Aging Process on Spectrally Determined
advertisement

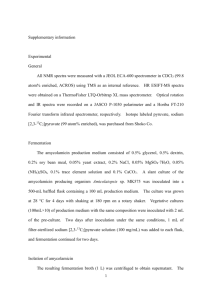
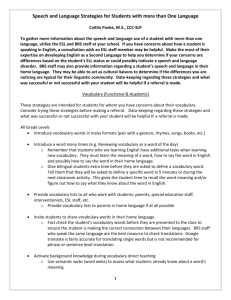
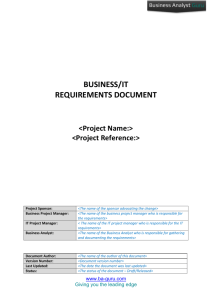
Aging Process on Spectrally Determined Spontaneous Baroreflex Sensitivity A 5-Year Prospective Study Jean-Pierre Fauvel, Catherine Cerutti, Ignace Mpio, Michel Ducher Abstract—The interindividual age-related decrease in baroreflex sensitivity (BRS) was reported in many cross-sectional studies. However, the long-term intraindividual decrease in BRS has never been confirmed by longitudinal studies. Data obtained from a 5-year prospective study designed to assess the 5-year stress effects on blood pressure (BP) provided the opportunity to assess longitudinal aging process on spectrally determined BRS (S-BRS) using the cross spectral analysis. This analysis was carried out in 205 men aged between 18 and 50 years who had 2 valid beat to beat BP recordings (Finapress) at a mean 5-year interval. At inclusion and at end of follow-up, S-BRS was significantly correlated with age (r⫽⫺0.50, P⬍0.001, r⫽⫺0.33, P⬍0.001 respectively). Interestingly, the slopes and the intercepts were not significantly different at a 5-year interval. This result is in favor of the good reproducibility of S-BRS. The attenuation with age of S-BRS was calculated at 3.6% a year. This decrease was slightly higher than the one obtained with the baseline data (2.3% per year). This longitudinal study provided, for the first time, an estimate of the slope of the age-related physiological S-BRS decrease in a mid-aged healthy male population. Our findings reinforce the interest of evaluating spontaneous BRS reported to predict hypertension and cardiovascular events in various populations. (Hypertension. 2007;50:543-546.) Key Words: mental stress 䡲 baroreflex 䡲 hypertension 䡲 blood pressure 䡲 reproducibility B aroreflex sensitivity (BRS) is a relevant index of the autonomic control of blood pressure (BP). Historically, BRS was determined using drug-induced BP and heart rate (HR) opposite variations. More recently, noninvasive techniques of determining spontaneous BRS have been implemented,1–3 the spectral method being one of the most popular. The spectral determination of BRS (S-BRS) is a reliable measure of BRS because it has often been reported to be correlated with the pharmacologically determined BRS.4 –7 S-BRS is easy to determine, and repeated measures are easy to make. Aging process on S-BRS has already been reported in several cross sectional studies.8 –12 Such studies only report interindividual S-BRS variation with age. Thus, S-BRS has consistently been reported to decrease with age. Physiological aging in men was associated with a marked reduction in baroreflex buffering. A differential aging process on baroreflex buffering BP and cardiovagal baroreflex was reported.10 The decrease in baroreflex buffering with aging was related to an increase in basal sympathetic nerve activity and to a reduction in systemic Alpha1-adrenergic vascular responsiveness whereas the decrease in cardiovagal baroreflex was related to a decrease in parasympathetic pathways.10,13 However, to our knowledge, the intraindividual BRS alteration with age has never been reported. For that purpose, we analyzed the S-BRS 5-year aging process in a cohort of 205 healthy young men. This unique data set was extracted from a 5-year follow-up study designed to assess stress effects on BP.14 In our study, because the sensitivity of the BRS control of HR was studied using the cross spectral analysis of SBP and HR, only the cardiovagal baroreflex was analyzed. Subjects and Methods Subjects The study was conducted on full-time employment subjects working in a chemical company, aged between 18 and 55 years (37⫾10 years). Among the 473 eligible subjects, 370 volunteered to participate in the study: 330 healthy subjects were included if their dipstick urinalysis were within normal limits