March-April 2013 | Volume 15 | Issue 63 www.noiseandhealth.org
advertisement

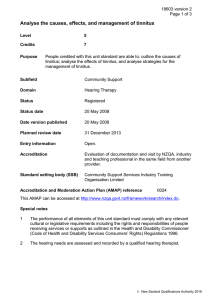
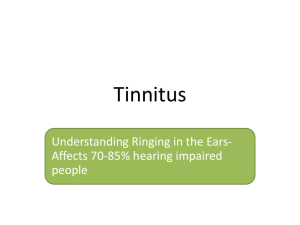
I ith & w SE d e A ex MB d In E, E N LI ED SC ISSN 1463-1741 Impact Factor® for 2011: 1.254 M Noise & Health • Volume 15 • Issue 63 • March-April 2013 • Pages 81-152 A Bi-monthly Inter-disciplinary International Journal www.noiseandhealth.org March-April 2013 | Volume 15 | Issue 63 Recent technological advances in sound‑based approaches to tinnitus treatment: A review of efficacy considered against putative physiological mechanisms Derek J. Hoare1,2, Peyman Adjamian3, Magdalena Sereda1,2, Deborah A. Hall1,2 NIHR Nottingham Hearing Biomedical Research Unit, Ropewalk House, 113 The Ropewalk, Nottingham, NG1 5DU, UK, 2School of Clinical Sciences, University of Nottingham, 3MRC Institute of Hearing Research, University Park, Nottingham, NG7 2RD, UK 1 Abstract The past decade has seen an escalating enthusiasm to comprehend chronic tinnitus from the perspective of both scientific understanding and clinical management. At the same time, there is a significant interest and commercial investment in providing targeted and individualized approaches to care, which incorporate novel sound‑based technologies, with standard audiological and psychological strategies. Commercially produced sound‑based devices for the tinnitus market include Co‑ordinated Reset Neuromodulation®, Neuromonics©, Serenade®, and Widex® Zen. Additionally, experimental interventions such as those based on frequency‑discrimination training are of current interest. Many of these interventions overtly claim to target the underlying neurological causes of tinnitus. Here, we briefly summarize current perspectives on the pathophysiology of tinnitus and evaluate claims made by the device supporters from a critical point of view. We provide an opinion on how future research in the field of individualized sound‑based interventions might best provide a reliable evidence‑base in this growing area of translational medicine. Keywords: Electroencephalography, frequency discrimination, magnetoencephalography, plasticity, reorganization, sound therapy Introduction Self‑reported tinnitus affects around 4.4‑15.1% of the adult population.[1] Tinnitus is a symptom of diverse pathologies, including otologic, neurologic, infectious, and drug‑related effects and evidence suggests that various levels of the nervous system are involved in its manifestation.[2,3] Although often co‑morbid with peripheral hearing loss, chronic tinnitus persists after auditory nerve transection demonstrating involvement of central mechanisms.[4] The current consensus is that damage to the afferent input to the auditory pathway initiates events that results in plastic changes at the central level giving rise to the percept of tinnitus. As well as being co‑morbid with hearing loss, for a subset of people, tinnitus impairs quality of life and is associated with symptoms of anxiety, depression, insomnia, and stress.[5] Tinnitus care, therefore, can demand a multi‑faceted Access this article online Quick Response Code: Website: www.noiseandhealth.org DOI: 10.4103/1463-1741.110292 PubMed ID: *** 107 approach to patient assessment and management that can be highly individual.[6] Traditional methods for the clinical management of tinnitus involve three core elements: (i) education and counseling, (ii) stress reduction and relaxation, and (iii) use of therapeutic sound. Such approaches often combine sound enrichment and counseling elements such as in Tinnitus Retraining Therapy[7] or other less formalized “habituation” therapies. That therapeutic sound can affect changes in tinnitus percept has been appreciated for centuries. In recent decades, the use of sound or sound enrichment has become a central part of many tinnitus management programs delivered by clinicians, whether the intention is to mask tinnitus, suppress tinnitus, or interrupt the tinnitus generating neural activity. In the UK, the most popular audiological management approaches include hearing‑aid fitting and/or the provision of white noise generators.[8] Specific discussion of these particular devices is beyond the scope of this paper. Here, we introduce the primary physiological mechanisms hypothesized to underlie tinnitus. We also review a number of innovative individualized sound‑based interventions, considering their proposed physiological mechanisms of action, and conclude on future directions in the field. Pathophysiology of tinnitus Hearing loss causes dramatic functional and structural changes in the peripheral and central auditory system. The Noise & Health, March-April 2013, Volume 15:63, 107-116 Hoare, et al.: Sound‑based tinnitus treatment main cause of high‑frequency sensorineural hearing loss is ageing, such that, the prevalence of tinnitus increases with age.[1] High‑frequency hearing loss has been shown to induce an increase in stimulus‑driven activity, a reorganization of the tonotopic map, and an increase of the spontaneous activity at virtually all levels in the central auditory system, and synchrony in auditory cortex (An extensive review of the neurophysiological evidence, predominantly from the animal model, is provided by Noreña.[9]) As these changes are not accompanied by enhanced outputs from the auditory nerve, they probably result from neural mechanisms intrinsic to the central auditory system. It has been suggested that this overall hyperactivity could result from an increase in central gain (or sensitivity). The general purpose of such gain might be to adapt neural sensitivity to the reduced sensory inputs, preserving a stable mean firing and neural coding efficiency.[9] However, maintaining neural homeostasis is achieved at the cost of amplifying “neural noise” due to the overall increase of gain, ultimately resulting in the generation of tinnitus. The utility of auditory cortical evoked responses as an objective indicator of tinnitus is still debated. Conflicting results may reflect differences in choice of control group or experimental parameters. For example, inter‑stimulus interval is known to affect the amplitude of the evoked response with shorter intervals leading to smaller amplitudes and hence a smaller dynamic range within which to reveal differences across groups.[19] Another issue is that of comorbid symptoms such as hyperacusis. This condition refers to an abnormal sensitivity to everyday sounds[20] and may be a manifestation of increased neural excitability in the auditory system.[21] Hyperacusis is often associated with tinnitus. Recent evidence using functional magnetic resonance imaging (fMRI) suggests that diminished sound‑level tolerance (as in hyperacusis) might be sufficient on its own to enhance the stimulus‑evoked response, irrespective of tinnitus.