The physics of retinal delamination
advertisement

The physics of retinal delamination
Tom Chou
Depts. of Biomathematics and Mathematics, UCLA, Los Angeles, CA 90095-1766
(Dated: February 25, 2012)
Retinal detachments occur when adjacent layers of tissues comprising the retina delaminate from
each other or from the underlying choriocapillaris substrate that feeds it. Taking into account experimentally measured mechanical and transport properties of retinal tissue, we build a physical
model by treating the retina as a stack of layered, active, water permeable tissues bound by cellular adhesion forces. Our model provides a mechanistic and physiological understanding of how
changes in active fluid pumping or tissue conductivity affect overall retinal stability. Theoretical
predictions on the location of first retinal delamination may help guide prevention strategies and
the development of new, physically-motivated retinal reattachment protocols.
The retina is a multilayer tissue lining the inside of the
eye. It is composed of layers of photoreceptor cells (rods
and cones) and ganglion nerve cells that conduct the electrical signals from the rods and cones. Normally, the
retina is attached to a monolayer of cells, the retinal pigment epithelium (RPE), which in turn is attached to an
collagen layer (Bruch’s membrane). The Bruch’s membrane covers the choriocapillaris substrate, a capillaryrich tissue that supplies nutrients to the retina. Figure 1
depicts the main histological features of an intact retina
[1, 2].
(a)
(b)
nerve fiber layer
ganglion cell layer
inner plexiform layer
11111111111111111111111111111
00000000000000000000000000000
00000000000000000000000000000
11111111111111111111111111111
00000000000000000000000000000
11111111111111111111111111111
000000000000000
111111111111111
000000000000000
111111111111111
choriocapillaris
inner nuclear layer
outer plexiform layer
outer nuclear layer
cones and rods
RPE
Bruch’s membrane
blood vessels
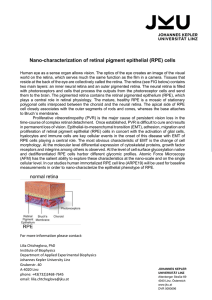
FIG. 1: (a) Histology of the retina (adapted, with permission
from http://www.anatomyatlases.org/). (b) The multiple
cell layers are labeled. The retina sits atop the retinal pigment
epithelium (RPE), a monolayer of cells that is both permeable
and that actively pumps fluid and waste products back into
the choriocapillaris. Separating the RPE from the underlying
vascularized choriocapillaris substrate that feeds the retina is
the Bruch’s membrane, a 2-4µm thick collagen sheet.
Retinal detachments disrupt the integrity of the layered retinal structure. Separation of any two retinal layers is a common mode of injury that can lead to tissue
death and vision loss [2, 3]. Often, the retina detaches
from the RPE, with fluid accumulating between the photoreceptor and RPE cell layers. However, the location
of the delamination can be highly variable. Fig. 2(a)
shows a retina that has suffered two separations with the
lower one occurring between the RPE and Bruch’s membrane, another relatively frequent site of delamination.
In Fig. 2(b), the separation has occurred at the inner
(more towards the eye interior) layer of cells, leaving the
rest of the retina and the RPE layer (thin red line) largely
intact.
(a)
(b)
FIG. 2: Optical Coherence Tomography (OCT) images of retinal separation. The lateral extent of each image is approximately 3mm. (a) Retinal detachment between the RPE and
Bruch’s membrane. Here, the RPE is lifted off the choroidal
substrate. Degeneration and crazing can also be seen interior to the outer nuclear layer. (b) Delamination of the nerve
fiber layer (NFL). Here, the outer layers, including the RPE
remain largely intact on the choriocapillaris substrate.
Detachments can be rhegmatogenous, where the retina
suffers a tear, or exudative, where fluid accumulates between layers of the retina. Traction forces on the retina
mediated through the polymeric vitreous humor in the
eye may contribute to both types of detachments. Detachments and cell layer separations can also be caused
by a variety of other factors including age, diabetes
[4], myopia, cataract surgery, infections, and tumors
[2, 3], which manifest themselves through changes in the
physical properties of the relevant tissue. For example,
changes in hydraulic conductivities have been thought to
affect retinal stability [6, 7].
