tenth pacific health ministers meeting pic10/9 27

TENTH PACIFIC HEALTH MINISTERS MEETING
Apia, Samoa
2–4 July 2013
Agenda item 9
PIC10/9
27 June 2013
ORIGINAL: ENGLISH
OUTBREAK SURVEILLANCE AND RESPONSE PRIORITIES FOR
MITIGATING THE HEALTH IMPACT OF DISASTER
Disaster risks are higher in the Pacific than in other regions. During the first six months of 2013, five major disasters impacted the Pacific, including three cyclones, an earthquake and tsunami, and a drought. Severe health and non-health consequences of disasters will continue to impact Pacific island countries and areas (PICs), and the poorest and most vulnerable populations will continue to bear the greatest burden. Climate change and related extreme weather events are expected to continue to exacerbate the impact of disasters in Pacific communities.
Disasters can increase the risk of disease outbreaks, particularly after floods or population displacements, both of which are regular consequences of disasters in the Pacific. Recent post-disaster disease outbreaks in the
Pacific included a large leptospirosis outbreak following floods in Fiji in 2012 and drought-associated diarrhoea outbreaks in Tokelau and Tuvalu in 2011.
Several PICs are working to integrate routine disease surveillance with post-disaster risk assessments and early warning surveillance and response systems. Solomon Islands, in particular, has demonstrated how to assess and respond effectively to disease threats in post-disaster settings. Many PICs need to enhance their response capacity, but insufficient human resources in technical areas continues to limit sustainable progress.
To effectively mitigate the health impact of disasters, especially the risks of disease outbreaks, PICs should prioritize post-disaster disease outbreak contingency planning and capacity-building. Key elements include developing protocols for rapid post-disaster assessment and response, characterizing the baseline epidemiology of important outbreak-prone diseases, promoting sub-regional human resource capacity-building initiatives, and supporting improved coordination between regional disaster and public health organizations and networks. Such considerations should be embedded in national disaster and public health emergency response plans.
This document calls on PICs to augment disaster preparedness and strengthen disaster response mechanisms while also reinforcing routine early warning disease surveillance and multisectoral response capacities. Regional partners and networks, such as the Pacific Public Health Surveillance Network (PPHSN) and the Pacific
Humanitarian Team (PHT), should support these priorities.
PIC10/9 page 2
1. BACKGROUND
Pacific island countries and areas (PICs) are in the highest risk category for disasters.
There have been 24 major disasters since 2009 (see Annex 1). Five PICs are ranked among the world’s top 15 at-risk countries according to the 2012 WorldRiskReport , with Vanuatu ranking first, Tonga second, Solomon Islands sixth, Papua New Guinea 12th and Fiji 15th.
1
Many PICs are particularly prone to geological disasters, including earthquakes and related disasters such as landslides and tsunamis. Weather-related disasters, specifically cyclones and severe flooding, are more frequent and have a greater cumulative impact.
PICs are inherently vulnerable to the adverse consequences of climate change as a result of their small size, topography, insularity, remoteness and limited disaster mitigation capacity.
2
Climate change is predicted to increase severe weather events, including extreme high temperatures, droughts and flood disasters. Cyclone intensity and associated precipitation are also expected to increase.
3
The Pacific can expect to continue to be adversely impacted as a result of the increased intensity of these hydrometeorological disasters.
Disasters can have a direct and immediate impact on the health status of populations, for example through traumatic injuries, as well as an indirect and delayed impact through the disruption of local health systems, transportation networks, and telecommunication, water and sanitation infrastructure. Disaster-associated infectious disease epidemics, when they do occur, are frequently delayed and not associated with the immediate disaster event, especially when the disaster is a sudden-onset event such as an earthquake or tsunami.
4
Different disaster settings can predispose an area to substantially different postdisaster epidemic risks. Specific factors associated with increased post-disaster outbreak risk include large-scale population displacement, particularly when leading to overcrowding and high population density, as well as flooding, lack of access to sanitation facilities, and an inadequate quantity and quality of water.