[22] This was especially true in inferior colliculus and medical geniculate body. This finding illustrates the importance of screening all tinnitus patients for sound‑level tolerance and interpreting many of the preceding results with due care. Increased stimulus‑induced activity Reorganisation of the tonotopic map Hearing loss can lead to dramatic changes in stimulus‑induced activity. Research in this field has been particularly informed by animal recordings made in dorsal cochlear nucleus. A number of human studies have examined hyperexcitability in tinnitus and have reported an abnormally elevated neural response to external sounds. Given that electroencephalography (EEG) and magnetoencephalography (MEG) reflect neural events on a macroscopic scale, hyperexcitability could be a measure of recruitment of a population of neurons provided that sufficient synchrony exists within that ensemble. A comprehensive review of the neuroimaging studies in tinnitus is given in Adjamian et al.,[10] and here we briefly discuss some of the relevant studies conducted in humans. Long‑term sensorineural hearing loss can lead to dramatic changes in the frequency‑based organization within central auditory structures. When peripheral hearing loss deprives central auditory neurons of their normal input they begin to show responsiveness to the characteristic frequency of less affected “neighbors’ rather than their original place in the tonotopic map (see review by Eggermont and Roberts[23]). The normal threshold at the new characteristic frequency of neurons suggests that these changes have been induced by plasticity mechanisms, perhaps through a process of rewiring in the cortex, or the unmasking of latent cochlear inputs to regions newly deprived of direct inputs. Neurons in the affected region also show increased spontaneous activity and synchrony.[24] Changes in response properties of neurons and tonotopic map reorganization are therefore not isolated events. Evidence for neuroplasticity after hearing loss and/ or tinnitus in the frequency organization of primary auditory cortex has been reported using both animal electrophysiology and human neuroimaging (see reviews by Eggermont and Roberts;[23] Adjamian et al.[10]). Increments of evoked signal amplitude have been reported for several components of the acoustically evoked signal; the middle latency response,[11] the steady‑state response[12] and the N1/N1m.[13‑15] Using MEG, Diesch and colleagues recently demonstrated that responses to the super‑position of three amplitude‑modulated tones were reduced in healthy controls (indicative of reciprocal inhibition), but increased in patients with tinnitus (indicative of abnormal reciprocal facilitation). This finding is compatible with the interpretation that tinnitus is associated with a reduced lateral or surround inhibition compared to control subjects. Similarly, a number of early studies reported abnormally enhanced transient N1 (N1m) responses to a 1‑kHz tone in a group of tinnitus patients,[13‑15] although these studies have not always been replicated.[16‑18] One might expect such hyperexcitability to be greatest at frequencies corresponding to the tinnitus pitch and/or to the region of hearing loss. However, this was not explicitly tested or supported by previous experimental findings. Noise & Health, March-April 2013, Volume 15 Neuroplastic reorganization has also been reported in the normal hearing system driven by auditory perceptual learning for pure tones.[25] In this study using owl monkeys, the changes reported were again predominantly in terms of an expanded representation of the trained frequency in primary auditory cortex (A1) of trained animals, compared to the corresponding area in animals that were untrained or were trained on tones of a different frequency. Tonotopic map reorganization in juvenile cat auditory cortex has also been observed as a result of long‑term exposure to a spectrally‑enhanced acoustic environment, without inducing hearing loss.[26] 108 Hoare, et al.: Sound‑based tinnitus treatment In our view, most convincing pieces of evidence in humans for an over‑representation of frequencies corresponding to the edge of the hearing loss are from behavioral, not neuroimaging, studies. Thai‑Van et al.,[27] demonstrated enhanced frequency discrimination at the edge frequency in individuals with steeply sloping hearing loss, suggesting that an expansion of the cortical area with specificity around this frequency would give the increase in computational power required for better performance at frequency discrimination. Moore and Vinay[28] also reported enhanced frequency discrimination at low frequencies, in individuals with cochlear dead regions at high frequencies. Increased spontaneous activity In the absence of external sound input, neural firing is randomly generated, and hearing loss may alter the synchronous neural discharge patterns in the central auditory system resulting in tinnitus. Animals with induced hearing loss show an increase in spontaneous synchronous firing of primary auditory cortical neurons.[24,29,30] The greatest increase in synchrony occurs in the deafferented region, which is most likely to reflect changes in lateral connectivity. Chronic tinnitus has been associated with increased oscillatory brain rhythm activity in the delta band (1.5‑4 Hz) and the gamma band (e.g., 25‑80 Hz) and decreased activity in the alpha band (8‑13 Hz).[31‑34] Abnormal increase in slow‑wave (delta/theta) oscillatory activity has been reported in a number of MEG/EEG studies providing the strongest evidence for the involvement of central auditory structures in tinnitus.[32,35,36] An example of this effect is illustrated in Figure 1 where cortical power in the delta band is shown as a function of time from two participants one with and one without tinnitus. Using MEG, spontaneous brain activity was recorded while participants listened to their tinnitus. Power in the delta band was estimated at each point in the brain volume using a beam former technique and superimposed on the anatomical MRI of each participant. In the participant with tinnitus, there was an increase in delta activity localized to the left auditory cortex while the participant with no tinnitus did not show such increase. For the tinnitus participant, the waveform corresponding to the peak location was extracted (solid blue line) while for the participant with no tinnitus, a corresponding point in the auditory cortex was chosen to extract the MEG time course (dotted red line). As can be seen, delta band power was enhanced for the tinnitus participant indicative of the tinnitus percept. This enhanced slow wave activity is likely to reflect a disruption of coherent activity between thalamus and cortex.