FORCE-TJR
Function and Outcomes Research/Registry for
Comparative Effectiveness in TJR
Patricia D. Franklin MD, MBA, MPH
MDEpiNet/ICOR
October, 2015
Copyright 2015 FORCE-TJR. All rights reserved.
Do not copy or distribute without permission.
Team at University of Massachusetts
Medical School; FORCE-TJR
•
•
•
•
•
•
•
•
David Ayers, MD
Wenjun Li, PhD
Hua Zheng, PhD
Jeroan Allison, MD MS
Milagros Rosal, PhD
John Ware, PhD
Norm Weissman, PhD
Celeste Lemay, RN MPH
Copyright 2015 FORCE-TJR. All rights reserved.
Do not copy or distribute without permission.
Orthopedics
Biostatistics
Informatics
Health Services
Behavioral Med
Psychometrics
Health Services
Nursing
2
Exponential growth in TJR utilization
overall and in adults <65 years
Ten-Year Trend Volume THR and TKR
700,000
600,000
500,000
400,000
• TJR procedures dramatically improve
quality of life, relieve pain, improve
function.
300,000
200,000
100,000
0
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
THR
TKR
Ten-Year Trend Volume THR and TKR <65
300,000
250,000
• Projected cost increase by 2015
• 340% to $17.4 billion for THR
• 450% to $40.8 billion for TKR.
• TJR procedures are #1 procedural
cost in the Medicare budget.
200,000
• Patients under 65 years are fastest
growing group of TJR patients.
150,000
100,000
50,000
0
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
THR <65
TKR <65
Source: HCUP.net
Copyright 2015 FORCE-TJR. All rights reserved.
Do not copy or distribute without permission.
FORCE-TJR: platform for TJR
outcomes monitoring
Competitive Application: $12 million AHRQ P50 award
Department of Orthopedics and Physical Rehabilitation
University of Massachusetts Medical School (2011-14)
Supplemental grants awarded/under review.
1. Develop a comprehensive TJR registry with sustainable data
infrastructure for comprehensive TJR outcome monitoring and
feedback to providers.
– UMass is the TJR data coordinating center for the next 20+ years
2. UMass TJR research team conducting comparative effectiveness
research in TJR quality and outcomes.
– Participating on CMS expert panels and national TJR leadership groups
Copyright 2015 FORCE-TJR. All rights reserved.
Do not copy or distribute without permission.
Today’s goals
1. FORCE-TJR is both a comprehensive TJR
outcomes Registry and conducts Comparative
Effectiveness Research
2. FORCE-TJR and appropriate TJR timing and use.
3. FORCE-TJR and value/safety to patients,
clinicians, hospitals and policy makers.
4. Collaborations with ICOR/MDEpiNet in postmarketing implant surveillance.
Copyright 2015 FORCE-TJR. All rights reserved.
Do not copy or distribute without permission.
FORCE-TJR
Paradigm Shift: PROs are primary outcome
JAMA 2012; 308(12): 1217-18
Copyright 2015 FORCE-TJR. All rights reserved.
Do not copy or distribute without permission.
JBJS 2014; 96:1567-9
FORCE-TJR: National Benchmarks
from >200 representative Surgeons
in 28 States
•
•
•
•
•
•
•
75% of surgeons are community
-based
Fellowship-trained, general
orthopedic surgeons
High and low volume
surgeons/hospitals; urban and
rural hospitals
Teaching hospitals, non-teaching
hospitals
Patients with private, public and
HMO insurance
All major implant manufacturers
Primary TJR, revision TJR, Uni, PF,
HR, all types of procedures
Copyright 2015 FORCE-TJR. All rights reserved.
Do not copy or distribute without permission.