5
Other important post-disaster risk considerations
1
WorldRiskReport 2012. www.worldriskresport .com (accessed 14 June 2013)
2
University of Technology Sydney. Disaster response systems in the Pacific—Policy Brief for Pacific Island Countries.
March 2013. www.preventionweb.net/files/32881_32881policybriefpicnationalfinal1.pdf (accessed 10 June 2013)
3
Intergovernmental Panel on Climate Change. Special Report for managing the risks of extreme events and disasters to advance climate change adaptation. 2012. www.ipcc-wg2.gov/SREX (accessed 18 June 2013)
4 Note: the terms “epidemics” and “outbreaks” are synonymous and interchangeable, but due to the public connotation of
“epidemic” the term “outbreak” is sometimes preferred.
5
Watson J, Gayer M, Connolly M. Epidemics after Natural Disasters. Emerg Infect Dis. 2007; 13:1–5.
PIC10/9 page 3 include the level of immunity to vaccine-preventable diseases, nutritional status, presence and type of endemic and epidemic-prone diseases, and access to health care. Different disasters in different settings, even within the Pacific context, will lead to substantially different risk profiles for disease outbreaks.
The five most common causes of non-traumatic death in emergencies and disasters are diarrhoea, acute respiratory infection, measles, malnutrition and, in endemic zones, malaria. All except malnutrition are communicable diseases directly related to environmental health conditions, and even malnutrition is greatly exacerbated by communicable disease.
Disaster-affected people are particularly vulnerable to communicable diseases when the disaster and its immediate consequences reduce resistance to disease because of malnutrition, stress, fatigue and other factors and when post-disaster living conditions are unsanitary.
Situational Analysis
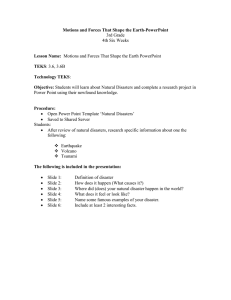
Many of the post-disaster factors that lead to high risk of epidemics are common features of disasters in the Pacific. The Marshall Islands, Tokelau and Tuvalu have experienced drought disasters since 2011, and both Tokelau and Tuvalu (see Figure 1) have experienced substantial associated diarrhoea outbreaks.
Figure 1. Diarrhoea cases reported through the Pacific Syndromic Surveillance System before and during a drought disaster — Tuvalu, 2010–2011
60
Tuvalu: Cases of Diarrhea Drought emergency
50
40
30
20
10
0
46 47 48 49 50 51 52 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40
Nov Dec
2010
Jan Feb Mar Apr May
2011
Jun Jul Aug Sep Oct
Epidemiological week
60
50
40
30
20
10
Tuvalu: Cases of Diarrhea
0
46 47 48 49 50 51 52 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40
Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct
2010 2011
Epidemiological week
PIC10/9 page 4
Flooding and/or population displacement, which are perhaps the most important factors predisposing populations to outbreaks, occur frequently in the Pacific. Sequential tropical depressions causing widespread flooding devastated much of Western Fiji in January
2012 and again in March 2012. The flooding resulted in substantial population displacement.
A significant post-disaster increase in suspected leptospirosis cases was observed in the three to eight weeks following each of the major flooding episodes (see Figure 2). Conservative estimates place the number of cases at 300 and the number of deaths at 25 following the floods.
Figure 2. Suspected leptospirosis cases after sequential flooding disasters — Western
Division, Fiji, 2012
The earthquake and subsequent tsunami on the remote Santa Cruz Islands, part of
Solomon Islands, in February 2013 led to displacement of over 40% of the population to makeshift camps, in addition to extensive damage and destruction to water systems, sanitation facilities and households. No large post-disaster outbreak was identified, but a number of outbreak alerts were identified and responded to including bloody diarrhoea, watery diarrhoea, and acute fever and rash.
