V.A.C. GranuFoam Silver® Dressings
The Only Antimicrobial Silver Foam Dressing
Specifically Engineered for Use with V.A.C.® Therapy
Archel Ambrosio, Ph.D., PMP | Robert Wilkes, MSME, PE | Joanna Payne, BS | KCI USA, Inc. (KCI) | San Antonio, TX
Contents
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Foam Structure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Finite Element Analysis . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Granulation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Sustained Antimicrobial Activity . . . . . . . . . . . . . . . . . . 11
Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Introduction
Adjunctive silver dressings are frequently used with V.A.C.® Therapy and are placed between the wound bed and
the V.A.C.® GranuFoam™ Dressing to prevent or control infection. However, these adjunctive silver dressings may
compromise the benefits of V.A.C. Therapy in promoting granulation tissue formation and could potentially affect
clinical outcome.
The purpose of this paper is to demonstrate the value of using V.A.C. GranuFoam Silver® Dressings with V.A.C.
Therapy. The research will also show how using an adjunctive silver dressing between the wound bed and V.A.C.
GranuFoam Dressings could interfere with the benefits of the foam dressing on healing with V.A.C. Therapy.
We will also demonstrate how the V.A.C. GranuFoam Silver Dressing maintains the properties of V.A.C. GranuFoam
Dressings that are critical to wound healing. Since the V.A.C. GranuFoam Silver Dressing is designed specifically for
use with V.A.C. Therapy Systems, this dressing provides the full benefits of V.A.C. Therapy, with the antimicrobial
benefits of silver in a one-step, user-friendly design.
Ionic silver has long been recognized as an effective antimicrobial against a broad spectrum of pathogens and is
considered to be biocompatible with mammalian tissue.1-6 Unlike traditional antibiotics, ionic silver binds to and
damages microbial cell walls at multiple sites and has various mechanisms of action.7,8 The existence of these
multiple sites and various antimicrobial mechanisms of action makes it difficult for microorganisms to develop
defense mechanisms against the multi-pronged attack of silver.
Thus, silver became the antimicrobial of choice when the V.A.C. GranuFoam Silver Dressing was designed. Maintaining
the reticulated open-cell, foam (ROCF) structure of the V.A.C. GranuFoam Dressing was a critical design element.
The V.A.C. GranuFoam Dressing was used as the substrate onto which silver was coated in a thin and uniform layer
such that the reticulated, open-cell structure of the foam was maintained. The silver used in the dressing is 99.9%
pure metallic silver, and it is bonded to the foam using a proprietary technology.
Foam Structure
The application of V.A.C. Therapy induces micromechanical effects at the dressing-to-tissue interface resulting
in characteristic tissue undulations and cell stretching, which in turn results in increased cell proliferation. Such
microstrain have only been demonstrated when ROCF dressings, such as V.A.C. GranuFoam Dressings and V.A.C.
GranuFoam Silver Dressings, are used (Figure 1).9 This reinforces the importance of maintaining the structure of the
V.A.C. GranuFoam Dressing and its physical properties after applying the silver coating to the foam. These properties
are key design characteristics necessary to help promote wound healing by enhancing granulation tissue formation
and ultimately contributing to successful clinical outcomes.9-11
2
V.A.C. GranuFoam Silver® Dressings
Figure 1. (Upper Right & Left) Application of V.A.C.® Therapy to wound induces surface undulations, stretching cells in the wound. (Below
Right) Wound with 7 days of V.A.C. Therapy using foam has a higher surface area (solid blue line) and more blood vessels than an area of
the same wound not exposed to the foam (Below Left).9 Reprinted with permission from Saxena V, Hwang CW, Huang S, et al.. VacuumAssisted Closure: Microdeformations of Wounds and Cell Proliferation. Plast Reconstr Surg 2004;114(5):1087.
3
As it was essential that V.A.C. GranuFoam Silver maintain a pore dimension similar to V.A.C. GranuFoam, it was
important to design the coating to be thin enough so as not to reduce the pore size of the foam substantially. Scanning
electron microscopy (SEM) shows a silver coating thickness of approximately 3 μm, thus preserving the 400-600 μm
pore size of the dressing (Figure 2).
