American Journal of Emergency Medicine (2011) 29, 582–589.e2
www.elsevier.com/locate/ajem
Original Contribution
The role of plain radiographs in patients with acute
abdominal pain at the ED☆,☆☆
Adrienne van Randen MD a,b , Wytze Laméris a,b , Jan S.K. Luitse MD c ,
Michiel Gorzeman MD d , Erik J. Hesselink MD e , Dennis E.J.G.J. Dolmans MD, PhD f ,
Jan Peringa MD g , Anna A.W. van Geloven MD, PhD h , Patrick M. Bossuyt PhD i ,
Jaap Stoker MD, PhD b , Marja A. Boermeester MD, PhD a,⁎
on behalf of the OPTIMA study group 1
a
Department of Surgery, Academic Medical Center, Amsterdam, 1105 AZ, The Netherlands
Department of Radiology, Academic Medical Center, Amsterdam, 1105 AZ, The Netherlands
c
Department of Emergency Medicine, Academic Medical Center, Amsterdam, 1105 AZ, The Netherlands
d
Department of Emergency Medicine, St Antonius Hospital, Nieuwegein, 3034 EM, The Netherlands
e
Department of Surgery, Gelre Hospitals, Apeldoorn, 7334 DZ, The Netherlands
f
Department of Surgery, University Medical Center, Utrecht, 3584 CX, The Netherlands
g
Department of Radiology, Onze Lieve Vrouwe Gasthuis, Amsterdam, 1091 AC, The Netherlands
h
Department of Surgery, Tergooi Hospitals, Hilversum, 1213 XZ, The Netherlands
i
Department of Clinical Epidemiology, Biostatistics, and Bioinformatics, Academic Medical Center,
Amsterdam, 1105 AZ, The Netherlands
b
Received 30 September 2009; revised 15 December 2009; accepted 16 December 2009
Keywords:
Plain radiography;
Acute abdomen;
Bowel obstruction
Abstract
Objective: The purpose of this study was to evaluate the added value of plain radiographs on top of
clinical assessment in unselected patients presenting with acute abdominal pain at the emergency
department (ED).
Methods: In a multicenter prospective trial, patients with abdominal pain more than 2 hours and less
than 5 days presented at the ED were evaluated clinically, and a diagnosis was made by the treating
physician. Subsequently, all patients underwent supine abdominal and upright chest radiographs, after
which the diagnosis was reassessed by the treating physician. A final (reference) diagnosis was assigned
by an expert panel. The number of changes in the primary diagnosis, as well as the accuracy of these
changes, was calculated. Changes in the level of confidence were evaluated for unchanged diagnoses.
Results: Between March 2005 and November 2006, 1021 patients, 55% female, mean age 47 years
(range, 19-94 years), were included. In 117 of 1021 patients, the diagnosis changed after plain
radiographs, and this change was correct in 39 patients (22% of changed diagnoses and 4% of total
study population). Overall, the clinical diagnosis was correct in 502 (49%) patients. The diagnosis after
☆
Manuscript presented at: RSNA in Chicago on December 2, 2008.
Funding: The Dutch Organization for Health Research and Development, Health Care Efficiency Research programme (ZonMw, grant number 945-04-308).
⁎ Corresponding author. Tel.: +31 20 5662666; fax: +31 20 5669243.
E-mail address: m.a.boermeester@amc.uva.nl (M.A. Boermeester).
1
Study group member are listed in the Appendix A.
☆☆
0735-6757/$ – see front matter © 2011 Elsevier Inc. All rights reserved.
doi:10.1016/j.ajem.2009.12.020
The role of plain radiographs in patients with acute abdominal pain at the ED
583
evaluation of the radiographs was correct in 514 (50%) patients, a nonsignificant difference (P = .14). In
65% of patients with unchanged diagnosis before and after plain radiography, the level of confidence of
that diagnosis did not change either.
Conclusion: The added value of plain radiographs is too limited to advocate their routine use in the
diagnostic workup of patients with acute abdominal pain, because few diagnoses change and the level of
confidence were mostly not affected.
© 2011 Elsevier Inc. All rights reserved.
1. Introduction
Acute abdominal pain is a common patient presentation in
the emergency department (ED). In the United States, 119.2
million people visited the ED in 2006, of which 8.1 million
people (6.8%) sought help for abdominal pain [1]. The imaging
workup of patients with acute abdominal pain generally starts
with acute abdominal series (supine and upright abdominal
radiographs and upright chest radiograph) [2-4]. Data on the
utilization of plain radiography in this patient population are
not exactly known in general US databases (Healthcare Cost &
Utilization Project, Medicare, and Medicaid). A number of
studies reported the use of plain radiography in patients with
acute abdominal pain. In 1 study, 45% of the patients suspected
with appendicitis received a plain radiograph in their
diagnostic workup [5], In another study, as much as 78% of
patients received 1 or more abdominal radiographs [6].
