predict that the Tacrolimus II assay would agree well with HPLC
advertisement

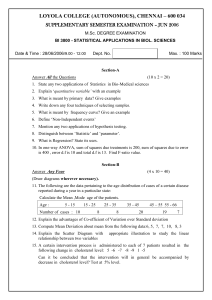
1870 Technical Briefs predict that the Tacrolimus II assay would agree well with HPLC-MS/MS. However, Cogill et al. (10 ) found that the Tacrolimus II method yielded ;16% overestimation of the true tacrolimus concentration in patient samples based on comparison to HPLC-MS/MS. Our data support the literature with respect to overestimation of tacrolimus concentrations in patient samples by the Tacrolimus II assay. In the first report of the ProTrac II method using proteolytic extraction, MacFarlane et al. (1 ) reported that the ProTrac II method yielded ;20% lower values than the predecessor ELISA that used methanol extraction. Salm et al. (9 ) reported that the ELISA method (methanol extraction) yielded results with minimal bias of ,0.2 mg/L relative to HPLC-MS/MS. Comparable data for the ProTrac II method currently in clinical use are not available other than one report from MacFarlane et al. (11 ), who demonstrated comparable results between ProTrac II and HPLC-MS/MS. However, insufficient methodologic detail is given for critique of the data. Taken together, the available data would suggest that the ProTrac II method would yield lower results than HPLC-MS/MS, which is consistent with our recovery data reported here. In comparison with Tacrolimus I, the ProTrac II method yielded .20% lower values than the Tacrolimus I assay on patient samples (mean difference, 4.2 6 2.6 mg/L; P ,0.05) (1 ). However, although the Tacrolimus II assay yields lower concentrations than Tacrolimus I (;2 mg/L on average), our data clearly demonstrate that a positive bias persists between the current ELISA and MEIA methods. The principal source of discrepancy between the MEIA I and ELISA I assays has been attributed to differences in the extraction procedures (1, 11 ), potentially related to differences in extraction efficiency of tacrolimus and cross-reacting metabolites. To address this possibility, we compared the recovery of pure tacrolimus introduced into samples containing tacrolimus and metabolites and drugfree whole blood. These results yielded recoveries of 112% 6 22% and 108% 6 2% from patient samples and drugfree samples, respectively, for the Tacrolimus II assay and 74% 6 15% and 71% 6 8%, respectively, for the ProTrac II assay. Although the results of this study cannot directly rule out differences in extraction efficiency of tacrolimus and cross-reacting metabolites, the consistent bias we observed in the absence and presence of metabolites [213% (95% CI, 24.5% to 221%) for patient samples vs 217% (95% CI, 29.6% to 223.2%) for drug-free samples with added tacrolimus] argues against potential differences in metabolite extraction efficiency. In summary, our data demonstrate differences in measured tacrolimus concentrations as great as 7.6 mg/L between the two most commonly used immunoassays for therapeutic monitoring of tacrolimus. Consistent with the current literature, neither immunoassay method is entirely accurate over the range of concentrations measured. The Tacrolimus II method overestimates true tacrolimus concentrations, and in contrast to current reports, we found that the ProTrac II ELISA underestimates the concentration of tacrolimus by ;25% on average. Based on the differences in tacrolimus concentrations measured using the two methods, laboratories should clearly communicate with physicians regarding methodbased bias and ensure that individual patients are not monitored by the two methods simultaneously. In addition, these data should be carefully evaluated with respect to the assay used in clinical studies that have defined the currently accepted therapeutic range. References 1. MacFarlane G, Scheller D, Ersfeld D, Jensen T, Jevans A, Wong PY, Kobayashi M. A simplified whole blood enzyme-linked immunosorbent assay (ProTrac II) from tacrolimus (FK506) using proteolytic extraction in place of organic solvents. Ther Drug Monit 1996;18:698 –705. 2. Tredger JM, Gilkes CD, Gonde CE. Therapeutic monitoring of tacrolimus (FK506) with first- and second-generation microparticle enzyme immunoassays: performance and results in four patient populations. Ther Drug Monit 1998;20:266 –75. 3. Wallenmacq PE, Leal T, Besse T, Squifflet J-P, Reding R, Otte J-B, et al. IMx Tacrolimus II vs Tacrolimus microparticle enzyme immunoassay evaluated in renal and hepatic transplant patients. Clin Chem 1997;43:1989 –91. 