MAJOR ARTICLE
In Vitro Studies of a Novel Antimicrobial
Luer-Activated Needleless Connector for Prevention
of Catheter-Related Bloodstream Infection
Dennis G. Maki
Section of Infectious Diseases, Department of Medicine, University of Wisconsin School of Medicine and Public Health and the University
of Wisconsin Hospital and Clinics, Madison
Background. We report in vitro studies of a commercially available novel antimicrobial Luer-activated connector with the inner surface coated with nanoparticle-silver to prevent contaminants from forming biofilm and
causing catheter-related bloodstream infection.
Methods. Sterile control nonmedicated connectors and antimicrobial connectors were filled with ∼1 ⫻ 10 5 cfu/
mL of Staphylococcus epidermidis, methicillin-resistant Staphylococcus aureus, vancomycin-resistant Enterococcus,
Enterobacter cloacae, Pseudomonas aeruginosa, or Candida albicans; after 24 h of incubation, the numbers of
remaining viable microorganisms were quantified and compared with the concentration in control connectors
(∼1 ⫻ 107 cfu/mL). In trials simulating clinical use, septal membranes of connectors were inoculated with E. cloacae,
were allowed to dry, and were then actuated and infused with lactated ringer’s solution for 72 h, with sampling
for microorganisms in downstream efferent fluid and for biofilm in the connector.
Results. Microorganisms suspended in the intraluminal fluid path of antimicrobial connectors were rapidly
killed. For 5 species, there was a 5.23–6.80 mean log10 reduction (199.999%), and with C. albicans, there was a
99.9% reduction. In clinical simulation trials, heavy contamination of downstream fluid was detected at all time
points with control connectors, reaching ∼1 ⫻ 10 5 cfu/mL at 72 h, and heavy biofilm was uniformly present; with
the antimicrobial connectors, there was complete prevention of downstream fluid contamination and total absence
of biofilm formation.
Conclusions. These simulation experiments show that needleless connectors readily acquire an internal biofilm
when microorganisms gain access to the internal fluid path and that biofilm formation allows an exponential
buildup of internal contamination, with shedding back into the fluid path and downstream sufficient to cause
bacteremia. Incorporation of nanoparticle silver into the lining surfaces of the novel connector kills microorganisms
in the fluid pathway and prevents internal biofilm formation, even with high levels of introduced contamination
and continuous fluid flow. This technology deserves to be evaluated in a prospective, randomized clinical trial to
determine its capacity to prevent catheter-associated bloodstream infection.
More than 500,000 intravascular device-related bloodstream infections (BSIs) occur in the United States each
year, the majority caused by central venous catheters
(CVCs) [1]. CVC-related BSIs are associated with prolongation of hospital stay and added costs to the health
care system of $33,000–$65,000 per case [2, 3].
Microorganisms cause CVC-related infection when
Received 18 June 2009; accepted 21 February 2010; electronically published
10 May 2010.
Reprints or correspondence: Dennis G. Maki, H4/574-University of Wisconsin
Hospital and Clinics, Madison, WI 53792 (dgmaki@medicine.wisc.edu).
Clinical Infectious Diseases 2010; 50(12):1580–1587
2010 by the Infectious Diseases Society of America. All rights reserved.
1058-4838/2010/5012-0005$15.00
DOI: 10.1086/652764
1580 • CID 2010:50 (15 June) • Maki
they gain access to the surface of the implanted device
where they can establish a biofilm [4, 5], allowing sustained surface colonization and, ultimately, dissemination into the bloodstream. With short-term intravascular devices—peripheral intravenous catheters, arterial
catheters, and noncuffed and nontunneled CVCs—
most catheter-related BSIs originate from skin of the insertion site and gain access extraluminally and occasionally intraluminally [6–8]. With long-term devices—
cuffed and tunneled CVCs, totally implanted central
venous ports, and peripherally inserted central venous
catheters (PICCs)—intraluminal contaminants are the
major cause of device-related BSI [9–13].
