T-Scan Clinical Application Sheet Centric Relation Utilizing the T
advertisement

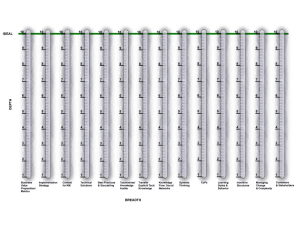
T-Scan Clinical Application Sheet Centric Relation Utilizing the T-Scan II Statement of Purpose/Treatment Significance The importance of isolating the centric relation prematurity when performing an occlusal equilibration has been advocated by numerous authors1-4. It is believed that when the condyles are properly positioned in centric relation, both articular discs are properly positioned between the head of the mandibular condyle and the superior aspect of the eminentia. At this fully seated condylar position, there is no stimulus for antagonistic muscle hyperactivity5. The centric relation prematurity can be located by various methods6-8 involving operator-guided mandibular positioning. Numerous studies have shown that joint position is influenced by the method used to record centric relation9-15. The method advocated by Dawson, known as bimanual manipulation8, has been widely recognized and accepted as a predictable way to assure the correctness of a mandibular closure into the centric relation position. The first occlusal contact that results from this bimanual manipulation procedure is known as the centric relation prematurity. To locate the centric relation prematurity, the operator relies on the patient to describe the general location of the perceived first tooth-to-tooth contact, by "feel", as the guided mandibular closure brings the first few teeth into contact. The isolation of the centric relation prematurity can be accomplished more precisely by performing bimanual manipulation in combination with a T-Scan II Real-Time Force Movie16 (recording) of the sequential tooth contacts that result from the guided closure. With real-time recording, it is possible to record a Force Movie16 of a guided mandibular closure into centric relation, which describes the sequential ordering of tooth contacts. Additionally, the duration of time in which the teeth are making occlusal contact, as they proceed from first contact in centric relation through the slide from centric relation to maximum intercuspation until maximum intercuspation is reached, can be recorded, and then visualized. The playback of the occlusal contact time data is presented to the operator on a sequential, frame-by-frame basis, or as a continuous movie from start to finish. The incremental playback of a real-time recording of a guided closure into centric relation can illustrate to the operator the location of the first tooth contact, its force content, and the length of time that it is premature to the rest of the occlusal contacts. This information enhances the operator's ability to locate the first tooth contact. Contributory factors affecting successful implementation of the T-Scan II Locating the centric relation prematurity is a "four-handed" procedure, during which the chair side assistant holds the articulating ribbon forceps intraorally, as the operator holds the condyles on the centric relation axis during closure. Tekscan, Inc., 307 West First St., So. Boston, MA 02127-1309 / (617) 464-4500 / (800) 248-3669 / Fax (617) 464-4266 Updated July 2002 1 The alternative technique is accomplished successfully with the chair side assistant managing the T-Scan II recording handle (instead of articulating ribbon forceps), while the operator performs the bimanual manipulation. Patient Preparation Place the patient in a supine position, with their body parallel to the floor and head cradled between the arms and midsection (see figure 1). Then practice the technique by attempting a few bimanual manipulation closures without the presence of the T-Scan II recording handle. This will help to orient both the patient and the operator to the technique, so that together they can repeatedly locate the centric relation position. Figure 1 T-Scan II Preparation Use the mouse to click the CR button on the T-Scan II toolbar (see Figure 2). This activates the centric relation recording mode, which insures that the T-Scan II allows for adequate recording time length for the operator to completely capture a bimanual manipulation procedure. The CR mode also raises the recording sensitivity to compensate for the low occlusal forces that a guided closure generally produces. Centric Relation Button Figure 2 T-Scan Toolbar (with CR Button) Recording technique Prior to recording a centric relation Force Movie, the chair side assistant should place the T-Scan II recording handle, with a sensor and arch support in place, between the maxillary Central Incisors of the patient. With the patient lying parallel to the floor, the recording handle should be held nearly perpendicular to the floor (see Figure 3). 