Guidelines for cardiac exercise testing
advertisement

European Heart Journal (1993) 14,969-988
Guidelines for cardiac exercise testing
ESC WORKING GROUP ON EXERCISE PHYSIOLOGY, PHYSIOPATHOLOGY AND ELECTROCARDIOGRAPHY
The Working Party agreed to produce Guidelines
which
embrace the full range of exercise testing in clinical
Exercise testing is one of the commonest non-invasive
as well as the requirements of research studies;
practice
cardiological tests performed to establish or confirm the
appropriate
end-points to measure efficacy of treatment
diagnosis and prognosis of cardiac disease and to evaluate
are
listed
for
each cardiac disorder, and the requirements
the effect of its treatment. Historically, exercise testing
of
the
various
regulatory agencies are also discussed.
developed as a diagnostic technique in the assessment of
and consideration should be taken
Where
special
care
coronary heart disease (CHD). While this is still the most
before
exercising
patients
with various categories of
common reason for requesting an exercise tolerance test
cardiac
disease,
this
has
been
indicated in the appropriate
(ETT), the spectrum of indications for exercise testing has
widened considerably — a fact only too obvious to those section. It is hoped that the recommendations made in the
who provide the service and who have seen an enormous report will form the basis of a European Guideline for
increase in demand for exercise tests in recent years. The Exercise Testing.
In the following sections, possible indications for
most important reasons for this are the use of exercise
testing post-myocardial infarction and in patients with exercise testing are classified in three groups: Disorders
known heart disease and new or recurrent symptoms after in which the use of exercise testing is generally accepted
interventions (PTCA or CABG). Two other areas have (accepted indications); Disorders in which exercise testing
also attracted increasing interest, namely to assess is often applied but in which the value and adequacy
functional capacity in patients with heart failure and to of testing is uncertain and a matter for discussion
provoke arrhythmias. More contentious areas, such as (possible indications); Disorders in which exercise testing
screening apparently healthy individuals for the presence is inappropriate, without any accepted value, or even
of CHD, have also contributed to the increase in exercise dangerous (not indicated or contra-indicated).
testing, as has its use in assessing fitness and guiding
exercise prescriptions.
General requirements relating to exercise testing
Refinements, such as computerization of the ECG
signal, have brought many advantages but also some LABORATORY REQUIREMENTS
Exercise testing should be carried out in a wellproblems. Measurement of gas exchange, formerly the
province of the physiologist, has quite definitely entered ventilated room, large enough to contain the equipment
and staff but with enough space for any emergency
the clinical arena, if as yet mainly in research.
More recently, the subject of protocol and method- procedures. The temperature should be controlled in the
ology has generated interest. Few apparently simple tests range of 18-22 °C, if necessary by air conditioning, and
have spawned such a diversity of methodology. Clinical humidity should not rise above 60%. A recovery couch
trials of new agents, especially for angina and heart should be available, and a telephone or other means
failure, have complicated the issue even further. Thus nearby to summon assistance if necessary. During all
there is now a plethora of protocols against a background tests on patients, full resuscitation equipment should be
of greatly increased demand. Thus, we believe it timely present (see below).
Subjects for testing should present at least 2 h after
to review the current situation and propose guidelines
for a greater degree of standardization on both the a light meal and be wearing comfortable clothes and
indications for exercise testing and on its methodology. suitable shoes. If repeated tests are to be performed,
In so doing we acknowledge previous European and they should be carried out at the same time of the day
and with the same (ergometer) test machine if there are
American recommendations on exercise testing'1"31.
A Working Party of the European Society of several in the laboratory. If a definitive quantification of
Cardiology's Working Group on Exercise Physiology, exercise capacity is required, one4 or more preliminary
Physiopathology and Electrocardiography was convened familiarization tests are necessary' '.
which met in Nyon, in February 1991, in Rotterdam in
June 1991, in Amsterdam in September 1991 and in Paris STAFFING
in January 1992. Names of those who assisted in the
Tests on normal subjects may be carried out by a
preparation of these Guidelines are given in Appendix 1.
trained nurse or technician, but for any tests on patients a
qualified physician and a technician familiar with exercise
Accepted for publication on 24 December 1992.
and resuscitation procedures must be in attendance. The
Correspondence: Dr Henry J. Dargie, Chairman: ESC Working Group
physician should carry out a pre-test examination and
on Exercise Physiology, Physiopathology and Electrocardiography, C/o
12-lead ECG to ensure that the patient is fit for the test.
Department of Cardiology, Western Infirmary, Glasgow G l 1 6NT, U.K.
Introduction
© 1993 The European Society of Cardiology
Downloaded from http://eurheartj.oxfordjournals.org/ by guest on September 30, 2016
0I95-668X/93/070969 + 20 $08.00/0
970
H. J. Dargie
Particular attention should be paid to the recovery phase,
when arrhythmias are most likely to occur. For more
complex procedures, such as cardiopulmonary exercise
tests, additional staff may be required.
EQUIPMENT
The ergometer used may be a treadmill or bicycle. The
apparatus should be maintained and calibrated at regular
intervals (about every 6 months). A treadmill may be
calibrated by measuring the angle with a protractor, and
speed by counting the revolutions of a chalk mark on the
belt over a fixed period of time. Bicycles are more difficult
to calibrate, as this involves measurement of work done
against a fixed load by a dynamometer.
During all tests, at least three ECG leads should be
monitored continuously. A facility for printing the lead
should be available, and records should be taken at rest in
the exercise position prior to exercise, at the end of each
exercise stage, at peak exercise and at each minute of
recovery up to 6 min. An automated ST segment monitor
is desirable, with the sensing point usually set at 60 ms
after the J point. Care should be taken with electrode
positioning, skin preparation and lead fixation to ensure a
good quality signal throughout exercise. For diagnostic
tests in coronary artery disease, a full 12-lead disclosure is
preferable to a single lead system to permit more accurate
localization of any ischaemic changes. The diagnostic
value of the orthogonal three-lead system is still under
investigation.
Blood pressure (systolic) should be recorded every
3 min, or more frequently if indicated by the clinical state.
A wall-mounted mercury sphygmomanometer is most
convenient, although Doppler instruments are also
useful. Blood pressure should always be recorded at the
final workload. If high-risk patients are to be studied,
it may be necessary to measure blood pressure more
frequently, e.g. each minute throughout exercise and
recovery.
Certain centres may supplement the above minimum
essentials with additional equipment, such as apparatus
for measurement of respiratory gas exchange during
exercise, a gamma camera for radionuclide imaging, or an
echocardiogram for measuring stress-induced changes. If
respiratory gas exchange is to be measured, then the
temperature and humidity of the room will need to be
recorded, as well as barometric pressure. Gas analysis
may be slow (such as paramagnetic) or fast (mass
spectrometers, zirconium cells), and the results are usually
collected and displayed by an on-line dedicated computer.
Fast analysers are capable of breath-by-breath analysis,
but the results are difficult to interpret and so are usually
averaged over a 15 or 30 s period. The ventilometer
used must be regularly inspected, and the whole system
requires daily calibration and meticulous care. Other
parameters which it may be found useful to measure
during exercise include end-tidal CO2 (for detection
of hyperventilation and computing Vd/Vt), oxygen
saturation (for detection of pulmonary disease), and
transcutaneous O, or CO, tensions.
All centres should have full emergency equipment
immediately available including: (a) Oxygen, by cylinder
or wall-pipe; (b) A defibrillator, regularly checked and
on charge; (c) Facilities for intubation and manual
respiration; (d) A box containing resuscitation drugs such
as atropine, adrenaline, nitroglycerin, lignocaine, sodium
bicarbonate and calcium chloride; suction apparatus is
also desirable.
TEST TERMINATION
The test is terminated at the discretion of the physician
for one or more of the following reasons: (i) Symptom
limitation — the patient cannot continue because of
pain, fatigue or dyspnoea; the use of Borg scales is
recommended; (ii) A diagnostic end-point has been
achieved — a suitable ST change (see below), an arrhythmia provoked, or the occurrence of the presenting
complaint (chest pain, leg pain, etc); (iii) Safety reasons
compel cessation — a sustained fall in systolic blood
pressure of 20 mmHg or other inappropriate response to
increasing workload; patient distress; excessive ST change
such as a rise or fall of more than 4 mm; or arrhythmias,
such as atrial fibrillation, sustained ventricular tachycardia, bradycardia or AV block; (iv) The physician in
attendance is concerned for the welfare of the patient on
clinical grounds.
The reason for stopping the test and the symptoms at
that time (including their severity) should always be
recorded.
COMPUTER-ASSISTED TESTING
In order to facilitate interpretation of the ECG during
exercise, the noise level can be reduced by computer
processing. Nevertheless the emphasis should be on
the prevention of excessive noise by proper electrode
preparation. Early exercise systems used computer
analysis of a single lead during exercise. It is now evident
that optimal results can only be obtained by analysis of
multiple leads recorded simultaneously. Most modern
systems use three leads or a full 12-lead system.
Analog-digital conversion is performed at a rate
between 200 and 500 samples per second or more. The
QRS complexes are detected with the aid of a combination of the derivatives of multiple ECG leads. Thus the
characteristic feature used for QRS detection is the large
voltage changes which occur in all leads simultaneously
during ventricular activation. The QRS complexes are
then classified as 'normal' or 'abnormal'. Abnormal
beats may be a result of premature ventricular or supraventricular complexes, or they may be normal beats
distorted by excessive noise or baseline drift. The normal
beats are then combined into a single representative
complex by computation of an average (mean) or median
beat. Signal averaging can be performed at pre-selected
intervals, for example during 20 s of each minute or
continuously. The latter is the method of choice because
it permits continuous display of the up-dated ECG
waveform. Since the averaging procedure will be subject
to errors in some patients, the user should compare the
shape of the averaged signal with the original ECG
Guidelines for cardiac testing 971
tracings. From the representative complexes, measurements can be obtained. The noise level during exercise is
rather high in comparison with resting ECGs, so it is not
appropriate to take measurements from individual beats
as is the case in some resting ECG programs. In several
commercially available systems, the baseline and ST
segment are defined at fixed intervals before and after a
singlefiducialpoint in the QRS complex. This method will
fail in many patients with abnormal ECGs at rest, while
the measurement points will shift in time if the shape of
the QRS waveform changes during exercise. Therefore it
is necessary to define the proper onset and end of the QRS
complex. Such precise definition of QRS onset and end is
only possible if a combination of multiple leads is used.
Unfortunately, several commercially available systems
for computer-assisted exercise electrocardiography do
not meet the necessary requirements. The cardiologist
who wishes to buy such a system should check the design
and performance of the systems under consideration.
Key points which should be considered include the
following:
The number of leads which are simultaneously
analysed; a minimum of three leads is required for
adequate signal processing.
Verification of the averaging procedure; verification
requires presentation of both the original ECG and the
representative average complexes. These should be
presented preferably on the same paper using the same
amplitude and time scales.
Measurements included for ECG interpretation and
how they can be checked: the detection of the onset and
end of the QRS complex can be checked if markers are
provided in the display of the averaged beats which
indicate where these points have been defined. If these
markers are not in the correct position, the whole ECG
analysis should be disregarded.
Whether or not the system has been tested rigorously
under clinical conditions; in our opinion, all commercially
available systems should be tested in clinical practice.
Such tests should include a description of the system
performance in a large number of patients with various
abnormalities, together with a summary of the diagnostic
performance of the system in comparison with an
independent method such as coronary arteriography or
thallium scintigraphy. Unfortunately, as far as is known,
the latter type of testing has not been undertaken with the
commercially available systems.
Studies which have compared the diagnostic performance of visual reading and computer-assisted ECG
interpretation during exercise, support an improved
diagnostic performance by computer analysis when ST
amplitude and slope measurements were used in combination with heart rate and peak workload or treadmill
time.
In addition to improving the ECG interpretation
by quantitative ECG analysis, by presentation of
ST-isopotential plots and by facilitation of visual
interpretation through noise reduction, the computer
system can be used to regulate the bicycle or treadmill
according to one of several pre-defined protocols, to start
and stop the ECG writer at appropriate times and to
generate a summary report of the test.