[31] All the above models consider the pathophysiology of tinnitus purely from the point of view of changes happening within the central auditory system. However, this approach could be criticized for being somewhat reductionist in its focus because the primary complaints of tinnitus from the patient perspective relate to the psychosocial aspects of the condition (distress, depression, social withdrawal, etc.) rather than the perceptual aspects of the condition (i.e., the auditory attributes Figure 1: Power estimate of spontaneous activity from the auditory cortex in the delta band from a participant with tinnitus (right, solid blue line) and one without tinnitus (left, dotted red line). This illustrative figure shows the abnormal enhancement of delta activity in tinnitus which has been reported in various studies 109 Noise & Health, March-April 2013, Volume 15 Hoare, et al.: Sound‑based tinnitus treatment of the sound percept itself). While hearing loss is commonly implicated in tinnitus, for most people, deafness does not lead to tinnitus. Therefore, activity outside the classical central auditory pathway is likely to play an important role in turning tinnitus on or off, perhaps via a gating mechanism. Role of emotional processing Several recent theoretical models have proposed a central role of the amygdala in tinnitus.[37,38] The basic assertion is that tinnitus is continuously associated with aversive emotional states through a process of learning. Rauschecker et al.,[38] have asserted that the amygdala is part of a larger circuit in limbic and paralimbic regions, responsible for a “noise cancellation system” that is disordered in tinnitus [Figure 2]. The proposed mechanism occurs via the projection of the tinnitus signal for emotional evaluation along the auditory pathway through the amygdala to the subcallosal area (nucleus accumbens, dorsal raphe nucleus, and ventromedial prefrontal cortex) that sends excitatory projections to the thalamic reticular nucleus. The thalamic reticular nucleus has a frequency‑selective inhibitory input to the medial subdivision of the medial geniculate body. In Rauschecker’s model, limbic and paralimbic structures play an active role in tinnitus. For example, the tinnitus signal can be “cancelled” when the subcallosal relay acts appropriately on the thalamic reticular nucleus to inhibit the tinnitus percept before it reaches the cortex. Preliminary spontaneous EEG data are generally supportive of a role for limbic regions. Support for enhanced activity in the amygdala during tinnitus comes from EEG measures of resting‑state oscillatory electrical activity in the brain.[39] Greater synchronous alpha band activity was found in a cohort of patients more distressed by their tinnitus, and these signals were attributed to the amygdala, parahippocampal gyrus, anterior cingulate cortex, and insula (see also De Ridder et al.[37]). Such differences in Figure 2: Putative brain networks involved in tinnitus. [36] Paralimbic networks in the ventromedial prefrontal cortex linked to the nucleus accumbens play an important role in evaluating the sound’s emotional content and in the long‑term habituation to continuous unpleasant sounds. Dashed circles indicate amygdala (medial view) and auditory cortex, AC (lateral view) Noise & Health, March-April 2013, Volume 15 neural activity suggest that neural systems or mechanisms associated with chronic tinnitus are distinct from those responsible for a person’s tinnitus‑related distress. Indeed even in a population of healthy participants without tinnitus, Irwin et al.,[40] found evidence for two functionally different neural networks associated with either the acoustic attributes of an external sound, or its emotional content. Evidence from current anatomical studies comparing people with tinnitus to controls lacks consensus on this issue. For example, Mühlau et al.,[41] found decreased grey matter volume only in the subcallosal area and an increase in grey matter volume in the right posterior thalamus, including medical geniculate nucleus, in people with tinnitus compared to healthy controls. However, a more recent study from Melcher et al.,[42] found no significant difference in grey matter volume between people with tinnitus and healthy controls. Instead, Melcher et al.,[42] reported a highly significant negative correlation between grey matter volume in the subcallosal area (ventromedial prefrontal cortex) and supra‑clinical audiometric thresholds (≥8 kHz). This frequency range was not measured by Mühlau et al.,[41] which may explain the discrepancy between the two studies. At the same time, Leaver et al.,[43] also found reduced grey matter volume in the ventromedial prefrontal cortex of people with tinnitus compared to people without tinnitus. Although no significant difference in audiometric profiles were reported by Leaver et al.,[43] it is noted that mean cut‑off frequency for normal hearing in their control group was 6 kHz whereas for their tinnitus group, it was only 2 kHz, which may have influenced their result. This is clearly an area that requires further research. For an extensive review of fMRI evidence for the involvement of limbic activity in patients with tinnitus see Adjamian et al.[10] In his review of neurophysiological mechanisms, Noreña[9] argues for a greater understanding of central changes within the pattern of brain activity as a pre‑requisite to develop efficient therapies for alleviating tinnitus. Focused on the central auditory system, he outlines two potential strategies depending on the individual neuropathology. First, one might decrease the gain controlling neural sensitivity through the restoration of a near‑normal distribution of sensory inputs such as by amplification through a hearing aid. Second, one might decrease spontaneous activity of the cochlear nerve (the main driver of “neural noise” in the central auditory system) such as by blocking pharmacologically the synaptic transmission between inner hair cells and cochlear nerve fibers. At present, we are some way off validating these strategies, especially in the clinical context. Hence, we believe that human neuroimaging can play an important role in bridging the gap between animal and human models of tinnitus in order to evaluate how some of the recent sound‑based interventions might be effective. Let’s review some of the current evidence here. 110 Hoare, et al.: Sound‑based tinnitus treatment Some recent sound‑based technological innovations Acoustic co‑ordinated reset (CR) neuromodulation® This technology is an intervention recently developed by the German medical technology research company, Adaptive Neuromodulation GmbH (ANM) (www.anm‑medical.com/). The technology was first developed to treat Parkinson’s disease using electrical stimulation of the cortical neurons to disrupt (“reset”) pathological neuronal synchronization. The pioneers of this technology consider both Parkinson’s disease and tinnitus to be