4. Cao Z, Linder M, Brown G, Valdes R Jr. Evaluation of the new Tacrolimus II microparticle enzyme immunoassay [Abstract]. Ther Drug Monit 1997;19: 564. 5. Murthy JN, Soldin SJ. Performance characteristics of the Abbott Tacrolimus-II IMx assay [Abstract]. Ther Drug Monit 1997;19:559. 6. Strike PW. Medsnap. A statistical toolkit for health professionals, Ver. 2 [Computer program]. Oxford, UK: Butterworth-Heinemann, 1996. 7. Bland JM, Altman DG. Comparing methods of measurement: why plotting difference against standard method is misleading. Lancet 1995;346: 1085–7. 8. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986;i:307–10. 9. Salm P, Taylor PJ, Clark A, Balderson GA, Grygotis A, Norris RL, et al. High-performance liquid chromatography-tandem mass spectrometry as a reference for analysis of tacrolimus to assess two immunoassays in patients with liver and renal transplants. Ther Drug Monit 1997;19:694 – 700. 10. Cogill JL, Taylor PJ, Westley IS, Morris RG, Lynch SV, Hohnson AG. Evaluation of the Tacrolimus II microparticle enzyme immunoassay (MEIA II) in liver and renal transplant recipients. Clin Chem 1998;44:1942– 6. 11. MacFarlane G, Scheller D, Ersfeld D, Fox B, Obritsch J, Roesler J. Analytical characterization of the ProTrac II ELISA for the determination of tacrolimus in whole blood [Abstract]. Ther Drug Monit 1997;19:559. Detection of Dietary Antioxidant Phenolic Compounds in Human LDL, Rosa M. Lamuela-Raventós,1 Marı́a-Isabel Covas,2,3* Montserrat Fitó,2 Jaume Marrugat,2 and M. Carmen de la Torre-Boronat1 (1 Departament de Bromatologia i Nutrició, Facultat de Farmàcia, Universitat de Barcelona, 08028 Barcelona, Spain; 2 Unitat de Lipids i Epidemiologia Cardiovascular, Institut Municipal d’Investigació Médica (IMIM), Carrer Doctor Aiguader, 80, 08003 Barcelona, Spain.; 3 Laboratori de Referència de Catalunya, 8027 Barcelona, Spain; * author for correspondence: fax 34-932213237, e-mail mcovas@imim.es) There is growing interest in the role of phenolic compounds in the diet as antioxidants. Epidemiological studies support a relationship between the consumption of phenolic rich food products (1, 2 ) and a low incidence of coronary heart disease. Strong evidence exists that oxidation of LDL lipids is a risk factor for atherosclerosis and coronary heart disease (3 ). Oxidation of LDL appears to occur predominantly in arterial intima in microdomains Clinical Chemistry 45, No. 10, 1999 1871 Fig. 1. Phenolic compounds in human LDL. Peaks: 2, rutin; 3, quercetin-3-glucuronide. Peaks 1, 4, and 5 have flavonoid-like spectra. sequestered from antioxidants of plasma (4 ). In this situation, phenolics that bind LDL are good candidates for preventing lipid peroxidation and atherosclerotic processes. The reduction of LDL oxidation observed after consumption of foods rich in phenolic compounds (5, 6 ) provides indirect evidence of a binding of phenols to LDL. However and to our knowledge, the binding of individual phenolic compounds to LDL has not yet been demonstrated. Using a solid-phase extraction with HPLC-diode array detection (DAD), we have identified and quantified some phenolic compounds in LDL isolated after long-term spins to ensure the purity of the lipoprotein. Blood samples from 10 male healthy volunteers on nonsupplemented diets were obtained by venipuncture and collected in EDTA-containing tubes after an overnight fast. The study was done in accordance with the Helsinki Declaration of 1975, as revised in 1989. The protocol was approved by a local ethics committee. Plasma was pooled, and LDL was isolated by a two-step sequential flotation ultracentrifugation. Isotonic saline (1 mL; d 5 1.006 kg/L) containing 1.091 mmol/L EDTA was layered on top of plasma (2 mL) in centrifuge tubes (Beckman polycarbonate tubes, total volume, 5 mL; Beckman). The tubes were centrifuged in a Beckman XL-70 ultracentrifuge with a Beckman 50.4 rotor at 227 000g for 18 h at 4 °C. The VLDL fraction was separated by aspiration. The plasma (3 mL) was deposited in a centrifuge tube (Kontron polyallomer tubes, total volume, of 13 mL; Kontron) containing 0.1155 g of KBr (Sigma). Isotonic saline (3 mL; d 5 1.21 kg/L) containing 1.091 mmol/L EDTA and 2.704 mol/L KBr was layered on top of the plasma. Tubes were centrifuged in a Kontron 41.14 rotor at 215 000g for 20 