It is of advantage if such a report includes a statistical
analysis of the test results. If the test is performed to
document the presence or absence of coronary disease in a
given subject, the report should specify: the pre-test
probability of disease based on age, gender, classification
of symptoms and possibly the classical risk factors; the
post-test probability of disease by combining the pretest probability and the observations during the test:
workload, chest pain, ST changes.
In tests conducted in patients with known coronary
disease, the results should be presented in terms of:
probability of exercise-induced ischaemia based on ECG
changes and symptoms during the test; prognosis, using
exercise tolerance and/or the blood pressure response
during exercise.
LEAD SYSTEMS FOR EXERCISE ELECTROCARDIOGRAPHY
The selection of a lead system may depend on the
subject under investigation. For monitoring the heart rate
and arrhythmias, for example in sports medicine, any
bipolar chest lead will suffice. In patients with suspected
coronary artery disease and with a normal ECG at rest,
a single lead system may be used but three leads are
preferred. The optimal single lead for detection of ST
segment depression during exercise is a bipolar lead from
the right infraclavicular region to V5. With such a single
lead (CM5), precordial ST segment depression will be
missed in approximately 10% of patients. The reader
should appreciate that leads like CS5, CM5 and V5 are
different and that criteria applied to one lead do not
correspond in a 1:1 fashion when another lead is used.
In patients with a previous myocardial infarction or
other heart disease, a single lead system is certainly
inadequate. Such patients may be tested with a pseudoorthogonal lead system'51, with a corrected orthogonallead system (computer-processed Frank leads) or with
three or more standard leads. If a three-lead ECG writer is
used, V2, V4 and V5 can be monitored continuously
with intermittent recordings of leads I, II and III. The
electrodes for the limb leads should then be placed below
the clavicles or above the crista scapulae, and just above
the spina iliaca superior posterior'6'. A similar system can
be used to record the standard 12 leads, with or without
additional special bipolar chest leads'71. A further
improvement is the use of a limited precordial map'81, for
example the 16-lead map which can be constructed from
alternating recordings on paper of four sets of four
precordial leads, or preferably by computer processing of
16 leads.
For computer processing, a combination of three
pseudo-orthogonal or orthogonal leads is preferred.
However, modern computer systems can provide
continuous analysis of the 12 standard leads.
FORM OF REPORT
It is essential that all details of the test are recorded and
a suitable form should be designed. The form should
contain the following information:
972 H. J. Dargie
(1) Patients name, address, age/date of birth, sex, weight
and height.
(2) Hospital or other identification number.
(3) Date and time of test.
(4) In laboratories using various equipment for exercise
testing, the identification number of the equipment
used should be included in the report.
(5) Reason for referral.
(6) Previous drug therapy, especially digoxin or betaadrenoreceptor antagonists — were they stopped
beforehand? If so, when? Is there a pacemaker insitul If so, how is it programmed? Anti-anginal drug
therapy need not be stopped routinely although in
cases of diagnostic doubt a repeat test should be
carried out of treatment if possible.
(7) Baseline 12 lead ECG rhythm, abnormalities.
(8) Ambient conditions — temperature, humidity,
barometric pressure.
(9) Exercise protocol used — MET equivalents if VO2
not measured.
(10) Duration achieved and reason for stopping.
(11) MET equivalents if VO2 not measured.
(12) Peak VO2, VE and AT.
(13) Symptoms at peak exercise and their severity.
(14) Heart rate, systolic pressure and ST segment levels at
rest, at each stage, at peak and during recovery.
(15) Pre- and post-test probability of CHD.
(16) Comments and conclusions.
Physiological differences between
protocols: is there an optimum?
Introduction
Exercise testing in clinical practice has two primary aims.
Firstly, to provoke an identifiable clinical response which
may be a symptom, such as chest pain or dyspnoea, a
change in one or more of a number of physiological
variables, including heart rate and blood pressure, or
the appearance of a specific ECG abnormality, most
commonly ST segment shift/arrhythmia. And, secondly,
to determine the workload achieved at the time of the
response or at the maximum effort. Many protocols
within differing modes of exercise have been described
and are currently in clinical use in different countries in
Europe and elsewhere191. These will be briefly reviewed,
but since the responses we seek from exercise testing
have important implications for diagnosis, prognosis,
treatment, screening, or fitness assessment, it is also
necessary to exclude the possibility that the type of
protocol used could influence the result of exercise testing.
Moreover, the increasing clinical demand for exercise
testing dictates that the average time taken to complete
the protocol should be as short as is conducive with the
collection of the maximum possible information from the
test.
Background
The currency of exercise is oxygen and its uptake by the
body (VO2) is directly related to the work performed. At
2500
1
I 2000
j» 1500
a
1
g
100
°
be
°
500 h
I
0
20
I
I
40
.
I
'
I
I
I
'
I
I
I
L.
60
80 100 120 140 160
Load (W)
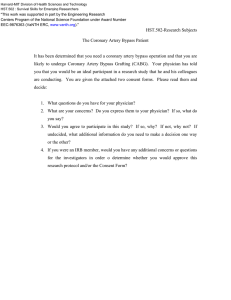
Figure 1 Oxygen uptake and workload. Absolute VO2 increases
linearly with workload.
rest, the VO2 is approximately 3-5 ml. kg ' . min ',
which is often referred to as one metabolic equivalent or
1 MET. During maximum exercise, the oxygen uptake
(VO2 max) may rise to 70-80 ml. kg" 1 . min"1 in an elite
athlete, although in the modern sedentary man or woman
values of 30-40 ml. kg"'. min"' are more typical'3-101.
Patients exhibit a wide spectrum of exercise capacity
which is best reflected by the peak VO2 which ranges from
less than 10 ml. k g " ' . min"' in patients with severe heart
failure to values approaching normal in fitter patients
being investigated for chest pain. This creates difficulty in
recommending a single test appropriate for all patients.
Tests that start with very low energy costs to accommodate subjects with a poor exercise capacity result in very
long tests for better performers. Such long protocols may
produce unrepresentative values as subjects become
bored, experience discomfort or lack commitment for a
sustained effort. Conversely, short duration tests with
large energy cost increments may limit the attainment of a
true maximum as some subjects will experience difficulty
in coping with large energy cost increases between
stages. In practice, the average peak VO2 of the spectrum
of symptomatic patients undergoing cardiac investigations or taking part in clinical trials corresponds to
approximately 6 METS or 21 ml. kg" 1 . min"2.
There are certain fundamental differences between
treadmill and bicycle exercise. During bicycle testing,
the workload is independent of body weight, and total
oxygen consumption is closely related to workload
(Fig. 1); however, the relative oxygen consumption (i.e.
ml O 2 . k g " ' . min"1) for a given workload will be different for subjects of different body weight. During treadmill
exercise the total oxygen consumption varies while the
relative oxygen consumption during each stage is similar
because each subject supports his/her body weight. Thus
treadmill testing is automatically standardized for body
weight since, obviously, subjects have to carry their own
body weight. With both modalities, variations will occur
as a result of inter-individual differences in efficiency of
exercise.
Guidelines for cardiac testing
^ 50 .5
40
7' 30
bo
A
y*'
*''
•
•
973
the main criticism of the modified Bruce, Balke and
Naughton protocols, which could be termed 'slow"
protocols, is their long duration.
BICYCLE
In contrast to the Anglo-Saxon world, in many
European countries the bicycle ergometer is preferred to
the treadmill for exercise testing. In German-speaking
10 countries,
a survey covering 712 285 test procedures
i
1
1
I
I
1
showed that exercise tests were bicycle ergometer tests
6
9
12
18
15
in 88%, climbing tests in 11% and treadmill tests in
Time (min)
0-5%"41. Even though not so many muscles are involved,
Figure 2 Estimated energy costs. A =60 kg at 20 W; • =90 kg at
workloads in absolute terms are independent of body
20 W; O = either on Modified Bruce.
weight and most people can carry out the test without
having specially been taught before. There are bicycle
The practical importance of this is apparent from tests in both the sitting and the supine position: out of
Fig. 2, where it can be seen that to achieve a VO2 88% performed in the German-speaking countries of
of 25ml .kg" 1 . min"1 (approx 7METS) would take Europe, 57% were performed in the supine and 31% in
(a) 5 min for a 60 kg person starting at 20 W and increas- the sitting position.
ing by 20 W . min"1 to 100 W; (b) 8 min (>60% longer)
The advantages of the supine position are excellent
for a 90 kg person on a similar bicycle protocol; and (c)
quality of the exercise ECG, safer conditions in case of
12 min for either subject on a Modified Bruce treadmill
emergency, comparability with the results of other tests
protocol.
in cardiology which are preferably performed in the
Finally, it should be emphasized that the physiological supine position, such as radionuclide studies, exercise
responses to exercise are related more closely to relative echocardiography, and evaluation of haemodynamics
oxygen uptake than to absolute uptake. Thus, in subjects with floating catheter during exercise. In addition,
of similar fitness and ability but not necessarily of the ischaemia in an exercise test in the supine position is easier
same weight, any given treadmill workload should 'feel' to provoke than in the sitting position.
approximately the same since the relative energy costs are
The advantages of the sitting position are higher
similar. In contrast, the same bicycle workload is likely to
exercise tolerance as a consequence of later onset of leg
'feel' harder for smaller subjects since their relative energy
fatigue, and fewer occurrences of lung oedema as a
costs will be higher'1''.
complication of exercise testing in patients with mitral
At the present time, most bicycle protocols utilise stenosis or with impaired left ventricular function.
absolute workloads, which is certainly simpler. The
The workload is usually described in terms of watts (W)
alternative view is that workloads relative to body weight
and many permutations of wattage increases and
or surface area should be adopted so that rates of oxygen
duration of stages have been described. In one protocol,
uptake within individual subjects would be as similar as
fairly widely used in Europe, increments are of 20 W per
possible.
1 min stage starting from a base of 20 W'151 which, for an
average subject, produces a rate of oxygen uptake similar
Protocols
to that of the Bruce protocol. However, variations of this
The various general types of exercise protocol have are common in individual laboratories. In terms of
been extensively reviewed'91. The most common exercise 'speed', the commonly used graded bicycle protocols
protocols have a graded increase in workload with time beginning at 10, 20 or 30 W will be 'fast' or 'slow'
rather than employ a fixed workload. It has been shown depending on the weight and muscle power of individual
during both bicycle and treadmill exercise that, in terms of subjects.
a number of performance indicators, protocols with short
stages and small increases in workload are better than 'DESIGNER' PROTOCOLS
long stages with large increments; and that virtually
A large number of protocols have been designed
continuous increases in work using a 'ramp' protocol according to the individual patient circumstances
produce similar results to 1 min work increments'12'31.
especially for research purposes and for clinical trials.
Some of these include a 'steady state' at a sub-maximal
workload.
TREADMILL
In clinical practice, the Bruce protocol or one of its
modifications is by far the commonest treadmill protocol,
Free walking tests
being favoured by approximately 70% of all centres in the
The 6 or 12 min corridor walking tests have proved
United States. Other commonly used protocols include
the Balke and Naughton tests. The Bruce protocol, which useful in clinical trials, especially in heart failure patients.
could be termed a 'fast' protocol, has been criticized Such tests require no sophisticated equipment, but do
because of its large increases in workload at each stage require a free hospital corridor or area of uninterrupted
which patients may be unable to complete. Conversely, space'16'. There are obvious disadvantages to the
|
20
974
H. J. Dargie
application of this in a busy clinical practice, and
standardization of the test, especially with regard to the
availability, business and temperature of the corridor,
could be a problem. Currently the 6 min test has been
advocated and been shown to correlate well with peak
VO2 obtained from formal exercise testing1'7'.
5-
• Bruce
4 --
o
i
(20 W min
_
Weld.
Towards standardization
DOES THE PROTOCOL MATTER?
In both normal subjects and patients with heart failure,
the peak oxygen consumption is partly dependent upon
the type of protocol used, as is the limiting symptom'18'"1.