characterized by pathological nerve cell hyperactivity and synchronization. Hence the acoustic version of this intervention for tinnitus aims to disrupt aberrant neural firing using sound stimulation, not electrical stimulation as in the device for Parkinson’s disease. In both cases, patient benefit is believed to be derived through reduction of the pathological neural activity causing the disorder. The sound‑stimulation regime is tailored to each individual patient and is a sequence of tones carefully selected to span the frequency corresponding to the dominant tinnitus pitch. The recommendation for treatment is that these tone sequences are played at a low level for 4‑6 h and up to a maximum of 8 h daily, while engaging in other daily activities. An additional recommendation is that the treatment can be used intermittently throughout the day but in block periods of at least 1 h. It is suggested that the sound sequence desynchronizes the pathologically synchronous neuronal populations by decreasing mean synaptic weight,[44] effectively “resetting” the population from a stable synchronous state to a stable asynchronous state. Evaluation of its efficacy and neurophysiological mechanism of action Behavioral results from an early‑phase trial conducted in Germany indicate that 75% of participants reported a reduction in tinnitus distress (≥6 points on the Goebel Hiller Tinnitus Questionnaire) after using the device.[45] The specific claims about the mechanism of action can be objectively tested using neuroimaging techniques, which are sensitive to measuring synchronous neural activity. Such measures include the spontaneous oscillatory rhythms that are well documented in the healthy resting brain[46] and in tinnitus patients (see above). In the trial conducted by Tass et al.,[45] EEG activity was measured before and after 12 weeks of Acoustic CR Neuromodulation® therapy. Using the standardized low‑resolution brain electromagnetic tomography (sLORETA) technique, 3 dimensional maps of significant change in oscillatory activity were constructed revealing an increase in alpha band power that was strongest in temporal and prefrontal cortex, a widespread reduction in delta that was strongest in primary and secondary auditory cortices, and widespread reduction in gamma power after treatment. Theta power was significantly reduced in frontal regions and the anterior cingulate area, and beta power was also significantly reduced in the temporal area, particularly 111 in the superior temporal gyrus. Overall, these neuroimaging results support the notion that the sound‑based tinnitus treatment modulates spontaneous brain activity in perceptual (temporal lobe), cognitive (frontal lobe) and emotional (sub‑cortical) regions of the human brain [consistent with Figure 2]. The findings from this recently published work[45] are promising, but at an early stage of evaluation, and thus require more extensive and independent study. A large scale, randomized, placebo‑controlled, double‑blind trial is currently underway in the UK. Registration details of this trial can be found on clinicaltrials.gov (identifier NCT01541969). Serenade® This sound‑based intervention was recently produced in the US by SoundCure Inc. (www.soundcure.com). It is delivered as part of a broader tinnitus treatment program, but the specific mode of action of the sound device is purported to be that of suppression where the patterned sounds modulate auditory cortical activity and interrupt tinnitus generation.[47] The device delivers multiple tracks of temporally patterned sounds (“S tones”) that are again customized to each individual’s tinnitus so that they span the frequency region of hearing loss and dominant tinnitus pitch. Intermittent use of Serenade® is recommended by its manufacturers to achieve an “instant” temporary relief, such as for an hour in preparation for sleep. Evaluation of its efficacy and neurophysiological mechanism of action The developers refer to the initial work of Zeng et al.,[48] although this piece of research was a single‑case study exploring protocols of electrical stimulation delivered by a unilateral cochlear implant, for tinnitus benefit. In this study, the electrophysiological measures revealed that a 100‑Hz electrical stimulation pulse delivered to an apical electrode not only provided total tinnitus suppression, but also reduced and delayed the evoked N1 response to a frequency‑change stimulus. The oscillatory brain rhythms during the stimulus also showed an increase in alpha band (7‑9 Hz) power when tinnitus was suppressed compared to when tinnitus was present. No benefits were found for high‑rate (2‑5 kHz) electrical stimulation. From these results, the authors conclude that low‑rate stimulation maximally excites auditory cortex, which could interfere or suppress the tinnitus‑induced abnormal central activity. Indeed, animal electrophysiology has shown how sustained, synchronized neural discharge rates occur for comparable acoustic stimuli, such as click trains with longer (>40 ms) inter‑click intervals[49] and continuous sounds amplitude modulated at a slow rate (16‑32 Hz).[50] Compatible with this idea, a case study exploring protocols of acoustic stimulation reported how a 6‑kHz tone amplitude‑modulated at a rate of 40 Hz was judged to provide tinnitus suppression.[47] More recently, Reavis et al.,[51] examined the short‑term suppressive effects of external sounds (17 modulated sounds at different Noise & Health, March-April 2013, Volume 15 Hoare, et al.: Sound‑based tinnitus treatment modulation rates and carrier frequencies, and un‑modulated sounds at different carrier frequencies) matched to the tinnitus loudness. They found that the greatest immediate suppression was induced by 40‑Hz amplitude‑modulated tones with carrier frequencies near the tinnitus pitch. These stimulus conditions generated up to 100% suppression during a 3 min stimulation period, with residual inhibition lasting up to 90 s after the stimulus ended. The long‑term and specific neurophysiological effects of “S tones”, on auditory cortical activity, however, are yet to be demonstrated. Neuromonics® This tinnitus treatment makes claims to address the underlying neurological causes of tinnitus to deliver clinically proven long‑term relief naturally, without medication or surgery (http://www.neuromonics.com/). As with some of the other sound‑based devices it is delivered as part of a broader tinnitus treatment program, involving a counseling element that incorporates principles of cognitive behavioral therapy.[52] The sound‑based component of the treatment provides a means to “more readily promote desensitization to patients’ tinnitus perception” using sound stimuli more acceptable to patients than broadband masking noises.