The American College of Radiology provide guidelines
for referring physicians to help them making efficient use of
radiology. The guidelines are developed by expert panels in
diagnostic imaging, and appropriateness criteria are presented per clinical condition, thereby enabling the treating
physician to request the most appropriate imaging modality
for that specific clinical condition. For patients with acute
abdominal pain and fever at the ED, the American College of
Radiology considers abdominal radiographs equally appropriate as unenhanced computed tomography (CT) scan and
ultrasound. Only a CT scan with intravenous contrast is
considered more appropriate [7].
Despite these recommendations, there is little evidence to
support the widespread usage of plain radiography in the
diagnostic workup in patients with acute abdominal pain [8].
There is even some evidence in the literature that the
diagnostic value and clinical utility of plain radiography in
patients with acute abdominal pain are limited [9-15]. Only
in patients suspected with urinary tract calculi [16,17],
perforation [10,16,18], bowel obstruction [10,17,19], and
radio-opaque gastrointestinal foreign bodies [20] plain
radiographs are presumably diagnostic. The approximate
cost price of a plain abdominal radiograph is $53.90. If we
assume that of all people presenting to the ED with
abdominal pain, only half of them receive an abdominal
radiograph, the annual costs will approximately be 218.3
million dollar annually in the United States.
The purpose of this study was to evaluate the proportion
of changes in primary diagnosis between clinical assessment
before and clinical assessment after plain radiography in
unselected patients presenting to the ED with acute
abdominal pain. We also wanted to evaluate the accuracy
of these diagnoses before and after plain radiography, as well
as changes in the level of confidence in the unchanged
diagnoses and for diagnoses in which plain radiography is
presumed diagnostic.
2. Materials and methods
2.1. Design and eligibility
In a large multicenter trial [9,21], patients presenting at
the ED with acute abdominal pain, for more than 2 hours and
less than 5 days, were prospectively invited. The study was
conducted in 2 university and 4 large teaching hospitals.
Excluded were patients discharged by the treating physician
at the ED without any diagnostic imaging (no plain
radiography, ultrasonography, CT, or other imaging techniques), patients younger than 18 years, pregnant women,
patients with a blunt or penetrating trauma, and patients in
hemorrhagic shock. This study had been approved by the
institutional review boards of the participating hospitals.
Eligible patients were asked for written informed consent.
All consenting patients were evaluated by one of the treating
physicians at the ED, who were surgical or emergency
medicine residents. After history, physical, and laboratory
examination, the physician recorded the most likely
diagnosis. Diagnoses were selected from a list of potential
diagnoses (Appendix B), provided in the online case record
form. Furthermore, a level of confidence of the diagnosis was
asked before and after radiographs, on a scale from 0 to 10
(low to high confidence).
2.2. Image evaluation
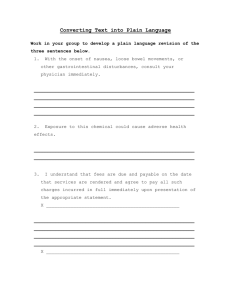
All included patients underwent plain supine abdominal
and upright chest radiography shortly after presentation at
the ED (Fig. 1). Plain radiographs were evaluated by the
treating physicians at the ED in the acute setting. After image
evaluation, a new diagnosis and level of confidence were
provided by the physician, selected from the same list of
diagnoses as used before (Appendix B).
584
A. van Randen et al.
selected a final diagnosis from the same list of diagnoses as
provided to the treating physicians. If panel members
disagreed on the final diagnosis after individual evaluation,
consensus was reached in a group discussion
Expert panel evaluation of all cases and consensus
meetings took place between June 2007 and December
2007. The expert panel reached consensus after individual
evaluation in 76% of the patients; 244 (24%) patients were
discussed during consensus meetings.
2.4. Analysis
Fig. 1
Flow chart of the study.
The following image characteristics were assessed on plain
upright posterior-anterior chest radiograph: image quality in
general, if previous radiographs were available for comparison,
visualization of free intraperitoneal gas, mediastinal abnormalities, enlarged heart, pulmonary edema, apical vascular
redistribution, pneumothorax, consolidation, pleural fluid,
skeletal abnormalities, and/or soft tissue abnormalities.
On plain supine abdominal radiograph, the following
image characteristics were assessed: dilated small bowel
loops (N25 mm), dilated colon (N55 mm), a dilated cecum
(N100 mm), calcifications, fluid (collections), retroperitoneal
gas, and other abnormalities (skeletal or soft tissue
abnormalities). Dilated cecum and dilated colon were
measured independently because the upper limit of normal
differs between cecum and the other parts of the colon.
2.3. Reference standard
Included patients also underwent ultrasonography and CT
after radiography (Fig. 1). After 6 months of follow-up, a
final diagnosis was assigned by an independent expert panel
(see Appendix C for panel members), who had not been
involved in the workup of included patients.
Panel members first evaluated all available data for each
patient for at least 6 months postinclusion and individually
Our focus in the analysis was on the value of plain
radiographs after clinical assessment. We recorded the
proportion of changes in primary diagnosis between clinical
assessment only and assessment after plain radiographs. We
also evaluated the accuracy of all changes, by comparing them
with the final diagnosis. If diagnoses did not change, the
corresponding change in the level of confidence was evaluated.