A fast test usually results in more breathlessness while a
slow test is usually terminated by fatigue. Similarly, in
angina patients, the ischaemic response to exercise can be
influenced by the exercise protocol used. During a slow
protocol, the rate-pressure product at the onset of
ischaemia is significantly lower than when a fast protocol
is employed'201, while a fast protocol, such as the standard
Bruce or 20 kg. min" 1 bicycle, may be more reliable in
provoking ST segment changes suggestive of ischaemia.
Thus, the primary aims of exercise testing with respect to
the provocation of symptoms, physiological variables, ST
segment shift and exercise duration all can be significantly
influenced by the protocol.
IS THERE AN IDEAL PROTOCOL''
While no single protocol could possibly suit all clinical
and experimental purposes, the prospect of a protocol
which could be applied to a wide range of subjects for
routine exercise testing is, nevertheless, appealing. Such a
test would have a low starting oxygen requirement that
rose only gradually at first. However, in order that it
terminated timeously (a median duration of 10 min is
recommended'19') and to stress the patients with better
exercise capacity to their maximum (which even in the
fittest patients is extremely unlikely to exceed 14 METS),
the later stages would require to be progressively harder.
Initial attempts to develop different physiological
protocols have met with some success and research in this
area is continuing'13'2'1.
It is customary to record effort capacity in terms of
minutes for treadmill tests and watts for bicycle tests.
As should be clear from the foregoing, these values vary
enormously according to the protocol used, creating
unnecessary confusion in the interpretation of the result.
Thus, effort capacity should be expressed in METS rather
than minutes or watts. Clinicians should become familiar
with, for example, the fact that stages 1 and 3 of the Bruce
protocol represent 3 and 10 METS respectively. This
conversion is more difficult for bicycle exercise, but
standard tables are available based on workload and body
mass index. With practice in Europe divided in the choice
of exercise modality, there is a strong case for adopting
protocols that require similar energy costs over unit time.
Conclusions and recommendations
It is desirable that, in the investigation of similar groups
of patients such as those with angina, post-myocardial
Lj-ToWmin
2 O
1
1
1
i'
6
9
12
Time (min)
i
i
15
18
Figure 3 Comparison of oxygen requirements over time for two
bicycle protocols (steps of 20 W . min"' or 10 W . mm" 1 ) and two
treadmill protocols (Bruce, Weld). The horizontal axis represents
time in minutes and the vertical axis represents average oxygen
uptake (1 min"'). It should be noted that the actual oxygen consumption of a given patient at a certain level of exercise varies widely and
depends on their level of physical condition. Furthermore, oxygen
consumption on the treadmill is dependent on body weight.
infarction, heart failure or arrhythmias, there is more
uniformity in the type of protocol used. At the present
time, the 'ideal' protocol, suitable for all cardiac patients
has not been validated and no single protocol is likely
to satisfy all needs. For the time being, the Group
recommends the following for clinical testing but different
protocols may be preferred for clinical trials:
TREADMILL EXERCISE TESTING
(a) Angina and post-MI and arrhythmia: Bruce protocol
(b) Heart failure or severe angina: Modified Bruce or
Balke
BICYCLE EXERCISE TESTING:
(a) Angina, post-MI and arrhythmia: 20 W. min"1
(b) Heart failure or severe angina: 10 W . min"1
These protocols are described in Fig. 3.
The Working Group recognizes that, particularly with
respect to bicycle protocols, many different variations are
already established in clinical practice. Nevertheless
these differences are not likely to be of major clinical
importance and much would be gained in terms of
standardization if the recommended protocol were to be
adopted by members of the ESC.
Within these recommendations, it may be considered
quite reasonable for larger, fitter persons to start the
protocol at an appropriately higher workload to avoid an
excessively long test.
Moreover it must be emphasized that, for scientific
purposes, other protocols appropriate to the question
being addressed may be perfectly valid.
Guidelines for cardiac testing 975
Table I Coronary artery disease post test likelihood (%) based on age, sex, symptom classification and exercise-induced electrocardiographic
STsegment depression
Typical angina
Possihlc or
atypical angina
Non-specific or
non-anginal
chest pain
Asymptomatic
Male
Female
Male
Female
Male
Male
0-00-0-04
005-009
010-014
015-0-19
0-20-0-24
>0-25
25
68
83
91
96
99
7
24
42
59
79
93
6
21
38
55
76
92
I
4
9
15
33
63
1
5
10
19
39
68
000-004
005-009
0-10-0-14
015-019
0-20-0-24
>0-25
61
86
94
97
99
>99
22
53
72
84
93
98
16
44
64
78
91
97
3
12
25
39
63
86
4
13
26
41
65
87
I
3
6
11
24
53
50-59
000-004
0-05-0 09
010-014
015-019
0-20-0-24
>O-25
73
91
96
98
99
>99
47
78
89
94
98
99
25
57
75
86
94
98
10
31
50
67
84
95
6
20
37
53
75
91
60-69
000-004
005-009
010-0-14
015-019
0-20-0-24
>0-25
79
94
97
99
99
>99
69
90
95
98
99
>99
32
65
81
89
96
99
21
52
72
83
93
98
8
26
45
62
81
94
Age
(years)
ST depression
(mV)
30-39
40-49
Female
Female
< I
1
2
2
4
7
18
43
3
8
24
<1
4
<1
1
3
11
39
69
<1
1
2
4
10
28
2
8
16
28
50
78
2
9
19
31
54
81
1
3
7
12
27
56
5
17
33
49
72
90
3
11
23
37
61
85
2
7
15
25
47
76
1
5
11
20
Reprinted from Neth J Cardiol 1989; 2.
Future directions
Little research has been carried out in recent years
concerning the impact of protocol on the outcome of
exercise testing. Nevertheless, some recent evidence
suggests that the protocol can influence the result of
the test. Whether these differences would influence
management decisions remains to be seen. The group
recommend that further research is needed with respect
to diagnosis, tolerability, convenience and patient
acceptability.
Coronary artery disease
Introduction
Exercise testing can be used to establish or confirm the
diagnosis of coronary heart disease (CHD) and to
measure exercise tolerance in order to evaluate the
symptoms and assess the prognosis of a given patient. It
is valuable in the assessment of treatment with antiischaemic drugs, percutaneous transluminal coronary
angioplasty (PTCA) or coronary artery bypass surgery
(CABG). These interventions are aimed at the improvement of both symptoms and ischaemia and, in some
subgroups of patients, prognosis. The evaluation of
atheroma regression studies by cholesterol lowering
drugs, lifestyle change or other interventions also now
require to be considered.
Recommendations
EXERCISE TESTING IN PATIENTS WITH SYMPTOMS
SUGGESTIVE OF CORONARY ARTERY DISEASE OR WITH
KNOWN CORONARY ARTERY DISEASE
Key points
In addition to a careful history and physical
examination, exercise testing can help in diagnosing
coronary artery disease'221. A pre-test probability of the
presence of coronary artery disease should be estimated
based on history, age, sex and risk factors. In accordance
with Bayes theorem, the symptoms should be classified as
either typical, or possible/atypical angina or non-specific
chest pain. Typical angina has three characteristics: location on the chest, triggering by exertion, stress, etc, and
prompt relief by rest or nitrates. Possible or atypical
angina has two of these characteristics and non-specific or
non-anginal chest pain only one.
By combining this pre-test probability and the results
of the stress test, the final post-test probability of the
presence (or absence) of coronary artery disease can be
calculated, as shown in Table 1. A continuous scale of
976 H. J. Dargie
Table 2 Conditions and circumstances that can cause a false-positive
exercise test
Valvular heart disease
Congenital heart disease
Cardiomyopathy
Pericardial disorders
Drug administration
Electrolyte abnormalities
Non-fasting state
Anaemia
Sudden excessive exercise
Inadequate recording equipment
Bundle branch block
Left ventricular hypertrophy
WolfT-Parkinson-White syndrome and other types of pre-excitation
Mitral valve prolapse
Vasoregulatory abnormality
Hyperventilation repolarization abnormalities
Hypertension
Improper lead systems
Incorrect criteria
Adapted from Froelicher VF. Exercise and the heart: clinical
concepts.
Year Book Medical Publishers Inc, 1987: 123.
probability is preferable to artificial separation into
'positive' or 'negative' tests'231. The predictive value of the
test is related to the prevalence of coronary artery disease
in the population examined.
ST segment depression in the absence of coronary
artery disease, so-called false-positive tests, are frequently found in women, in the presence of mitral valve
prolapse, electrolyte disturbances, anaemia, and with
baseline repolarization abnormalities related to left
bundle branch block (LBBB), left ventricular hypertrophy (LVH) or other conduction disturbances, preexcitation, sympathetic overdrive, digitalis therapy and
continuous or intermittently paced rhythm (Table 2)[24).
Absence of ST depression despite the presence of CHD,
so-called false-negative results, can be found when
beta-blockers, calcium antagonists or nitrates are not
withdrawn, when the level of exercise during the test is
inadequate, or when inappropriate lead systems are used.
It should be appreciated that complete agreement
between functional information, such as ECG changes
during exercise, and anatomy as revealed by coronary
angiography cannot exist. If coronary angiography is
considered to be the gold standard for the presence or
absence of coronary disease, all non-invasive tests will
result in a proportion of false-positive and -negative
results.
It has been shown by multivariate analysis that the
sensitivity and specificity of the test are markedly
improved when heart rate, blood pressure response,
duration of the test, and the appearance and duration of
symptoms are taken into consideration in addition to the
ECG1251. Computerization of the ECG signal together
with these variables also can enhance the accuracy of
exercise testing in diagnosing CHD.
In patients with a high pre-test probability, the test
provides little additional diagnostic information, but
evaluation of exercise tolerance provides a basis for
counselling on work, recreational activities, medical or
surgical therapy and assessment of prognosis.
Accepted indications
(1) Diagnosis of coronary artery disease in patients with
suspected episodes of myocardial ischaemia;
(2) Risk stratification of patients with known coronary
artery disease;
(3) Assessment of symptoms and disability.
(4) Evaluation of suitability for and assessment of
exercise training and rehabilitation;
(5) Regular follow-up of patients with known coronary
artery disease.
Possible indications
(1) Diagnosis of coronary artery disease in patients with
atypical anginal chest pain;
(2) Diagnosis of coronary artery disease in patients using
digitalis;
(3) Diagnosis of coronary artery disease in patients with
conduction disturbances (bundle branch block,
Wolff-Parkinson-White Syndrome);
(4) Evaluation of patients with variant angina pectoris;
(5) Follow-up of exercise tolerance in patients after
cardiac rehabilitation.
Contra-indicated
Patients with serious unstable angina (chest pain at rest
within the previous 48 h) or suspected acute myocardial
infarction.
SCREENING FOR CORONARY ARTERY DISEASE OF
APPARENTLY HEALTHY INDIVIDUALS
Key point
Many false-positive tests occur (low predictive value)
due to the low prevalence of coronary artery disease in this
population and the limited sensitivity and specificity of
the test. The potential iatrogenic harm in this population
is fairly large. The 'possible indications' should, therefore,
be applied with caution.
Accepted indications
(1) Evaluation of asymptomatic males over 40 years
with specific professions including pilots, firemen,
policemen, bus- and lorry-drivers, etc (see under
Regulatory Affairs).
Possible indications
(1) Asymptomatic males and females over 40 years
having two or more risk factors for coronary artery
disease, e.g. history of vascular disease, raised
cholesterol, raised blood pressure, heavy cigarette
smoking, diabetes mellitus, and family history
predisposed to cardiovascular disease;
(2) Those taking up sport, vigorous exercise.
Guidelines for cardiac testing 977
Not indicated
(1) Evaluation of asymptomatic persons with a pre-test
probability of CHD of < 10%, e.g. persons with nonspecific symptoms and little suggestion of cardiac
disease ('exclusion of disease') with the exception of
those with specific professions as listed above.
EXERCISE TESTING IN PATIENTS AFTER MYOCARDIAL
INFARCTION
Key points
The optimal time for exercise testing after acute
myocardial infarction (AMI) is when the gain in terms of
management decisions is substantially greater than the
risk of the test. These risks are determined mainly by the
selection of patients, but also by the timing of the test and
the method of testing. Good clinical judgement is the
major factor in these situations. With appropriate
selection, a symptom-limited exercise test can safely be
conducted 7-14 days after AMI (pre-discharge) although
for clinical or logistic reasons it may be carried out at
3-4 weeks (post-discharge).
