observed indicators (items) are enclosed in rectangles. Latent variables (factors) are enclosed in circles, whereas measurement errors are enclosed in ellipses. Referring to Figure 1, the structural model is identified by three interrelated constructs (Threat, Challenge and Harm/Loss) connected to each other with double-headed arrows representing a pattern of intercorrelations. The single-headed arrows leading from the latent constructs to the boxes are regression paths representing the link between the factors and their respective set of observed variables; these coefficients represent factor loadings. Finally, the single-headed arrows pointing from ellipses to rectangles represent measurement error associated with observed variables. The Harm/Loss factor (five items) describes the damage that has already occurred as perceived by patients with prostate cancer, such as ‘This health problem has damaged my life’ and ‘I have a sense of loss over the things I can no longer do’. The Threat factor (five items) describes the harm Psychometric evaluation of the CAHS 0·62 0·72 Threat 0·60 a17 a18 a4 0·59 0·46 a23 a5 0·38 e17 0·52 e18 0·36 e4 0·35 e23 0·22 e5 –0·25 0·77 0·68 0·62 Challenge a26 e11 0·33 e1 0·39 e21 a3 0·37 e3 a13 0·56 a8 0·46 a19 0·38 a1 –0·48 0·61 Harmless a21 0·75 0·68 0·62 e26 0·46 a11 0·57 0·63 0·59 e13 e8 e19 Figure 1 Standardized estimates for the 13-item three-factor structure. or loss anticipated by the patients that has not yet occurred, such as ‘I worry about what will happen to me’ and ‘The health problem is frightening to me’. The Challenge factor (three items) involves a judgment made by the patients that demands associated with a stressful encounter can be met and overcome, such as ‘I can control what will happen to me’ and ‘There is a lot that I can do to overcome this health problem’. The Cronbach’s alphas for the 13-item three-factors model of CAHS in the present study were 0Æ79 for harm/ loss appraisal, 0Æ74 for threat appraisal, 0Æ70 for challenge, and 0Æ70 for the total scale. Internal validity of the CAHS three-factor model was established by principal component factor analysis. Construct validity is confirmed through SEM by examining the standardized regression coefficients in the regression of observed variables on latent variables. The evidence that the measured variables or factors represent the underlying constructs becomes stronger when the factor loadings or coefficients, as compared with their corresponding t-values, become larger (Bollen 1989). As shown in Table 5, all the items had t-values above 4Æ23 (P < 0Æ01) which means that the three-factor model has strong constructs. 2005 Blackwell Publishing Ltd, Journal of Advanced Nursing, 49(1), 78–86 83 M.M. Ahmad Table 5 Parameter estimates, error terms, and t-values for the threefactor model Latent variable Unstandardized Standardized Error Item factor loading factor loading term t-values* Harm/loss a13 a19 a8 a21 a3 1Æ29 0Æ72 1Æ13 1 1Æ12 0Æ75 0Æ62 0Æ68 0Æ63 0Æ61 0Æ20 0Æ13 0Æ19 0Æ20 6Æ42 5Æ65 6Æ09 a 5Æ53 Threat a18 a17 a4 a23 a5 1Æ13 1 0Æ99 1Æ03 0Æ73 0Æ72 0Æ62 0Æ60 0Æ59 0Æ46 0Æ20 5Æ65 0Æ19 0Æ20 0Æ17 5Æ24 5Æ19 4Æ23 Challenge a26 a11 a1 1 0Æ73 0Æ90 0Æ77 0Æ68 0Æ57 0Æ14 0Æ20 5Æ08 4Æ53 *t-values >2Æ58 considered significant at the 0Æ01 level. Indicates a parameter fixed at 1Æ0 in the original solution. Discussion The measurement of unobserved (latent) variables is considered a recent phenomenon in nursing research. Most available empirical research in nursing has been exploratory in nature and has borrowed its methods extensively from other fields, such as psychology and sociology. Traditional exploratory techniques have been used to provide preliminary scales and assess measurement properties. These techniques are useful in the early stages of empirical enquiry where theoretical models do not exist and the basic purpose is exploration. Exploratory methods can help in developing hypothesized measurement models, which subsequently can be tested via confirmatory analytic technique. None of the EFA techniques employed to assess the psychometric properties of scales tests unidimensionality. Unidimensionality can be defined as the existence of one latent trait or construct underlying a set of measures (Koufteros 1999). CFA affords a stricter interpretation of unidimensionality than can be provided by EFA (O’Leary-Kelly & Vokurka 1998), thus providing different conclusions about the acceptability of the instrument. According to Kessler (1998), the CAHS was used in her study because it measures the multiple dimensions of appraisals associated with the diagnosis of breast cancer and its treatment consequences. However, further evaluation was needed for the instrument because, although it was derived from the Lazarus and Folkman (1984) transactional model, it was not consistent with that model. Kessler (1998) assumed that cognitive