Figure 2. SEM image showing a silver coating
thickness of approximately 3 μm.
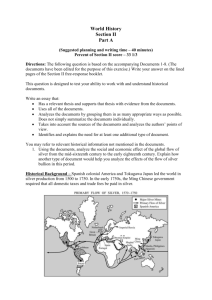
Equally important is the retention of the reticulated open-cell, foam structure, which is demonstrated through an
SEM of the foam structure (Figure 3a). Since, in clinical practice, the dressing is often cut into the size and shape of
the wound, it was also important that the silver coating was evenly distributed along and around the struts of the
foam throughout the entire dressing. SEM with energy dispersive x-ray spectroscopy (EDS) analysis for silver demonstrates that silver (as indicated by the green dots) is evenly distributed throughout the entire dressing (Figure 3b).
3a
3b
Figure 3. a) SEM image showing open cell, reticulated structure of V.A.C. GranuFoam Silver® Dressings.
b) SEM image with EDS analysis demonstrating even distribution of silver throughout the entire dressing.
4
V.A.C. GranuFoam Silver® Dressings
By retaining the same reticulated open-cell, structure of V.A.C. GranuFoam, the V.A.C. GranuFoam Silver Dressing
provides the same pressure distribution characteristics as V.A.C. GranuFoam (Figure 4). As shown in this figure, the
pressure measured at the wound-contacting surface of the V.A.C. GranuFoam Silver Dressing is similar to the pressure
setting of the therapy unit (-125mmHg) and is almost identical to that for the V.A.C. GranuFoam Dressing. Anything
that alters the wound contacting interface, such as the use of antimicrobial silver interface layers, may affect the
delivery of negative pressure to the wound. As illustrated in Figure 4, a significant pressure drop was observed within
an hour of the application of negative pressure when a commonly used antimicrobial silver dressing was used as an
interface layer in conjunction with the V.A.C. GranuFoam Dressing (P<0.01).
Figure 4. Negative pressure distribution
profile as a function of time of V.A.C.
GranuFoam Silver® Dressings and V.A.C.®
GranuFoam™ Dressing with an antimicrobial
silver interfacial layer.
Finite Element Analysis
The reticulated, open-cell structure of V.A.C. GranuFoam Silver combined with negative pressure is also vital in
providing the appropriate microstrain to the wound, which is essential to granulation tissue formation. Thus,
anything that alters this structure will also affect microstrain and by extension, granulation tissue formation.
Computer finite element analysis (FEA) was used to demonstrate this by evaluating the effect of V.A.C. GranuFoam
on microdeformations on the wound bed. A soft tissue model, representing the wound bed, was formulated from
earlier published work.12-13
5
Since the base material of V.A.C. GranuFoam Silver is V.A.C. GranuFoam, and because it has been demonstrated
that the silver coating does not compromise the open-cell, reticulated structure of the dressing, a microCT 3D image
of V.A.C. GranuFoam was used for the baseline geometry. The greatest strains were found to occur in specific areas
relative to the foam microarchitecture (Figure 5). The greatest dilatational (volumetric) compression was found in the
tissue beneath the strut contact. Adjacent to this area was the largest distortional strain. At the “hilltop” regions
between the struts, distortion was minimal, while dilatational expansion was at its highest value.
Figure 5. Areas on the wound bed where strain occurs during V.A.C.® Therapy with V.A.C.® GranuFoam™ Dressing.
Overall, the maximum compressive and tensile strains are significantly higher (p < 0.05) for V.A.C. GranuFoam than
that for V.A.C. GranuFoam with an antimicrobial interface layer (Acticoat® 7 [Smith & Nephew] or Silverlon® NPD
[Argentum Medical LLC]). This is illustrated visually in Figure 6, where the highest principal strains are seen in the
V.A.C. GranuFoam model (indicated by the red areas) and the tell-tale undulations corroborate the results illustrated
in Figure 1.