There are no data to show that exercise to an arbitrary
percentage of the estimated maximal heart rate or work
load is safter than a symptom-limited exercise. The usual
stopping criteria can be applied. Since heart rate is a
poor indicator of the stress on the heart, especially in the
presence of beta-blockers or in patients with severely
impaired LV function, a symptom-limited ETT is
preferred. This is safe but clinical judgement must be
applied (see under General Requirements).
The prognosis of a patient after AMI is closely related
to left ventricular function, exercise tolerance and the
increase of systolic blood pressure during exercise. In
earlier studies patients with ST segment depression
appeared to have a worse prognosis but in most recent
studies this is less apparent. The appearance of ventricular arrthymias during exercise is usually related to
impaired left ventricular function and probably has little
independent prognostic value'26271.
A ccepted indications
(1) Risk stratification and assessment of exercise
tolerance in patients after myocardial infarction. The
risk of subsequent cardiac events in over 1000 hospital
survivors of AMI stratified by exercise testing is
shown in Table 3[28].
(3) Atrio-ventricular block/new intra-ventricular conduction defects.
EXERCISE TESTING IN THE ASSESSMENT OF INTERVENTIONS
Key points
Irrespective of which anti-ischaemic intervention is
to be evaluated, exercise testing before and after the
intervention must be standardized with consideration of
the guidelines generally accepted in exercise testing.
Different protocols can be used to evaluate the antiischaemic effects of drugs, PTCA and CABG. However,
protocols with small increments of load or ramp protocols
and a total test duration up to 10-12 min should be
recommended. It is important, however, that not only
the protocol but also the equipment, time of day,
laboratory temperature etc. are identical before and after
the intervention, especially in research studies, e.g.
pharmacological investigations.
Also independent of the specific intervention are the
measured variables used to evaluate anti-ischaemic
interventions which should include (i) Angina pectoris
(e.g. Borg scale—Table 4) and ST segment depression
during identical workloads, especially the highest workload reached pre- and post-intervention, (ii) Maximal
exercise tolerance (watts, exercise time, rate pressure
product [RPP]). (iii) Exercise tolerance (watts, exercise
time, RPP) without angina pectoris, i.e. 'angina-free
exercise tolerance, (iv) Exercise tolerance (watts, exercise
time, RPP) at 0-1 mV (1 mm) ST segment depression; this
may be called 'ischaemia-free' exercise tolerance.
EVALUATION OF CLINICAL DRUG THERAPY
Key points
At present, exercise testing is not performed routinely
in the clinical evaluation of anti-ischaemic drugs in the
individual patient. In most cases, reduction in the
frequency or severity of episodes of chest pain is the sole
criterion.
In patients with only silent myocardial ischaemia (SMI)
(e.g. post MI), ST segment depression during exercise
testing can be used to assess therapy. However, it remains
to be seen whether eradication or reduction of SMI by
drug therapy in patients with CH D is an important goal of
clinical management including drug therapy.
Exercise testing provides objective assessment in
clinical trials of anti-ischaemic drugs when more precise
variables can be measured (see under Evaluation of Drug
Therapy).
Possible indications
(1) Evaluation of patients with an accepted indication,
e.g. angina, but in whom the baseline repolarization
or concomitant medical problems restrict the value of
the test. The duration of exercise, the behaviour of the
blood pressure response and/or the appearance of
symptoms may provide valuable information in these
patients.
Possible indications
(1) Monitoring of silent myocardial ischaemia;
(2) Clinical evaluation of drug therapy in individual
patients.
Conlra-indications
(1) Early post-infarction angina;
(2) Presence of severe heart failure;
Contra-indications
(1) Unstable angina or suspected acute myocardial
infarction.
A ccepted indications
None.
mis
5-3%
—
—
15-8%
—
n=l9
1-4%
3-3%
5-7%
4-5%
0-6%
4-4%
4-4%
—
>=30
n = 489
2-2%
2-9%
<30
n=I36
mis
29-4%
5-9%
—
11-8%
—
n=17
10-4%
—
6-3%
—
<30
n = 48
Exercise test
Exercise test
5-6%
10 3%
0-9%
3-7%
5-6%
>=30
n=107
Mis = missing data; PTCA = percutaneous coronary angioplasty; CABG = coronary artery bypass grafting.
PTCA
CABG
Both
Mortality
Reinfarct
SBP
(mmHg)
Repeat infarction
and/or
diuretics/digitalis
First infarction
no diuretics/digitalis
No ischaemia
n = 816
211%
15-8%
—
5-3%
5-3%
n=19
mis
Hospital survivors
n=1043
1-3%
3-8%
101%
12-7%
1-3%
11-6%
20-9%
2-3%
>=30
n = 79
2-3%
4-7%
<30
n = 43
Exercise test
First infarction
no diuretics/digitalis
5-9%
2-4%
—
11-8%
—
n= 17
mis
Angina/reinfarction
n = 227
Table 3 Mortality, reinfarction and revascularizalion procedures withinfirstyear in patients categorized according to clinical data and exercise test results
Downloaded from http://eurheartj.oxfordjournals.org/ by guest on September 30, 2016
200%
171%
—
11 -4%
—
<30
n = 35
Exercise test
Repeat infarction
and/or
diuretics/digitalis
14-7%
8-8%
—
2 9%
—
>=30
n = 34
Guidelines for cardiac testing 979
Table 4 The Borg scale for rating of perceptual intensities constructed as a category scale with ratio properties can be used for quantitive evaluation of chest pain
Grade
Symptoms (chest pain)
0
0-5
1
2
3
4
5
6
7
8
9
10
Nothing at all
Extremely weak (just noticeable)
Very weak
Weak (light)
Moderate
Somewhat strong
Strong (heavy)
Very strong
Extremely strong (almost maximal)
Maximal
EVALUATION OF PATIENTS UNDERGOING PTCA OR CABG
Key points
In individual patients, exercise testing pre- and
post-PTCA/CABG can provide objective evidence for the
immediate or late success or failure of the procedure and
establish a baseline for any future evaluation'2930'.
In large cohorts of patients with CHD, which include a
wide spectrum of symptoms and evidence of ischaemia,
the results of exercise testing do not correlate closely with
either graft or arterial patency. In addressing this specific
question, it is recommended that radionuclide imaging
during exercise should be performed'31"33'.
While an early test provides information on the
immediate effect of the procedure, only after 6 months can
a more definite statement on success or failure be made,
when the opposing effects of restenosis and graft closure
and of rehabilitation are more stable.
Although theoretically valuable, it may not be possible
to stop anti-anginal medication before the intervention
and it is not always customary to do so thereafter.
Moreover, beta-blockers might be deemed desirable as
long-term secondary preventive agents in some countries.
Although exercise testing increases platelet aggregation
and coagulability, there is no evidence that an early test
enhances thrombus formation at the site of the PTCA.
Accepted indications
(1) Reassessment of recurrence of or deterioration in
symptoms.
(2) Routine evaluation pre- and post-intervention
(a) Early: 2-7 days after PTCA, 6 weeks after CABG;
(b) Late: 6 months after PTCA or CABG.
Possible indications
(1) Detection and evaluation of restenosis or graft
occlusion/stenosis;
(2) Annual routine evaluation.
Contra-indications
(1) Unstable angina pre- or post-intervention.
EVALUATION OF ANTI-ISCHAEMIC DRUGS IN SCIENTIFIC
STUDIES
Key points
Exercise testing is widely used to assess the antiischaemic effects of new drugs and to address new aspects
of therapy still relevant to established medications.
A profusion of methodology has grown from the
increasing demands of the pharmaceutical industry with
respect to the acquisition of objective data with which
to support new drug applications (NDAs) to the Drug
Regulatory Authorities.
The European Community will eventually have a
common policy towards new drugs allowing transfer of
licenses granted in one member country to all others. It is,
therefore, timely to establish in broad terms European
guidelines for those aspects of the clinical pharmacology
of anti-ischaemic drugs pertaining to exercise testing.
The aims of individual studies will vary but it is
recommended that all clinical trials adhere to the basic
principles of clinical pharmacology. Although placebocontrolled trials are of great scientific value, there may be
circumstances where this is inappropriate. Nevertheless, it
is important to emphasize that patients with stable angina
pectoris randomized to placebo do not generate more
adverse events than the active treatment groups and,
therefore, placebo-controlled trials in patients with a
stable pattern of symptoms should be considered quite
ethical.
In terms of analysis, the variables described for the
assessment of interventions (see 4 Key points) are
recommended.
But in clinical trials a more sophisticated method of
analysis is required.
Two approaches are recommended:
(1) The total exercise time is substituted for the time to
angina or 01 mV (1 mm) ST segment depression in
those who do not develop these manifestations. These
times are then said to be censored.
(2) Any measured variable that may develop during the
test (e.g. angina or 1 mm ST segment depression)
can be entered into a survival analysis in which
the proportion of patients free of that variable is
displayed at each time point. Censored values may be
added for those in whom the particular variable does
not occur; or the model may estimate from the total
data the likely time at which it would have appeared
had the test continued'34'.
Clearly these analyses are suited to the scientific
analysis of interventions, although, as clinical practice
comes under closer fiscal scrutiny, more objective
methods such as these might become necessary.
Heart failure
Introduction
It is usually only when cardiac dysfunction is far
advanced that the patient with heart failure develops
symptoms at rest. Thus, exercise testing can provoke
980 H. J. Dargie
symptoms which may be useful in improving the accuracy
of both diagnosis and prognosis in patients with lesser
degrees of cardiac dysfunction. In clinical practice,
however, exercise testing in heart failure patients is not yet
widely practised but is increasing. In providing valuable
information on functional capacity, exercise testing
potentially is of considerable value in assessing the
patients requirement for, and response to, a growing
number of interventions including drug therapy, valve
replacement, cardiac transplantation and rehabilitation
including exercise training.
EXERCISE TESTING IN PATIENTS WITH SYMPTOMS
SUGGESTIVE OF HEART FAILURE OF WITH KNOWN HEART
FAILURE
Key points
Exercise testing can reveal the true aetiology of the
symptoms in suspected heart failure. Breathlessness and
fatigue can be due to reversible ischaemia and be revealed
by ST segment changes during exercise. Exercise-induced
tachy- or brady-arrhythmias also may present with
breathlessness or fatigue. Patients may also be shown to
be limited by symptoms of conditions unrelated to heart
failure.
Exercise testing can be of considerable value in assessing the severity of heart failure, especially in patients who
restrict their activities as the disease progresses, since they
may not appreciate the severity of the reduction in their
functional capacity. Detecting symptoms at any early
stage of the disease allows progress to be monitored
and may aid the timing of pharmacological or surgical
interventions. The disparity between the patients'
symptoms and exercise performance is often striking.
Good ventricular function in the face of poor exercise
performance and marked symptoms needs careful evaluation before symptoms are ascribed to cardiovascular
disease.
Respiratory gas analysis can give further insights into
patients' symptoms. Respiratory frequency, ventilation,
oxygen consumption and carbon dioxide production are
all disturbed in heart failure. However, considerable skill
is required in the interpretation of individual results since
some patients hyperventilate during exercise, producing a
falsely low peak oxygen consumption. Moreover, there is
a grey area between those who are merely unfit and those
who have impaired exercise peformance and low peak
VO2 due to cardiac pathology. Even sophisticated
non-invasive exercise testing may be unable to distinguish
the two.
Oxygen uptake during exertion depends on the cardiac
output and the degree of desaturation of venous blood
returning to the lungs. Arterial oxygen saturation is
usually normal or only slightly depressed. During more
severe exertion venous desaturation is relatively fixed
and cardiac output becomes the main determinant of
oxygen consumption. Consequently measurement of
oxygen consumption is a valuable tool for measuring
cardiac reserve'18'.