Map of Participating Core Centers and Community Sites
ND
MT
WA
WI
MI
WY
IA
NE
NV
VT
MI
SD
ID
OR
MN
UT
CO
IN
IL
KS
MO
AZ
PA
OH
VA
NC
AR
MS
TX
NJ
WV
TN
OK
NM
AL
ME
NY
KY
CA
NH
DC
MA
CT RI
DE
MD
SC
GA
LA
FL
Core Clinical Centers
UMass Medical School, Worcester, MA
Connecticut Joint Replacement Institute, Hartford, CT
The University of Rochester Medical Center, Rochester, NY
Medical University of South Carolina, Charleston SC
Baylor College of Medicine, Houston, TX
Community Sites
Community Sites currently enrolled
Effective procedures
for PRO collection
FORCE-TJR proven methods
•
•
•
•
•
96% pre-TJR
85% completion post-TJR*
Web-based surveys with real-time scores
Completed in Office or at Home
PC or Tablet
*other US registry PRO follow-up rates from 20-30%. Franklin et al, JBJS, 2014.
Copyright 2015 FORCE-TJR. All rights reserved.
Do not copy or distribute without permission.
FORCE-TJR Data collected across TJR Care Cycle
>25,000 patients
Patient
Surgeon
Before
Surgery
Hospital
Surgery
• PRO
Global health
(VR12; PROMIS)
HOOS/KOOS
• CLINICAL RISKS
Medical &
MSK risks
Demographic
• CLINICAL
Implant
Operative
Notes
Direct to Patient (validate EHR)
30 -90 days
6 months
Annual
• PRO
Pain
• PRO
• PRO
Global health
Global health
(VR12; PROMIS)
(VR12; PROMIS)
HOOS/KOOS
HOOS/KOOS
• CLINICAL
Complication
(if any)
• CLINICAL
Complication
(if any)
• CLINICAL
Complication
(if any)
Revision
CMS DATA ANNUALLY
Copyright 2015 FORCE-TJR. All rights reserved.
Do not copy or distribute without permission.
FORCE-TJR Registry with quality
improvement feedback to surgeons
Public DATA USES
Hospital DATA USES
1. Comparative reports to anticipate
1. Quality monitoring
public reporting
2. PROs for incentives, insurer/ACO
models
3. FORCE-TJR is a Qualified Clinical Data
Registry (PQRS); Submit FORCE data.
4. US News acknowledging FORCE-TJR
hospitals (and surgeons)
Copyright 2015 FORCE-TJR. All rights reserved.
Do not copy or distribute without permission.
– Patient risk factors
– Pre-op pain/function
– 30 day readmissions
– 90 day complications
– Revisions
– Post-op pain/function
Risk-adjusted Post-TJR Outcomes
Site Outcome Summary (SF/PCS)
• Site pre-op mean PCS is
comparable to national norm.
•
•
•
Site post6m mean PCS = 44
Post6m risk-adjusted PCS= 43
National post 6m PCS= 45
Risk adjustment is critical if
scores are used for public
reporting or reimbursement.
Copyright 2015 FORCE-TJR. All rights reserved.
Do not copy or distribute without permission.
Site level variation: MSK, SES, BMI Key
Copyright 2015 FORCE-TJR. All rights reserved.
Do not copy or distribute without permission.
29
FORCE-TJR: RESEARCH AND POLICY
1. PROs: TJR Appropriateness and Value
Validated assessment of pain and function before and
after TJR to improve health, reduce cost, and increase
value.
1. Timing/Need: Reduce untimely and/or
inappropriate procedures by identifying patients
unlikely to benefit from TJR.
2. Episode Costs: Reduce post-operative
complications and readmissions by identifying
high risk patients before surgery who can be
managed to reduce risk.
Copyright 2015 FORCE-TJR. All rights reserved.
Do not copy or distribute without permission.
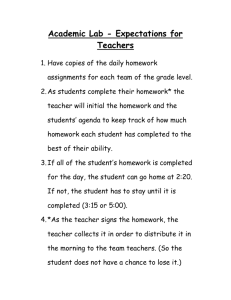
FORCE-TJR Site Report: Pre-TKR Function
Site Pre-TKR Patient Profile:
•
National Norm for Healthy = 50
(SD=10) Green arrow
•
•
Site Median PCS = 32
National Median PCS for TJR = 32
(2SD below healthy; Red arrow)
•
•
Site 75th%ile PCS = 38
National 75th%ile PCS = 39
Patient selection matches national norms;
>83% have PCS scores reflecting disability.
