Acro Synagis Form - Acro Pharmaceutical Services
advertisement

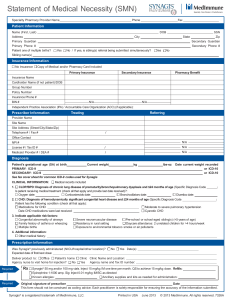
Pennsylvania Pharmacy Tennessee Pharmacy Synagis® (palivizumab) Statement of Medical Necessity Ph. 800-906-7798 Synagis Ph. 855-229-0952 For additional information, please contact your Fax 877-381-3806 Ph. 800-906-7798 x 129 account manager or visit acropharmacy.com. Fax 844-612-9057 ✂————————————————————————————————————————————————————————— PATIENT INFORMATION: PRESCRIBER INFORMATION: PATIENT NAME: ______________________________________________ SEX: M F PRESCRIBER’S NAME: __________________________________________________ ALLERGIES: _____________________________ WEIGHT: ______lbs. /kg HEIGHT: ______ MD LICENSE #: ____________________ MD NPI#: ___________________________ DATE OF BIRTH: _____________ SOCIAL SECURITY #: ____________________________ CLINIC NAME: ____________________________SPECIALTY:___________________ ADDRESS: _________________________________________________ APT#__________ CONTACT NAME: _____________________________________________________ CITY: ______________________________________ STATE: ______ ZIP: ____________ ADDRESS: _________________________________ SUITE #: ___________________ HOME PHONE: ________________________ WORK PHONE: ______________________ CITY: _________________________________ STATE: ________ ZIP: ____________ CELL PHONE: ________________________ EMAIL: ______________________________ PHONE: __________________________ FAX: _______________________________ CAREGIVER NAME: _________________________ PHONE: ________________________ EMAIL: ______________________________________________________________ INSURANCE INFORMATION: Please include copies of the patient’s insurance/drug benefit cards (front and back) to expedite benefit clearance. PRIMARY INSURANCE: ______________________________________ POLICY #: _________________________________ GROUP #: __________________________________ POLICY HOLDER: _________________________________________ EMPLOYER: __________________________ INSURANCE PHONE #: _______________________________ CLINICAL INFORMATION: To ensure prompt processing please complete all of the questions. Patient’s Gestational Age: _______ weeks _______ days Birth Weight: ________ g / kg / lbs Current Weight: ________ g / kg / lbs Date Recorded: __________ Please Document All Diagnoses and Document to the Highest Degree of ICD-10 Detail ≤ 24 Weeks of Gestation (P07.21-P07.22) 25-26 Weeks of Gestation (P07.24-P07.25) 27-28 Weeks of Gestation (P07.26-P07.27) 29-30 Weeks of Gestation (P07.32-P07.33) 31-32 Weeks of Gestation (P07.34-P07.35) 33-34 Weeks of Gestation (P07.36-P07.37) 35 Weeks of Gestation (P07.38) Other Respiratory Conditions of Fetus & Newborn – ICD-10: ____ Secondary Diagnosis (If Applicable): ___________ Breakthrough RSV Hospitalization Additional Risk Factors: Child Care Attendance by the Infant Home or Facility Sibling(s) Younger than 5 Years of Age Living in the Same Household. Medical Criteria (Please attach clinical documentation for all diagnoses below) 1. Diagnosis of Chronic Lung Diseases (CLD) (ICD-10:P27.8)? Yes No Oxygen Concentration: ___________ Dates: ___________ Supporting Clinical Documents are attached for Oxygen Use. Bronchodilator Corticosteroids Diuretics ___ / ___ /___ ___ / ___ /___ ___ / ___ /___ 2. Diagnosis of Hemodynamically Significant Congenital Heart Disease? Yes No IDC-10: ___________ Patient has the following conditions: Diagnosis of Moderate-Severe Pulmonary Hypertension Cyanotic Heart Disease Acyantoic Heart Disease Medications for CHF (list): _______________ Last Date Received: ___ / ___ /___ Recent Surgical Procedure Requiring Cardiopulmonary Bypass Yes No If yes, an additional post-operative dose of palivizumab may be medically necessary. NICU History Yes No NICU Name: ________________________________ Please Attach the NICU Discharge Summary Was there a NICU Dose Administered? Yes No Dates: ____ / ____ /____ 3. Diagnosis of Cystic Fibrosis with one of the following risk factors? Yes No IDC-10: ___________ Clinical Evidence of CLD Nutritional Compromise Manifestations of sever lung disease (previous hospitalization for pulmonary exacerbation in the first year of life or abnormalities on chest radiography or chest computed tomography that persist when stable) Weight for length less than 10th percentile 4. 5. Diagnosis of profoundly immunocompromised? Reason: _______________________ Diagnosis of Congenital Abnormalities of the airway and 12 months of age or less? Yes No IDC-10: ___________ Neuromuscular condition that compromises handling of respiratory secretions and 12 months of age or less? Yes No IDC-10: ___________ Expected Date of First/Next Injection: ___ / ____ / ____ Previous Injections? Yes No Dates: ____ / ____ /____ Rx Synagis (palivizumab) 50 mg and/or 100 mg Vials Sig: Inject 15 mg/kg IM One Time per Month Dispense Quantity: QS Refills Through: ____ / ____ /____ Other: Parent/Caregivers have been contacted and we have been granted permission to contact. 6. Agency Nurse to Visit Home for Injection? Yes No Prescribers Signature: ______________________________________ Date: ____________ Dispense as Written Deliver Medication to: Patient’s Home ________________________________________ Date: __________________ Substitution Permissible Physician’s Office Other: ___________________________ Requested Date of Delivery: ________________________ Thank you for using Acro Pharmaceutical Services! Important Notice: This communication contains information that is confidential and protected from disclosure. If the reader of this message is not the intended recipient, employee or agent responsible for delivering the message to the intended recipient, you are hereby notified that any dissemination, distribution, or copying of this communication is strictly prohibited. ______________________________________ If you have received this communication in error, please reply to the sender thatDate: you have received the message in error and destroy this copy. Prescriber’s Signature