Cardiac output is commonly preserved at rest until
ventricular dysfunction is far advanced. Assessing cardiac
output by VO2 during exercise is a more sensitive method
of stratifying degrees of ventricular dysfunction, may help
in the timing of cardiac transplantation'35' and other
interventions and be an aid to assessing prognosis'36-37'.
Sudden death is poorly predicted by exercise testing in
patients with moderate or severe heart failure'38'
although patients with heart failure who develop complex
ventricular arrhythmias during exercise are at increased
risk of sudden death'39'.
In patients with heart failure, regular exercise may
improve the haemodynamic response to exercise and
increase exercise performance, while reducing symptoms'40'41'. Formal exercise testing is an important part
of such management to document the safety of exercise
and in order to prescribe an appropriate amount of
exercise. Further evidence of the benefits of exercise
training and patient compliance is needed before wider
recommendations can be made.
Recommendations
Accepted indications
(1) Diagnosis of underlying cause (e.g. ischaemia,
exercise induced arrhythmias);
(2) Evaluation of symptoms in relation to exercise
capacity;
(3) Assessment of functional capacity;
(4) Assessing the need for and timing of cardiac
transplantation.
Possible indications
(1) Evaluation of prognosis;
(2) Determination and evaluation of exercise training
prescriptions.
Con tra-indications
(1) Recent acute pulmonary oedema;
(2) Heart failure due to aortic stenosis;
(3) Co-incident left main coronary artery stenosis and
heart failure;
(4) Acute myo-pericarditis.
EXERCISE TESTING IN THE ASSESSMENT OF DRUG THERAPY
Key points
Exercise testing is not performed routinely to evaluate
drug therapy in individual patients; assessment is usually
based on symptoms and signs.
Exercise testing provides objective evidence of
functional capacity and is used extensively in clinical trails
of new and established medications.
Recommendations
Accepted indications
(1) The scientific evaluation of new or established
medications by clinical trial.
Possible indications
(1) Clinical evaluation of drug therapy in individual
patients.
Guidelines for cardiac testing 981
Contra-indications
(1) Recent acute pulmonary oedema;
(2) Previous demonstration of exercise induced life
threatening arrhythmias;
(3) Co-incident left main coronary artery stenosis and
heart failure.
EVALUATION OF DRUG TREATMENT OF HEART FAILURE
In seeking to demonstrate the effect of any given
intervention on exercise capacity, there are a number of
important basic requirements.
Maximal test — ideal characteristics, (i) Duration should
average 9 min with a range of 3-12 min; (ii) Increments
should be small and occur every minute.
The use of severe protocols such as a 'fast' ramp on a
bicycle or the Bruce protocol on a treadmill will lead to the
test being terminated too quickly. Conversely, if the test
lasts for 15 min or more, boredom is a common reason
for stopping. Recently an exponential protocol has been
developed which may prove to be a useful compromise for
patients with CCF while also permitting comparison
between bicycle and treadmill modalities'2'1.
Objective assessments (i) Peak O2 consumption: in earlier
studies on healthy volunteers, a true maximum oxygen
Patient selection
consumption (VO2max) was defined as a plateau in VO2
(i) Underlying disease. This should be established as far despite an increment in workload. Since a plateau is not
as is possible, preferably by full invasive investigation in usually observed in heart failure patients, it is best to refer
the case of suspected CHD. Obstructive valve conditions to a symptom-limited peak achieved VO2 (PVO2) which is
and other structural abnormalities, such as congenital reproducible within subjects after familiarization, (ii) In
heart disease, are grounds for exclusion. Most patients order to demonstrate that the patient has been adequately
will have systolic dysfunction as evidenced by a left stressed, two or more of the following should be observed:
ventricular end-diastolic diameters > 5-5 and a fractional (1) A respiratory exchange ratio (VCO2/VO2) at peak
shortening <25% or left ventricular ejection fraction exercise of 10 or more, or an increase of 0-2 from the
<40%. Dominant diastolic dysfunction should consti- lowest value; (2) Peripheral venous lactate at peak exercise
tute a separate group and patients with hypertrophic at least double the resting value; (3) A biphasic VE/VO2
cardiomyopathy are usually excluded from studies of or VCO2 curve, or other respiratory evidence of an
heart failure.
anaerobic threshold, (iii) Consideration should be given
to alternative objective indices of exercise performance,
(ii) Symptoms. Despite the drawbacks, the NYHA classi- e.g. (1) Extrapolated maximal oxygen uptake; (2) The
fication remains a useful tool for selection of subjects for slope of ventilation/CCs production as a measure of lung
clinical trials. Thus patients should be in NYHA II-III, function; (3) O2 pulse (VO2/HR).
i.e. their symptoms should be potentially improvable.
During drug treatment, patients' symptoms are usually Reproducibility
more extensively explored by using quality-of-life quesExercise time in patients with heart failure can be
tionnaires or by using banks of visual analogue or Likert variable; up to 11 exercise tests were required in one study
scales1421.
before a reproducible test could be guaranteed'431. This
is generally impractical, and all exercise protocols may
(iii) Exercise tolerance. If exercise testing is to be used as a not suffer from a similar lack of reproducibility. The
primary end-point, then it is essential to demonstrate largest difference is between the first and second test
exercise intolerance. Weber has classified patients and due largely to patient familiarization with the exercise
41
according to their peak oxygen uptake and the maximum technique' . Only very frequent exercise testing (more
value acceptable in the context of heart failure is than three times per week) is likely to have a true training
25 ml. kg ' . min '. In practice, the great majority of effect. When using exercise duration as a baseline for
patients who fulfil the other entry criteria will have a peak observation over time or after intervention, three exercise
VO2of =$20ml. kg"'. min"' (women 5 ml. k g " ' . min"1 tests are generally required to minimize changes due to
less). In order to demonstrate the efficacy of a drug on familiarization.
the accepted clinical characteristics of effort-related
When used in conjunction with exercise protocols that
symptoms and limitation of exercise capacity, it is, by limit exercise duration to 5-7 min, peak minute oxygen
definition, necessary that patients fulfil these criteria.
consumption (VO2) appears highly reproducible,
In addition to measuring the efficacy of treatment, although at least one test run is advised. Peak VO2
exercise testing confirms the severity of disability, measured during exercise protocols that entail longer
classifies the patient in terms of severity of heart failure, periods are more variable. Peak achieved VO2 is greater
with high intensity protocols1'8-44-46'.
and helps to predict the prognosis.
Type of test
This may be maximal with increasing workloads. Less
commonly, exercise duration at a constant workload is
recorded. The amount of exercise performed in a limited
time can be measured.
Submaximal test
As patients rarely exercise to their maximum, submaximal tests may better reflect their everyday exercise
capacity. These may be conducted on a bicycle or treadmill at a stage approximating to 50% (PVO2 (i.e. below an
anaerobic threshold), and are usually of 10-15 min
982 H. J. Dargie
duration. Even simpler are tests which measure the distance the patient can walk in a 6-min period. The only
requirement for this test is a piece of straight level
ground of known length along which the patient may
walk uninterrupted. This test has been shown to be a
reliable measure of submaximal exercise capacity and is
clearly suited to those centres unable to carry out more
formal exercise testing.
Absence of gas measurements
In multi-centre studies, most centres will not have
access to, or be experienced in, the use of gas exchange
measurements. Provided the exercise test conforms to the
protocol guidelines stated, there is no reason to exclude
such centres from participation. Standardization of the
conduct of the test should be mandatory, e.g. extent of
patient encouragement, etc. This is facilitated by
technician training days prior to and during the study.
Clinical assessment of maximum effort
Employment of an experienced technician is probably
the best method of ensuring a maximal test or in assessing
its attainment. However, experience in the use of a Borg
scale (category ratio 0-5-10) should be encouraged since
in practised centres this correlates well with respiratory
variables.
Arrhythmias
Introduction
Exercise testing may identify an arrhythmic origin for
exercise-related complaints such as dizziness, syncope,
dyspnoea or palpitations and may also help in identifying the type, site of origin, initiating mechanism, and
aetiology in addition to assessing prognosis (risk
stratification) and results of treatment of arrhythmias.
A complete ECG recording of multiple channels
simultaneously is essential and monitoring for up to
lOmin after termination of exercise is recommended
because arrhythmias may also be provoked during the
recovery phase as a result of changes in autonomic tone.
The exercise test requires to be conducted in the presence
of well-trained personnel with optimal monitoring and
treatment facilities.
Recommendations
Accepted indications
(1) Diagnostic tool in patients with exercise-related
complaints of palpitations, dizziness or syncope.
(2) To evaluate effect of exercise in sustained or nonsustained supraventricular or ventricular tachycardia.
Not indicated
(1) Isolated uniform ventricular premature beats without
evidence of organic cardiac disease.
EXERCISE TESTING AND UNDERLYING MECHANISM OF
ARRHYTHMIAS
Key points
Exercise testing may give information on the initiating
and/or underlying mechanism of arrhythmias.
Initating mechanisms
In patients with exercise-related tachycardias, the mode
of onset can be documented by exercise testing, e.g. tachycardia initiated by exercise-induced supraventricular or
ventricular premature beats.
In the Wolff-Parkinson-White syndrome, anterograde
conduction through the accessory pathway may be
blocked at a critical sinus rate during exercise thereby
initiating circus movement tachycardia'521.
Underlying mechanisms
Ischaemia may be documented by recording STsegment changes before the onset of such arrhythmias.
Ischaemia-induced ventricular tachycardias are frequently polymorphic ventricular tachycardia (VT) or
ventricular fibrillation'531.
Exercise testing may document the influence of
autonomic tone in a variety of tachycardias including
atrial fibrillation, atrial flutter, atrial tachycardia and
incessant circus movement tachycardias using a slowly
retrogradely conducting accessory pathway'541. Also,
some forms of idiopathic ventricular tachycardia are not
only initiated by exercise but also show a marked increase
in rate during exercise.
Of limited help only in the sick sinus syndrome'461,
exercise testing can be of more value in assessing the site
of atrio-ventricular (AV) block'471. In AV nodal block,
AV-conduction will improve during exercise due to
increased sympathetic tone. In contrast, distal AV
conduction disturbances will worsen as more impulses
will traverse the AV node to reach the distal conduction
system during exercise.
EXERCISE TESTING AND THE DIAGNOSIS OF ARRHYTHMIAS
Key points
Exercise testing can provide an objective assessment,
not only of tachycardia, but also bradycardia due to sinus
node disease'461 or AV-block'471. Bundle branch block can
also be provoked'481.
In general, the inducibility of supraventricular or
ventricular tachycardias by exercise testing is relatively
low, with the exception of some forms of atrial tachycardia'491, idiopathic ventricular tachycardia'301, and that
due to right ventricular dysplasia'51'.
A ccepted indications
(1) Documentation of mode of onset and underlying
mechanisms of tachycardias.
(2) Assessment of role of autonomic nervous system.
(3) Localization of AV-block.
Possible indications
(1) Formes frustes of QT-prolongation syndrome.
(2) Sick sinus syndrome.
Guidelines for cardiac testing 983
Table 5 Methods available in nuclear cardiology using standard gamma camera equipment suitable for
stress testing
Perfusion scmtigraphy:
Acquisition1'-21
Perfusion agents'^51
Planar scintigraphy
Single photon emission computed tomography
(SPECT)
201 thallium
99m Tc 2 methoxy-isobutil-isonitrile (MIBI)
99m Tc teboroxime
Radionuclide ventriculography"1
first pass
equilibrium ventriculography
Stress modalities
exercise (bicycle or treadmill)1'1
atrial pacing171
dipyridamole'4-8'1
dobutamine'101
adenosine1"-12'
EXERCISE TESTING AND RISK STRATIFICATION
Key points
In patients exercised for suspected coronary artery
disease, induction of ventricular arrhythmias may
identify a subgroup with increased risk for future cardiac
events'55"571.
In the Wolff-Parkinson-White syndrome, patients
with a relatively long anterograde refractory period of
their accessory pathway will develop antegrade block in
the accessory pathway during exercise. This finding
identifies patients at low risk for high ventricular rates
and, therefore, ventricular fibrillation and sudden death
when atrial fibrillation occurs'581.