Needleless valved connectors for CVCs have come
into near-universal use throughout the United States
as part of the national movement to reduce the risk to health
care workers of biohazardous sharps injuries and exposure to
bloodborne viruses, such as human immunodeficiency virus,
hepatitis B virus, and hepatitis C virus, following the Occupational Safety and Health Administration’s Needlestick Safety
and Prevention Act of 2000 [14–16]. A recent meta-analysis
has shown that these devices have reduced the incidence of
biohazardous needlestick injuries in health care workers [17].
Unfortunately, over the past 15 years a growing number of
reports have suggested that valved needleless connectors are
associated with significantly increased risks of CVC-associated
BSI [18–27]. In most of these reports, the adoption of a new
Luer-activated, valved needleless connector by a hospital or
home care infusion therapy program—usually replacing a splitseptum connector—has been associated with an abrupt and
significant increase in the incidence of nosocomial BSI, particularly CVC-associated BSIs. Multiple manufacturers’ valved
connectors have been implicated in these reports. In a number
of institutions, increased rates of BSI persisted despite intensified efforts to achieve a high level of compliance with infection control practices to prevent CVC-associated BSI, including routinely vigorously disinfecting the membranous septum
of the connector before actuation and entry, and BSI rates decreased only after discontinuing use of the new valved connector [18–27].
Frequent handling and access of catheter hubs, needless connectors, and injection ports has been shown to put patients at
increased risk of CVC-associated primary BSI [18, 20–22, 28],
presumably because they facilitate entry of microorganisms into
the connector and fluid path. In support of this hypothesis,
studies have shown a high incidence of biofilm formation on
the interior surface of valved connectors that have been used
clinically [29].
Although needleless connectors and injection ports are rec-
ognized sites of access for microbial contamination, no national
standard exists defining the best and recommended form of
antiseptic preparation to prevent microbial entry when the needleless connector or injection port is accessed. Although studies
have examined the efficacy of various disinfectants to remove
microorganisms from the membranous surface of needleless
connectors or injection ports [28, 30–32], there have been no
randomized clinical trials that have prospectively examined the
efficacy of various approaches to disinfection of connectors for
prevention of CVC-related BSI. Most importantly, numerous
studies have shown that if there is significant contamination
of the membranous septum prior to actuation, conventional
disinfection may fail to prevent entry of microorganisms [28,
30–36].
It seems clear that there is an urgent need to develop new
technologies that can implicitly reduce the risk of contamination of needleless connectors and associated BSI. We report
in vitro studies of a novel antimicrobial luer-activated connector,
with a nanoparticle-silver coating of the entire surface, to ascertain its capacity to resist internal fluid contamination and biofilm
formation and potential to confer protection against catheterassociated BSI.
METHODS
The novel antimicrobial needleless connector. The novel antimicrobial connector evaluated in this study (V-Link; Baxter
Healthcare) is an adaptation of the company’s nonmedicated
single-use, disposable, luer-activated, valved connector constructed of polycarbonate (Clearlink; Baxter Healthcare), which
is designed to connect an administration set or extension set
to a vascular catheter and provide needleless access for administration of fluid or withdrawal of blood specimens. However,
with the exception of the silicone membranous septum, the
Figure 1. Internal structure of the novel antimicrobial connector. The entire polycarbonate surface contains nanoparticles of silver.
Antimicrobial Needleless Connector for Prevention of BSI • CID 2010:50 (15 June) • 1581
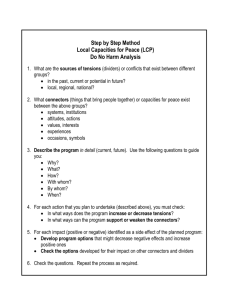
Figure 2. Design of Study 3, a clinical simulation with heavy contamination of the membranous septum of the connector before actuation and
continuous use for 72 h, to assess the capacity of the connector to resist internal biofilm formation and downstream contamination of efferent
intravenous fluid flowing into the patient. A sufficient number of control and antimicrobial connectors was studied in this trial to permit sampling of
infusate as well as assess biofilm formation on the interior surface of the connector at each sampling period for 36 trials with control connectors
and 36 with antimicrobial connectors.
entire surface of the antimicrobial connector (Figure 1), including the entirety of the internal fluid path and the external
casing, has a novel nanoparticle silver coating (V-Link with
VitalShield; Baxter Healthcare) to prevent introduced contamination and internal biofilm formation within the device, with
the goal of reducing the risk of catheter-associated BSI. The
device is not intended to be used as a treatment for established
catheter-related BSI.