and if they were free of any current medication that could interfere with BP regulation; 319 subjects had a valid baseline Finapres recording. After inclusion in 1995, subjects were followed for outcome until 2001. None of the subjects was lost for follow-up and each subject who was planned to discontinue the study had a final evaluation for the primary end point of the stress study. During the 5-year follow-up, 94 subjects had a premature final visit. Main reasons for discontinuation during follow-up were retirement (31 subjects), job transfer (22 subjects), and medical reason (n⫽9). No Finapres recording was planned in case of premature discontinuation. Among the 257 subjects who had a final visit 5 years later, 5 subjects refused to have a Finapres Received March 10, 2007; first decision March 30, 2007; revision accepted June 8, 2007. From the Hôpital E. Herriot (J.-P.F., I.M., M.D.), Department of Nephrology, and INSERM ERI22 and Université Lyon 1 EA4173 (J.-P.F., C.C.), Université Claude Bernard, Lyon, France. Correspondence to J-P. Fauvel, Département de Néphrologie et Hypertension Artérielle, Hôpital E. Herriot, 69437 Lyon Cedex 03, France. E-mail jean-pierre.fauvel@chu-lyon.fr © 2007 American Heart Association, Inc. Hypertension is available at http://hyper.ahajournals.org DOI: 10.1161/HYPERTENSIONAHA.107.090811 543 544 Hypertension September 2007 Characteristics of the 205 Study Subjects at Baseline and at the End of Follow-Up tion of the modulus of the transfer function between SBP and HR variations in the mid-frequency band (0.07 to 0.15 Hz). Parameter Baseline End of Follow-Up P Values Statistical Analysis BMI, kg/m 24.9⫾3.4 25.6⫾5.7 ⬍0.001 Alcohol, score 2.10⫾0.99 1.91⫾0.95 ⬍0.05 SBP, mm Hg 127⫾9 131⫾13 ⬍0.001 63⫾8 63⫾9 NS 12.4⫾5.6 10.0⫾5.7 ⬍0.001 Data are expressed as mean⫾SD in the text and tables. Mean S-BRS was computed for 6 clusters of age (ⱕ25, 26 to 30, 31 to 35, 36 to 40, 41 to 45, ⱖ46 years). Mean values of S-BRS in each cluster of age were compared using an ANOVA followed by a post hoc Fischer test. The normal distribution of each variable was tested using a KolmokorowSmirnoff test. The age-related decrease in S-BRS in each cluster of age was compared in absolute values and in percentage. The paired Student t test was used to compare inclusion to end of follow-up mean values. Pearson coefficients of correlation were computed to assess time process for each variable. All statistical analyses were performed using Statistica 6 software (StatSoft Inc). P⬍0.05 was considered statistically significant. 2 HR, bpm S-BRS, ms/mm Hg Data are expressed as means⫾SD. recording and 27 recordings were not valid for S-BRS assessment. Because the population was mainly composed of men (20 women), the presented data of baroreflex aging process were restricted to the 205 men who had 2 valid beat-to-beat BP recordings at a 5-year interval (5.3⫾1.4 years). Anthropometric variables (age, body mass index [BMI]) are summarized in the Table. Alcohol consumption was classified into 5 levels after interview (⬍1 drink/week, ⬍1 drink/d, 1 to 2 drinks/d, 3 to 4 drinks/d, ⬎4 drinks/d). All patients gave their written informed consent and the study protocol was approved by the independent Lyons Ethics Committee. Protocol of Work-Site BP Measurement The study was conducted at work site, in a quiet room with a controlled temperature at 20°C. Work-site systolic (SBP) and diastolic (DBP) BP were measured 3 times in a row with the use of a mercury sphygmomanometer, after 5 minutes resting in a recline position. The average of the last 2 SBP and DBP measurements was taken into account. These measurements were made at the beginning and end of follow-up. Beat-to-beat BP was also recorded using a Finapres device (model 2300, Ohmeda). The cuff was wrapped around the forefinger of the nondominant arm resting on a table, whose level was adjusted to obtain a less than 5 mm Hg difference with the previously