Induction of ventricular tachycardia by exercise has no
prognostic significance in patients with idiopathic ventricular tachycardia'501 and right ventricular dysplasia'51'.
Accepted indications
(1) Risk stratification in patients with coronary artery
disease.
(2) Risk stratification in the Wolff-Parkinson-White
syndrome.
EXERCISE TESTING TO EVALUATE EFFECT OF INTERVENTIONS
Key points
Currently, arrhythmias are treated with drugs, different
forms of catheter ablation, antitachycardia pacemakers,
automatic implantable defibrillators and by a variety of
surgical procedures. The use of exercise testing for
assessing effectiveness of treatment strongly depends on
the reproducibility of arrhythmias induction by this
technique.
Available data suggest clinically useful reproducibility
for different forms of ventricular ectopic activity'59'601
including sustained or recurrent non-sustained ventricular
tachycardia'6".
If an ischaemic component can be identified, the effect
of anti-ischaemic drug treatment, coronary angioplasty
and coronary bypass grafting can be assessed.
Persistence of exercise-induced ventricular arrhythmias
following bypass surgery has not been found to be related
to an increased risk of cardiac death'55621.
In non-ischaemic exercise-related VT, the effect of
beta-blockade, frequently combined with Class I or
Class III drugs'631 can be evaluated, as can the effect of
verapamil'531.
In malignant ventricular arrhythmias, previous
(uncontrolled) studies'641 suggest that suppression of
Lown grade 4B and 5 arrhythmias during exercise testing
and on 24 h monitoring, leads to reduction in mortality.
Based on these findings, treatment protocols have been
advised'65661. Recent data from the CAST study, however,
have shown that suppression of ventricular ectopy by
certain antiarrhythmic drugs does not equate with
prevention of cardiac death'671.
Another possible indication for exercise testing is the
evaluation of pro-arrhythmia. In patients developing
Torsades de Pointe with Class la drugs, the QT interval
during exercise may lengthen1681.
In patients using Class lc drugs, widening of the QRScomplex may occur favouring re-entry and induction of
ventricular tachycardia'47691.
Accepted indications
(1) Evaluation of treatment on exercise related supraventricular tachycardias.
(2) Evaluation of treatment on exercise related ventricular
tachycardias.
Possible indications
(1) Reduction in mortality by antiarrhythmic treatment
of exercise-related ventricular arrhythmias.
(2) Identification of patients at risk for pro-arrhythmia
with Class la and lc drugs.
Nuclear cardiology
Nuclear cardiology comprises a large array of methods
(Table 5), some of which, like single photon emission
computed tomography*70"71' and the technetium 99mbased perfusion agents'72"761, have only recently been
applied in clinical practice.
984 H. J. Dargie
Broadly speaking, in the setting of stress testing,
nuclear cardiology includes two major categories of techniques1761: radionuclide ventriculography and myocardial
perfusion scintigraphy. Both provide useful and complementary information on ventricular function (global and
regional) and myocardial perfusion.
Compared to 201 thallium, an important potential
advantage of 99m TcMIBI is that a combined study on
function (first pass) and pefusion is feasible after the same
injection of the radiotracer'751.
Positron emission tomography (PET) is a more
sophisticated and expensive tool for the diagnosis of
coronary artery disease, based on the evaluation of
regional myocardial blood flow with myocardial perfusion tracers. However, due to its high costs and since its
putative advantages are still unproven compared to the
newest methods with the standard gamma cameras and
the 99m Tc perfusion agents, it is not yet recommended
for routine clinical use'77'. Therefore, the following
recommendations will apply to the standard gamma
camera imaging.
Thallium 201 scintigraphy and radionuclide ventriculography during stress have been proven to be superior to
exercise electrocardiography alone for all their potential
clinical uses (differential diagnosis of chest pain, assessing
the functional significance of coronary disease, assessing
the results of PTCA or CABG)'78"8'1 and evaluating
prognosis.
However, for cost considerations, the indications for
nuclear cardiological studies must be stratified according
to the benefits in the individual patient.
The selection of study modality (perfusion or myocardial function study, exercise vs non-exercise stress)
will depend on the individual clinical problem and the
different experience of the individual laboratory with
the different techniques. It is, however, important to
remember that, according to several studies, the results
of pharmacological stress testing are comparable to conventional exercise, for the diagnosis of coronary
disease1731.
A ccepted indications
(1) Diagnosis of coronary artery disease in patients
with equivocal ECG exercise test, or resting ECG
abnormality;
(2) Diagnosis of coronary artery disease in patients with
chest pain and normal ECG exercise test;
(3) For assessing the function significance of 'borderline'
coronary stenoses in patients considered for PTCA or
CABG.
Possible indications
(1) Risk stratification in patients after myocardial
infarction;
(2) Assessment of re-stenosis 3-6 months after PTCA or
CABG;
(3) Risk assessment of patients for major noncardiac vascular surgery (dipyridamole 201 thallium
scintigraphy);
(4) Assessment of the presence and severity of functional
abnormalities in patients with silent 'ischaemia' on
ECG exercise stress;
(5) In patients with poor ventricular function, to
decide between coronary revascularization of heart
transplantation, based on the amount of viable
ischaemic myocardium;
(6) Assessment of the presence of functional abnormalities (ventricular function and/or perfusion) in patients
after heart transplantation;
(7) Differential diagnosis between ischaemic and
congestive cardiomyopathy;
(8) Follow-up and management of patients with
aortic and/or mitral regurgitation (radionuclide
ventriculography).
Contra- indications
(1) All the usual contra-indications to ECG exercise
testing;
(2) When the clinical information together with exercise
testing provides the answer to the clinical problem.
Regulatory aspects
Introduction
Regulation of the aviation environment is agreed by
international statute and is laid down by the International
Civil Aviation Organisation (ICAO) in Montreal'821.
Requirements are minimum standards and an individual
nation may apply a more, but not less, rigorous standard.
Any departure has to be filed with ICAO. The European
nations have come together to contribute to the European
Civil Aviation conference and evolve common standards
for all regulatory aspects of aviation in the continent. In
1992, these are in the process of agreement'83-84', although
the Joint Airworthiness Authority, as it will become, will
not assume full authority until 1996.
In contrast, there are no internationally agreed
standards in relation to cardiovascular fitness to drive,
although reciprocity agreements exist between many
countries. The European states have adopted differing
approaches towards regulation and different attitudes
with regard to certain aspects of road transport safety.
Due to greater exposure, vocational drivers, like pilots,
deserve closer scrutiny than other road users. But they
also depend on driving for their livelihood, and it is
encumberent upon both legislators and cardiological
advisers to be fair and even in the standard of fitness they
require.
Key points
On a kilometre for kilometre basis, passenger air
transportation is significantly safer than travel by road in
many parts of the world. In the past 3 years, over one
billion passengers have been carried in 15 000 aircraft over
16 million flying hours, flown by 160 000 professional
aircrew. Eighty percent of all aviation accidents are
Guidelines for cardiac testing
due to human factors, which include degradation of
performance by illness, and 20% of the 1000-2000 lives
lost each year in fatal aircraft accidents are due to
sabotage or warfare.
Death at the wheel is rare and has been thought to be
causal in 6/10000'85' road accidents while other sudden
illness-related events occur at a rate between 1/1000 and
1/4000'86-871. It can be calculated that, for a 40 h week,
one accident attributable to myocardial infarction would
occur every 10 million hours driven. Thus, such events are
remarkably rare and it should be recognized that the
ability of medical screening perceptibly to reduce the
overall accident rate is limited.
It is sometimes claimed that there is a divarication
between the problems of medical certification to fly and
to drive. This is because there is a perception that air
transport operations necessarily carry at least two crew
whereas road transport operations invariably involve
only one driver. This is not true: the smaller helicopters on
public transport flights together with the smallest air-taxi
aircraft (i.e. non-turbine aircraft) may be flown under
public transport rules with a single crew-member only.
A man aged 65 years in the U.K. has approximately 1 %
chance of dying of cardiovascular cause each year, an
event rate which approximates to 1 per 106 h[88891. Some of
these deaths will be sudden but presumably the level of
associated risk is acceptable to the licensing authorities.
The greatest number of these cardiovascular events will
occur in that part of the population without known
cardiological problems because the greatest part of the
population falls into that group.
The issue of certification to fly following myocardial
infarction, percutaneous transluminal coronary angioplasty and coronary artery bypass grafting was discussed
extensively at the First'901, the Second19'1 UK Workshops
and the First1921 European Workshop in Aviation
Cardiology. Other authorities have also reviewed the
problem193"951. It has been stated that the industry target
for scheduled jet aircraft transportation world wide was
one fatal accident in every 107flyinghours. This has not
yet been achieved and the figure remains at or around one
such accident every 106 flying hours. It has further been
stated that accidents should not be due to medical cause
more often than 1 in every 100. This implies a multi-crew
target accident rate of I in 108-l in 109flyinghours. There
has been one such fatal flying accident in the past 300
million flying hours.
For single-crew operations in which a fatal outcome is
almost inevitable following total incapacitiation of the
pilot, the situation is necessarily different. The observed
accident rate in single-crew professional operations is of
the order of 1 such accident every 105flyinghours. If 1 in
100 of these is due to medical incapacitation, then the
implication is that a medical cause accident should not
occur more often than 1 in 107 flying hours and by
extrapolation from the paragraph above, this is approximately the cardiovascular mortality of a 45-year-old male
in the U.K.
From these data, the various Workshops recommended that the acceptable probability of a major
985
incapacitating event (not all of which would cause
accidents) should not exceed 1 % per annum for the above
targets to have some reasonable hope of being achieved,
corresponding to 1 event in every 1 million hours, making
certain assumptions. This target event rate is likely to be
accepted by the Joint Airworthiness Authority (JAA).
The prognosis of ischaemic heart disease presenting as
angina pectoris'961 following myocardial infarction'97981
has received much attention. Although the use of exercise
electrocardiography in the 1970s interest focused on the
prediction of the extent and severity of coronary artery
disease'991 and of outcome both in myocardial infarction'1001 and following coronary artery surgery'10'1, it
became clear that careful risk classification using, inter
alia, exercise electrocardiography could identify good risk
subjects amongst patients with known coronary artery
disease, the most favourably placed of whom should
be capable of fulfilling European requirements for
certification to drive or to fly'99"'071.
Exercise electrocardiography for certificatory purposes
To maintain an even standard, it is necessary that a
protocol be recommended which takes into account
somatic differences between subjects. If more than one
protocol is to be recommended (treadmill/bicycle), a
statement on equivalents is required.
Of greatest interest to a certificatory authority is not the
extent of coronary artery disease but its likely outcome.
This is also of interest to the individual patient. More data
are needed on the prediction of probability of event using
standard exercise protocols.
Licensing authorities have to be prepared to accept that
screening will not remove all at risk, but the hope is that
the system will identify those at lowest risk within certain
confidence intervals. Although the certificatory requirements lean heavily on the predictive power of the exercise
electrocardiogram standing alone, simple algorithms may
need to be identified to enhance its predictive accuracy.
The certificatory authorities have identified exercise
electrocardiography as a simple and useful technique to
help identify patients at risk of known or suspected coronary artery disease with lowest risk of event. Guidance
from the ESC Taskforce in Exercise Electrocardiography
with regard to protocols and probability analysis is
needed.
Recommendations
EXERCISE TESTING IN VOCATIONAL DRIVING LICENCE
HOLDERS AND AIRCREW
Accepted indications
(1) Assessment of those with suspected episodes of
myocardial ischaemia;
(2) Evaluation of subjects with chest pain of uncertain
aetiology;
(3) Risk stratification of, and assessing exercise tolerance in, subjects after acute myocardial infarction,
coronary artery bypass surgery and angioplasty.
986
H. J. Dargie
CRITERIA FOR A NORMAL RESPONSE
Those with symptoms
In such cases, a symptom-limited exercise electrocardiogram test should be carried out on a treadmill
(Bruce protocol) or an equivalent using a bicycle
ergometer. Vocational driving should not be permitted
if the subject cannot complete Bruce Stage III (i.e. a
workload of 8-10 METS), reach 180 W (adjusted for
body surface area) of the 20 W protocol or achieve the
maximum heart rate predicted for his (her) age without
evidence of myocardial ischaemia. If an exercise electrocardiogram cannot be performed or if the response is
masked by therapy, it is for the judgement of the cardiologist whether further investigation is necessary,
including discontinuation of anti-anginal therapy prior to
repetition of the test.