Diagnoses in which plain radiographs are presumed to
have diagnostic value were evaluated in more detail. These
diagnoses are bowel obstruction, perforated viscus, and
urinary tract stones [10,16,17,20,22]. The sensitivity and
positive predictive value were calculated for these specific
diagnoses. Changes in the overall accuracy of the diagnosis
were evaluated for statistical significance with the McNemar
test statistic, as were changes in the sensitivity for the 3
specific diagnoses. Differences in the positive predictive
value were evaluated with the χ2 test statistic. Analyses were
performed in SPSS 15.0.1 statistics (SPSS Inc, Chicago, Ill)
and CIA (Statistics With Confidence, London, UK).
3. Results
Between March 2005 and November 2006, 1101 patients
were included. Data of 80 (7%) patients were incomplete and
could not be used in the analysis. No patients were lost to
follow-up. The mean age of the 1021 patients available for
the analysis was 47 years (range, 19-94 years), and the male
to female ratio was 456 to 565 (44%:56%). Patients had been
evaluated at the ED by surgical residents (74%) and
emergency medicine residents (26%) with a mean experience
of 25 months.
Table 1 lists the clinical diagnoses, the diagnoses after
plain radiography, and the final diagnoses. The most frequent
final diagnoses were acute appendicitis, nonspecific abdominal pain (NSAP), and acute diverticulitis.
Thirteen of the 1021 radiographs were judged to be of
poor quality. Three patients had a left lateral decubitus
radiography. One patient had a sitting, and no erect, chest
radiograph. Three patients had a substantially rotated chest
radiograph. Three patients had poor inspiration chest radiographs and in another 3 patients overlying structures
impaired evaluation of the chest radiograph. None of these
The role of plain radiographs in patients with acute abdominal pain at the ED
Table 1 Diagnosis assigned after clinical evaluation, after
evaluation of plain radiography, and by the expert panel after 6
months
Diagnosis
Appendicitis
Diverticulitis
Gastrointestinal
nonurgent
Bowel obstruction
Hepatic, pancreatic
and biliary
disorders (HPB) a
Cholecystitis
Pancreatitis
Nonspecific
abdominal pain
Gynecologic disorder
urgent
Urinary tract disorder
urgent
Urinary tract stones b
Perforated viscus
Abscess
Gynecologic disorder
nonurgent
Peritonitis c
Inflammatory bowel
disorder
Hernia d
Bleeding
Bowel ischemia
Other e
Pneumonia
Malignancy
Clinical
evaluation
After plain Final
radiography
n
n
%
%
n
%
422
126
80
41.3
12.3
7.8
402
118
87
39.4
11.6
8.5
284
118
56
27.8
11.6
5.5
72
65
7.1
6.4
82
64
8.0
6.3
68
43
6.7
4.2
62
28
27
6.1
2.7
2.6
57
27
30
5.6
2.6
2.9
52
28
183
5.1
2.7
17.9
24
2.4
28
2.7
27
2.6
21
2.1
21
2.1
17
1.7
21
18
18
11
2.1
1.8
1.8
1.1
26
15
18
11
2.5
1.5
1.8
1.1
25
13
14
9
2.4
1.3
1.4
0.9
6
5
0.6
0.5
9
6
0.9
0.6
3
30
0.3
2.9
4
0.4
4
0.4
2
0.2
4
0.4
4
0.4
9
0.9
3
0.3
7
0.7
12
1.2
2
0.2
3
0.3
12
1.2
1
0.1
1
0.1
11
1.1
1
0.1
1
0.1
5
0.5
1021 100 1021 100 1021 100
a
In the final diagnosis, HPB consisted of cholecystolithiasis (33),
choledocholithiasis (5), hepatitis (3), chronic pancreatitis (1), and liver
metastasis (1).
b
In the final diagnoses, urinary tract stones were with obstruction
(18) and without obstruction (7).
c
In the final diagnosis, peritonitis was not caused by perforation or
bowel ischemia.
d
In the final diagnosis, hernia without strangulation; otherwise, it
would have been classified as bowel ischemia.
e
In the final diagnosis, other diagnoses consisted of abdominal wall
infiltration, esophagitis (2), renal infarction (2), gastric band problem
(2), Systemic lupus erythematosus, mesenteric lymphadenitis,
postprocedural pain, uterine hemorrhage, and a testical torsion.
patients were clinically suspected with perforated viscus, nor
was this their final diagnosis.
3.1. Changes in primary diagnosis
The primary clinical diagnosis corresponded with the
final diagnosis in 502 patients (49%). After evaluation of the
radiographs, the primary diagnosis corresponded with the
585
final diagnosis in 514 patients (50%). This improvement in
accuracy was not significant (P = .14). The treating
physicians changed the primary diagnosis from the initial
clinical diagnosis in 117 (11%) of 1021 cases, of which 39
changes were accurate, which stands for 22% of patients with
changed diagnoses and 4% of all patients. This accuracy of
the clinical diagnosis and the diagnosis after plain radiography did not differ among participating hospitals and among
residents with different level of experience (Appendix D). In
571 (65%) of 875 patients with an unchanged diagnosis
before and after plain radiography, the level of confidence of
that diagnosis did not change (Table 2).