appraisal would be initiated 84 from non-stressful events as well as stressful ones. As evidence of this inconsistency with Kessler’s assumption, a study that aimed to measure how patients with prostate cancer appraise their diagnosis, the benign/irrelevant appraisal was found to have no effects on any of the outcome measures (Bjorck et al. 1999). This result is consistent with what Lazarus and Folkman (1984) reported, namely that coping strategies are stimulated when an event is appraised as stressful (threat, harm/loss, and or challenge) but not as benign/irrelevant. A three-factor solution was chosen for this study. The widely accepted assumption of parsimony (Kim & Mueller 1978) supports this decision. Furthermore, Nunnally and Bernstein (1994) suggest that each factor needs at least three items, and the three factors have met this criterion. Moreover, in the Principal Components with Varimax rotation, the three factor model accounted for more than half of the variance (55Æ48%). Our results show that the reduced version of 13 items improves the validity. Furthermore, internal consistency coefficients were acceptable in the reduced version. Therefore, we consider that it would be advisable to recommend using the reduced version model of CAHS, especially with people experiencing a stressful health encounter. Conclusion A cancer diagnosis is still associated with a life-threatening disease by many people. However, different types of cancer induce different levels of fear among individuals (American Cancer Society 1996). When informed that they have prostate cancer, patients may view this as a threat to their lives. However, in terms of appraisal, men in the present study identified threat appraisal with less frequency than appraisals of harm/loss or challenge. It is likely that the high survival rate among and long survival time for patients with prostate cancer make living with the disease less threatening than doing so with other types of cancer having lower cure rates and/or shorter life expectancies. Although prostate cancer treatment leaves some permanent sexual and urological sideeffects (Davison et al. 1995), the overall effects of the disease, beyond the obvious complications, may influence how patients estimate the threat level presented by their prostate cancer. In order to help their patients, nurses need to develop an understanding of how prostate cancer diagnosis affects people’s appraisal of their situation. Thus, nurses need to help patients perceive the disease in ways that are less threatening or less associated with harm/loss and work to empower patients with information to face the disease as a 2005 Blackwell Publishing Ltd, Journal of Advanced Nursing, 49(1), 78–86 Methodological issues in nursing research What is already known about this topic • Measurement of appraisal is a relatively new area in the health studies literature. • Cognitive appraisal of potentially stressful events becomes important when individuals face a crisis such as a change in their health status. • Confirmatory factor analysis has not been used to study the factor structure of the Cognitive Appraisal of Health Scale. What this paper adds • Confirmatory factor analysis for the factor structure of the Cognitive Appraisal of Health Scale did not support the previous four-factor model. • Exploratory factor analysis and confirmatory factor analysis indicated that the 13-item scale is better than the 23-item scale in measuring the cognitive appraisals of patients with prostate cancer. • The three-factor model is parsimonious, valid, reliable, and empirically supported, and supports the work on cognitive appraisal derived from the transactional model of Lazarus and Folkman. challenge. Detailed analyses of appraisal, such as that in this study, will facilitate this. Acknowledgements I am indebted to the University of Jordan, approval number (184/2001–2002) for funding, and acknowledge the support of the Deanship of Academic Research at the university. The invaluable contributions of Dr Elizabeth Madigan and Mr Rafat Qahoush are also appreciated. References Aluja A., Garcia O. & Garcia L. (2003) Psychometric properties of the Zuckerman-Kuhlman personality questionnaire (ZKPQ-III-R): a study of a shortened form. Personality and Individual Differences 34, 1083–1097. American Cancer Society (1996) Cancer statistics: a measure of progress. CA–A Cancer Journal For Clinician 46, 9–27. Arbuckle J. (2003) Amos 5.0 Update to the Amos User’s Guide. Smallwaters, Chicago. Bjorck J.P., Hopp D.P. & Jones L.W. (1999) Prostate cancer and emotional functioning: effects of mental adjustment, optimism, and appraisal. Journal of Psychosocial Oncology 17, 71–85. Bollen K.A. (1989) Structural Equations with Latent Variables. Wiley, New York, NY, USA. Psychometric evaluation of the CAHS Bollen K.A. & Long J.S. (1993) Testing Structural Equation