Many clinical procedures have been developed to repair
or prevent separated retinas. Besides vitrectomy (surgery
to remove the vitreous that may be connected to and
pulling on the retina), pneumatic retinopexy (injection
of gas into the eye) can provide a gas-vitreous interface
allowing surface tension to reseal torn retinas [3]. Scleral
buckles have also long been used to indent the eye near
the location of retinal separation. The physical mechanism of this procedure is unclear, but is thought to involve hydrodynamic forces as the vitreous flows over the
indentation [8]. Finally, photocoagulation or cryopexy
can be used to induce microinjuries, allowing the result-
2
ing scar tissue to help re-adhere the tissue [2, 3].
Many material properties of retinal tissue have been
experimentally quantified. For example, the hydraulic
conductivities of the layers of the retina have been measured by successive laser ablation of the layers [5]. Adhesion energies between the RPE and photoreceptor cells
have been determined by classic pulling experiments
[9, 10]. Flows across various tissues, especially the active
RPE pump flux, have also been measured [11]. Although
these measured physical properties have been known to
qualitatively influence retinal stability [12, 13], how they
conspire to influence retinal stability has not been quantitatively explored. Given the wide variety of tissue types,
causative factors, locations of delamination, and treatment protocols, a mathematical model of the underlying physical mechanisms associated with delamination
is desirable. Here, we build and analyze a theoretical
model for retinal delamination that incorporates the venous pressure in the choriocapillaris Pc , the intraocular
pressure PIOP (both measurable and to some degree, controllable quantities), the hydraulic conductivity of the
cell layers Lk , active fluid pumping, and the intrinsic
maximum yield stress of the cellular adhesion bonds holding the layers together (see Fig. 3).
First, consider the molecular forces holding adjacent
tissue layers together in the absence of fluid flow and external traction forces. In the absence of fluid flow, we
define σk∗ as the maximum separation force per area that
can be sustained between tissue layers k and k − 1. In
equilibrium, externally applied normal forces lifting the
retina off the choroid (labeled T in Fig. 3(b)) act throughout all layers and the effective yield stress between layer
k and k − 1 becomes σk∗ − T . If the remaining stress arising from fluid flow and exceeds σk∗ , tissue layers k and
k − 1 will spontaneously delaminate.
We next include fluid flows and associated hydraulic
forces on the separate tissue layers. Figure 3 labels all
the relevant pressures and hydraulic conductivities of the
main tissue layers. The pressure-driven volume flux Jk
across tissue layer k is given by
PIOP
L10
L8
L4
L9
L7
L5
L3
L6
T
J
{
{
{
{
{
{
P9
P8
P6
{111111111111111111111111111111
000000000000000000000000000000
Jp
000000000000000000000000000000
111111111111111111111111111111
P4
{
1111111111111111
0000000000000000
0000000000000000
{
0000000000000000
1111111111111111
L2 1111111111111111
{
L1
P5
P3
P2
P0
L0
P7
P1
Pc
FIG. 3: Tissue layers of an attached retina (not to scale), with
the hydraulic conductivity of each layer labeled Li , and the
interlayer fluid pressures denoted Pi . The net flux J in the
inward direction and the outward RPE pump flux Jp are indicated by the long blue and short green arrows, respectively.
The most common type of delamination occurs between the
photoreceptor layer (L4 ) and the RPE (L3 ), labelled with the
extracellular pressure P3 . “RPE detachments” can also occur at the interface between the RPE and Bruch’s membrane
(L2 ), labelled with pressure P2 .
the only tissue that actively pumps fluid, the total inward
volume flow across it, instead of (1), is now
Jn = Ln ∆n − Jp (∆n ),
(2)
where the metabolically-driven outward pump flux Jp
depends on both the physiological state of the RPE
cells and possibly the intercellular pressure difference
∆n = Pn−1 − Pn across the RPE.
At steady-state, fluid incompressibility requires that
the total volume flux across each layer is constant. Summing (1) and (2) over all k and imposing Jk = J =
constant, we find the relation
∆P ≡ Pc − PIOP = J
N
X
Rj + Rn Jp (∆n ),
(3)
j=0
Jk = Lk (Pk−1 − Pk ) ≡ Lk ∆k ,
0 ≤ k ≤ N,
(1)
where P−1 ≡ Pc , PN ≡ PIOP , Lk is the hydraulic conductivity of tissue or cell layer k, and ∆k = Pk−1 − Pk
is the local pressure difference in the intercellular space
across layer k. By treating the flow resistance of each
layer in series, we can relate the total current J with a
known pressure difference ∆P ≡ Pc − PIOP .