3.2. Bowel obstruction, perforated viscus, and
urinary tract stones
The changes in primary diagnosis between clinical
evaluation before and after plain radiography for the 3
specific diagnoses are shown in Table 3. Seven patients
were newly diagnosed with bowel obstruction after
viewing the radiographs; 17 patients were no longer
diagnosed with bowel obstruction. Sixteen (66%) of these
24 changes were accurate.
The changes in diagnoses were correct in 6 (55%) of the 11
patients suspected with urinary tract stones and in 5 (71%) of
the 7 patients suspected with perforated viscus. There were no
significant changes in the number of patients primarily
suspected with bowel obstruction, urinary tract stone, and
perforated viscus before and after reviewing radiographs.
The level of confidence did not change in most patients
suspected with bowel obstruction and urinary tract stones
before and after plain radiography (Table 2). In 6 (46%) of 13
patients with the clinical diagnosis of perforated viscus, the
level of confidence increased after plain radiographs.
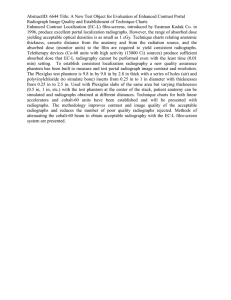
3.3. Sensitivity and positive predictive value
The sensitivity and positive predictive values were
calculated for bowel obstruction, urinary tract stones, and
perforated viscus, both after clinical assessment and after
plain radiography (Fig. 2). After radiography, the sensitivity
of bowel obstruction was significantly higher than after
clinical evaluation only: 74% versus 57%, respectively (P b
.01). For urinary tract stones and perforated viscus, there
was no significant difference in sensitivity before and after
evaluation of radiographs. The sensitivity of plain radiographs in detecting perforated viscus was low (15%) in this
patient population. Of the patients with a final diagnosis of
perforation (n = 13), 4 patients had a contained perforation
(3 perforated diverticulitis and 1 contained perforated
foreign body). The radiographs of these patients were
evaluated retrospectively with an abdominal radiology
expert; free air could not be detected.
The positive predictive value did not differ significantly
between clinical assessment only and after plain radiographs
586
A. van Randen et al.
Table 2
The level of confidence in patients with an unchanged diagnosis after evaluation of the plain radiographs
Diagnoses
a
Overall
Bowel obstruction
Urinary tract stones
Perforated viscus
Unchanged
diagnosis, n b
Level of confidence
increased, n (%)
Level of confidence
decreased, n (%)
Level of confidence
unchanged, n (%)
875
61
17
13
182
23
2
6
122
6
4
2
571
32
11
5
(21)
(38)
(12)
(46)
(14)
(10)
(24)
(15)
(65)
(52)
(65)
(38)
a
Because the level of confidence was not recorded in all patients, only 983 patients (of which 875 had an unchanged diagnosis) were included in
this analysis.
b
The number of diagnoses that did not change after evaluation of plain radiographs.
for all 3 diagnoses. Most false-positive diagnoses of bowel
obstruction were finally diagnosed with bowel ischemia (n =
3), diverticulitis (n = 6), or NSAP (n = 7). Most patients
falsely suspected of urinary tract stones after clinical and
plain radiography evaluation were finally diagnosed as
NSAP (n = 8). The final diagnoses of patients falsely
suspected of perforated viscus were diverticulitis (n = 3),
appendicitis (n = 2), or NSAP (n = 2).
4. Discussion
This study shows that plain radiography in patients with
acute abdominal pain has limited additional value. The clinical
diagnosis after evaluation of plain radiographs did not change
significantly from the primary diagnosis based on clinical
evaluation alone. The level of confidence remained the same in
most patients in whom the primary diagnosis did not change.
Only the sensitivity in detecting bowel obstruction was
significantly higher after evaluation of the plain radiographs.
For other diagnoses, such as perforated viscus and urinary tract
stones, plain radiographs have no added diagnostic value.
Some potential limitations of this study have to be
acknowledged. The added value of plain radiography in
patients clinically suspected for a gastrointestinal foreign
body was not evaluated separately, because the study cohort
Table 3
included only 1 patient with a foreign body. Plain
radiography may be able to show a gastrointestinal radioopaque foreign body adequately, and sensitivity of 80% to
90% is reported [20,23]. However, in this cohort, there was 1
patient with a gastrointestinal foreign body, and this foreign
body was not radio-opaque. It was therefore missed at the
abdominal film. Furthermore, we did not perform an upright
abdominal radiography in addition to the supine abdominal
and upright chest radiographs. For detecting bowel obstruction, multiple air-fluid levels of different heights within 1
bowel segment and an air fluid level width of more than 2.5
cm are the most significant features at upright abdominal
radiography [24,25]. We were unable to evaluate these
specific features of bowel obstruction with the supine
abdominal radiograph, but we did evaluate features as
dilated small bowel loops, dilated colon, dilated cecum,
calcifications, fluid collections, and intraperitoneal and
retroperitoneal gas. The evaluation of the location of the
obstruction may be easier to detect on a supine film because
bowel loops are more or less at their anatomical position. It is
also stated in the literature that a small bowel obstruction
(SBO) can be diagnosed equally adequate on a supine
abdominal radiograph [26]. A lateral chest radiograph has
been suggested by some, to achieve a higher diagnostic
accuracy in detecting free intraperitoneal air than with a
posterior-anterior chest radiograph [27]. For patients with
Changes in diagnosis after reviewing plain radiographs
Diagnoses in which
plain radiographs are
possibly diagnostic
Final diagnosis a
(n)
PPV clinical
evaluation b
PPV after
radiographs b
Difference
primary
diagnosis c
Newly
diagnosed
No longer
diagnosed
Correctly
changed d
Bowel obstruction e
Urinary tract stone
Perforated viscus
68
25
13
54% (39/72)
57% (12/21)
11% (2/18)
61% (50/82)
58% (15/26)
13% (2/15)
0.06
0.23
0.45
17
8
2
7
3
5
66% (16/24)
55% (6/11)
71% (5/7)
PPV indicates positive predictive value.