Study 1: Antimicrobial efficacy, 24-hour challenge. This
study was designed to test the capacity of the antimicrobial
device to resist contamination of the fluid path, by killing high
concentrations of microorganisms present in the fluid path,
when tested immediately after removal from the sterile package.
Sterile control nonmedicated connectors and antimicrobial
connectors were actuated (the administration set was attached
to the device, penetrating the membranous septum, triggering
the internal valve as the luer connection is completed) and
flushed with sterile saline, then filled with ∼1 ⫻ 10 5 cfu/mL of
test microorganisms in bacteriologic media containing 0.1%
neopeptone, 0.25% glucose, and 1% bovine serum. After incubation for 24 h, the number of remaining viable microorganisms was quantified and compared with the final concentration in control connectors. Bacteriologic media containing
large quantities of protein was employed to provide a worstcase challenge to the device, similar to what might be encountered in clinical use with total parenteral nutrition admixtures
or blood, because ionic silver binds to thiol residues, quenching its antibacterial activity [37].
Tests were performed with suspensions of pure cultures of
6 recent clinical isolates of each of the following microorganisms: Staphylococcus epidermidis, methicillin-resistant Staphylococcus aureus, vancomycin-resistant Enterococcus faecium, Enterobacter cloacae, Pseudomonas aeruginosa, and Candida albicans.
All devices to be tested were sterilized and flushed with sterile
saline prior to inoculation. The internal fluid path of each device
was challenged by aseptically infusing ∼2 mL of the microbial
suspension through the device with a syringe to ensure that the
entire 0.25-mL fluid-path volume was exposed. After the inoc-
Figure 3. Results of Study 1, the 24-h challenge of connectors with approximately 1 ⫻ 107 cfu/mL of 6 species of nosocomial pathogens. The
antimicrobial device demonstrated the a rapid killing of suspended microorganisms within the intraluminal fluid path. With 5 of the 6 species tested,
there was a 5.23–6.80 mean log10 reduction (199.999%), compared with controls, and with Candida albicans, there was a 99.9% reduction.
1582 • CID 2010:50 (15 June) • Maki
Figure 4. Results of Study 2, the microbial challenge after 96 h of repeated actuation and continuous infusion through the connector. It can be
seen that the 96-h challenge had minimal effect on the capacity of the antimicrobial connectors to rapidly kill microorganisms within the intraluminal
fluid path.
ulum was instilled, the syringe was removed and the device was
oriented top end down and transferred to a sealed container with
residual moisture to prevent evaporation. The device was incubated at 37C for 24 h, using the bacteriologic incubation
temperature rather than room temperature (25C) to provide an
even greater microbial challenge to the device. After incubation,
the connectors were flushed with 2.5 mL of sterile saline containing Tween 20 and sodium thioglycolate to neutralize any
remaining ionic silver [37]. The recovered fluid was then cultured
quantitatively by plating serial 10-fold dilutions on trypticase soy
agar plates in triplicate, which were incubated at 37C in a temperature-controlled incubator for 48 h, after which the number
of surviving microorganisms was enumerated.
Study 2: Antimicrobial efficacy, 96-hour challenge. This
study was designed to assess the persistence of surface antimicrobial activity on the interior of the device after exposure
to stresses intended to simulate 96 h of continuous heavy clinical use. This was achieved via repeated chemical disinfection
of the membranous surface with isopropyl alcohol, multiple
actuations and prolonged continuous infusion of intravenous
fluid through the connector. After exposing the test connectors
to repeated actuations and continuous infusion with normal
saline for 96 h, connectors were inoculated with the same 6
test microorganisms in bacteriologic media, incubated and sampled using the same protocol as in Study 1.