[53] A small, lightweight Oasis™ device with headphones delivers music that is spectrally modified according to an individual’s hearing thresholds, embedded within a broadband noise. At the first phase of treatment, the device is worn for at least 2 h per day, which can be during activities like reading, preparing meals or at the office. independent review of three controlled clinical trials that had been conducted by investigators having financial links with the Neuromonics company.[53,57,58] Again, they were critical of the lack of methodological rigor which, together with the potential for commercial bias, restricts any possible conclusions of effectiveness relative to other treatments. The manufacturers of the Neuromonics device do not make detailed claims for the specific mechanism of action for the sound delivery system, although generally, it is proposed that the “specialized acoustic stimulus targets the effects of auditory deprivation, while it’s relaxing music is intended to reduce involvement of the limbic and autonomous nervous system in the perception of tinnitus.”[54] To the best of our knowledge, the specific neurophysiological effects have yet to be investigated. Widex®Zen Zen is a music program that is available in some Widex® hearing aids (http://www.widex.co.uk/en/products/ thewidexsound/zen/). Zen plays random, wind‑chime‑like (fractal) tones with harmonic, but not predictable, relationships that can be used for relaxation[59] or for making tinnitus less noticeable.[60] There is a range of different Zen programs and each sound type can be adjusted to individual preference in terms of pitch, tempo and volume. The device is recommended to form part of a more holistic audiological management program incorporating education and counseling.[60,61] Evaluation of its efficacy and neurophysiological mechanism of action Evaluation of its efficacy and neurophysiological mechanism of action Clinical observations of patient benefit are generally encouraging. For example, in the House Clinic (Los Angeles, USA), 14 patients had completed the treatment by the end of the study period and reported a mean reduction in tinnitus distress (Tinnitus Reaction Questionnaire, TRQ) score from 46 to 17 (62% average reduction).[54] However, the authors do note that 15 patients returned their device, indicating rather poor overall compliance. In the only randomized trial of the device so far, Davis et al.,[52] examined the efficacy of the Neuromonics treatment compared to counseling with the provision of a noise generator or counseling alone. The authors’ metric of patient benefit was a clinically significant change in tinnitus distress at 6 months (40% reduction in overall TRQ) score. This criterion was achieved for 86% of patients receiving the “full Neuromonics© package,” 47% of patients receiving the noise generator and counseling, and just 23% of those who received counseling alone. Despite these positive reports, in our systematic review of randomized clinical trials (RCTs) for tinnitus[55] we assessed that the study quality in Davis et al.,[52] to be low. Study design and procedures for blinding researchers and patients were weak, and there was a risk of bias through inadequate randomization. Henry and Istvan[56] have also published an The intervention is based on the hypothesis that bothersome tinnitus involves limbic system activity where tinnitus is associated with a stress response, and that music has de‑stressing properties.[59] A survey of Widex® Zen use found that the Zen “Aqua” program was generally preferred by patients, possibly because it has a restricted range of low‑pitched sounds compared to the other Zen programs involving moderate to higher pitched sounds.[59] Kuk et al.,[59] investigated efficacy in a self‑selecting sample of 26 patients. The protocol of treatment reported in this study required the patient to listen to the stimuli for a 15‑30 min period each day in a quiet and relaxing situation. All 26 patients showed a reduction in tinnitus distress (TRQ score) at their final assessment and for 18 patients (69%), the change was greater than 20 points. Visual inspection of the data plot suggests that only 7 participants (~27%) had a clinically significant reduction in TRQ (i.e., 40%) at follow‑up. Sweetow and Sabes concluded from a further small cohort study (N = 14) patient benefits were generally greater when amplification was combined with fractal tones, compared to amplification alone.[61] However, improvements over 6 months were modest at best. Only four patients showed a reduction of at least 40% on their TRQ scores, while one patient reported Noise & Health, March-April 2013, Volume 15 112 Hoare, et al.: Sound‑based tinnitus treatment that their tinnitus got worse by more than 40% on the TRQ. Future opportunities for evaluation might also benefit from considering neurophysiological measures of limbic system activity to quantify the effect of listening to the fractal tones on the underlying stress response. Auditory perceptual training At present, this is an experimental intervention using personalized sounds to reduce the perceived tinnitus distress, using either single‑frequency tones or auditory sound objects. A common approach has been to train people with tinnitus on a frequency‑discrimination task (FDT) using either fixed‑frequency differences[62‑64] or an adaptive procedure.[35,65‑67] In a typical approach, patients might be presented with trials of sound pairs or triplets and required to make a decision as to which interval has the higher pitch (two‑alternative forced‑choice paradigm) or, which is the odd‑one out (three‑alternative forced‑choice paradigm). This type of paradigm forms the basis of psychophysical measures of perceptual thresholds and the rules of the procedure can be selected to track performance at a particular point on the psychometric curve (such as 71% or 79% accuracy).[68] Evaluation of its efficacy and neurophysiological mechanism of action The putative mechanism of action exploited by FDT concerns what is known about auditory cortical reorganization in the treatment of tinnitus, predominantly from animal studies. The concept draws on those observations which indirectly link tinnitus, hearing loss, and auditory perceptual learning, to altered patterns of neural activity within the central auditory system. If tinnitus is the unfortunate perceptual consequence of neural plasticity, then interventions that can drive changes in frequency representation at the level of the cortex, and potentially disrupt the tinnitus‑generating network, offer therapeutic possibilities. The reference tone for the discrimination task is typically tailored to the individual pattern of hearing loss or dominant tinnitus pitch, so to provide maximal sound enrichment to this region of frequency tuning within the central auditory system. At present, these links are rather speculative. For example, no human studies of tinnitus have yet provided substantial physiological evidence in support of evoked or induced changes in tinnitus‑related activity as a result of auditory training. An equally plausible (cognitive) alternative is that effects on attention may be the determining factor of benefit when it comes to FDT. A recent systematic review considered 10 studies that have so far been conducted to evaluate the efficacy of auditory perceptual training.