PIC10/9 page 5
2. ACHIEVEMENTS AND PROGRESS
Country-level initiatives
In Fiji, soon after the flood disaster in January 2012, the Ministry of Health (MOH) established a multisectoral National Taskforce for the Control of Outbreak-Prone Diseases
(NT-COPD) to guide the post-disaster response to leptospirosis and other potential outbreakprone diseases, including typhoid fever and dengue. NT-COPD is a led by MOH and includes members from multiple sectors and external development partners. NT-COPD developed a comprehensive leptospirosis outbreak response strategy that included enhancing clinical and laboratory surveillance, upgrading leptospirosis clinical management skills with practical leptospirosis workshops, developing a comprehensive public communications strategy and developing national leptospirosis guidelines. A post-outbreak review by NT-
COPD concluded that leptospirosis, a globally neglected disease, was a very serious epidemic and endemic public health threat. The task force recommended a national summit of leptospirosis experts to address gaps in knowledge necessary for implementation of effective and efficient leptospirosis control. In May 2013, the Fiji MOH convened the International
Expert Meeting on Controlling Leptospirosis in Suva, Fiji, with 10 global leptospirosis experts and 30 country counterparts. Key outputs from the meeting were the finalization— with the Secretariat of the Pacific Community (SPC), the World Health Organization (WHO) and the University of Queensland—of a Fiji Leptospirosis National Strategic Plan and the identification of key projects, with collaboration from experts, to inform efficient leptospirosis control. The series of steps taken in Fiji, from the response to flooding and associated outbreaks to conceiving and planning the leptospirosis summit, demonstrate a strong commitment to address important public health threats.
The Federated States of Micronesia has a robust state-based series of EpiNET teams for responding to disease outbreaks in disaster and non-disaster settings. The Federated States of Micronesia has also explored how to effectively link disasters and public health emergencies through the annual Federated States of Micronesia Public Health and Hospital
Emergency Preparedness Summit. The fourth annual summit, entitled Readiness Is
Everyone’s Business, was held in Pohnpei in March 2013. The summit included all four states of the Federated States of Micronesia, plus American Samoa, the Commonwealth of the Northern Marianas Islands, Guam, the Marshall Islands and Palau. PICs shared experiences relating to state and regional public health disaster coordination and performed
PIC10/9 page 6 tabletop and full-scale disaster exercises, testing some of the key public health emergency capacities in the Federated States of Micronesia.
Following the twin earthquake and tsunami disasters on the Santa Cruz Islands, the
Solomon Islands Ministry of Health and Medical Services (MHMS) conducted a disease outbreak risk assessment to determine the risk of a post-disaster epidemic, and which, if any, diseases pose the greatest threat (see Table 1). Post-disaster disease risk assessments are a key element to ensure appropriate and targeted surveillance and response activities. The risk assessment stratified the outbreak-prone diseases and concluded that dengue was the most likely serious outbreak-prone disease, but other important disease outbreaks were possible.
One key recommendation of the risk assessment was the implementation of an early warning surveillance and response system (EWARN) to rapidly detect and respond to any increase in diseases with outbreak potential. A second key recommendation was implementation of fever surveillance using a newly developed filter-paper method to identify important etiologies of fever on the Santa Cruz Islands in the post-disaster environment.
MHMS implemented the EWARN system for three months and investigated a number of alerts that were identified when predefined disease thresholds were crossed. There were no large outbreaks, but rapid identification and response to EWARN alerts reduced the risks of small outbreaks progressing to large post-disaster epidemics. Fever surveillance provided key insight into important and unexpected etiologies of fever in this setting, including two not previously identified on the Santa Cruz Islands. This important information was communicated to clinicians in a training workshop and was used to inform local treatment protocols for undifferentiated fevers. The post-disaster risk assessment and implementation of an EWARN system in Solomon Islands is an excellent model for PICs and other countries.
MHMS and its partners are drafting a journal article to describe the risk assessment and
EWARN implementation process, including lessons learnt, that will ensure that other countries can learn from the experience of Solomon Islands.