a
Final diagnosis as assigned by the expert panel (reference standard).
b
Positive predictive value of the diagnosis after clinical examination (clinical history and physical and laboratory examination).
c
Change in primary diagnoses (McNemar).
d
Correct, as compared with reference diagnosis, change (newly diagnosed or no longer diagnosed) with a specific diagnosis.
e
Fifty-eight patients had a final diagnosis of SBO, 41 of which were correctly diagnosed with bowel obstruction after plain radiographs; 10 patients had
a final diagnosis of LBO, and 9 of which were correctly diagnosed with bowel obstruction after plain radiographs.
The role of plain radiographs in patients with acute abdominal pain at the ED
Fig. 2 Comparison of positive predictive value (PPV) and
sensitivity between clinical diagnosis and clinical including
radiography diagnosis of bowel obstruction, urinary tract stones
and perforated viscus in relation to final reference diagnoses. A, a.
Bowel obstruction: percentage sensitivity significantly (*Pb.01)
higher after clinical assessment plus plain radiographs, whereas
PPV was not significantly different (P=.39). B, Urinary tract stones:
sensitivity and PPV did not differ significantly between clinical
assessment and clinical assessment including plain radiographs
(P=.97 and P=.38 respectively). C, Perforated viscus: sensitivity
and PPV did not differ significantly between clinical assessment
and clinical assessment including plain radiographs (both P=1.00).
bowel obstruction, especially for evaluation of the location
and common causes of the obstruction, such as adhesions,
herniation, or neoplasms, differentiation between these
causes of bowel obstruction on abdominal radiography is
difficult [28]
Most patients and most radiographs were evaluated by
surgical and emergency medicine residents. They are
known to be less accurate in their evaluation of abdominal
radiographs than surgeons and radiologists [11,13]. If plain
radiographs had been prospectively evaluated by a
radiologist, their accuracy could have been higher. In
many ED settings, radiographs are usually evaluated by
the treating physician, and afterward, a report is made by
the radiologist.
In this study, SBO and large bowel obstruction (LBO)
were not separately indicated when a diagnosis of bowel
obstruction was made. The treating physicians were not
asked to distinguish patients with SBO from LBO. Plain
radiographs are presumed to be more diagnostic for SBO
than for LBO. Because 9 of 10 patients with LBO on plain
radiography had been correctly diagnosed with bowel
obstruction after clinical evaluation plus plain radiography,
587
we assume that the analysis was not negatively influenced by
the fact that SBO and LBO were lumped together.
We evaluated unselected patients with acute abdominal
pain, because plain radiographs are requested in all types
of patients with acute abdominal pain, not just for patients
suspected with a specific disease. All patients were
evaluated in 2 university hospitals and 4 teaching
hospitals. These hospitals are a mixture of university and
teaching hospitals and represent both urban and rural
hospitals. However, our study results do not apply to all
patients with acute abdominal pain. Only patients who
required some kind of diagnostic imaging for their workup
at the ED were invited, and patients' discharged from the
ED without imaging were not included. Furthermore, most
patients were referred to the ED by general practitioners.
Both selection criteria resulted in a population with a
relative high percentage of more serious diagnoses, which
should be kept in mind when applying the results to other
settings.
The focus of our data analysis was on the added value
of radiography on top of clinical assessment, not on the
accuracy of radiography as a separate entity. We reported
changes in the primary diagnosis between clinical
assessment only and clinical assessment after radiographs.
We feel that this presentation of data is more informative
for clinical practice than just reporting predictive values
after clinical assessment and after clinical assessment
including radiographs. Positive predictive values show the
proportion of correctly diagnosed positive patients, whereas for clinicians, it is probably more relevant to show how
changes are built up for each diagnosis and whether these
changes are correct.