[69] Nine out of the 10 studies reported some significant change in either qualitative or quantitative outcomes measures after auditory training. However, all studies were quality rated as providing low or moderate levels of evidence for the estimated effects they reported. 113 Our systematic review highlighted a pressing need for randomized controlled studies that will generate high‑quality unbiased and generalizable evidence for whether or not auditory perceptual training has a clinically relevant effect on tinnitus. We recently reported two randomized controlled trials of FDT involving 70 people with chronic subjective tinnitus.[70] The first study assessed the effect of FDT using (A) a single frequency in the region of normal hearing, (B) a single frequency in the region of hearing loss, or (C) a high‑pass (missing fundamental) harmonic‑complex tone that provided high‑frequency stimulation but evoked a low pitch percept. Hence, we compared training at hearing loss frequencies (conditions B and C) with a previously untested “active control,” condition (A). In Study 1, all the participants were trained for 30 min per day on 5 days each week for 4 weeks. In study 2, all the participants were trained on condition A for either 15 min per day for 4 weeks, or 1 h per day for 2 weeks. We adopted self‑report (Tinnitus Handicap Questionnaire, THQ) and psychoacoustic outcome measures of tinnitus, we provided full familiarization of those measurement procedures before the baseline assessment, and we obtained data at 1 month follow‑up. Overall there was a reduction in tinnitus distress (THQ scores) that was significant within the training period and again at 1‑month follow‑up [Figure 3]. However, against the general hypothesis, our results indicated that benefit was not specifically associated with training that provided enrichment at hearing‑loss frequencies, because benefits were also present for the “control” group in condition (A). Although there was a noticeable increase in dominant tinnitus pitch in participants who trained in condition (A), overall there was no significant change in tinnitus loudness, Figure 3: Improvements on Tinnitus Handicap Questionnaire (THQ) score after frequency discrimination training. Data are the mean THQ scores (±95% confidence intervals) for 70 individuals who completed a course of 10 h training over a 4‑week period. Compared to baseline, mean THQ score was significantly reduced after 2‑weeks training and at a 4‑week follow‑up assessment (*, P < 0.05) Noise & Health, March-April 2013, Volume 15 Hoare, et al.: Sound‑based tinnitus treatment dominant pitch or bandwidth after training. Further work is needed to assess the reliability of these findings and to investigate whether any changes might be in terms of generic cognitive effects such as changes in the focus of selective attention. Points to consider in the design of device evaluation trials Standards for conducting clinical trials include the Consolidated Standards of Reporting Trials (CONSORT) and the CONSORT supplement for non‑pharmacological interventions.[71] This standard provides rigorous review criteria for RCTs and hence the appropriate transparency to evaluate the merits of these clinical approaches. Although the guidelines provided by the CONSORT criteria are principally aimed at study review, they do describe many of the key components that a high‑quality clinical trial should either document or incorporate into their study design. Indeed, our recent trial of FDT was designed specifically with these standards in mind.[50] Although focused on auditory perceptual training, some of the recommendations in our previous review[55] are equally valid for any studies that set out to evaluate the efficacy of a technological sound‑based device to be used as part of a tinnitus treatment program. Specific recommendations for future trials were, (i) use a combination of quantitative (e.g., neuroimaging) and qualitative (e.g., validated questionnaire) outcome measures, (ii) choose a qualitative outcome measure that is sensitive to change (i.e., preferably not the Tinnitus Handicap Inventory), (iii) be able to have confidence in the stability of the pre‑treatment baseline for outcome measures, (iv) choose an active control, i.e., compare to more than “no intervention,” and (v) demonstrate longer‑term patient benefits. Many of the clinical interventions reviewed here comprise treatment regimes, which include sound stimulation in the context of a structured assessment and counseling package that is individualized to each patient profile. It has been argued that sound therapies actually result in little or no benefit over and above that offered by the psychological component of tinnitus therapy.[72] Indeed psychological therapies, including cognitive behavior therapy, are well known to be effective at relieving tinnitus distress.[55] Two questions for further consideration are highly relevant to the UK perspective, if not elsewhere too. First, are audiologists (working in the National Health Service (NHS)) and hearing‑aid dispensers (on the high street) sufficiently skilled and supported to administer psychological or counseling interventions?[73] Second, is the additional cost and resource implication of a multi‑component treatment package really worth it? These are provocative, but valid, questions given the “culture shift” towards availability and marketing of new technological sound‑based interventions. We would therefore welcome high‑quality evidence of efficacy and cost benefits provided by large‑scale randomized controlled clinical trials. Noise & Health, March-April 2013, Volume 15 Conclusions and future directions In this paper, we have briefly introduced the reader to the putative physiological mechanisms of tinnitus within the central auditory system (hyperexcitability, reorganization of frequency tuning, spontaneous hyperactivity, and modulation by emotional processing). Although many of the recent technological innovations for individualized sound‑based interventions make reference to central auditory mechanisms as a key, underlying principle for their efficacy, there is insufficient rigorous neurophysiological evidence as yet to strongly support those claims. We would therefore advocate the use of both qualitative and quantitative outcome measures, including neuroimaging where feasible, as preand post‑intervention assessments. Ultimately, the most comprehensive perspective on treatment efficacy and its neural mechanism of action will be informed by such trial designs. Acknowledgments DJH, MS, and DAH are funded by the National Institute for Health Research (NIHR) Biomedical Research Unit Program. however, the views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. PA is funded by the UK Medical Research Council. Address for correspondence: Dr. Derek Hoare, NIHR Nottingham Hearing Biomedical Research Unit, Ropewalk House, 113 The Ropewalk, Nottingham, UK, NG1 5DU. E‑mail: derek.hoare@nottingham.ac.uk References 1. Hoffman HJ, Reed GW. Epidemiology of tinnitus. In: Snow JB, editor. Tinnitus: Theory and Management 2000. Hamilton, Ontario: BC Decker Inc; 2004. p. 16‑41. 