PIC10/9 page 7
Table 1. Example of a post-disaster risk assessment matrix — Santa Cruz Islands,
Temotu Province, Solomon Islands, March 2013
Disease
Malaria
Scrub typhus
Shigella
Dengue
Hazard
Vector is present
Possibly present, not epidemic disease
Potential increase in post disasters
Vector is present, but not primary dengue vector
Leptospirosi s
Reportedly not present
Typhoid
Reportedly not present
Measles
Hepatitis A
Cholera
Reportedly not present
Reportedly not present
Only in
Papua New
Guinea
Exposure Context
Incidence decreased
No cases from screening
Health assessment found cases
Potentially hyperendemic
No increase in cases noted
Endemic in most developing countries
No documented evidence in Santa
Cruz
Good prevention methods
Lab challengin g
Treatment effective
Displaced population s
Increase in Honiara
Increased travel between Honiara and Santa Cruz
Tsunami may decrease vectors
Good prevention methods
Increased rainfall
Possibly increased with displacement and heavy rains
Poor sanitation facilities and limited access to clear water
Vaccination 86%
No cases in 2011–
2012
Increased rainfall
Unknown
Unknown
Poor sanitation facilities and limited access to clear water
Unknown
Unknown
Likelihoo d of event occurring
Medium
Low
Low
High
Unknown
Unknown
Low
Low
Low
Public health impact
Medium
Low
Medium
Medium
Medium
Medium
Medium
Low
Medium
Level of risk
Medium
Low
Low
High
Unknown
Unknown
Low
Low
Low
Regional initiatives
Pacific Public Health Surveillance Network
The Pacific Public Health Surveillance Network (PPHSN) was founded under the auspices of SPC and WHO in 1996 as a network of and for PICs. For almost 20 years,
PPHSN has been building capacity and providing expertise in outbreak surveillance and response across the Pacific. PPHSN provides PICs practical access to five service networks that correspond to the different stages of outbreak-prone disease surveillance and response
PIC10/9 page 8 during health emergencies: the Pacific Syndromic Surveillance System (PSSS) for timely detection of outbreaks; PacNet for early regional warning and communications; LabNet for identification, confirmation and characterization of causal agents; EpiNet for public health field investigations and response; and PICNet for hospital-borne infection control. In May
2012, Pacific delegates attending a meeting on the International Health Regulations (IHR
2005), the Asia Pacific Strategy for Emerging Diseases (APSED) and PPHSN confirmed that
PPHSN is very important to support surveillance and response and to fulfil IHR obligations.
The recommendations, although not specifically focusing on disasters, align with the underlying principles of this paper—that strong early warning surveillance mechanisms are fundamental to developing robust disaster preparedness plans. For a complete description of
PSSS and PPHSN see Annex 2.
International Health Regulations and Asia Pacific Strategy for Emerging Diseases
Most PICs are working to align their public health response to disasters with other public health emergency frameworks, such as IHR (2005) and/or APSED. Fourteen of the 22
PICs, which excludes New Zealand, are State Parties to IHR (2005) and use the IHR global monitoring questionnaire to assess their capacity to detect and respond to important public health emergencies. By June 2012, six of the 14 PIC State Parties reported achieving the core capacities obligations as defined in IHR. The remaining eight PICs requested a two-year extension to meet these global obligations, and all eight are actively engaged in strengthening capacities, including IHR workplan reviews, cross-sectoral IHR workshops, specific IHR capacity implementation activities, and engaging external expertise to help address specific gaps. PPHSN partners are supporting these initiatives. APSED is a tool to help countries build IHR capacities and the updated strategy, APSED (2010), was endorsed in 2010 by the
WHO Regional Committee for the Western Pacific. Both IHR and APSED build generic public health emergency capacity with substantial overlap and implications for post-disaster surveillance and response activities.
The Pacific Humanitarian Team
The Pacific Humanitarian Team (PHT) is a unique coordination mechanism to prepare for and respond to disasters in the Pacific. It consists of United Nations agencies and other major humanitarian actors. The PHT “cluster approach” is the primary global humanitarian coordination mechanism to clarify organizational roles and responsibilities during emergencies. A recent review of PHT performance found that PHT is playing a
positive role in improving partnerships and coordination of international humanitarian
PIC10/9 page 9 response in PICs in meeting challenges during the emergencies. On the country level, the national health and nutrition clusters are led by the ministries of health and supported by
PHT.