Quantitatively, Figure 7 demonstrates that V.A.C. GranuFoam had significantly higher compressive strains at
-125mmHg pressure setting than when an antimicrobial interfacial layer was used. Similarly, tensile strains were
significantly higher (p < 0.05) for V.A.C. GranuFoam than for V.A.C. GranuFoam with a silver interfacial layer (Figure
8). A statistical analysis using the Kruskal-Wallis test for data with non-normal distribution indicated that the differences in compressive and tensile strain between V.A.C. GranuFoam and the antimicrobial interfacial layer + V.A.C.
GranuFoam samples were statistically significant (p <0.05).
6
V.A.C. GranuFoam Silver® Dressings
A
B
C
Figure 6. Wound bed FEA microdeformation results at 125mmHg negative pressure for V.A.C.® GranuFoam™ Dressing alone (a), Acticoat 7
with V.A.C. GranuFoam overlay (b) and Silverlon NPD with V.A.C. GranuFoam Overlay (c). The color contours correspond to maximum
principal strain in megapascals (MPa).
7
Figure 7. Maximum compressive strain (mm/mm) at 125mmHg negative pressure for V.A.C.® GranuFoam™
Dressing, V.A.C. GranuFoam + Acticoat 7 and V.A.C. GranuFoam + Silverlon NPD. Differences between V.A.C.
GranuFoam and the antimicrobial interfacial layer + V.A.C. GranuFoam samples were statistically significant (P<0.05).
Figure 8. Maximum tensile strain (mm/mm) at 125mmHg negative pressure for V.A.C.® GranuFoam™ Dressing,
V.A.C. GranuFoam + Acticoat 7 and V.A.C. GranuFoam + Silverlon NPD. Differences between V.A.C. GranuFoam
and the antimicrobial interfacial layer + V.A.C. GranuFoam samples were statistically significant (P<0.05).
8
V.A.C. GranuFoam Silver® Dressings
Thus, this FEA study showed the use of an antimicrobial interface layer between the wound-contacting surface of
V.A.C. GranuFoam and the wound bed drastically reduced the tissue strain. This was corroborated by placing the
samples on top of a translucent gel-like substrate (Dermasol DS-300 [California Medical Innovations]) and sealing
it with drape, followed by taking photographs through the gel at a 45 degree angle (Figure 9). Figure 9a shows a
relatively smooth surface on the Dermasol. After compression of the foam, pronounced indentations on the gel was
observed (Figure 9b), which correspond to the highest principal strains in the FEA model. These indentations were
minimized when antimicrobial interfacial layers were used between the foam and the Dermasol (Fig. 9c & 9d).
Figure 9. Microdeformation patterns induced by
-125mmHg pressure.
9a
a)V.A.C.® GranuFoam™ Dressing on
Dermasol, before compression
b) V.A.C. GranuFoam on Dermasol
after compression
c) Acticoat 7 between V.A.C. GranuFoam and Dermasol after compression
d) Silverlon NPD between V.A.C. GranuFoam and Dermasol after compression.
9b
9c
Acticoat
Imprint
9d
Silverlon
Imprint
9
Granulation
To assess the performance of the GranuFoam Silver Dressing, a porcine model of acute wound healing was used to
show that granulation formation rates would not be compromised through the addition of the silver component to
the V.A.C. GranuFoam Dressing. A total of 9 domesticated Yorkshire pigs (55-63 kg) each received four 5cm fullthickness dorsal wounds on each side of the spine under a protocol approved by an Institutional Animal Care and Use
Committee for a total of 72 wounds. Each of the 3 treatment groups consisted of a total of 24 randomly selected
full-thickness wound sites.
A three-factor (location, treatment, and time) repeated measures of variance analysis was performed to compare
rates of granulation for the V.A.C. GranuFoam Dressing and V.A.C. GranuFoam Silver Dressing treatment groups
using a 95% confidence interval. On an intra-treatment assignment basis, changes from baseline (Day 0) were
evaluated using a paired-difference t-test. Each dressing was placed in accordance with the manufacturer’s instructions
for use. Specifically, each V.A.C. Dressing was sized to fit the shape of each wound and sealed with a V.A.C. Drape. A
V.A.C. Therapy unit was then applied at 125mmHg of continuous negative pressure, and dressing changes occurred
every 48 hours. A total of 4 dressing changes occurred through the duration of the study, at which point complete
granulation was achieved on Day 8.