2. Lockwood AH, Salvi RJ, Burkard RF. Tinnitus. N Engl J Med 2002;347:904‑10. 3. Saunders JC. The role of central nervous system plasticity in tinnitus. J Commun Disord 2007;40:313‑34. 4.Silverstein H. Transmeatal labyrinthectomy with and without cochleovestibular neurectomy. Laryngoscope 1976;86:1777‑91. 5. Langguth B. A review of tinnitus symptoms beyond ringing in the ears: A call to action. Curr Med Res Opin 2011;27:1635‑43. 6. Searchfield G. A commentary on the complexity of tinnitus management: Clinical guidelines provide a path through the fog. Eval Health Prof 2011;34:421‑8. 7. Jastreboff PJ, Jastreboff MM. Tinnitus Retraining Therapy (TRT) as a method for treatment of tinnitus and hyperacusis patients. J Am Acad Audiol 2000;11:162‑77. 8. Hoare DJ, Gander PE, Collins L, Smith S, Hall DA. Management of tinnitus in English NHS audiology departments: An evaluation of current practice. J Eval Clin Pract 2012;18:326‑34. 9. Noreña AJ. An integrative model of tinnitus based on a central gain controlling neural sensitivity. Neurosci Biobehav Rev 2011;35:1089‑109. 10.Adjamian P, Sereda M, Hall DA. The mechanisms of tinnitus: Perspectives from human functional neuroimaging. Hear Res 2009;253:15‑31. 11.Gerken GM, Hesse PS, Wiorkowski JJ. Auditory evoked responses 114 Hoare, et al.: Sound‑based tinnitus treatment in control subjects and in patients with problem‑tinnitus. Hear Res 2001;157:52‑64. 12.Diesch E, Andermann M, Flor H, Rupp A. Interaction among the components of multiple auditory steady‑state responses: Enhancement in tinnitus patients, inhibition in controls. Neuroscience 2010;167:540‑53. 13. Hoke M, Feldmann H, Pantev C, Lütkenhöner B, Lehnertz K. Objective evidence of tinnitus in auditory evoked magnetic fields. Hear Res 1989;37:281‑6. 14. Hoke ES, Mühlnickel W, Ross B, Hoke M. Tinnitus and event‑related activity of the auditory cortex. Audiol Neurootol 1998;3:300‑31. 15. Noreña A, Cransac H, Chéry‑Croze S. Towards an objectification by classification of tinnitus. Clin Neurophysiol 1999;110:666‑75. 16. Jacobson GP, Ahmad BK, Moran J, Newman CW, Tepley N, Wharton J. Auditory evoked cortical magnetic field (M100‑M200) measurements in tinnitus and normal groups. Hear Res 1991;56:44‑52. 17.Colding‑Jørgensen E, Lauritzen M, Johnsen NJ, Mikkelsen KB, Saermark K. On the evidence of auditory evoked magnetic fields as an objective measure of tinnitus. Electroencephalogr Clin Neurophysiol 1992;83:322‑7. 18. Attias J, Urbach D, Gold S, Shemesh Z. Auditory event related potentials in chronic tinnitus patients with noise induced hearing loss. Hear Res 1993;71:106‑13. 19. Hari R, Kaila K, Katila T, Tuomisto T, Varpula T. Interstimulus interval dependence of the auditory vertex response and its magnetic counterpart: Implications for their neural generation. Electroencephalogr Clin Neurophysiol 1982;54:561‑9. 20. Vernon JA. Pathophysiology of tinnitus: A special case– Hyperacusis and a proposed treatment. Am J Otol 1987;8:201‑2. 21. Jastreboff PJ, Hazell JW. A neurophysiological approach to tinnitus: Clinical implications. Br J Audiol 1993;27:7‑17. 22.Gu JW, Halpin CF, Nam EC, Levine RA, Melcher JR. Tinnitus, diminished sound‑level tolerance, and elevated auditory activity in humans with clinically normal hearing sensitivity. J Neurophysiol 2010;104:3361‑70. 23.Eggermont JJ, Roberts LE. The neuroscience of tinnitus. Trends Neurosci 2004;27:676‑82. 24. Seki S, Eggermont JJ. Changes in spontaneous firing rate and neural synchrony in cat primary auditory cortex after localized tone‑induced hearing loss. Hear Res 2003;180:28‑38. 25. Recanzone GH, Schreiner CE, Merzenich MM. Plasticity in the frequency representation of primary auditory cortex following discrimination training in adult owl monkeys. J Neurosci 1993;13:87‑103. 26. Noreña AJ, Gourévitch B, Aizawa N, Eggermont JJ. Spectrally enhanced acoustic environment disrupts frequency representation in cat auditory cortex. Nat Neurosci 2006;9:932‑9. 27.Thai‑Van H, Micheyl C, Moore BC, Collet L. Enhanced frequency discrimination near the hearing loss cut‑off: A consequence of central auditory plasticity induced by cochlear damage? Brain 2003;126:2235‑45. 28. Moore BC, Vinay SN. Enhanced discrimination of low‑frequency sounds for subjects with high‑frequency dead regions. Brain 2009;132:524‑36. 29. Engineer ND, Riley JR, Seale JD, Vrana WA, Shetake JA, Sudanagunta SP, et al. Reversing pathological neural activity using targeted plasticity. Nature 2011;470:101‑4. 30.Noreña AJ, Eggermont JJ. Changes in spontaneous neural activity immediately after an acoustic trauma: Implications for neural correlates of tinnitus. Hear Res 2003;183:137‑53. 31.Llinás RR, Ribary U, Jeanmonod D, Kronberg E, Mitra PP. Thalamocortical dysrhythmia: A neurological and neuropsychiatric syndrome characterized by magnetoencephalography. Proc Natl Acad Sci U S A 1999;96:15222‑7. 32.Weisz N, Moratti S, Meinzer M, Dohrmann K, Elbert T. Tinnitus perception and distress is related to abnormal spontaneous brain activity as measured by magnetoencephalography. PLoS Med 2005;2:E153. 33.Weisz N, Müller S, Schlee W, Dohrmann K, Hartmann T, Elbert T. The neural code of auditory phantom perception. J Neurosci 2007;27:1479‑84. 34. Weisz N, Dohrmann K, Elbert T. The relevance of spontaneous activity for the coding of the tinnitus sensation. Prog Brain Res 2007;166:61‑70. 35. Dohrmann K, Elbert T, Schlee W, Weisz N. Tuning the tinnitus percept by modification of synchronous brain activity. Restor Neurol Neurosci 115 2007;25:371‑8. 36. van der Loo E, Gais S, Congedo M, Vanneste S, Plazier M, Menovsky T, et al. Tinnitus intensity dependent gamma oscillations of the contralateral auditory cortex. PLoS One 2009;4:E7396. 37. De Ridder D, Elgoyhen AB, Romo R, Langguth B. Phantom percepts: Tinnitus and pain as persisting aversive memory networks. Proc Natl Acad Sci U S A 2011;108:8075‑80. 38.Rauschecker JP, Leaver AM, Mühlau M. Tuning out the noise: Limbic‑auditory interactions in tinnitus. Neuron 2010;66:819‑26. 39. Vanneste S, Plazier M, der Loo Ev, de Heyning PV, Congedo M, De Ridder D. The neural correlates of tinnitus‑related distress. Neuroimage 2010;52:470‑80. 