Study 3: Clinical simulation trial with assessment biofilm
formation. This study was intended to simulate clinical use
of the test connectors and to assess their capacity to resist
contamination of the fluid path and internal biofilm formation,
despite heavy contamination of the membranous portion of
the connector at the time of actuation and initiation of continuous flow of intravenous fluid for 72 h. As depicted in Figure
2, the membranous surface of each test connector was disinfected with 70% isopropyl alcohol, which was allowed to dry,
after which it was inoculated with ∼1 ⫻ 10 3 cfu/mL of E. cloacae
(ATCC 2355) suspended in lactated Ringer’s with 5% dextrose
solution with 1% fetal bovine serum and again allowed to dry.
The connector was then actuated with the male Luer adapter
of a Continu-Flo infusion set (Baxter Healthcare), which was
connected to a 1- liter bag of 5% dextrose-in-lactated Ringer’s
solution (Baxter Healthcare) containing 1% trypticase soy
broth. Fluid was infused at 25C at a rate of 0.5 mL/min for
72 h. Aliquots of infusate from the distal end of an extension
tubing connected to the outflow portion of the connector,
which were immediately frozen until culturing, were collected
at baseline, during hours 1–5, and after 24, 48, and 72 h. Concentrations of viable E. cloacae in each aliquot were determined
by plating and culturing serial dilutions in triplicate.
For ascertaining biofilm formation, the exterior surface of
the connector was disinfected with sterile gauze saturated with
Antimicrobial Needleless Connector for Prevention of BSI • CID 2010:50 (15 June) • 1583
Figure 5. Results of the clinical simulation trial to assess the capacity of the connector to resist internal biofilm formation and downstream
contamination of intravenous fluid flowing into the patient. The control connectors rapidly became contaminated and significant contamination of
downstream intravenous fluid was seen by 48 h of continuous infusion. In contrast, the antimicrobial connectors provided near-complete protection
from downstream contamination of fluid and totally prevented internal biofilm formation.
a 1:10 dilution of commercial bleach, which was then inactivated with sterile 5% sodium thiosulfate. The connectors were
then cut in half longitudinally with a sterilized pipecutter (Spear
and Jackson). Both halves were immersed in a container of
sterile 0.9% saline and rinsed by gentle agitation. One half was
placed in a tube with 10 mL of a fixing solution of 2% glutaraldehyde in 1N cacodylate buffer and refrigerated prior to
processing for scanning electron microscopy.
When processing for scanning electron microscopy, samples
were purged of glutaraldehyde by rinsing with 0.1 mol/L cacodylate buffer solution, after which they were dehydrated by
serial exposure to 25%, 35%, 50%, 70%, 80%, 90%, and 95%
ethanol for 10 min each, followed by a dehydration step with
200-proof ethanol, twice, for 20 min. The samples were then
solidified by serial exposure to 2:1, 1:1, and 1:2 ethanol:hexamethyldisilazane baths, each for 15 min, followed by a 100%
hexamethyldisilazane solidification 3 times, each for 15 min.
The samples were then allowed to dry at room temperature
overnight, after which they were mounted on aluminum supports, affixed with carbon tape, and the surfaces sputter-coated
with palladium. They were then examined by scanning electron
microscopy.
The approximate number of microorganisms present in the
biofilm was quantified by processing the other half of the bivalved device by placing it in a 50-mL centrifuge tube containing 10 mL of sterile saline with 0.01% Tween 80 and sodium
thioglycolate and vortexing vigorously 3 times, each for 1 minute, then sonicating for 3 min. Ten-fold dilutions of the solution
were plated and cultured in triplicate.
1584 • CID 2010:50 (15 June) • Maki
RESULTS
Study 1: Antimicrobial efficacy, 24-hour challenge. With all
of the control devices tested immediately after removal from
the package, contamination of the contained fluid increased to
∼1 ⫻ 107 cfu/mL by 24 h. The antimicrobial device showed a
powerful capacity to rapidly kill microorganisms within the
intraluminal fluid path. With 5 of the 6 species tested, there
was a 5.23–6.80 mean log10 reduction (199.999%) compared
with controls; with C. albicans, there was a 99.9% reduction
(Figure 3).