determined BP (mercury sphygmomanometer). The equipped arm of the seated subject was held in the same position throughout the procedure. After a 2-minute period of familiarization, the automatic calibration was switched off. BP and HR were then recorded for 10 minutes at rest. BP Signal Analysis Signal acquisition and data processing to assess spontaneous BRS was previously described.15 In brief, BP signals were sampled at a rate of 100 Hz and data were stored for further processing. Data processing was performed on a 4-minute recording. The spectral determination of BRS was assessed on a 256 points completed to 512 points by zero padding. Cross-spectral analysis of SBP and HR was performed. The zero padding was used to increase the frequency resolution of the LF band. S-BRS was estimated through computa- Results Mean age of subjects was 36⫾10 years at baseline. Subjects whose baseline BP was greater than 140/90 mm Hg represented 11.2% of the population. The Table summarizes the mean characteristics of the study population at baseline. SBP and HR individual values were significantly correlated 5 years later (r⫽0.61, P⬍0.001; r⫽0.59, P⬍0.001, respectively). S-BRS had a normal distribution (d⫽0.072, NS). S-BRS individual values were negatively correlated with age at inclusion and end of follow-up (r⫽⫺0.50, P⬍0.001, Figure 1A; r⫽⫺0.33, P⬍0.001, Figure 1B). After a 5-year interval, mean S-BRS was significantly lower (Table). S-BRS at baseline was significantly correlated with S-BRS at the end of follow-up (r⫽0.45, P⬍0.001; Figure 1C). The 5-year decrease in S-BRS was significant in clusters of ages (20 to 25, 26 to 30, 36 to 40, 41 to 45 years; Figure 2). However, the age-related decrease in SBRS, neither in absolute values (Figure 3) nor in percentage (data not shown), were significantly different between clusters of age. The age related decrease in S-BRS was significantly correlated with the baseline S-BRS (r⫽⫺0.51; P⬍0.001). BRS was slightly correlated with BMI at baseline (r⫽⫺0.18, P⬎0.05) but not at the end of follow-up (r⫽⫺0.09; NS). Five-year changes in S-BRS were not significantly linked with those in BMI (r⫽⫺0.14; NS). Discussion Cross-sectional studies suggested that BRS decreased with age when comparing the BRS of subjects of various ages.8 –12 Our longitudinal study is the first to confirm the decrease in S-BRS Figure 1. Correlations between age and S-BRS at inclusion (A) and 5 years later (B). Correlation between S-BRS at inclusion and 5 years later (C). S-BRS indicates spectral baroreflex sensitivity. Fauvel et al Aging Process on Baroreflex 545 Figure 3. Box plot representation of the 5-year S-BRS alteration by cluster of age. S-BRS indicates spectral baroreflex sensitivity. Figure 2. S-BRS at inclusion and 5 years later in each cluster of age. *P⬍0.05 at a 5-year interval. S-BRS indicates spectral baroreflex sensitivity. over time in men. Furthermore, between 20 and 50 years, the 5-year decrease in S-BRS is constant and not age-related. We implemented a longitudinal study designed to assess the stress effects on 5-year BP alteration in a large sample of subjects.14 Individual BP stress reactivity and individual impact of job strain were tested for BP alteration. Stress BP reactivity was measured with Finapres device at a 5-year interval between inclusion and end of follow-up. This data set provided a unique opportunity to assess aging process on S-BRS. BRS can be determined in the frequency domain by the computation of cross-spectral analysis but also in the time domain using the sequence method.3 The determination of BRS in the temporal domain using the sequence method had consistently been reported to be strongly correlated with spectral BRS determination.15–18 As in our experience the sequence method appeared to be slightly less reproducible at short term (1 week), we now only determine BRS in the frequency domain. Recently, Johnston et al also reported lower