Besides passive, pressure-driven flows, tissues can actively pump fluid across cell layers. In the eye, the RPE
monolayer of cells underneath the retinal photoreceptors
actively pumps fluid outward through the Bruch’s membrane back into the choriocapillaris. If the RPE is defined
as the nth structural layer (n = 3 in Fig. 3(b)), and is
where the resistance of layer j is Rj ≡ 1/Lj . The total
inward volume flux toward the vitreous space is thus
J=
∆P − Rn Jp (∆n )
,
RT
(4)
PN
where RT ≡ j=0 Rj is the total hydraulic resistance.
Typically, ∆P ≃ 5 − 10mm Hg [15] so that in the absence of active pumping, there is a passive inward volume
flow. Substituting (4) in ∆k = Rk J (Eq. 1), we find the
pressure difference across the k th layer:
∆k =
Rk
[∆P − Rn Jp (∆n )] ,
RT
k 6= n.
(5)
3
For the pressure difference ∆k=n across the active RPE
layer, we use J in (2) to find
∆n =
Rn
Rn
> 0.
∆P + Rn Jp (∆n ) 1 −
RT
RT
(6)
Eqs. (5) and (6) represent the flow-induced stresses
pulling apart layer k from layer k − 1. By comparing ∆k
against the total yield stresses σk∗ − T between layers, we
determine the conditions for retinal stability. For example, layer j is unstable to separation from layer j − 1 as
soon as ∆j > σj∗ − T . Since at equilibrium, the vitreous traction force −T is transduced equally through all
the layers, increasing external pulling forces alone will
not change which layer first becomes unstable. However,
layer-specific changes in adhesion energy, hydraulic conductivity Lj , or RPE pump function can control which
layer first becomes unstable.
The stabilizing influence of the RPE pump flux on all
interfaces other than the RPE-Bruch’s membrane junction is evident from (5), where Jp > 0 decreases the
pressure difference tending to separate layer k from layer
k − 1. In fact, ∆P − Rn Jp can become negative for sufficiently large RPE resistance Rn and pump flux Jp , giving
rise to an net outward volume flux and a hydraulic compression of all layers k 6= n. While a leaky RPE with
low resistance Rn can short-circuit the pump flux and
diminish the stabilizing effect of the pumping, the overall magnitude of the stress on layer k is maximal when
its own conductivity vanishes. Here, the entire hydraulic
stress ∆P −Rn J0 head is supported by layer k. However,
from (6), any pump flux Jp > 0 will tend to destabilize
the photoreceptor-RPE interface k = n. In detachments
where the retina first detaches from the RPE, the stress
∗
− T while ∆k < σk∗ − T for k 6= n + 1.
∆n+1 > σn+1
By specifying a functional form for Jp (∆n ), we can
self-consistently solve (6) to find an explicit solution to
∆n and determine all fluxes and pressures as functions of
known parameters. Since the RPE is highly metabolic,
its pump activity may be insensitive to the pressure difference across the cell layer. The active flux Jp (∆n )
across isolated dog RPE at different trans-RPE pressures
has been shown to be insensitive to a wide range of pressures ∆n < 0 [11]. However, other measurements show
that the in vitro pump flux across isolated RPE is significantly greater than that across the intact, in vivo RPE,
where ∆n is probably positive. Given these observations,
we propose a piece-wise linearly decreasing pump flux
Jp (∆n ):
Jp (∆n ) =
1−
0,
∆n
∆∗
n
J0 , ∆n ≤ ∆∗n
(7)
∆n > ∆∗n
where ∆∗n is the maximum pressure against which the
RPE can pump fluid, and J0 is the pump amplitude when
∆n = 0. Other simple forms such as Jp ∝ e−∆n or one
where Jp vanishes above a threshold value of ∆n can also
be used but will yield qualitatively similar results. Using
(7) in (6) we find an explicit expression for ∆n > ∆∗n ,
∆n = ∆∗n
(1 −
(1
Rn
Rn
RT )Rn J0 + RT ∆P
Rn
)Rn J0 + ∆∗n
−R
T
.
(8)
Using (8) in (7) yields an expression for Jp which can be
used to explicitly find ∆k6=n :
∆k6=n =
Rk ∆∗n (∆P − Rn J0 ) + Rn J0 ∆P
Rn
RT
)Rn J0 + ∆∗n
(1 − R
(9)
T
From (8), if ∆∗n < Rn ∆P/RT (∆n > ∆∗n ), the RPE
pump flux vanishes and ∆j = Rj ∆P/RT . Note that
for strong RPE pumps such that ∆∗n ≫ Rn ∆P/RT ,
∆n+1 < ∆n , and retinal-RPE detachments are likely to
be favored over RPE-Bruch’s membrane delaminations
∗
(“RPE detachments”) only if σn+1
< σn∗ .