Study 2: Antimicrobial efficacy, 96-hour challenge. In this
experiment, despite heavy manipulation and continuous infusion of normal saline for 96 h before instilling the inoculum
and incubating for 24 h, the antimicrobial connectors showed
durable capacity to rapidly kill the initial inoculum and prevent
growth of microorganisms within the intraluminal fluid path.
There was a 3.0–6.8 mean log10 reduction (99.9%–99.9999%
reduction), compared with control nonmedicated connectors
(Figure 4), which again demonstrated a rapid increase in contamination to ∼1 ⫻ 107 cfu/mL.
Study 3: Clinical simulation trial with assessment biofilm
formation. In all 36 trials with control connectors, large numbers of microorganisms were detected in efferent infusate (Figure 5). Approximately 1 ⫻ 10 2 cfu/mL were detected at 1 h,
1 ⫻ 10 3 at 48 h, and 1 ⫻ 10 5 at 72 h. Commensurate biofilm
formation was present at each of these sampling periods (Figure 6).
In contrast, only 1–3 cfu/mL were detected at 1 h in 5 of
36 trials with antimicrobial connectors, with no detectable fluid
Figure 6. Scanning electron microscopy of connectors after 72 h of exposure in Study 3 (magnification, ⫻10,000). The control connectors all had
a heavy biofilm observed on scanning electron microscopy, with ∼1 ⫻ 104 cfu recovered per connector, whereas none of the antimicrobial connectors
demonstrated any biofilm formation on scanning electron microscopy, and all were sterile in culture.
contamination thereafter (Figure 5). There was no biofilm formation whatsoever detected at any of the sampling periods
(Figure 6).
DISCUSSION
Numerous epidemics of nosocomial BSI have been traced to
the entry of microorganisms through the lumen of the catheter
into the patient’s bloodstream, most often in contaminated
infusate [1]. However, in a growing number of recent outbreaks,
needleless valved connectors for CVCs appear to have become
extrinsically contaminated by microorganisms which traversed
the septal membrane to colonize the internal surface of the
connector, presumably resulting in the formation of a biofilm
and shedding of microorganisms into the fluid path [18–27].
Unfortunately, there have not been adequate studies to assess
the relative importance of this mechanism of microbial access
as a cause of endemic CVC-related BSI. However, Donlan et
al [29] found that up to 63% of randomly sampled needleless
connectors in clinical use demonstrated viable biofilms.
The in vitro simulation studies we report demonstrate unequivocally the capacity of microorganisms to gain access to
the interior of the connector at the time of actuation or, later,
during continuous use to rapidly form a luxurious biofilm
which, within 24–48 h, begins to shed into the fluid path downstream (Figure 5) and ultimately into the bloodstream of the
patient receiving the infusion. Moreover, studies have shown
that if there is significant contamination of the membranous
septum prior to actuation, conventional disinfection often fails
to prevent entry of microorganisms [28, 30–36].
With the recent reports that many hospitals in the United
States have experienced increased rates of nosocomial BSI that
appear to be related to commercial needless connectors that
are being used universally, particularly with CVCs or peripherally-inserted CVCs [1827], it seems clear that there is an
urgent need for the development of novel technologies to reduce the risk of in-use contamination of connectors which can
cause catheter-related BSI. It is noteworthy that the first technologic approaches to preventing contamination of CVC-administration set-catheter connections by use of a povidoneiodine “shield” [33] or a novel antiseptic-containing connector
showed greatly reduced rates of CVC-associated BSI in trials
in Europe, where there was a very high baseline incidence of
CVC-associated infection [34–36].
