Pathologic Analysis of Tissue Destruction with
advertisement

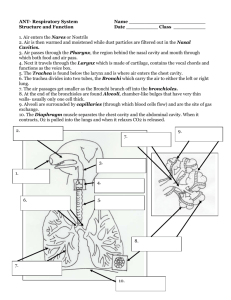
Pathologic Analysis of Tissue Destruction with Neutral Argon Plasma Madhuri TK1, Butler-Manuel SA1, Tailor A1 & Haagsma B2 1Department of Gynaecological Oncology, 2Department of Histopathology Royal Surrey County Hospital NHS Foundation Trust, Guildford, UK Background Results from Sigmoid Bowel Table 2 DTD varied from 0.2 -3.5mm (mean 1.29) LTS was minimal at all the settings ranging from 0.1-0.4(mean: 0.22) Tissue damage at the base of the cavity ranged from 0.07 to 0.4 (mean 0.15) Various electrosurgical devices have been developed to coagulate tissues and achieve haemostasis. Both conventional electrosurgery and the argon beam coagulator (ABC) employ a monopolar current passing though the patient. Plasmajet (PJ) is a novel electrically neutral device which uses a jet of high energy Argon Plasma for direct tissue effects. Energy is dissipated as light, kinetic energy and heat and PJ may be used for tissue dissection, coagulation of small vessels and even vapourization of tissues depending on the distance from the tissues, time of application and power setting used. Aim Leiomyoma Figure 1 showing cavity at 40% setting (3sec) Leiomyoma Figure 2 showing eschar at 40% setting (3sec) Figure 3 showing cavity at 40% setting (1sec) Figure 4 showing cavity at 40% setting (5sec) Figure 5 showing eschar at 40% setting (1sec) Figure 6 showing eschar at 40% setting (5sec) The aim of this study is to investigate the histopathological effects of tissue destruction (TD) and lateral thermal spread (LTS) following PJ use at different power settings used and tissue interaction time at a fixed distance of 1cm. Materials & Methods The study was performed in 3 phases using the same PJ handpiece and console. Consent was obtained from all women and tissue obtained at surgery was subjected to the PJ at different power settings and time duration. Initially this was performed on uterine fibroids. Subsequently, from women undergoing debulking for EOC, fresh tissue was harvested intraoperatively from the sigmoid bowel following anterior resection. Following tissue excision, 1cm3 sections of tissue was exposed to PJ at varied power settings and increasing time duration. These were formalin-fixed and stained. Histological examination of tissue destruction included assessment of cavity depth and extent of burn at the base of cavity.. Lateral thermal spread is remarkably constant and predictable with PJ tissue destruction, despite changes in power used. Increasing both power and tissue interaction time resulted in a deeper crater of tissue vapourization but with constant size of surrounding eschar. Discussion We previously reported the use of PJ for various applications in benign and malignant gynaecological procedures and these uniques tissue properties may well be of use in other specialties.1 In ovarian cancer debulking where optimal cytoreduction is desired, but many tumour deposits are on the surface of vital organs, the PJ appears to effectively vaporize cancer cells effectively. Minimal LTS and DTD is necessary especially when ablating tumour deposits around viscera and bowel surfaces. Results 144 specimens were analysed. These included 48 specimens each from a uterus (hysterectomy specimen for benign leiomyomata), omentum and from the sigmoid colon following anterior resection. Depth of Tissue Destruction DTD was defined by the depth of the cavity left by the ablated tissue. Conclusion Lateral Thermal Spread LTS was defined by the depth of histologically visible tissue damage. This was measured from the surface of the eschar to the level of normal tissue morphology. Leiomyoma Results Table 1 DTD for leiomyoma varied from 0.2 -3.48mm (mean 2.25mm) LTS was minimal at all the settings mentioned. (mean: 0.38 range 0.24 to 1) Tissue damage at the base of the cavity ranged from 0.1-0.22 (mean 0.17) The above data suggests that the PJ has unique properties which render it inherently safe and well suited to may be used optimal cytoreduction of metastatic ovarian cancer. An RCT to assess the role of this device including assessment of cost-effectiveness has been setup further evaluation. References 1. Madhuri TK, Papatheodorou D, Tailor A, Sutton CJG, Butler-Manuel SA. First clinical experience of argon neutral plasma energy in gynaecological surgery in the UK. Gynecol Surg. 2010:7(4):423-425 Table 1 showing the results of PJ use on leiomyomas Cavity Eschar Cavity Eschar Superficial Margin (mm) Cavity Base (mm) Depth (mm) 0.2 0.15 0.1 0.5 0.3 1.3 0.3 0.1 1 0.35 3 2 0.45 0.2 1.5 0.3 Exposure Time (Seconds) Depth (mm) 1 2 Superficial Margin (mm) Cavity Cavity Base (mm) Eschar Cavity Depth (mm) Superficial Margin (mm) Cavity Base (mm) 0.2 0.7 0.25 0.14 1.45 0.35 0.2 1.75 Eschar Depth (mm) Superficial Margin (mm) Cavity Base (mm) 0.22 1 0.25 0.1 0.2 1.25 0.24 0.2 0.35 0.15 1.57 0.24 0.22 5 2.25 0.4 0.15 4.25 0.45 0.2 3.1 0.47 0.13 2.25 0.4 0.2 7 3.5 0.44 0.1 3 0.4 0.13 3.3 0.51 0.15 3.05 0.25 0.15 9 4.5 0.6 0.19 3.9 1 0.14 3.6 0.65 0.16 3.48 0.25 0.22 Power Setting 10% 20% 40% 60% Table 2 showing the results of examination of the tumour tissue (serous carcinoma from sigmoid bowel) Cavity Exposure Time (Seconds) Depth (mm) 1 0.45 2 0.2 3 0.3 4 0.4 Power Setting Corresponding Eschar Superficial Margin (mm) Cavity Eschar Superficial Margin (mm) Cavity Base (mm) Depth (mm) 0.1 0.4 0.2 0.1 0.15 0.1 0.6 0.15 0.2 0.13 0.4 0.2 0.4 0.1 0.2 0.21 10% 20% Cavity Eschar Cavity Eschar Depth (mm) Superficial Margin (mm) Cavity Base (mm) Depth (mm) Superficial Margin (mm) 0.08 1 0.35 0.15 0.6 0.18 0.07 1.2 0.3 0.11 1 0.25 0.17 1.5 0.23 0.12 3.5 0.25 0.17 3.5 0.4 0.08 2.75 0.32 Cavity Base (mm) 40% 60% Cavity Cavity Base (mm) Eschar Depth (mm) Superficial Margin (mm) Cavity Base (mm) 0.3 1 0.12 0.1 0.15 1.25 0.18 0.12 0.2 2.25 0.25 0.2 0.15 3.5 0.25 0.15 80% PlasmaJet® is a trademark of Plasma Surgical, Ltd