40. Irwin A, Hall DA, Peters A, Plack CJ. Listening to urban soundscapes: Physiological validity of perceptual dimensions. Psychophysiology 2010;48:258‑68. 41.Mühlau M, Rauschecker JP, Oestreicher E, Gaser C, Röttinger M, Wohlschläger AM, Simon F, et al. Structural brain changes in tinnitus. Cereb Cortex 2006;16:1283‑8. 42.Melcher JR, Knudson IM, Levine RA. Subcallosal brain structure: Correlation with hearing threshold at supra‑clinical frequencies (>8 kHz), but not with tinnitus. Hear Res 2013;295:79‑86. 43. Leaver AM, Seydell‑Greenwald A, Turesky TK, Morgan S, Kim HJ, Rauschecker JP. Cortico‑limbic morphology separates tinnitus from tinnitus distress. Front Syst Neurosci 2012;6:21. 44.Hauptmann C, Tass PA. Therapeutic rewiring by means of desynchronizing brain stimulation. Biosystems 2007;89:173‑81. 45. Tass PA, Adamchic I, Freund HJ, von Stackelberg T, Hauptmann C. Counteracting tinnitus by acoustic coordinated reset neuromodulation. Restor Neurol Neurosci 2012;30:137‑59. 46.Mantini D, Perrucci MG, Del Gratta C, Romani GL, Corbetta M. Electrophysiological signatures of resting state networks in the human brain. Proc Natl Acad Sci U S A 2007;104:13170‑5. 47.Reavis KM, Chang JE, Zeng FG. Patterned sound therapy for the treatment of tinnitus. Hear J 2010;63:21‑4. 48. Zeng FG, Tang Q, Dimitrijevic A, Starr A, Larky J, Blevins NH. Tinnitus suppression by low‑rate electric stimulation and its electrophysiological mechanisms. Hear Res 2011;277:61‑6. 49.Lu T, Liang L, Wang X. Temporal and rate representations of time‑varying signals in the auditory cortex of awake primates. Nat Neurosci 2001;4:1131‑8. 50. Liang L, Lu T, Wang X. Neural representations of sinusoidal amplitude and frequency modulations in the primary auditory cortex of awake primates. J Neurophysiol 2002;87:2237‑61. 51. Reavis KM, Rothholtz VS, Tang Q, Carroll JA, Djalilian H, Zeng F‑G. Temporary suppression of tinnitus by modulated sounds. J Assoc Res Otolaryngol 2012;13:561‑571. 52. Davis PB, Wilde RA, Steed LG, Hanley PJ. Treatment of tinnitus with a customized acoustic neural stimulus: A controlled clinical study. Ear Nose Throat J 2008;87:330‑9. 53. Davis PB, Paki B, Hanley PJ. Neuromonics Tinnitus Treatment: Third clinical trial. Ear Hear 2007;28:242‑59. 54.Goddard JC, Berliner K, Luxford WM. Recent experience with the neuromonics tinnitus treatment. Int Tinnitus J 2009;15:168‑73. 55.Hoare DJ, Kowalkowski VL, Kang S, Hall DA. Systematic review and meta‑analyses of randomized controlled trials examining tinnitus management. Laryngoscope 2011;121:1555‑64. 56.Henry JA, Istvan J. An independent review of neuromonics tinnitus treatment controlled clinical trials. Aust N Z J Med 2010;32:41‑55. 57. Davis PB, Wilde RA. Clinical trial of a new tinnitus masking technique. In: Reich GE, Vernon JA, editors. Proceedings of the Fifth International Tinnitus Seminars. Portland, Oregon: American Tinnitus Association; 1996. p. 305‑9. 58.Davis PB, Wilde RA, Steed LG. Trials of tinnitus desensitisation music: Neurophysiology‑influenced rehabilitation. In: Patuzzi R, editor. Proceedings of the Seventh International Tinnitus Seminars. Perth, Australia: The University of Western Australia; 2002. p. 74‑7. 59. Kuk F, Peeters H, Lau C. The efficacy of fractal music employed in hearing aids for tinnitus management. Hear Rev 2010;17:32‑42. 60.Jeppesen AM, Andersen HP. Tinnitus and the Widex Zen program. Widexpress; 2011.February issue, No. 27. Noise & Health, March-April 2013, Volume 15 Hoare, et al.: Sound‑based tinnitus treatment 61. Sweetow RW, Sabes JH. Effects of acoustical stimuli delivered through hearing aids on tinnitus. J Am Acad Audiol 2010;21:461‑73. 62.Herraiz C, Diges I, Cobo P, Plaza G, Aparicio JM. Auditory discrimination therapy (ADT) for tinnitus managment: Preliminary results. Acta Otolaryngol Suppl 2006;126:80‑3. 63. Herraiz C, Diges I, Cobo P. Auditory discrimination therapy (ADT) for tinnitus management. Prog Brain Res 2007;166:467‑71. 64.Herraiz C, Diges I, Cobo P, Aparicio JM, Toledano A. Auditory discrimination training for tinnitus treatment: The effect of different paradigms. Eur Arch Otorhinolaryngol 2010;267:1067‑74. 65.Norena A, Micheyl C, Chéry‑Croze S, Collet L. Psychoacoustic characterization of the tinnitus spectrum: Implications for the underlying mechanisms of tinnitus. Audiol Neurootol 2002;7:358‑69. 66.Flor H, Hoffmann D, Struve M, Diesch E. Auditory discrimination training for the treatment of tinnitus. Appl Psychophysiol Biofeedback 2004;29:113‑20. 67. Herraiz C, Diges I, Cobo P, Aparicio JM. Cortical reorganisation and tinnitus: Principles of auditory discrimination training for tinnitus management. Eur Arch Otorhinolaryngol 2009;266:9‑16. 68. Barry JG, Ferguson MA, Moore DR. Making sense of listening: The IMAP test battery. J Vis Exp 2010;44;2123. 69. Hoare DJ, Stacey PC, Hall DA. The efficacy of auditory perceptual training for tinnitus: A systematic review. Ann Behav Med 2010;40:313‑24. 70.Hoare DJ, Kowalkowski VL, Hall DA. Effects of frequency discrimination training on tinnitus: Results from two randomised controlled trials. J Assoc Res Otolaryngol 2012;13:543‑59. 71. Boutron I, Moher D, Altman DG, Schulz KF, Ravaud P, CONSORT Group. Extending the CONSORT statement to randomized trials of nonpharmacologic treatment: Explanation and elaboration. Ann Intern Med 2008;148:295‑309. 72.McKenna L, Irwin R. Sound therapy for tinnitus‑sacred cow or idol worship? An investigation of the evidence. Audiol Med 2008;6:16‑24. 73. Martinez Devesa P, Waddell A, Perera R, Theodoulou M. Cognitive behavioural therapy for tinnitus. Cochrane Database Syst Rev 2007;9:CD005233. How to cite this article: Hoare DJ, Adjamian P, Sereda M, Hall DA. Recent technological advances in sound-based approaches to tinnitus treatment: A review of efficacy considered against putative physiological mechanisms. Noise Health 2013;15:107-16. Source of Support: Nil, Conflict of Interest: DJH and DAH are principal investigators on the clinical trial of Acoustic CR Neuromodulation referred to in this manuscript.. Staying in touch with the journal 1) Table of Contents (TOC) email alert Receive an email alert containing the TOC when a new complete issue of the journal is made available online. To register for TOC alerts go to www.noiseandhealth.org/signup.asp. 2) RSS feeds Really Simple Syndication (RSS) helps you to get alerts on new publication right on your desktop without going to the journal’s website. You need a software (e.g. RSSReader, Feed Demon, FeedReader, My Yahoo!, NewsGator and NewzCrawler) to get advantage of this tool. RSS feeds can also be read through FireFox or Microsoft Outlook 2007. Once any of these small (and mostly free) software is installed, add www.noiseandhealth.org/rssfeed.asp as one of the feeds. Noise & Health, March-April 2013, Volume 15 116