6
3. CHALLENGES AND ISSUES
Few PICs have operational plans to systematically perform post-disaster risk assessments or implement enhanced post-disaster early warning surveillance and response systems. All PICs, however, have routine early warning systems coordinated through
PPHSN’s Pacific Syndromic Surveillance System (PSSS) and, therefore, a robust framework to build additional capacity.
There is a critical lack of high-quality evidence on the epidemiology of the main outbreak-prone diseases in the Pacific. The example of the post-disaster fever surveillance on the Santa Cruz Islands that identified serious and important—but previously unrecognized— causes of fever highlights a problem common in PICs and likely in many low-resource settings. Without a detailed understanding of the prevalence, distribution and local risk factors of important outbreak-prone diseases, it will be extremely difficult to characterize post-disaster risk and ensure appropriate prioritization of limited post-disaster resources. The role of climate change on priority outbreak-prone diseases is also poorly understood and requires urgent detailed study.
Well-trained human resources are essential to develop the sustainable capacity necessary to mitigate the health impact of disasters in the Pacific. Routine surveillance capacity-building initiatives overlap with specific disaster and post-disaster needs, and there is a lack of human resource capacity in epidemiology, biostatistics, information management, disaster risk management and coordination. Many of these needs have been previously identified and overlap with other key public health priorities. At the Ninth Meeting of
Ministers of Health for the Pacific Island Countries in Honiara, Solomon Islands, in 2011, health ministers concluded that “the first step is to address the lack of trained and experienced epidemiologists in the region. There is a need to ensure that data literacy be strengthened at
6
Pacific Humanitarian Team Performance Review 2008–2012 http://reliefweb.int/sites/reliefweb.int/files/resources/Pacific%20Humanitarian%20Team%20Performance%20Review%2020
08-2012.pdf (accessed 15 June 2013)
PIC10/9 page 10 all levels of the health system.”
These challenges continue to hinder the ability to develop robust and sustainable programmes to mitigate the health impact of disaster.
Disaster response mechanisms and disease surveillance and outbreak response mechanisms require harmonization and coordination in many PICs. National and regional disaster response systems have been strengthened with the support of the Pacific
Humanitarian Team, but the link with all-hazard public health emergency plans is frequently weak. Cross-sectoral coordination, for example between national disaster management offices and ministries of health, is often challenging and requires political commitment to ensure clear delineation of responsibilities and a smooth, effective and efficient post-disaster response.
3. FUTURE DIRECTIONS
The importance of post-disaster risk assessment and specific surveillance and response activities has historically been neglected in PICs and elsewhere. Increasing engagement, as demonstrated by a request by Pacific health ministers for the current discussion of this subject, reflects increased recognition of the importance of this topic. The strengthening of post-disaster health mitigation strategies requires prioritization of the following key areas:
1) Develop and implement post-disaster health risk-assessments and early warning disease surveillance and response protocols with an emphasis on clear, simple and practical tools. These protocols should be linked with existing, routine early warning disease surveillance structures, including the Pacific Syndromic
Surveillance System (PSSS) and Pacific Public Health Surveillance Network
(PPHSN). Ensuring robust existing systems is an important foundation on which to develop disaster response capacities.
2) Prioritize operational research that investigates the epidemiology of outbreakprone diseases in the Pacific. As demonstrated in Solomon Islands, new fever surveillance tools are available to aid in the easy and accurate identification and characterization of important outbreak-prone diseases.
3) Support capacity-building initiatives to address the lack of human resource capacity in technical areas in PICs, particularly in the areas of epidemiology, data
PIC10/9 page 11 management, disaster risk management and coordination. Sufficient human resources in these key areas are essential to mitigate the adverse health impacts of disasters.
4) Implement clear policies to ensure effective coordination and division of responsibilities between national disaster management offices and ministries of health in disasters and other public health emergencies.