If certain ECG abnormalities pre-exist or develop
during exercise:
These ECG abnormalities include: left bundle branch
block; non-specific ST/T changes; complete or second
degree atrioventricular block; paroxysmal arrhythmias,
whether supraventricular or ventricular; ventricular
premature beats occurring singly, as couplets, or as runs.
Such disturbances do not necessarily constitute a
reason for revoking a licence provided that there is no
constitutional disturbance and the heart is demonstrably
normal. Runs of monomorphic ventricular tachycardia, if
they occur, must not exceed 30 s in duration and not be
associated with demonstrable abnormality of the heart.
Patients should be able to complete Stage IV of the Bruce
protocol with a normal ECG blood pressure and heart
rate response.
References
[1] Lollgen H, Ulmer HV, Crean P, eds. Recommendations and
standard guidelines for exercise testing: a report of the task
force conference on ergometry. Eur Heart J 1988;9(Suppl K):
3-37.
[2] Guidelines for exercise testing: a report of the American
College of Cardiology/American Heart Association task
force on assessment of cardiovascular procedures. J Am Coll
Cardiol 1986; 8: 725-38.
[3] Exercise standards: a statement for health professionals from
the American Heart Association. AHA Medical-Scientific
Statement: Special Report. Circulation 1990; 82: 2286-322.
[4] Cleland JGF, Stirling KW, Henderson E, Dargie HJ.
Symptom limited exercise and respiratory gas exchange in
heart failure. Br Heart J 1986; 55: 519.
[5] Ellestad MH. Memorial hospital protocol. In: Ellestad MH,
ed. Stress testing, principles and practice. Philadelphia,
Pennsylvania: Davis, 1975:67-84.
[6] Mason RE, Likar I, Biern RO, Ross RS. Multiple-lead
exercise electrocardiography. Experience in 107 normal subjects and 67 patients with angina pectoris, and comparison
with coronary cinearteriography in 84 patients. Circulation
1967; 36: 517-25.
[7] Chaitman BR, Bourassa MG, Wagniart P, Corbara F,
Ferguson RJ. Improved efficiency of treadmill exercise testing
using a mutliple lead ECG system and basic hemodynamic
exercise response. Circulation 1978; 57: 71-9.
[8] Fox K, Selwyn A, Shillingford J. Precordial electrocardiographic mapping after exercise in the diagnosis of coronary
artery disease. Am J Cardiol 1979; 43: 541 6
[9] Foelicher VF. Exercise and the heart, clinical concepts. Year
Book 1987. Medical Publishers Inc.
[10] Astrand P-O, Rodahl K. Textbook of work physiology.
Physiological bases of exercise, 3rd edn, McGraw-Hill, 1986.
[11] Grant S, Crawford J, Gilmour H, Henderson E, Dargie HJ.
Comparison of treadmill and bicycle oxygen costs. Am J
Nonlnvas Cardiol 1992; 6: 173-6.
[12] Astrom H, Jonsson B. Design of exercise test with special
reference to heart patients. Br Heart J 1976, 38: 289-96.
[13] Myers J, Froelicher VF. Optimizing the exercise test for
pharmacological investigations. Circulation 1990, 802:
[14] Scherer D, Kaltenbach M. Haufigkeit lebensbedrohlicher
KomplikationenbeiergometrischenBelastrungsuntersuchungen.
Z Kardiol 1979; 68: 240.
[15] Brasseur LA, Mairiaux PH, Kandouci AB, Detry JM.
Respiratory and metabolic parameters during submaximal
and maximal exercise in normal men. In: Rulli V, Messin R,
Denolin H, eds. Normal values in adult ergometry according to age, sex and training. Torino: Eur Soc Cardiol,
Schiapparelli Farmaceutici Ed, 1983: 3-14.
[16] Guyatt GH, Sullivan MJ, Thompson PJ et ai. The 6-minute
walk: a new measure of exercise capacity in patients with
chronic heart failure. Can Med Assoc J 1985; 132: 919-23.
[17] Riley M, McParland T, Stamford CF, Nicholls DP. Oxygen
consumption during corridor walk testing in chronic cardiac
failure. Eur Heart J 1992; 13: 789-93.
[18] Lipkin DP, Canepa-Anson R, Stephens MR, Poole-Wilson
PA. Factors determining symptoms in heart failure: comparison of fast and slow exercise tests. Br Heart J 1986; 55:
439-45.
[19] Buchfuhrer MJ, Hansen JE, Robinson TE, Sue DY,
Wasserman K, Whipp BJ. Optimizing the exercise protocol
for cardiopulmonary assessment. J Appl Physiol 1983; 55:
1558-64.
[20] McLenachan JM, Weidinger FF, Barry J et al. Relations
between heart rate, ischaemia and drug therapy during daily
life in patients with coronary artery disease. Circulation 1991;
83: 1263-70.
[21] Northridge DB, Grant S, Henderson E, Ray S, McMurray J,
Dargie HJ. A novel exercise protocol suitable for use on a
treadmill or a bicycle ergometer. Br Heart J 1990; 64: 313-6.
[22] Diamond GA, Forrester JS, Hirsch M el al. Application of
conditional probability analysis to the clinical diagnosis of
coronary artery disease. J Clin Invest 1980; 65: 1210-21.
[23] Selzer A, Cohn K, Goldschlager N. On the interpretation of
the exercise test. Circulation 1978; 58: 193-95.
[24] Detrano R, Froelicher VF. Exercise testing, uses and
limitations considering recent studies, prog Cardiovasc Dis
1988; 31: 173-204.
[25] Deckers JW. Diagnostic and prognostic implications of
exercise testing in coronary artery disease. Thesis, Rotterdam
1988.
[26] Simoons ML. Exercise electrocardiography and exercise
testing. In: Macfarlane PW, Lawrie TDV, eds, Comprehensive electrocardiology. Section 8 (Specialized aspects of
electrocardiology). Pergamon Press, 1988.
[27] Fioretti P, Brower RW, Simoons ML et al. Prediction of
mortality during the first year after acute myocardial infarction from clinical variables and stress test at hospital
discharge. Am J Cardiol 1985; 55: 1313-18.
[28] Arnold AER, Simoons ML, Detry J-MR et al. for the
European Co-operative Study Group. Prediction of mortality
after hospital discharge in patients treated with and without
recombinant tissue plasminogen activator for myocardial
infarction: is there a need for coronary angiography? In:
Benefits and Risks of Thrombolysis for Acute Myocardial
Infarction. Rotterdam: AER Arnold, 1990: 135-53.
[29] Mulcahy D, Keegan J, Phadke K et al. Effects of coronary
artery bypass surgery and angioplasty on the total ischemic
burden, a study of exercise testing and ambulatory ST segment
monitoring. Am Heart J 1992; 123: 597 603.
Guidelines for cardiac testing 987
[30] Dubach P, Froelicher V, Klein J, Detrano R. Use of the
exercise test to predict prognosis after coronary artery, bypass
grafting. Am J Cardiol 1989; 63: 530-3.
[31] Honan MB, Bengtson JR, Pryor DB el al. Exercise treadmill
testing is a poor predictor of anatomic restenosis after angioplasty for acute myocardial infarction. Circulation 1989; 80:
1585-94.
[32] Bengston JR, Mark DB, Honan MB el al. Detection of
restenosis after elective percutaneous transluminal coronary
angioplasty using the exercise treadmill test. Am J Cardiol
1990; 65: 28-34.
[33] Dubach P, Lehmann KG, Froelicher VF. Comparison of
exercise test responses before and after either percutaneous
tranluminal coronary angioplasty or coronary artery bypass
grafting. Am J Cardiol 1989; 64: 1039-41.
[34] France LA, Lewis JA, Kav R. Statistics in Medicine 1991; 10:
1099-115.
[35] Mancini DM, Eisen H, Kussmaul W, Mull R, Edmunds LH,
Wilson JR. Value of peak exercise oxygen consumption of
optimal timing of cardiac transplantation in ambulatory
patients with heart failure. Circulation 1991; 83: 778-86.
[36] Szlachic J, Massie BM, Kramer BL, Topic N, Tubau J.
Correlates and prognostic implication of exercise capacity
in chronic congestive heart failure. Am J Cardiol 1985; 50:
1037^*2.
[37] Cleland JGF, Dargie HJ, Ford I. Mortality in heart failure:
clinical variables of prognostic value. Br Heart J 1987; 58:
572-82.
[38] Gradman A, Deedwania P, Cody R et al. Predictors of total
mortality and sudden death in mild to moderate heart failure. J
Am Coll Cardiol 1989; 14: 564-70.
[39] Cleland JGF, Dargie HJ. Ventricular arrhythmias during
exercise in patients with heart failure' the effect of amiodarone
Eur Heart J (Suppl D) 1987, 8: 65-9.
[40] Sullivan MH, Higginbotham MB, CobbFR. Exercise training
in patients with severe left ventricular dysfunction. Circulation
1988; 78: 506-15.
[41] Coats AJS, Adamopoulos S, Meyer TE, Conway J, Sleight P.
Effects of physical training in chronic heart failure Lancet
1990; 335: 63-6.
[42] Rector TS, Spencer HE, Cohn JN. Patients self-assessment of
their congestive heart failure. Part 2: Content, reliability and
validity of a new measure, The Minnesota Living with Heart
Failure Questionnaire. Heart Failure October/November
1987; p. 198-209.
[43] Pinsky DJ, Ahem D, Wilson PB, Kukin ML, Packer M. How
many exercise tests are needed to minimize the placebo effect of
serial testing in patients with chronic heart failure? Circulation
1989; 80 (Suppl II): 11-426 (Abstr).
[44] Elborn JS, Standford CF, Nicholls DP. Reproducibility of
cardio-pulmonary parameters during exercise in patients with
chronic cardiac failure: the need for a preliminary test. Eur
Heart J 1990; 11:75-81.
[45] Cleland JGF, Henderson E, McLenachan J, Findlay IN,
Dargie HJ. Effect of captopril, an angiotensin-converting
enzyme inhibitor, in patients with angina pectoris and heart
failure. J Am Coll Cardiol 1991; 17: 733-9.
[46] Valin HD, Edhag KD. Heart rate responses in patients
with sinus node disease compared to controls: Physiological
implications and diagnostic possiblities. Clin Cardiol 1980;
391-8.
[47] Podrid PJ, Venmditti FJ, Levine PA, Klein MD. The role of
• exercise testing in evaluation of arrhythmias. Am J Cardiol
1988;62:24H-33H.
[48] Vasey C, O'Donnell J, Morris S, McHenry P. Exercise induced
left bundle branch block and its relation with coronary artery
disease. Am J Cardiol 1985; 56: 892-5.
[49] Gilette PC, Crawford FC, Zeigler VL. Mechanisms of atrial
tachycardias. In: Zipes, Jalife, eds. Cardiac electrophysiology.
Philadelphia: W. B. Saunders, 1990: 559-663.
[50] Lemery R, Brugada P, Delia Bella P, Dugernier T, Van den
Dool A, Wellens HJJ. Non-ischemic ventricular tachycardia:
clinical course and long-term follow-up in patients without
clinicially overt heart disease. Circulation 1989; 79: 990-9.
[51] Lemery R, Brugada P, Janssen J, Cheriex E, Dugernier T,
Wellens HJJ. Non-ischemic sustained ventricular tachycardia:
clinical outcome in 12 patients with arrhythmogenic right
ventricular dysplasia. J Am Coll Cardiol 1989; 14: 96-105.
[52] Wellens HJJ, Brugada P, Penn OC, Gorgels APM, Smeets
JLRM. Pre-excitation syndromes. In: Zipes, Jalife, eds.
Cardiac electrophysiology. Philadelphia: W. B. Saunders,
1990:691-702.