The stresses ∆k are functions of the parameters
Rj , ∆P, J0 , and the threshold ∆∗n . Although tissues from
different animals, measured using different experimental
protocols display a wide range of parameter values, estimates are available. The entire retina, excluding RPE
and choroid has a hydraulic conductivity of approximately 3 × 10−10 m/(sPa) [5], with the inner and outer
plexiform layers providing nearly all of the resistance.
Another measurement of dog RPE-choroid gave a conductivity of ∼ 1.7 × 10−11m/(sPa), and an intrinsic RPE
pump flux J0 ∼ 2 × 10−8 m/s [11]. For ∆P = 5mm
Hg ≈ 650Pa, the active pump flux J0 & LT ∆P ≈
1.7 × 10−8 , indicating that at this pressure difference,
the active RPE pumping slightly over-compensates the
passive, pressure-driven inward volume flow. The combined resistance of the Bruch’s membrane-choroid tissue
in humans decreases with age from ∼ 10−8 m/(sPa) to
∼ 10−10 m/(sPa). Using these experimental observations,
we estimate that under typical conditions rn ≡ Rn /RT ∼
0.75 − 0.95, rn−1 ≡ Rn−1 /RT ∼ 0.001 − 0.2. We now explore the features of the normalized hydraulic stresses
˜ n ≡ ∆n /(∆P ) and ∆
˜ n+1 ≡ ∆n+1 /(∆P ) with these
∆
parameter estimates in mind.
˜ n and ∆
˜ n+1 /rn+1 (rj ≡ Rj /RT ), the
Figure 4 plots ∆
hydraulic stresses pulling apart the RPE-Bruch’s membrane and photoreceptor-RPE interfaces, respectively, as
˜ ∗ ≡ ∆∗ /(∆P )
functions of the dimensionless variables ∆
n
n
˜
and J0 ≡ RT J0 /(∆P ). Since an active RPE pump evacuates the photoreceptor-RPE space by pumping fluid into
the space between the RPE and Bruch’s membrane, increasing the pump rate J˜0 destabilizes the RPE-Bruch’s
˜ n ) and stabilizes the
membrane interface (increases ∆
˜ n+1 ).
photoreceptor-RPE interface (decreases ∆
Age-related decreases in the hydraulic conductivity
of the Bruch’s membrane (Ln−1 = L2 in Fig. 3) have
4
˜ n ≡ ∆n /(∆P )
FIG. 4: (a) Normalized hydraulic stress ∆
tending to separate the RPE from Bruch’s membrane, plotted as functions of the normalized pump threshold ∆∗N /(∆P )
and J˜0 ≡ RT J0 /(∆P ). (b) The normalized hydraulic stress
˜ n+1 /rk+1 separating the photoreceptor-RPE interface. The
∆
flat portions of both plots correspond to regions where
rn ∆P > ∆∗n and Jp = 0. The value rn ≡ Rn /RT = 0.8
as assumed in both plots.
been hypothesized to block resorption of fluid into the
choroid and increase the incidence of RPE detachments
in elderly patients [16]. In Fig. 5(a), we display the
˜ n as a function of the normalized, indebehavior of ∆
pendent hydraulic resistances of the RPE and Bruch’s
membrane, fn ≡ Rn /R′ and fn−1 ≡ Rn−1 /R′ (where
R′ ≡ RT −Rn −Rn−1 ), respectively. Contrary to this hypothesis, our model shows the effect of increasing fn−1 on
˜ n is more subtle. Fig. 5(a) shows, for reasonable values
∆
˜ n as a function of fn = Rn /R′ and fn−1 =
FIG. 5: (a) ∆
Rn−1 /R′ (R′ ≡ RT − Rn − Rn−1 ), the normalized RPE and
˜ n+1 /fn+1
Bruch’s membrane resistances, respectively. (b) ∆
is largely negative, indicating that the active pump flow compresses the photoreceptor layer to the RPE. Only for small
˜ n+1 > 0, allowing the photoreceptors
RPE resistance fn is ∆
to possibly spontaneously separate from the RPE. Stresses are
˜ ∗n = ∆∗n /(∆P ) = 3 and R′ J0 /(∆P ) = 1.
plotted for fixed ∆
˜ ∗n = 3 and R′ J0 /(∆P ) = 1, very little destabilizaof ∆
tion of the RPE-Bruch’s interface occurs as the Bruch’s
membrane resistance fn−1 is increased. While increasing
fn−1 hinders fluid pumped under the RPE from resorbing back into choroid, it also blocks most of the capillary
pressure Pc from being transduced past the Bruch’s membrane. Therefore, the dominant destabilizing factor is an
increase in the normalized RPE resistance fn allowing
significant pressure to build underneath the RPE.