Regional partners and networks, in particular the Pacific Public Health Surveillance
Network (PPHSN) and the Pacific Humanitarian Team (PHT), should support these priorities.
8
9
6
7
3
4
5
10
11
12
13
14
19
20
21
22
15
16
17
18
23
24
Number
1
2
2009
2009
2009
2009
2009
2010
2010
2010
2010
2011
2011
2011
2011
2011
2012
2012
2012
2012
2012
2012
2013
2013
PIC10/9 page 13
ANNEX 1
Disaster events since 2009 that required involvement of
Pacific Humanitarian Team (PHT) for response and recovery
Year
2009
2009
Disaster
Floods (January)
Floods (February)
Country
Fiji
Solomon Islands
— Guadalcanal
Ambrym
Samoa
Tonga
Gaua
Fiji
Solomon Islands
Cooks Islands
Fiji
Solomon Islands
Vanuatu
Vanuatu
Kiribati
Tuvalu
Tokelau
Fiji
Vanuatu
Fiji
Palau
Samoa
Fiji
Solomon Islands
Marshall Islands
Volcano and Flood (April)
Tsunami (September/October)
Tsunami (September/October)
Volcano (December 2010)
TC Mick (December)
Rendova Tsunami (January)
TC Pat (February)
TC Tomas (March)
TC Ului (March)
TC Vania (January)
TC Atu (February)
Drought Response Planning (February)
Drought response (October/November)
Drought response (October/November)
Floods — TD 06F (January)
TC Wilma (March)
Floods — TD 17F (March/April)
Typhoon Bopha (November)
TC Evan (December)
TC Evan (December)
Earthquake & Tsunami (February)
Drought (April–June)
PIC10/9 page 15
ANNEX 2
Pacific Syndromic Surveillance System and Pacific Public Health Surveillance Network
The Pacific Syndromic Surveillance System (PSSS) is a routine early warning disease surveillance system implemented in 2010. Within 18 months 23 of 23 PICs were reporting (including
New Zealand and the Pitcairn Islands). PPPS is intended to improve outbreak detection by indicator based surveillance in addition to facilitating communication among PICs and other Pacific Public
Health Surveillance Network (PPHSN) members on outbreaks, disasters and other important public health threats. For example, the surge in diarrhoea cases associated with the droughts in Tokelau and
Tuvalu were identified through PSSS. An external evaluation of PSSS in 2011 reported a substantial improvement compared to previous systems by a large majority of users.
PacNet has been a cornerstone of public health surveillance, communication and coordination in PICs since 1997. PacNet is a regional early warning and alert e-mail network for outbreak preparedness, surveillance and response information purposes. PacNet allows rapid transmission of relevant information and alerts PICs to health risks and encourages them to prepare, especially for epidemics and disasters. It also provides PIC health care services with a wide range of technical manuals and well-adapted operating protocols via the PPHSN web site, such as the Pacific Outbreak
Manual and PPHSN Infection Prevention and Control Guidelines . Recent major disasters and outbreaks threats that have been documented and communicated on PacNet include the earthquake, tsunami and dengue in Solomon Islands, the drought disaster in the Marshall Islands, chikungunya in
Papua New Guinea and dengue in New Caledonia, among many others.
LabNet is a Pacific laboratory network that supports PICs to access a network of high-quality diagnostic services not available in country. These specialized laboratories provide diagnostics of agents responsible for outbreaks in the Pacific. LabNet is based on a three-tier laboratory network system with national level (Level 1) laboratories, regional referral laboratories (Level 2), for example
Institut Louis Malardé in French Polynesia and Mataika House in Fiji, and (Level 3) referral laboratories in Australia, New Zealand and the United States of America (Hawaii and mainland).
EpiNet, established in 2001, is PPHSN’s preparedness and response arm and consists of multidisciplinary national teams. National EpiNet teams should lead outbreak response in the field.
Several EpiNET teams continue to guide outbreak surveillance and response activities in country, but there are opportunities to reinforce and strengthen the current network.