[53] Sung RJ, Huycke EC, Wen Ter-Lai et al. Clinical and electrophysiologic mechanisms of exercise induced ventricular
tachyarrhythmias. Pace 1988; 11: 1347-57.
[54] Gorgels APM, Brugada P, Wellens HJJ. When to treat
arrhythmias in heart failure. In: Brachmann J, Dietz R, Kubler
W, eds. Heart failure and arrhythmias 1990. Berlin: Springer
Verlag, 1990: 100-10.
[55] Weinter DA, Levine SR, Klein MD, Ryan TJ. Ventricular
arrhythmias during exercise testing: mechanism, response to
coronary bypass surgery and prognostic significance. Am J
Cardiol 1984; 53: 1553-7.
[56] Marieb MA, Beller GA, Gibson RS et al. Clinical relevance
of exercise-induced ventricular arrhythmias in suspected
coronary artery disease. Am J Cardiol 1990; 66: 172-8.
[57] O'Hara GE, Brugada P, Rodriquez LM et al. High incidence
of sudden death in patients with exercise-induced ventricular
tachyarrhythmias and old myocardial infarction. Circulation
1989; 80:11-654
[58] Levy S, Bronstet JP, Clemency J. Syndrome de WolffParkinson-White. Correlations entre l'exploration electrophysiologique et reflect de l'epreuve de l'effort sur l'aspect
electrocardiographique de preexcitation. Arch Mai Coeur
1979; 72: 634-43.
[59] Sami M, Kraemer H, Debusk RF. Reproducibility of exercise
induced ventricular arrhythmias after myocardial infarction.
Am J Cardiol 1979; 43: 724-30.
[60] Saini V, Graboys TB, Towne V, Lown B. Reproducibility of
exercise induced ventricular arrhythmia in patients undergoing evaluation for malignant ventricular arrhythmia. Am J
Cardiol 1989; 63: 697-701.
[61 ] Woelfel A, Foster JR, Simpson RJ, Gettes LS. Reproducibility
and treatment of exercise induced ventricular tachycardia. Am
J Cardiol 1984; 53: 751-6.
[62] Yli-Mayry S, Huikuri HV, Korhonen UR et al. Prevalence
and prognostic significance of exercise-induced ventricular
arrhythmias after coronary artery bypass grafting. Am J
Cardiol 1990; 66: 1451^1.
[63] Cleland JGF, Dargie HJ. Ventricular arrhythmias during
exercise in patients with heart failure: the effect of amiodarone.
Eur Heart J 1987; 8 (Suppl D): 65-70.
[64] Graboys TB, Lown B, Podrid P, DeSilva R. Long-term
survival of patients with malignant ventricular arrhythmias
treated with antiarrhythmic drugs. Am J Cardiol 1982; 50:
437-43.
[65] Podrid PJ. Treatment of ventricular arrhythmia. Chest 1985;
o o . 1Z1—o.
[66] Bayes de Luna A, Guindo J, Tomer P et al. Value of
effort testing and acute drug testing in the evaluation of
antiarrhythmic treatment. Eur Heart J 1987; 8 (Suppl A):
77-82.
[67] Echt DS, Liebson PR, Mitchell LB et al. Mortality and
morbidity in patients receiving encainide, flecainide or
placebo. N Engl J Med 1991; 324: 781-8.
[68] Kadish AH, Weisman HF, Veltri EP el al. Paradoxical effects
of exercise on the QT interval in patients with polymorphic
ventricular tachycardia receiving Type la anti-arrhythmic
agents. Circulation 1990; 81: 14-19.
[69] Ranger S, Talajic M, Lemely R, Roy D, Nattel S. Amplification of flecainide-induced ventricular conduction slowing by
exercise. Circulation 1989; 79: 1000-6.
[70] Fintel DJ, Links IM, Frank TL et al. Improved diagnostic
performance of exercise Thallium-201 single photon emission
computed tomography over planar imaging in the diagnosis of
988 H. J. Dargie
coronary artery disease: a receiver operating characteristic
analysis. J Am Coll Cardiol 1989; 13: 600-12.
[71] Diamond GA. How accurate is SPECT Thallium
scintigraphy?J Am Coll Cardiol 1990; 16: 1017-21.
[72] Kahn JK, McGhie I, Akers MS et al. Quantitative rotational
tomography with 201 TI and 99m Tc 2-methoxy-isobutyllsonitrile: a direct comparison in normal individuals and
patients with coronary artery disease. Circulation 1989; 79:
1282-93.
[73] Kettunen R, Huikuri HV, Heikkila J Takkunen JT. Usefulness
of Technetium-99m-MIBI and Thallium-201 in tomographic
imaging combined with high-dose dipyndamole and handgrip
exercise for detecting coronary artery disease. Am J Cardiol
1991; 68: 575-9.
[74] Fleming RM, Kirkceide RL, Taegtmeyer H et al. Comparison
of technetium-99m Teboroxime tomography with automated
quantitative coronary arteriography and Thallium-201
tomographic imaging. J Am Coll Cardiol 1991; 17: 1297-1302.
[75] Baillet GY, Mena 1G, Kuperus JH et al. Simlutaneous
technetium 99m MIBI angiography and myocardial perfusion
imaging. J Nucl Med 1989; 30: 38-44
[76] O'Rourke RA, Chattergee K, Dodge HT et al. Guidelines for
clinical use of cardiac radio-nuclide imaging, December 1986.
A Report of the American College of Cardiology/American
Heart Association Task Force on Assessment of Cardiovascular procedures (Sub-committee on Nuclear Imaging). J
Am Coll Cardiol 1986; 8. 1471-83.
[77] Bonow RO, Berman DS, Gibbons RJ et al. Cardiac position
emission tomography. A report for health professionals from
the committee on advanced cardiac imaging and technology
of the Council on Clinical Cardiology, American Heart
Association. Circulation 1991; 84: 447-54.
[78] Beller GA, Gibson RS. Sensitivity, specificity and prognostic
significance of non-invasive testing for occult or known
coronary disease. Progr Cardiovasc Dis 1987; 29:241-70.
[79] Hung J, Chaitman BR, Lam J et al. Noninvasive diagnostic
test choices for the evaluation of coronary artery disease in
women: a multivariate comparison of cardiac fluoroscopy,
exercise electrocardiography and exercise thallium myocardial
perfusion scintigraphy. J Am Coll Cardiol 1984; 4: 8-16.
[80] Heinsimer JA, Witt CM de. Exercise testing in women. J Am
Coll Cardiol 1989; 14: 1448-9.
[81] Puey EG de, Guertier-Krawczynska E, Robbins WL.
Thallium-201 SPECT in coronary artery disease patients with
left bundle branch block. J Nucl Med 1988; 29: 1479-85.
[82] Personnel licensing. International standards and recommended
practices. Annex I to the Convention in International Civil
Aviation. Montreal. ICAO. 1985.
[83] Chapter 2. Class I Medical Assessment FCLSubgroup(Medical)
3 — SD Appendix 2, pp. 7-9 ECAC-CEAC Neuilly-sur-Seine
1990.
[84] Joy M. Cardiovascular Standards. In: European Manual of
Civil Aviation Medicine ECAC-CEAC Neuilly-sur-Seine: in
press.
[85] Baker SP, Spitz WU. An evaluation of the hazard created by
natural death at the wheel. N Engl J Med 1970; 283:405-9.
[86] Herner B, Smedley B, Ysander L. Sudden illness as a cause of
motor vehicle accidents. Br J Industr Med 1966; 23: 37-41.
[87] Gratten E, Jeffcoate GO. Medical factors in road traffic
accidents. Br Med J 1968; i: 75-9.
[88] Tunstall-Pedoe H. Acceptable cardiovascular risk in aircrew.
Eur Heart J 1988; 9 (Suppl G): 9-11.
[89] Tunstall-Pedoe H. The concept of risk. Eur Heart J 1988; 9
(Suppl G): 12-15.
[90] The First UK Workshop in Aviation Cardiology. Joy M,
Bennett G, eds. Eur Heart J 1984; 5 (Suppl A): 1-79.
[91] The Second UK Workshop in Aviation Cardiology. Joy M,
Bennett G, eds. Eur Heart J 1988; 9 (Suppl G): 1-179.
[92] The First European Workshop in Aviation Cardiology. Joy
M.ed. Eur Heart J 1992; 13 (Suppl H): 1-175.
[93] Vohra J, Plowright R. An appraisal of cardiovascular
standards for Australian civilianflyinglicences. Aus NZ J Med
1989; 19:76-82.
[94] Guidelines for the assessment of cardiovascular fitness in
Canadian pilots, 1988. Health Advisory Services: Ottowa,
Department of National Health and Welfare, 1988.
[95] Engelberg AL, Gibbons HL, Doege TC. A review of the
medical standards of civilian airmen. Synopsis of a two year
study. JAMA 1986; 255: 1589-99.
[96] Sigler LH. Prognosis of angina pectoris and coronary
occlusion: follow up of 1700 cases. JAMA 1951; 146:
998-1008.
[97] Re) S, D'Alonzo CH. Immediate mortality and 5 year survival
of employed men with first myocardial infarction. N Engl J
Med 1964; 270: 915-22.
[98] Harris PJ, Howell FE Jr, Lee KL et al. Survival in medically
treated coronary artery disease. Circulation 1979; 60: 1259-69.
[99] Goldschlager N, Seltzer A, Lohn K. Treadmill stress tests
as indicators of the presence and severity of coronary artery
disease. Am Ann Med 1976; 85: 277-86.
[100] Stone PH, Turi ZG, Muller JE et at. Prognostic significance of
the treadmill exercise performance 6 months after myocardial
infarction. JACC 1986; 8: 1007-17.
[101] DeBusk RF, Blomqvist G, Kouchoukos NT el al. Identification and treatment of low risk patients after acute myocardial infarction and coronary artery bypass graft surgery.
New Eng J Med 1986; 314: 161-66.
[102] McNeer FJ, Margolis JR, Lee KL et al. The role of the exercise
test in the evaluation of patients for ischaemic heart disease.
Circulation 1978; 57: 64-70.
[103] Gohike H, Samek L, Betz P, Roskamm H. Exercise testing
provides additional prognostic information in angiographically defined sub-groups of patients with coronary artery
disease. Circulation 1983; 68: 979-85.
[104] Mock MB, Rinqvist I, Fisher LD et al. Survival of medically
treated patients in the Coronary Artery Surgery Study (CASS)
Registry. Circulation 1982; 66: 562-68.
[105] Bruschke AVG, Proudfit WL, Stones FM. Progress study of
590 consecutive non-surgical cases of coronary artery disease
followed 5-9 years. I. arteriographic correlations. Circulation
1973; 47: 1147-53.
[106] Chaitman BR, Davis KB, Dodge HT et al. Should airline
pilots be eligible to resume active flight status after coronary
bypass surgery?: A CASS Registry Study. J Am Coll Cardiol
1986; 8: 1318-24.
[107] Luwaert RJ, Mellin JA, Brohet CR et al. Non-invasive data
provide independent prognostic information in patients
without previous myocardial infarction: findings in male
patients who have had cardiac catheterisation. Eur Heart J
1988; 9: 418-36.
Appendix I
CONTRIBUTORS
The following members of the Working Group on
Exercise Physiology, Physiopathology and Electrocardiography contributed to the Guidelines: H. Astrom,
Stockholm, Sweden; R. A. Binkhorst, Nijmegen, The
Netherlands; J. P. Broustet, Pessac, France; B. Caru,
Tradate, Italy; J. G. F. Cleland, London, U.K.; D. V.
Cokkinos, Athens, Greece; H. J. Dargie, Glasgow, U.K.;
M. De Kock, Brussels, Belgium; J.-M. Detry, Brussels
Belgium; P. Fioretti, Rotterdam, The Netherlands;
A. P. M. Gorgels, Maastricht, The Netherlands; M. Joy,
Chertsey, U.K.; J. K. Lubsen, Givrins, Switzerland; D. P.
Nicholls, Belfast, U.K.; P. Poole-Wilson, London, U.K.;
H. Roskamm, Bad Krozingen, Germany; L. Samek,
Bad Krozingen, Germany; M. L. Simoons, Rotterdam,
The Netherlands.