h at 4 °C. The LDL-containing middle layer was aspirated. Protein content was determined by a red pyrogallol method (Sigma). Acidulated LDL (1 mL of LDL plus 20 mL of concentrated phosphoric acid) was applied to a Waters OasisTM HLB extraction cartridge and washed with water (1 mL) and 50 mL/L methanol in water (1 mL). The phenols were eluted with methanol, and the methanolic extract was evaporated under a nitrogen stream. The residue was dissolved in mobile phase and analyzed by HPLC-DAD. Briefly, the eluted fraction (100 mL) was injected in a 1050 Hewlett-Packard gradient liquid chromatograph (Hewlett Packard) equipped with an automatic injector. A Nucleosil (Tracer) C18 120 (25 3 0.4 cm, 5 mm) reversed-phase column was used with a precolumn of the same material, both columns set at 40 °C. The flow rate was 1.5 mL/min. The HPLC conditions were similar to those described previously (7 ); however the elution profile was slightly modified as follows: 0 min, 100% A, 0% B; 5 min, 98% A, 2% B; 10 min, 96% A, 4% B; 15 min, 90% A, 10% B; 26 min, 81% A, 19% B; 26.5 min, 79.5% A, 20.5% B; 35 min, 70% A, 30% B; 40 min, 60% A, 40% B; 45 min, 0% A, 100% B, where solvent A was acidulated water containing 27 mL/L glacial acetic acid, and solvent B was 200 mL/L phase A and 800 mL/L acetonitrile. Detection was performed using a Hewlett Packard 1050M diode array ultraviolet-visible detector coupled to a Hewlett Packard Chem Station. The chromatogram was monitored at 280, 320, and 365 nm. To study the recovery, known amounts of rutin (270 ng) were added to the LDL, and then the LDL samples were acidulated and extracted with the same procedure described above. The results obtained at 280 nm are shown in Fig. 1. Two compounds were identified by retention times and spectral properties as rutin (peak 2) and quercetin-3-glucuronide (peak 3). Three major peaks had spectra consistent with those of flavonoids (peaks 1, 4, and 5), but all remain unidentified. Phenolic compounds with flavonoid-like spectra were present in the highest concentrations in LDL (16.27, 0.92, and 5.37 nmol catequin equivalents/mg LDL protein for peaks 1, 4 and 5, respectively). The concentrations of rutin and quercetin-3-glucuronide were 0.093 1872 Technical Briefs nmol/mg LDL protein and 0.073 nmol rutin equivalents/mg LDL protein, respectively. The analytical within-run imprecision (n 5 10), expressed as the CV, ranged from 4.2% for peak 1 to 6.3% for rutin. The analytical between-run imprecision (n 5 10), expressed as the CV, ranged from 4.6% for peak 1 to 13% for rutin. The recovery obtained (n 5 6) was 80.6% 6 6.7% (mean 6 SD). Rutin, quercetin, and flavonoids are phenolics present in fruits, vegetables, spices, olive oil, and red wine (5–9 ). Quercetin-rich foods such as onions or red wine have been shown to delay the susceptibility of LDL to oxidation after their supplementation in in vivo human studies (5, 6 ). Rutin and quercetin have been shown to delay the susceptibility of VLDL plus LDL to oxidation in in vitro studies after their addition to the isolated lipoproteins (10 ). Increased total phenol content of LDL after ingestion of red wine, as measured by the Folin-Ciocalteau method, has been reported (6 ). This method, however, is sensitive to nearly all oxidizable compounds, and the development of a reliable HPLC method to detect and identify phenolic compounds in LDL is needed (6 ). Our results provide evidence that several dietary phenolic compounds are bound to LDL lipoproteins. The binding of these phenolic compounds to LDL supports the role of phenolics in the protection of the autocatalytic chain reaction of fatty acid peroxidation in LDL directly and/or by preservation of other chain-breaking antioxidants such as a-tocopherol (9 ). Phenolics bound to LDL were found in nonsupplemented individuals, and thus routine diets already appear to achieve this binding. HPLC-DAD with previous solid-phase extraction can potentially be used to evaluate the relationship between the binding of phenolic compounds to LDL and their biological activity as antioxidants in supplementation studies with dietary or nutraceutical foods. The fact that these phenolic compounds remain associated to LDL after long-term spins could suggest a strong binding with LDL. However, further studies are required to measure and compare the in vivo and in vitro kinetics of association and release, to