The novel nanosilver-impregnated polycarbonate valved needleless connector we have studied was recently approved by the
Food and Drug Administration and is now in use in many
hospitals in the United States. The nanosilver particles are stably imbedded in the polycarbonate matrix and release minute
quantities of bactericidal ionic silver off the surface into the
fluid path. Simulation studies have shown that the total amount
of ionic silver eluted into the fluid pathway with continuous
infusion—and infused into the patient—is ∼0.80 mg per day,
resulting in an incremental increase in the blood level of silver
of ∼0.05 ng/mL. This is far below levels of silver exposure
considered to pose a risk to human health; silver concentrations
in drinking water up to 100 mg/L are considered to be safe by
the United States Environmental Protection Agency, and mean
blood silver levels in unexposed healthy humans range from
0.2–5 ng/mL [38, 39]. The amounts of silver entering the bloodstreams of patients exposed to this nanosilver-impregnated connector are magnitudes less than occurs in patients treated with
topical silver sulfadiazine or silver dressings, where blood levels
of silver can reach hundreds of micrograms per milliliter [38].
Most absorbed silver is excreted in the feces and urine.
Antimicrobial Needleless Connector for Prevention of BSI • CID 2010:50 (15 June) • 1585
Our in vitro studies (Studies 1 and 2), which posed microbial
challenges to the antimicrobial connector far beyond those
likely be encountered in clinical practice and used incubation
temperatures of 37C and high concentrations of protein in
nutrient media, similar to what would be encountered with
infusion of warmed blood or protein-containing total parenteral nutrition admixtures, demonstrate that incorporation of
the nanoparticle-silver coating onto the interior surfaces of the
polycarbonate connector rapidly kills microorganisms in the
fluid path and prevents biofilm formation, even in the presence
of high concentrations of protein that can sequester silver and
neutralize its antibacterial activity [37]. With 5 of the 6 species
tested, there was a 5.23–6.80 mean log10 reduction (199.999%),
compared with controls (Figure 3), and with C. albicans, there
was a 99.9% reduction. Stressing connectors for 96 h with
repeated actuations and a continuous infusion had no material
effect on the capacity of the connectors to rapidly kill microorganisms suspended in the internal fluid path (Figure 4). Even
more importantly, in Study 3, which simulated clinical use by
exposing connectors to heavy contamination and continuous
flow for 72 h, there was near-total prevention of downstream
fluid contamination (Figure 5) and complete suppression of
biofilm formation (Figure 6).
In conclusion, this promising novel technology deserves to
be evaluated in prospective, adequately powered, randomized clinical trials with catheter-associated BSI as the primary
outcome measure [40], to ascertain its capacity to prevent
bacteremia deriving from in-use contamination of needless
connectors.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
Acknowledgments
I am grateful to Winnie Kubey (Sr. Research Scientist-Microbiology,
Baxter); Dustin Cawthon (Engineering Specialist-NPD, Baxter), and David
Lamb, PhD, (Group Product Manager, Baxter) for insightful scientific input
during the design and conduct of these studies, and to Paul Straka, Mark
Hunter, Steve Strathmann, James Diorio, and Neal Zupec, Baxter Healthcare Technology Park, IL, for excellent laboratory support and professional
consultation.
Financial support. Baxter Healthcare.
Potential conflicts of interest. D.G.M. designed studies reported, analyzed the data, and wrote the manuscript but has received no compensation from Baxter Healthcare for this research, for consultation, or for
participation in company-sponsored continuing medical education programs. D.G.M.: no conflicts.
15.
16.
17.
18.
19.
References
1. Crnich CJ, Maki DG. Infections caused by intravascular devices: epidemiology, pathogenesis, diagnosis, prevention, and treatment. In:
APIC Text of Infection Control and Epidemiology. 2nd ed. Vol 1.
Washington D.C.: Association for Professionals in Infection Control
and Epidemiology, 2005:24.1–24.26.
2. Pittet D, Tarara D, Wenzel RP. Nosocomial bloodstream infection in
critically ill patients: excess length of stay, extra costs and attributable
mortality. JAMA 1994; 271:1598–1601.
3. Orsi GB, Di Stefano L, Noah N. Hospital-acquired, laboratory-con-
1586 • CID 2010:50 (15 June) • Maki
20.
21.
22.
firmed bloodstream infection: increased hospital stay and direct costs.
Infect Control Hosp Epidemiol 2002; 23:190–197.
Marrie TJ, Costerton JW. Scanning and transmission electron microscopy of in situ bacterial colonization of intravenous and intraarterial
catheters. J Clin Microbiol 1984; 19:687–693.