Comparable literature on the accuracy of plain radiographs in acute abdomen is scarce. In 2 recent studies, the
accuracy of plain radiography was reported in terms of
sensitivity and specificity and comparable to our results. In
one of these studies, a prospective evaluation of acute
abdominal series (upright chest radiograph and upright and
supine abdominal radiographs) was performed. The
sensitivity and specificity of plain radiographs were
estimated at 30% and 88%, respectively [2]. In a
retrospective evaluation of plain radiographs in patients
with acute abdominal pain, the sensitivity was 43% at a
specificity of 74% [29]. In comparison with the results of
these studies, the reported accuracy for specific diagnoses
in our analysis was relatively good for bowel obstruction
(sensitivity of 74%) and urinary tract stones (sensitivity
60%). Accuracy of bowel obstruction and urinary tract
stone are comparable to the sensitivity reported in literature
of studies evaluating patients suspected these specific
diagnoses [18,30,31]. The sensitivity and positive predictive value reported with this prospective study are
comparable to or even higher than the accuracy values
reported in recent literature [19] for (upright) abdominal xray. Therefore, it is reasonable to assume that addition of
an upright abdominal radiograph would not have increased
588
the accuracy in such manner that the conclusion would
have been changed. For this reason, the results of the
present study are likely well generalizable even to clinics
in which an upright abdominal radiograph is performed
instead or in combination with a supine abdominal. It is
well known that free intraperitoneal air, and thereby,
perforated viscus can sometimes be missed at plain
radiography. Up to 25% of the free intraperitoneal air
might be not visible at imaging [17]. In our study, both the
proportion of false-positive diagnoses of perforated viscus
and the number of false negatives were high. This could
have been caused by the study design, because the treating
physician who evaluated the radiographs had also
performed the clinical evaluation. When a perforated
viscus was suspected after clinical evaluation but free
intraperitoneal air was not detected at plain radiographs,
the suspicion of a perforated viscus was not always
dismissed. A more accurate diagnosis can be made with
CT in these patients [32]. Moreover, attention must be paid
to the low sensitivity of the clinical diagnosis. Therefore, if
there is any (even a very low) suspicion of perforation,
additional diagnostic workup is warranted and most likely
CT should be performed.
A. van Randen et al.
[6]
[7]
[8]
[9]
[10]
[11]
[12]
[13]
[14]
[15]
5. Conclusions
[16]
Plain abdominal and chest radiographs in patients with
acute abdominal pain were shown to have limited added
diagnostic value. Their added value is too limited to
advocate their routine use in the diagnostic workup of
patients with acute abdominal pain at the emergency
department, because few diagnoses changed and the level
of confidence of the diagnosis was usually not affected.
Therefore, we suggest that plain radiography should be
omitted from the routine diagnostic workup of patients with
acute abdominal pain presenting to the ED, which may
provide substantial cost savings.
[17]
[18]
[19]
[20]
[21]
References
[1] National Hospital Ambulatory Medical Care Survey. 2005 emergency department summary; 2008 [Url: www.cdc.gov/nchs/data/
nhsr/nhsr007.pdf] accessed: 01-14-2010.
[2] MacKersie AB, Lane MJ, Gerhardt RT, et al. Nontraumatic acute
abdominal pain: unenhanced helical CT compared with three-view
acute abdominal series. Radiology 2005;237:114-22.
[3] Mirvis SE, Young JW, Keramati B, McCrea ES, Tarr R. Plain film
evaluation of patients with abdominal pain: are three radiographs
necessary? AJR Am J Roentgenol 1986;147:501-3.
[4] Sala E, Watson CJ, Beadsmoore C, et al. A randomized, controlled
trial of routine early abdominal computed tomography in patients
presenting with non-specific acute abdominal pain. Clin Radiol 2007;
62:961-9.
[5] Otero HJ, Ondategui-Parra S, Erturk SM, Ochoa RE, GonzalezBeicos A, Ros PR. Imaging utilization in the management of
[22]
[23]
[24]
[25]
[26]
appendicitis and its impact on hospital charges. Emerg Radiol 2008;
15:23-8.
Rao PM, Rhea JT, Rao JA, Conn AK. Plain abdominal radiography in
clinically suspected appendicitis: diagnostic yield, resource use, and
comparison with CT. Am J Emerg Med 1999;17:325-8.
Shuman WP, Ralls PW, Balfe DM, et al. Imaging evaluation of
patients with acute abdominal pain and fever. American College of
Radiology. ACR Appropriateness Criteria. Radiology 2000;215
(Suppl):209-12.
Smith JE, Hall EJ. The use of plain abdominal x rays in the emergency
department. Emerg Med J 2009 Mar;26(3):160-3.
Laméris W, van Randen A, van Es HW, et al. Imaging strategies for
detection of urgent conditions in patients with acute abdominal pain:
diagnostic accuracy study. BMJ 2009 Jun 26;338:b2431.
Anyanwu AC, Moalypour SM. Are abdominal radiographs still
overutilized in the assessment of acute abdominal pain? A district
general hospital audit. J R Coll Surg Edinb 1998;43:267-70.
Boleslawski E, Panis Y, Benoist S, Denet C, Mariani P, Valleur P.
Plain abdominal radiography as a routine procedure for acute
abdominal pain of the right lower quadrant: prospective evaluation.
World J Surg 1999;23:262-4.