coefficients of variation and reproducibility coefficients if BRS were determined with the spectral method instead of the sequence method.19 As already reported in cross-sectional studies, S-BRS among subjects aged between 18 and 50 years decreased with age. In young adults, Davy et al20 showed that baroreflex sympathetic pathway was preserved with age. Baroreflex control of sympathetic nerve activity was not altered whereas baroreflex control of parasympathetic nerve activity was attenuated by aging in humans.13 Moreover Laitinen et al12 confirmed these results in a larger sample of subjects (n⫽63, aged 23 to 77 years) using both the sequence and the cross-spectral determination of BRS for Finapres recordings. Such a result is important to consider because a baroreflex impairment that is the consequence of the decrease of the vagal autonomic function is considered as an independent marker of mortality.21–22 We also found such an aging process on BRS when analyzing baseline data. Five years later, S-BRS was also significantly correlated with age. Interestingly, the slopes and the intercepts were not significantly different at a 5-year interval, which is in favor of the good reproducibility of the spectral determination of BRS. The significant test-retest correlation obtained in a large number of subjects at a 5-year interval showed that S-BRS has a predictable time evolution. For instance, at a 5-year interval the test-retest correlation coefficient of S-BRS (r⫽0.45, P⬍0.001) was within the range of the SBP one (r⫽0.61, P⬍0.001). Time evolution of S-BRS is thus as predictable as the SBP one. Because S-BRS is partly derived from SBP determination, any estimate of its time evolution is limited by the time evolution of the BP signal. Because S-BRS is reproducible in the short term15,23–25 and has a predictable evolution in the long term, S-BRS can be considered an intrinsic characteristic of each subject and therefore used in research studies and clinical practice. In cross-sectional studies, a large variability in interindividual BRS was consistently observed. Our study is the first one to analyze the aging process on BRS by means of a prospective design. A longitudinal design provided a better control of BRS variability, each subject being his own control. The slope of the age-related decrease in S-BRS (⫺0.45 ms/mm Hg/year) was higher to the one obtained with the cross-sectional data (⫺0.28 ms/mm Hg/year). In our longitudinal study, the decrease in S-BRS represented 3.6% per year. Although not significant, Figure 3 suggests that S-BRS decrease with age could be attenuated after 45 years. However, Umetani et al26 reported a linear decrease in autonomic control from 10 to 99 years. A longitudinal study including older subjects would be of major interest. Limitations Although controversial, cardiovagal baroreflex gain has been reported to be significantly lower in women compared with men.27 In our study, it was not possible to analyze gender effects. Thus, our results should be restricted to measuring S-BRS decrease between 18 and 50 years in a male population. In our study, physical activity was not recorded. Physical training increases BRS and might decrease cardiovascular risk in a given subject. The physiological decrease in BRS is unclear. Major hypotheses include aging process on the intima/media ratio of the carotid and aging process on the speed of nerve conduction. The age-related decrease in S-BRS could also be a mixture of cell aging, reduced physical 546 Hypertension September 2007 activity, and BMI increase. As our cohort study did not control these factors, it was not possible to differentiate relative influences of each potential mechanism. Perspectives The BRS that is easily determined using a 5-minute rest BP recording should be more frequently monitored. A normal BRS is an index of the integrity of the autonomic nervous system. It is an intrinsic characteristic of each