Murga R, Miller JM, Donlan RM. Biofilm formation by gram-negative
bacteria on central venous catheter connectors: effect of conditioning
films in a laboratory model. J Clin Microbiol 2001; 39:2294–2297.
Bjornson HS, Colley R, Bower RH, Duty VP, Schwartz-Fulton JT, Fischer JE. Association between microorganism growth at the catheter
insertion site and colonization of the catheter in patients receiving total
parenteral nutrition. Surgery 1982; 92:720–727.
Mermel LA, McCormick RD, Springman SR, Maki DG. The pathogenesis and epidemiology of catheter-related infection with pulmonary
artery Swan-Ganz catheters: a prospective study utilizing molecular
subtyping. Am J Med 1991; 91(suppl 3B):1897–1205.
Safdar N, Maki DG. The pathogenesis of catheter-related bloodstream
infection with short-term noncuffed central venous catheters. Intensive
Care Med 2004; 30:62–67.
Sitges-Serra A, Puig P, Linares J, et al. Hub colonization as the initial
step in an outbreak of catheter-related sepsis due to coagulase negative
staphylococci during parenteral nutrition. JPEN J Parenter Enteral Nutr
1984; 8:668–672.
Raad I, Costerton W, Sabharwal U, Sacilowski M, Anaissie E, Bodey GP.
Ultrastructural analysis of indwelling vascular catheters: a quantitative
relationship between luminal colonization and duration of placement.
J Infect Dis 1993; 168:400–407.
Cheesbrough JS, Finch RG, Burden RP. A prospective study of the mechanisms of infection associated with hemodialysis catheters. J Infect Dis
1986; 154:579–589.
Safdar N, Maki DG. The risk of catheter-related bloodstream infection
with peripherally-inserted central venous catheters used in the inpatient
setting. Chest 2005; 128:489–495.
Garland JS, Alex CP, Sevallius JM, et al. Pathogenesis of catheter-related
bloodstream infections in neonates with peripherally-inserted central
venous catheters (PICCs): a cohort study with molecular epidemiology.
Infect Control Hosp Epidemiol 2008; 29:243–249.
Tan L, Hawk III, JC, Sterling ML; for the Council on Scientific Affairs,
American Medical Association. Report of the Council on Scientific Affairs. Preventing needlestick injuries in health care settings. Arch Intern
Med 2001; 161:929–936.
Centers for Disease Control and Prevention. Public Health Service
guidelines for the management of health-care worker exposures to HIV
and recommendations for postexposure prophylaxis. MMWR Morb
Mortal Wkly Rep 1998; 47:1–33.
Management of Occupational Exposures to Hepatitis B, Hepatitis C
and HIV and Recommendations for Postexposure prophylaxis, Updated U.S. Public Health Service Guidelines, 2001. http://www.cdc.gov/
ncidod/hip/guide/phspep.htm. Accessed 18 June 2009.
Tuma S, Sepkowitz KA. Efficacy of safety-engineered device implementation in the prevention of percutaneous injuries: a review of published studies. Clin Infect Dis 2006; 42:1159–70.
Danzig LE, Short LJ, Collins K, et al. Bloodstream infections associated
with a needleless intravenous infusion system in patients receiving
home infusion therapy. JAMA 1995; 273:1862–1864.
Kellerman S, Shay DK, Howard J, et al. Bloodstream infections in home
infusion patients: the influence of race and needleless intravascular
access devices. J Pediatr 1996; 129:711–717.
Cookson ST, Ihrig M, O’Mara EM, et al. Increased bloodstream infection rates in surgical patients associated with variation from recommended use and care following implementation of needleless device.
Infect Control Hosp Epidemiol 1998; 19:23–27.
McDonald LC, Banerjee SN, Jarvis WR. Line-associated bloodstream
infections in pediatric intensive-care-unit patients associated with a
needleless device and intermittent intravenous therapy. Infect Control
Hosp Epidemiol 1998; 19:772–777.
Do AN, Ray BJ, Banerjee SN, et al. Bloodstream infection associated
23.