Feyler S, Williamson V, King D. Plain abdominal radiographs in acute
medical emergencies: an abused investigation? Postgrad Med J 2002;
78:94-6.
Kellow ZS, MacInnes M, Kurzencwyg D, et al. The role of abdominal
radiography in the evaluation of the nontrauma emergency patient.
Radiology 2008;248:887-93.
Lee PW. The plain X-ray in the acute abdomen: a surgeon's
evaluation. Br J Surg 1976;63:763-6.
McCook TA, Ravin CE, Rice RP. Abdominal radiography in the
emergency department: a prospective analysis. Ann Emerg Med 1982;
11:7-8.
Eisenberg RL, Heineken P, Hedgcock MW, Federle M, Goldberg HI.
Evaluation of plain abdominal radiographs in the diagnosis of
abdominal pain. Ann Surg 1983;197:464-9.
Gupta K, Bhandari RK, Chander R. Comparative study of plain
abdomen and ultrasound in non-traumatic acute abdomen. Ind J Radiol
Imag 2005;15:109-15.
Grassi R, Romano S, Pinto A, Romano L. Gastro-duodenal
perforations: conventional plain film, US and CT findings in 166
consecutive patients. Eur J Radiol 2004;50:30-6.
Maglinte DD, Howard TJ, Lillemoe KD, Sandrasegaran K, Rex
DK. Small-bowel obstruction: state-of-the-art imaging and its
role in clinical management. Clin Gastroenterol Hepatol 2008;6:
130-9.
Ahn SH, Mayo-Smith WW, Murphy BL, Reinert SE, Cronan JJ. Acute
nontraumatic abdominal pain in adult patients: abdominal radiography
compared with CT evaluation. Radiology 2002;225:159-64.
Laméris W, van Randen A, Dijkgraaf MG, Bossuyt PM, Stoker J,
Boermeester MA. Optimization of diagnostic imaging use in patients
with acute abdominal pain (OPTIMA): Design and rationale. BMC
Emerg Med 2007 Aug 6;7:9.
Chen SC, Wang HP, Chen WJ, et al. Selective use of ultrasonography
for the detection of pneumoperitoneum. Acad Emerg Med 2002;9(6):
643-5.
Krishnan A, Brown R. Plain abdominal radiography in the diagnosis of
the ‘body packer.’. J Accid Emerg Med 1999;16:381.
Lappas JC, Reyes BL, Maglinte DD. Abdominal radiography findings
in small-bowel obstruction: relevance to triage for additional
diagnostic imaging. AJR Am J Roentgenol 2001;176:167-74.
Thompson WM, Kilani RK, Smith BB, et al. Accuracy of
abdominal radiography in acute small-bowel obstruction: does
reviewer experience matter? AJR Am J Roentgenol 2007;188:
W233-8.
Field S, Guy PJ, Upsdell SM, Scourfield AE. The erect abdominal
radiograph in the acute abdomen: should its routine use be abandoned?
Br Med J (Clin Res Ed) 1985;290:1934-6.
The role of plain radiographs in patients with acute abdominal pain at the ED
[27] Woodring JH, Heiser MJ. Detection of pneumoperitoneum
on chest radiographs: comparison of upright lateral and
posteroanterior projections. AJR Am J Roentgenol 1995;165:
45-7.
[28] Fukuya T, Hawes DR, Lu CC, Chang PJ, Barloon TJ. CT diagnosis of
small-bowel obstruction: efficacy in 60 patients. Am J Roentgenol
1992;158(4):765-9.
[29] Nagurney JT, Brown DF, Novelline RA, Kim J, Fischer RH.
Plain abdominal radiographs and abdominal CT scans for nontraumatic abdominal pain—added value? Am J Emerg Med 1999;
17:668-71.
589
[30] Assi Z, Platt JF, Francis IR, Cohan RH, Korobkin M. Sensitivity of CT
scout radiography and abdominal radiography for revealing ureteral
calculi on helical CT: implications for radiologic follow-up. AJR Am J
Roentgenol 2000;175:333-7.
[31] Jackman SV, Potter SR, Regan F, Jarrett TW. Plain abdominal x-ray
versus computerized tomography screening: sensitivity for stone
localization after nonenhanced spiral computerized tomography.
J Urol 2000;164:308-10.
[32] Hainaux B, Agneessens E, Bertinotti R, et al. Accuracy of MDCT in
predicting site of gastrointestinal tract perforation. AJR Am J
Roentgenol 2006;187:1179-83.