see whether there is any process that actively partitions these substances into LDL. Our results provide further evidence that dietary phenolics are likely to protect LDL lipoproteins from oxidation in the subendothelial spaces of the arterial intima and thereby delay the onset or progression of atherosclerotic processes. In conclusion, through the integration of a solid-phase extraction system with HPLC-DAD, we have demonstrated the presence of individual dietary phenolic compounds bound to human LDL particles in nonsupplemented individuals. This method provides a simple, rapid, and accurate identification and quantification of phenolic compounds present in LDL. This work was supported by Grant ALI97-1607-CO2-01 from Comisión Interministerial de Ciencia y Tecnologı́a and by FPI Grant 98/9562 from Fondo de Investigación Sanitaria. We thank A. Waterhouse from the University of California at Davis for reviewing the manuscript. References 1. Hertog MGL, Fesrens EJM, Hollman PCH, Katan MB, Kromhout D. Dietary antioxidant flavonoids and risk of coronary hearth disease: the Zutphen Elderly Study. Lancet 1993;342:1007–11. 2. Renaud S, Ruf JC. The French paradox. Vegetables or wine. Circulation 1994;90:3118 –9. 3. Diaz MN, Frei B, Vita JA, Keaney JF. Antioxidants and atherosclerotic heart disease. New Engl J Med 1997;337:408 –16. 4. Witzum JL. The oxidation hypothesis of atherosclerosis. Lancet 1994;344: 793–5. 5. Hollman PCH, Katan MB. Absorption, metabolism and health effects of dietary flavonoids in man. Biomed Pharmacother 1997;51:305–10. 6. Nigdikar SV, Williams NR, Griffin BA, Howard AN. Consumption of red wine polyphenols reduces the susceptibility of low-density lipoproteins to oxidation in vivo. Am J Clin Nutr 1998;68:258 – 65. 7. Betes Saura C, Andrés-Lacueva C, Lamuela-Raventós RM. Phenolics in white free run juice and wines from Penedès by high-performance liquid chromatography: changes during vinification. J Agric Food Chem 1996;44:304 – 6. 8. Herrmann K. Occurrence and content of hydroxycinnamic and hydroxybenzoic acid compounds in foods. Crit Rev Food Sci Nutr 1989;28:315– 47. 9. Visioli F, Bellomo G, Montedoro G, Galli C. Low density lipoprotein oxidation is inhibited in vitro by olive oil constituents. Atherosclerosis 1995;117:25– 32. 10. Vinson JA, Jang J, Dabbagh YA, Serry MM, Cai S. Plant polyphenols exhibit lipoprotein bound antioxidant activity using an in vitro oxidation model for heart disease. J Agric Food Chem 1995;43:2798 –9. High-Speed Detection of the Two Common a1-Antitrypsin Deficiency Alleles Pi*Z and Pi*S by Real-Time Fluorescence PCR and Melting Curves, Charalampos Aslanidis,1* Markus Nauck,2 and Gerd Schmitz1 (1 Institute for Clinical Chemistry and Laboratory Medicine, University of Regensburg, Franz-Josef Strauss Allee 11, 93042 Regensburg, Germany; 2 Department for Clinical Chemistry, University Hospital Freiburg, 71106 Freiburg, Germany; * author for correspondence: fax 49-941-944-6202, e-mail Charalampos.Aslanidis@klinik.uni-regensburg.de) Protease inhibitor 1 (a1-antitrypsin; AT) is the main serum inhibitor of proteolytic enzymes. In AT deficiency, enzymes such as neutrophil elastase can damage the lung tissues, leading to pulmonary emphysema. More than 90 different alleles have been identified to date for the protease inhibitor 1 gene (PI). The three most important variants are type M (90% of population), type S (Pi*S), and type Z (Pi*Z), of which types S and Z are two of the more common abnormal variants. Homozygotes of type Z have a considerable reduction in the serum AT concentration and may develop pulmonary emphysema or hepatic cirrhosis. SZ-heterozygotes are less severely affected (1– 3 ). The allele frequencies of the most common alleles, Pi*S and Pi*Z, are 0.02– 0.04 or 0.01– 0.02, respectively, with 0.2% of the general population being homozygous for either the Pi*Z or Pi*S allele. Typically, different phenotypes have been characterized by isoelectric focusing. PCR-based technologies are now being used widely for the identification of the mutations underlying the Pi*Z allele (Glu342Lys, GAG to AAG) and the Pi*S allele (Glu264Val, GAA to GTA), thus simplifying mutation detection (4 ). Although these methods give rise to unequivocal results, they are time-consuming and require optimization of the PCR reaction to eliminate nonspecific PCR products that would disturb the genetic analysis.