2 Tekscan, Inc., 307 West First St., So. Boston, MA 02127-1309 / (617) 464-4500 / (800) 248-3669 / Fax (617) 464-4266 Updated July 2002 Figure 3 The chair side assistant commences the recording procedure by depressing, then releasing, the recording button that is located on the top surface of the recording handle. A computer prompt sounds (to mark the beginning of the real-time recording), after which the bimanual manipulation is commenced. After the mandible is properly seated in the centric relation position, the mandible is closed to tooth contact with the sensor. Locating the first centric relation contact The playback of the recording will reveal the location, the time duration of prematurity, and the force content of the first tooth contact. By attempting additional recordings (in the same manner as previously described), the reproducibility of the determination of the first contact can be validated. It is recommended that at least three bimanual manipulation recordings (Force Movies) be performed, to validate the location of the centric relation prematurity. Clinical Example Bimanual manipulation Force Movies of a 31 year-old female Prosthodontist, who exhibited the signs and symptoms often associated with chronic Myofascial Pain Dysfunction Syndrome, were taken. Her symptoms were characterized as mostly muscle contraction type, combined with mild TM Joint clicking and popping. Diagnostic load testing was accomplished to confirm the absence of non-adapted internal derangement in either temporomandibular joint. To begin testing, the patient was properly positioned. Initial training bimanual manipulation procedures were practiced by the operator and the patient, until the patient consistently reported her awareness of a repeatable first tooth contact. The patient reported that tooth #3 was consistently striking before all others. With CR mode activated, the T-Scan II handle was inserted intraorally, and an initial centric relation bimanual manipulation procedure was accomplished, using the sensor. The procedure was repeated three times for validation and reproducibility. The T-Scan II consistently located the palatal occlusal slope on tooth #12 as the first tooth contact that showed a moderate force level (see Figures 4 & 5). The first contact was consistent in all three movies. In figure 4, tooth #12 becomes forceful (the red contact) and tooth #14 approaches moderate force levels (the yellow contact) in advance of the earliest contacts on tooth #3 (the blue contact). Tekscan, Inc., 307 West First St., So. Boston, MA 02127-1309 / (617) 464-4500 / (800) 248-3669 / Fax (617) 464-4266 Updated July 2002 3 CR prematurity Palatal occlusal slope #12 Earliest forceful contacts on left side of arch Figure 4 Figure 5 In each of the centric relation recordings accomplished with bimanual manipulation, the first tooth contact on tooth #12 consistently preceded the appearance of light force on tooth #3 by an average of 1.1 seconds. The patientís perception of the first tooth contact was incorrect repeatedly. Figure 6 shows that the first contact is much lighter in color intensity than those tooth contacts that occur later. Figure 6 Conclusions Locating the Centric Relation Prematurity by performing Bimanual Manipulation in combination with the TScan II can significantly improve the precision of the procedure. With the real-time recording capability of the T-Scan II, tooth contact timing data can be sampled in .01 second increments. These fractional time increments will predictably reveal the correct sequence of tooth contact that results from performing the Bimanual Manipulation. Therefore, the first tooth contact can be isolated with improved predictability over the alternative methodology (without computer analysis), which relies on the patientís subjective occlusal assessments. 4 Tekscan, Inc., 307 West First St., So. Boston, MA 02127-1309 / (617) 464-4500 / (800) 248-3669 / Fax (617) 464-4266 Updated July 2002 References 1. Dawson, PE. Diagnosis and Treatment of Occlusal Problems, ed. 2. St. Louis, CV Mosby Co. 1989. 2. Schuyler, CH. Fundamental principles in the correction of occlusal disharmony, natural and artificial. JADA, Pp. 1193-1202, July, 1935 3. Glickman, l. Clinical Periodontology, ed. 4, Philadelphia, 1972, W.B. Saunders Co. 4. Long, JH. Occlusal adjustment. JPD 30:706-714, 1973. 5. Dawson, PE. Diagnosis and Treatment of Occlusal Problems. ed. 2. St Louis, CV Mosby Co. 1989. Pp. 31. 6. Long, JH. Location of the terminal hinge axis by intraoral means. JPD 23:11, 1970. 7. Lucia, VO. A technique for recording centric relation. JPD 14:492, 1964. 8. Dawson, PE. Diagnosis and Treatment of Occlusal Problems, ed. 2. St. Louis, CV Mosby Co. 1989. Pp. 41-47. 9. Kantor, ME, Silverman, SI, Garfinkel, L. Centric-relation recording techniques - a comparative investigation. JPD 1972; 28:593-600. 10. Hobo, S., Iwara, T. Reproducibility of mandibular centricity in three dimensions. JPD 1985;53:64954. 11. Roblee, RD. The determination of the accuracy of six maxillomandibular relation techniques. [Thesis] Waco, TX: Baylor University, 1989. 12. Wessberg GA, Epker, BN, Elliott AC. Comparison of mandibular rest position induced by phonetics, transcutaneous electrical stimulation, and masticatory electromyography. JPD 1983;49:100-5. 13. Remien, JC 2nd, Ash M Jr. "Myo-monitor centric: an evaluationî. JPD 1974;31:137-45. 14. Bessette RW, Quinlivan JT. Electromyographic evaluation of the MyoMonitor. JPD 1973;30:19-24. 15. Dao TT, Feine JS, Lund JP. Can electrical stimulation be used to establish a physiologic occlusal position? JPD 1988;60:509-14. 16. Maness, W.L., Force Movie. A time and force view of occlusion. Compendium 1989:10;404-8. Tekscan, Inc., 307 West First St., So. Boston, MA 02127-1309 / (617) 464-4500 / (800) 248-3669 / Fax (617) 464-4266 Updated July 2002 5