589.e1
Appendix A
Members of the OPTIMA study group:
Academic Medical Center, Amsterdam
A. van Randen MD, Departments of Radiology and Surgery
P.M.M. Bossuyt, PhD, Department of Clinical Epidemiology, Biostatistics, and Bioinformatics
W. Laméris, MSc, Departments of Surgery and Radiology
J. Stoker, MD, PhD, Department of Radiology
M.A. Boermeester, MD, PhD, Department of Surgery
St. Antonius Hospital Nieuwegein
B. van Ramshorst, MD, PhD, Department of Surgery
J.P.M. van Heesewijk, MD, PhD, Department of Radiology
M.P. Gorzeman, MD, Department of Emergency Medicine
Gelre Hospitals, Apeldoorn
W.H. Bouma, MD, PhD, Department of Surgery
W. ten Hove, MD, Department of Radiology
J. Winkelhagen, MD, Department of Surgery
University Medical Center Utrecht
H.G. Gooszen, MD, PhD, Department of Surgery,
M.S. van Leeuwen, MD, PhD, Department of Radiology
D.E.J.G.J. Dolmans, MD, PhD, Department of Surgery
Tergooi Hospitals, Hilversum
E. van Keulen, MD, Department of Radiology
J.W. Juttmann, MD, PhD, Department of Surgery
A.A.W. van Geloven, MD, PhD, Department of Surgery
M.J. van der Laan, MD, PhD, Department of Surgery
Onze Lieve Vrouwe Gasthuis, Amsterdam
S.C. Donkervoort, MD, Department of Surgery
V.P.M. van der Hulst, MD, Department of Radiology
Appendix B. List of possible diagnoses as
provided to the treating physician in the case
record form:
Diagnoses
Peritonitis
Perforated viscus
Bowel ischemia
Appendicitis
Diverticulitis
Acute cholecystitis
Acute pancreatitis
Nonspecific abdominal pain
No diagnosis
Nonspecific abdominal pain
Gastrointestinal disorder non urgent
Gastritis
Gastroenteritis
Ventricular ulcer
A. van Randen et al.
Epiploic appendagitis
Constipation
Abscess
Intraabdominal abscess
Retroperitoneal abscess
Liver abscess
Tubo-ovarian abscess
Abscess; located elsewhere
Bowel obstruction
Bowel obstruction most likely: carcinoma
Bowel obstruction most likely: inflammation
Bowel obstruction most likely: adhesion
Bowel obstruction most likely: pseudo-obstruction
Bowel obstruction most likely: other cause
Inflammatory bowel disorder
Small bowel or colon inflammation most likely: Crohn disease
Small bowel or colon inflammation most likely: ulcerative colitis
Small bowel or colon inflammation most likely: infectious colitis
Small bowel or colon inflammation: nonspecified
Hepatic-pancreatic-biliary disorders
Hepatitis
Liver metastases
Lever disorder nonspecified
Chronic pancreatitis
Cholecystolithiasis
Cholangitis
Choledocholithiasis
Urinary tract stones
Collecting system stones with obstruction
Uretheral stones with obstruction
Collecting system stones without obstruction
Uretheral stones without obstruction
Gynecologic disorders nonurgent
Endometrioses
Uterine myoma
Ovulation pain
Menstrual cramps
Benign ovarian cyst
Urgent gynecological disorders
Bleeding/rupture ovarian cyst
Ovarian torsion
Pelvic inflammatory disease
Extrauterine gravidity
Renal and urinary tract disorders
Urinary tract infection
Hydronephrosis
Pyelonephritis
Malignancy
Pancreas tumor
Renal tumor
Malignancy nonspecified
Extra-abdominal disorders
Myocardial infarction
Pneumonia
Mediastinitis
Other
Other
Mesenteric vein thrombosis
Herniation
Retroperitoneal or abdominal wall bleeding
The role of plain radiographs in patients with acute abdominal pain at the ED
Appendix C. Unblinded for review
OPTIMA trial expert panel members:
Academic Medical Centre, Amsterdam
O.R.C. Busch, Department of Surgery
T.M. van Gulik, Department of Surgery
O.D. Henneman, Department of Radiology,
Bronovo Hospital, Den Haag
589.e2
E.J. Hesselink, Department of Surgery
W. ten Hove, Department of Radiology
Appendix D. Differences in accuracy across
participating hospitals and level of experience
of the treating physicians at the ED
Tergooi Hospitals, Hilversum
A.A.W. van Geloven, Department of Surgery
J.W. Juttmann, Department of Surgery
E.M. van Keulen, Department of Radiology
Sites and treating
physicians
Accuracy after
clinical
evaluation
Accuracy after
evaluation of plain
radiographs
Onze Lieve Vrouwe Gasthuis, Amsterdam
S.C. Donkervoort, Department of Surgery
J. Peringa, Department of Radiology
M.P. Simons, Department of Surgery
Hospital
Hospital
Hospital
Hospital
Hospital
Hospital
47% (130/279)
53% (17/32)
48% (52/108)
50% (141/285)
53% (73/137)
54% (98/180)
50%
59%
46%
48%
53%
58%
48% (205/430)
49% (211/430)
52% (290/559)
53% (295/559)
St. Antonius Hospital Nieuwegein
H.W. van Es, Department of Radiology
P.M.N.Y.H. Go, Department of Surgery
M.J. Wiezer, Department of Surgery
Gelre Hospitals, Apeldoorn
W.H. Bouma, Department of Surgery
1
2
3
4
5
6
Low experienced
residents (b25 mo) ⁎
High experienced
residents (≥25 mo)
(140/279)
(19/32)
(50/108)
(138/285)
(72/137)
(105/180)
⁎ This cutoff is derived from a mean experience of 25 months for
all residents.