subject which might be considered as an integrator of many physiopathological events. BRS is increased by physical activity and conversely altered in diabetes and hypertension. A study whose aim would be to evaluate its prognostic value in healthy populations to predict hypertension should be undertaken. BRS has also been associated with metabolic risk factors and proposed to be an ideal index of cardiovascular risk in hypertension.28 Furthermore, the decrease in the vagal component of BRS may also be considered as an independent risk factor of cardiovascular events as recently reported in chronic renal failure.29 The contribution of BRS to treatment effects could be considered in clinical trial. For instance, in secondary prevention, endarterectomy of the internal carotid artery showed the increase of BRS and its improving was correlated to cardiovascular events at a 5-year interval.30 This longitudinal study confirms the age-related decrease in BRS already reported in cross sectional studies. In men aged 18 to 50 years, the decrease in BRS was evaluated at 3.6% a year. Our findings reinforce the interest of evaluating spontaneous BRS known to predict hypertension31 and cardiovascular events in various populations.21,22 Acknowledgments The authors thank Christiane Bertheux-Beaufrere for translation support. The authors also thank all of the subjects who volunteered for the study. Disclosures None. References 1. Robbe HW, Mulder LJ, Ruddel H, Langewitz WA, Veldman JB, Mulder G. Assessment of baroreceptor reflex sensitivity by means of spectral analysis. Hypertension. 1987;10:538 –543. 2. Pagani M, Somers V, Furlan R, Dell’Orto S, Conway J, Baselli G, Cerutti S, Sleight P, Malliani A. Changes in autonomic regulation induced by physical training in mild hypertension. Hypertension. 1988;12:600 – 610. 3. Bertinieri G, di Rienzo M, Cavallazzi A, Ferrari AU, Pedotti A, Mancia G. A new approach to analysis of the arterial baroreflex. J Hypertens. 1985;3:S79 – 81. 4. Colombo R, Mazzuero G, Spinatonda G, Lanfranchi P, Giannuzzi P, Ponikowski P, Coats AJ, Minuco G. Comparison between spectral analysis and the phenylephrine method for the assessment of baroreflex sensitivity in chronic heart failure. Clin Sci (Lond). 1999;97:503–513. 5. Pitzalis MV, Mastropasqua F, Passantino A, Massari F, Ligurgo L, Forleo C, Balducci C, Lombardi F, Rizzon P. Comparison between noninvasive indices of baroreceptor sensitivity and the phenylephrine method in postmyocardial infarction patients. Circulation. 1998;97:1362–1367. 6. Watkins LL, Grossman P, Sherwood A. Noninvasive assessment of baroreflex control in borderline hypertension: comparison with the phenylephrine method. Hypertension. 1996;28:238 –243. 7. Parlow J, Viale JP, Annat G, Hughson R, Quintin L. Spontaneous cardiac baroreflex in humans: comparison with drug-induced responses. Hypertension. 1995;25:1058 –1068. 8. Ebert TJ, Morgan BJ, Barney JA, Denahan T, Smith JJ. Effects of aging on baroreflex regulation of sympathetic activity in humans. Am J Physiol. 1992;263:H798 –H803. 9. Gribbin B, Pickering TG, Sleight P, Peto R. Effect of age and high blood pressure on baroreflex sensitivity in man. Circ Res. 1971;29:424 – 431. 10. Jones PP, Christou DD, Jordan J, Seals DR. Baroreflex buffering is reduced with age in healthy men. Circulation. 2003;107:1770 –1774. 11. Fluckiger L, Boivin JM, Quilliot D, Jeandel C, Zannad F. Differential effects of aging on heart rate variability and blood pressure variability. J Gerontol A Biol Sci Med Sci. 1999;54:B219 –B224. 12. Laitinen T, Hartikainen J, Vanninen E, Niskanen L, Geelen G, Lansimies E. Age and gender dependency of baroreflex sensitivity in healthy subjects. J Appl Physiol. 1998;84:576 –583. 13. Matsukawa T, Sugiyama Y, Mano T Age-related changes in baroreflex control of heart rate and sympathetic nerve activity in healthy humans. J Auton Nerv Syst. 1996, 12;60:209 –212. 