Volumetric wound measurements were taken following wound creation on Day 0 and upon removal of the dressings
on Days 2, 4, 6, and 8. The methodology to quantify wound volume involved covering and sealing each wound site
with an adhesive drape, injecting sterile saline with a 25cc syringe, and completely filling the void in the wound bed
to be flush with the adjacent intact skin.14
Figure 10 shows the rates of granulation measured by differences in wound volume. No significant differences were
detected among the baseline volume measurements, suggesting that the initial wound volumes were equivalent
between the two treatment groups. While physical evaluations, as well as FEA, indicated that the silver coating
on the V.A.C. GranuFoam Silver Dressing did not adversely affect granulation tissue formation, this in vivo study
reported comparable rates of granulation tissue formation for both ROCF dressings, providing conclusive evidence
that the addition of the silver component to the V.A.C. GranuFoam dressing did not negatively affect granulation
tissue formation.
10
V.A.C. GranuFoam Silver® Dressings
Figure 10. Rates of granulation determined by average wound volume measurement.
Sustained Antimicrobial Activity
In order to evaluate the antimicrobial efficacy of V.A.C. GranuFoam Silver, the dressing was subjected to daily
repeated bacterial challenge over a period of 3 days following the ASTM E2149 standard test method for
determining antimicrobial activity under dynamic contact conditions. The challenge organisms included grampositive and gram-negative bacteria as well as antibiotic-resistant bacteria. A sample of the dressing was added to
50 mL of the challenge organism at a concentration of approximately 105 – 107 CFU/mL and incubated at 37°C. At
pre-determined time points, the surviving organisms were plated and triplicate counts were performed to determine
the concentration of surviving organisms. After 24 hours, the same dressing was placed in fresh inoculum, and 24
hours later bacterial concentration was determined for the 48-hour time point. This process was repeated for the
72-hour time point.
The results indicated that within 30 minutes of exposure of Staphylococcus aureus, Pseudomonas aeruginosa and
Methicillin-resistant Staphylococcus aureus (MRSA) to the V.A.C. GranuFoam Silver Dressing, bacterial concentration
decreased by greater than a 4-log reduction (Figure 11), with a percent bacterial reduction of at least 99.9%.
11
Figure 11. Microbial reduction by V.A.C. GranuFoam Silver® Dressings within 30 minutes of exposure
of gram-positive, gram-negative and antibiotic-resistant bacteria to the dressing.
This microbial reduction was sustained over a period of 24 to 72 hours after daily repeated challenge of the same
dressing sample with fresh inoculum of the various microorganisms tested, (Figure 12). It is important that the
dressing demonstrate antimicrobial activity against common wound pathogens such as S. aureus, P. aeruginosa,
Escherichia coli, MRSA and vancomycin-resistant enterococcus (VRE) within a 24-, 48- and 72-hour period, because
these are the clinically relevant time points in the treatment of a wound with V.A.C. Therapy and correspond to the
dressing change intervals recommended in the V.A.C. Therapy Clinical Guidelines.15
Figure 12. Antimicrobial activity of V.A.C. GranuFoam Silver® Dressings over a period
of 72 hours after daily repeated challenge with bacteria.
12
V.A.C. GranuFoam Silver® Dressings
Also noteworthy is the fact that V.A.C. GranuFoam Silver has been shown to inhibit the in vitro growth of more than
150 microorganisms.16 These results, along with the other test results, highlight the ability of V.A.C. GranuFoam Silver
with V.A.C. Therapy to provide the antimicrobial benefits of silver combined with the full benefits of V.A.C. Therapy.
Conclusion
Studies have demonstrated that the V.A.C. GranuFoam Silver Dressing, which is specifically designed for use with
V.A.C. Therapy, provides the full benefits of V.A.C. Therapy by retaining the physical properties of traditional V.A.C.