Models. SAGE Publications, Thousand Oaks, CA, USA. Browne M.W. & Cudeck R. (1989) Single sample cross-validation indices for covariance structures. Multivariate Behavioral Research 24, 445–455. Byrne B.B. (1994) Structural Equation Modeling with EQS and EQS/ windows: Basic Concepts, Applications, and Programming. Sage, Thousands Oaks, CA, USA. Coyne J.C., Aldwin C. & Lazarus R. (1981) Depression and coping in stressful episodes. Journal of Abnormal Psychiatry 122, 47–51. Davison B., Degnar L. & Morgan T. (1995) Information and decision making preferences of men with prostate cancer. Oncology Nursing Forum 22, 1402–1408. Fawzy N.W. (1995) A psychoeducational nursing intervention to enhance coping and affective state in newly diagnosed malignant melanoma patients. Cancer Nursing 6, 427–438. Folkman S. (1984) Personal control and stress and coping process: a theoretical analysis. Journal of Personality and Social Psychology 46, 839–852. Folkman S. & Lazarus R. (1988) Manual for the Ways of Coping Questionnaire. Consulting Psychologists Press, Palo Alto, CA, USA. Folkman S., Lazarus R., Gruen R. & Delongis A. (1986) Appraisal, coping health status, and the psychological symptoms. Journal of Personality and Social Psychology 50, 571–579. Frank-Stromborg M. (1989) Reaction to the diagnosis of cancer questionnaire: development and psychometric evaluation. Nursing Research 38, 364–369. Gass K.A. (1988) Aged widows and widowers: similarities and differences in appraisal, coping, resources, type of death, and health dysfunction. Archives of Psychiatric Nursing 2, 200–210. Hair J., Anderson R., Tatham R. & Black W. (1998) Multivariate Data Analysis, 5th edn. Prentice Hall, NJ, USA. Joreskog K.G. & Sorbom D. (1993) LISREL 8: Structural Equation Modeling with the SIMPLIS Command Language. Lawrence Erlbaum, Hillsdale, NJ, USA. Kaiser H.F. (1974) An index of factorial simplicity. Psychometrika 35, 31–36. Kammer C.H. (1994) Stress and coping of family members responsible for nursing home placement. Research in Nursing and Health 17, 89–98. Kessler T.A. (1998) The cognitive appraisal of health scale: development and psychometric evaluation. Research in Nursing & Health 21, 73–82. Kim J. & Mueller C.W. (1978) Factor Analysis: Statistical Methods and Practical Issues. Sage, Newbury. Koufteros X. (1999) Testing a model of pull production: a paradigm for manufacturing research using structural equation modeling. Journal of Operations Management 17, 467–488. Krause K. (1991) Contracting cancer and coping with it: patients’ experiences. Cancer Nursing 14, 240–245. Lazarus R.S. (1998) Fifty years of the Research and Theory of R.S. Lazarus an Analysis of Historical and Perennial Issues. Lawrence Erlbaum Associates, NJ, USA. Lazarus R. & Folkman S. (1984) Stress, Appraisal, and Coping. Spring publishing Company, New York. Lev E. (1992) Patients’ strategies for adapting to cancer treatment. Western Journal of Nursing Research 14, 595–611. 2005 Blackwell Publishing Ltd, Journal of Advanced Nursing, 49(1), 78–86 85 M.M. Ahmad March H.W., Balla J.R. & Hau K. (1996) An evaluation of increment fit indices: a clarification of mathematical and empirical properties. In Advanced Structural Equation Modeling: Issues and Techniques (Marcoulides G.A. & Schumacker R.E., eds), Lawrence Erlbaum, Mahwah, NJ, USA, pp. 315–353. Menaghan E.G. (1982) Measuring coping effectiveness: a panel analysis of marital problems and coping efforts. Journal of Health and Social Behavior 23, 220–234. Mishel M. & Sorenson D. (1991) Uncertainty in gynecological cancer: a test of the mediating functions of mastery and coping. Nursing Research 36, 98–103. Munro B. (2001) Statistical Methods for Health Care Research. Lippincott, Philadelphia. Norusis M.J. (1998) SPSS Professional Statistics. Prentice-Hall, Upper Sadler River, NJ, USA. Nunnally J.C. & Bernstein I.H. (1994) Psychometric Theory. McGraw-Hill, New York. 86 O’Leary-Kelly S. & Vokurka R.J. (1998) The empirical assessment of construct validity. Journal of Operations Management 16, 387–405. Oberst M.T., Thomas S., Gass K. & Ward S. (1989) Caregiving demands and appraisal of stress among family caregivers. Cancer Nursing 12, 209–215. Oberst M.T., Hughes S., Chang A. & McCubin M. (1991) Self-care burden, stress appraisal, and mood among persons receiving radiotherapy. Cancer nursing 14, 71–78. Tabachnick B. & Fidell L. (2001) Using Multivariate Statistics, 4th edn. Allyn & Bacon, Needham Height, MA, USA. Wang L., Fan X. & Willson V. (1996) Effects of non-normal data on parameter estimates and fit indices for a model with latent and manifest variables: an empirical study. Structural Equation Modeling 3, 228–247. Youngblut J. (1993) Comparison of factor analysis options using the home/employment orientation scale. Nursing Research 42, 122–124. 2005 Blackwell Publishing Ltd, Journal of Advanced Nursing, 49(1), 78–86