24.
25.
26.
27.
28.
29.
30.
with needleless device use and the importance of infection-control practices in the home health care setting. J Infect Dis 1999; 179:442–448.
Maragakis LL, Bradley KL, Song X, et al. Increased catheter-related
bloodstream infection rates after the introduction of a new mechanical
valve intravenous access port. Infect Control Hosp Epidemiol 2006;
27:67–79.
Field K, McFarlane C, Cheng AC, et al. Incidence of catheter-related
bloodstream infection among patients with a needleless, mechanical
valve-based intravenous connector in an Australian hematology-oncology unit. Infect Control Hosp Epidemiol 2007; 28(5):610–613.
Salgado CD, Chinnes L, Paczesny TH, Cantey JR. Increased rate of
catheter-related bloodstream infection associated with use of a needleless mechanical valve device at a long-term acute care hospital. Infect Control Hosp Epidemiol 2007; 28:684–688.
Rupp ME, Sholtz LA, Jourdan DR, et al. Outbreak of bloodstream
infection temporally associated with the use of an intravascular needleless valve. Clin Infect Dis 2007; 44:1408–1414.
Jarvis WR, Murphy C, Hall KK, et al. Health care-associated bloodstream infections associated with negative- or positive-pressure or displacement mechanical valve needleless connectors. Clin Infect Dis 2009;
49:1821–1827.
Luebke MA, Arduino MJ, Duda DL, et al. Comparison of the microbial
barrier properties of a needleless and conventional needle-based intravenous access system. Am J Infect Control 1998; 26:437–441.
Donlan RM, Murga R, Bell M, et al. Protocol for detection of biofilms
on needleless connectors attached to central venous catheters. J Clin
Microbiol 2001; 39:750–753.
Salzman MB, Isenberg HD, Rubin LG. Use of disinfectants to reduce
microbial contamination of hubs of vascular catheters. J Clin Microbiol
1993; 31:475–479.
31. Arduino MJ, Bland LA, Danzig LE, et al. Microbiologic evaluation of
needleless and needle-access devices. Am J Infect Control 1997; 25:377–
380.
32. Menyhay SZ, Maki DG. Disinfection of needless catheter connectors
and access ports with alcohol may not prevent microbial entry: the promise of a novel antiseptic-barrier cap. Infect Control Hosp Epidemiol 2006;
27:23–27.
33. Halpin DP, O’Byrne P, McEntee G, et al. Effect of a betadine connection
shield on central venous catheter sepsis. Nutrition 1991; 7:33–34.
34. Stotter AT, Ward H, Waterfield AH, et al. Junctional care: the key to
prevention of catheter sepsis in intravenous feeding. JPEN J Parenter
Enteral Nutr 1987; 11:159–162.
35. Inoue Y, Nezu R, Matsuda H, et al. Experimental study of hub contamination: effect of a new connection device. The I system. JPEN J
Parenter Enteral Nutr 1992; 16:178–180.
36. Segura M, Alvarez-Lerma F, Tellado JM, et al. A clinical trial on the
prevention of catheter-related sepsis using a new hub model. Ann Surg
1996; 223:363–369.
37. Liau SY, Read WJ, Pugh JR, Russell AD. Interaction of silver nitrate
with readily identifiable groups: relationship to the antibacterial activity
of silver ions. Lett Appl Microbiol 1997; 25:279–283.
38. Wan AT, Conyers RA, Coombs CJ, Masterton JP. Determination of
silver in blood, urine, and tissues of volunteers and burn patients. Clin
Chem 1991; 37(10 Pt 1):1683–1687.
39. Armitage SA, White MA, Wilson HK. The determination of silver in
whole blood and its application to biological monitoring of occupationally exposed groups. Ann Occup Hyg 1996; 40:331–338.
40. Crnich CJ, Maki DG. The promise of novel technology for the prevention of intravascular device-related bloodstream infection. I. Pathogenesis and short-term devices. Clin Infect Dis 2002; 34:1232–1242.
Antimicrobial Needleless Connector for Prevention of BSI • CID 2010:50 (15 June) • 1587