14. Fauvel JP, M’Pio I, Quelin P, Rigaud JP, Laville M, Ducher M. Neither perceived job stress nor individual cardiovascular reactivity predict high blood pressure. Hypertension. 2003;42:1112–1116. 15. Ducher M, Fauvel JP, Gustin MP, Cerutti C, Najem R, Cuisinaud G, Laville M, Pozet N, Paultre CZ. A new non-invasive statistical method to assess the spontaneous cardiac baroreflex in humans. Clin Sci (Colch). 1995;88:651– 655. 16. Laude D, Elghozi JL, Girard A, Bellard E, Bouhaddi M, Castiglioni P, Cerutti C, Cividjian A, Di Rienzo M, Fortrat JO, Janssen B, Karemaker JM, Leftheriotis G, Parati G, Persson PB, Porta A, Quintin L, Regnard J, Rudiger H, Stauss HM. Comparison of various techniques used to estimate spontaneous baroreflex sensitivity (the EuroBaVar study). Am J Physiol Regul Integr Comp Physiol. 2004;286:R226 –R231. 17. Westerhof BE, Gisolf J, Stok WJ, Wesseling KH, Karemaker JM. Timedomain cross-correlation baroreflex sensitivity: performance on the EUROBAVAR data set. J Hypertens. 2004;22:1371–1380. 18. Porta A, Baselli G, Rimoldi O, Malliani A, Pagani M. Assessing baroreflex gain from spontaneous variability in conscious dogs: role of causality and respiration. Am J Physiol Heart Circ Physiol. 2000;279:H2558–H2567. 19. Johnson P, Shore A, Potter J, Panerai R, James M. Baroreflex sensitivity measured by spectral and sequence analysis in cerebrovascular disease: methodological considerations. Clin Auton Res. 2006;16:270 –275. 20. Davy KP, Tanaka H, Andros EA, Gerber JG, Seals DR. Influence of age on arterial baroreflex inhibition of sympathetic nerve activity in healthy adult humans. Am J Physiol. 1998;275:H1768 –H1772. 21. Osterziel KJ, Hanlein D, Willenbrock R, Eichhorn C, Luft F, Dietz R. Baroreflex sensitivity and cardiovascular mortality in patients with mild to moderate heart failure. Br Heart J. 1995;73:517–522. 22. La Rovere MT, Bigger TJ, Marcus FI, Mortara A, Schwartz PJ; for the ATRAMI (Autonomic Tone and Reflexes After Myocardial Infarction) investigators. Baroreflex sensitivity and heart rate variability in prediction of total cardiac mortality after myocardial infarction. Lancet. 1998;351: 478–484. 23. Iellamo F, Legramante JM, Raimondi G, Castrucci F, Massaro M, Peruzzi G. Evaluation of reproducibility of spontaneous baroreflex sensitivity at rest and during laboratory tests. J Hypertens. 1996;14:1099 –1104. 24. Davies LC, Francis D, Jurak P, Kara T, Piepoli M, Coats AJ. Reproducibility of methods for assessing baroreflex sensitivity in normal controls and in patients with chronic heart failure. Clin Sci (Lond). 1999;97:515–522. 25. Herpin D, Ragot S. Mid- and long-term reproducibility of noninvasive measurements of spontaneous arterial baroreflex sensitivity in healthy volunteers. Am J Hypertens. 1997;10:790 –797. 26. Umetani K, Singer DH, McCraty R, Atkinson M. Twenty-four hour time domain heart rate variability and heart rate: relations to age and gender over nine decades. J Am Coll Cardiol. 1998;31:593– 601. 27. Beske SD, Alvarez GE, Ballard TP, Davy KP. Gender difference in cardiovagal baroreflex gain in humans. J Appl Physiol. 2001;91:2088–2092. 28. Lantelme P, Khettab F, Custaud MA, Rial MO, Joanny C, Gharib C, Milon H. Spontaneous baroreflex sensitivity: toward an ideal index of cardiovascular risk in hypertension? J Hypertens. 2002;20:935–944. 29. Johansson M, Gao SA, Friberg P, Annerstedt M, Carlstrom J, Ivarsson T, Jensen G, Ljungman S, Mathillas O, Nielsen FD, Strombom U. Baroreflex effectiveness index and baroreflex sensitivity predict all-cause mortality and sudden death in hypertensive patients with chronic renal failure. J Hypertens. 2007;25:163–168. 30. Hirschl M, Kundi M, Blazek G. Five-year follow-up of patients after thromboendarterectomy of the internal carotid artery: relevance of baroreceptor sensitivity. Stroke. 1996;27:1167–1172. 31. Ducher M, Cerutti C, Chatellier G, Fauvel JP. Is high job strain associated with hypertension genesis? Am J Hypertens. 2006;19:694 –700.