Patients in yellow (1SD): evaluate clinical
circumstances warranting TJR.
Copyright 2015 FORCE-TJR. All rights reserved.
Do not copy or distribute without permission.
Pre-op
2. Predicting post-TJR readmission
morbidity and costs (CMS/AAHKS)
• Post-TJR hospital complication and readmission rates
first posted on Hospitalcompare.gov in 2013-14.
• FORCE-TJR documented that 1 in 4 (25%) of patients who
are readmitted do not go to hospital where TJR was
performed.
• Patients report post-TJR events (ER visit, return to OR,
readmission to any hospital); accuracy validated.
• Post-TJR readmissions
– Prevalence: 2 - 8%; mean 5.4%
– $17,000 per readmisison
Copyright 2015 FORCE-TJR. All rights reserved.
Do not copy or distribute without permission.
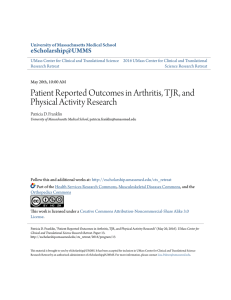
0.50
0.25
0.00
Sensitivity
Readmission- overall 4.7% of patients
Key new predictors of readmission:
• Pre-TJR function (PRO)
• BMI
• Medical and Musculoskeletal
Co-morbidities
C= 0.79 (TKR); C= 0.86 (THR)
0.75
1.00
Combined CMS + FORCE data
30 day post-TJR risk-adjustment
0.00
0.25
0.50
1 - Specificity
0.75
Area under ROC curve = 0.7881
CMS readmission risk models based only on ICD/CC codes are
less discriminating (CMS C= .64)
Copyright 2015 FORCE-TJR. All rights reserved.
Do not copy or distribute without permission.
1.00
3. PROs in post-market implant surveillance (FDA)
• New Zealand registry reported that patients
with significant pain at 6 months post-TJR
were 7 times more likely to have revision in 5
years.
• Metal on metal implant failure- pain was first
symptom
• FORCE will identify sub-group at risk
• Monitor for revision rates
Copyright 2015 FORCE-TJR. All rights reserved.
Do not copy or distribute without permission.
12 month post-TKR Pain and Function:
Patients <65 years with Implant X
28% of patients have 12 month pain score <75
Copyright 2015 FORCE-TJR. All rights reserved.
Do not copy or distribute without permission.
Goals/FDA ICOR (new UO1)
• Aim Enhance device surveillance using PRO and validate
claims based surveillance.
FORCE-TJR will define comprehensive post-marketing TJR
implant surveillance program to go beyond safety and include
implant effectiveness metrics.
(a) Patients report post-TJR adverse events, including
implant revision and complications, via web or a smartphone
App and validated by CMS or insurer claims data.
(b) Evaluate if pain and functional limitation at 6 months
vary by implant materials (e.g., ceramic vs. metal hip) or
design (e.g., mobile vs. static knee).
(c) Severity of post-TJR pain at 6 months post-TJR will
predict risk of revision at 2 and 5 years after adjusting for BMI
and medical and musculoskeletal comorbidities.
Copyright 2015 FORCE-TJR. All rights reserved.
Do not copy or distribute without permission.
FORCE-TJR
MISSION
Independent, unbiased, expert data collection and reporting to guide best
TJR surgical practices to assure patients achieve optimal pain relief and
functional gain with minimal adverse events and implant failures.
• 4 Years of experience with Pre and Post-TJR PROs on >25,000 patients
• Post-op adverse event surveillance
• Implant library and revision surveillance
• CONTINUING TO ADD NEW HOSPITALS AND SURGEONS
Copyright 2015 FORCE-TJR. All rights reserved.
Do not copy or distribute without permission.
Contact Us
Patricia.franklin@umassmed.edu
1-508-856-5748
1-855-99FORCE
www.force-tjr.org
Copyright 2015 FORCE-TJR. All rights reserved.
Do not copy or distribute without permission.