GranuFoam while offering the antimicrobial protection of silver. The reticulated, open cell structure of the foam
allows the even delivery of negative pressure across the entire wound and the efficient removal of exudate.
Additionally, this pore morphology, along with negative pressure, enables microdeformations of the wound tissue,
which assist granulation tissue formation as demonstrated in a non-infected swine model of acute wound healing.
The direct and complete dressing-to-tissue contact that results from the physical properties of the foam and negative
pressure coupled with the immediate and sustained antimicrobial activity of the V.A.C. GranuFoam Silver Dressing
against common pathogens may help to reduce infection in indicated wound types.
In summary, the V.A.C. GranuFoam Silver® Dressing provides the full benefits of V.A.C.® Therapy when used with
negative pressure, while offering antimicrobial protection against gram-positive and gram-negative bacteria, as well
as antibiotic-resistant bacteria in a one-step, user-friendly design.
References
1. Vanscheidt W, Lazareth I, Routkovsky-Norval C. Safety evaluation of a new ionic silver dressing in the management of chronic ulcers. Wounds 2003;15(11):371-378.
2. O’Meara SM, Cullum NA, Majid M, et al. Systematic review of antimicrobial agents used for chronic wounds. Br. J. Surg. 2001;88:4-21.
3. White RJ. An historical overview of the use of silver in wound management. Br. J. Nurs. 2001;10:S3-8.
4. Demling RH, DiSanti L. The role of silver technology in wound healing: Effects of silver on wound management. Wounds 2001;13(5):15-21.
5. Burrell RE, Heggers JP, Davis GJ, et al. Efficacy of silver-coated dressings as bacterial barriers in rodent burn sepsis model. Wounds 1999;11(4):64-71.
6. Tredget EE, Shankowsky HA, Groeneveld A, et al. A matched-pair, randomized study evaluating the efficacy and safety of Acticoat silver-
coated dressing for the treatment of burn wounds. J. Burn Care Rehabil. 1998;19:531-537.
7. Ovington LG. The truth about silver. Ostomy Wound Management 2004;50(9A Suppl):1S-10S.
8. Driver VR. Silver dressings in clinical practice. Ostomy Wound Management 2004;50(9A Suppl):11S-15S.
9. Saxena SM, Hwang C, Huang S, et al. Vacuum-assisted closure: Microdeformations of wounds and cell proliferation. Plast. Reconstr. Surg. 2004;114:1086-1096.
10. Joseph E, Hamori CA, Bergman S, et al. Prospective randomized trial of Vacuum-assisted closure versus standard therapy of chronic non-
healing wounds. WOUNDS 2000;12(3):60-67.
11. Clare MP, Fitzgibbons TC, McMullen ST, et al. Experience with the vacuum assisted closure negative pressure technique in the treatment of non-healing diabetic and dysvascular wounds. Foot Ankle Int. 2002;23(10):896-901.
12. Wilkes R, Zhao Y, Kieswetter K, et al. Effects of dressing type on 3D tissue microdeformations during negative pressure wound therapy; a computational study. J. Biomech. Eng. 2009;131:031012-1-031012-12.
13. Oomens CW, Bresser OF, Bosboom EM, et al. Deformation analysis of a supported buttock contact. Proceedings of the 2001
Bioengineering Conference, American Society of Mechanical Engineers, June 27-July1, 2001. Snowbird, Utah: American Society of
Mechanical Engineers; 2001.
14. KCI Data on file.
15.V.A.C.® Therapy Clinical Guidelines, August 2010.
16. KCI Data on file.
13
V.A.C. GranuFoam Silver® Dressings
The Only Antimicrobial Silver Foam Dressing
Specifically Engineered for Use with V.A.C.® Therapy
NOTE: Specific indications, contraindications, warnings, precautions and safety information exist for KCI products and therapies.
Please consult a physician and product instructions for use prior to application.
©2006-2012 KCI Licensing, Inc. All rights reserved. Unless otherwise indicated, all trademarks designated herein are proprietary to KCI
Licensing, Inc., its affiliates and/or licensors. This material is intended for healthcare professionals only. DSL#11-0751.OUS (Rev. 5/12)