In contrast, the photoreceptor-RPE interface is destabilized when the pressure can build up underneath the
photoreceptor layer. Therefore destabilization always occurs when the RPE becomes leakier (decreasing fn ), allowing pumped fluid to easily reenter the photoreceptorRPE space. Increasing the resistance of Bruch’s membrane fn−1 hinders fluid from reentering the choroid,
but if fn is large, the RPE provides the main resistance to pressure build-up underneath the photoreceptor cells due to passive flows. Therefore, for tight RPE
layers, an increase in fn−1 has a relatively greater effect
in destabilizing the photoreceptor layer from the RPE
than in destabilizing the RPE-Bruch’s membrane inter˜ n and ∆
˜ n+1 increase with fn−1
face. Specifically, both ∆
∗
∗
˜
˜
˜
when fn J0 > ∆n /(∆n − 1), but otherwise decreases with
decreasing Bruch’s membrane flow resistance fn−1 .
Our theoretical framework for retinal delamination is
analogous to a simple series of resistors bridging a voltage drop, but with an interior (possibly voltage gradientdependent) current source representing the RPE pumps.
Voltage gradients describe the amplitudes of local electric fields that contribute to dielectric breakdown. Although we have only considered the effects of RPE and
Bruch’s membrane conductivities on photoreceptor and
RPE delaminations, our model can be used to address
other possible physiological causes of detachment. For
example, inflammation of choroidal tissue and drugs such
as acetazolamide that reduce it [14], can be modeled by
increasing and decreasing the tissue permeabilities L0 or
L1 . Small blood vessels that invade the retina can also be
described by imposing a venous pressure within a specific
tissue layer. These simple adalptations allow our model
to address numerous clinical scenarios associated with
retinal delamination.
This work was supported by the Gerald Oppenheimer
Family Foundation, the Army Research Office through
grant 58386MA, and the NSF through grants DMS1032131 and DMS-1021818.
[1] H. Wässle and B. B. Boycott, Functional architecture of
the mammalian retina, Physiol Rev., 71, 447480, (1991).
[2] M. Yanoff and J. S. Duker, Ophthalmology,
[3] T. H. Williamson, Vitreoretinal Surgery, (SpringerVerlag, Berlin, 2008).
[4] H.-P. Hammes and M. Porta, editors, Experimental Approaches to Diabetic Retinopathy, (Karger, Basel, 2010).
[5] R. J. Antcliff, A. A. Hussain, and J. Marshall, Arch. Ophthalmol., 119, 539-544, (2001).
[6] D. J. Moore, A. A. Hussain, and J. Marshall, Invest.
Ophthalmol. & Vis. Sci., 36, 1290-1297, (1995).
[7] A. C. Bird and J. Marshall, Trans. Ophthalmol. Soc.,
105, 674682, (1986).
[8] W. J. Foster, N. Dowla, S. Y. Joshi and M. Nikolaou,
5
[9]
[10]
[11]
[12]
Graefe’s Arch. Clin. and Exptl. Ophthalmol., 248, 31,
(2009).
D. M. Maurice, J. Salmon, and H. Zauberman, 12, 212217, (1971).
H. Zauberman and E. R. Berman, Exptl. Eye Res., 8,
276-283, (1969).
S. Tsubai, Invest. Ophthalmol. & Vis. Sci., 28, 17761782, (1987).
I. Fatt and K. Shantinath, Exp. Eye Res. 12, 218-226,
(1971).
[13] A. Negi, S. Kawano and M. F. Marmor, Invest Ophthalmol Vis Sci., 28, 2099-2102, (1987); M. F. Marmor,
Graefe’s Arch. Clin. and Exp. Ophthalmol., 226, 548-552,
(1988).
[14] B. Moldow et al., Graefe’s Arch. Clin. and Exp. Ophthalmol., 236, 881-889, (1998).
[15] O. Maepea, Exp. Eye Res., 54, 731-736 (1992).
[16] C. Starita, et al., Exp. Eye Res., 62, 565-572, (1996).