Neuropathy
Genetic Testing for Hereditary Neuropathy
A Guide for Clinicians
KNOWING WHAT TO LOOK FOR KNOWING WHERE TO LOOK AND KNOWING WHAT IT MEANS
Introduction
The inherited neuropathies are a large group of genetically and phenotypically
heterogeneous disorders affecting the peripheral nervous system.
Hereditary neuropathies are categorized by involvement of motor, sensory
and/or autonomic nerve fibers (Dyck et al., 2005). They can be divided into
3 main categories: hereditary motor and sensory neuropathies (HMSN), also
known as Charcot-Marie-Tooth (CMT) disease, hereditary motor neuropathy,
and hereditary sensory and autonomic neuropathy (HSAN) (see Table 1). The
peripheral neuropathies have overlapping symptoms including muscle weakness,
foot deformities, depressed or absent reflexes and loss of sensation. In addition to
genetic causes, there are many non-genetic, or acquired, causes of neuropathy,
including: diabetes mellitus, trauma, alcohol, vitamin B12 deficiency, thyroid
disease, vasculitis, HIV infection, leprosy, neurosyphilis, amyloid neuropathies
and other inflammatory and immune related neuropathies. The diagnostic
process aims to determine if an individual’s symptoms are due to an acquired
or genetic form of neuropathy. The elucidation of a specific diagnosis and
etiology is mainly based on age of onset, family history, neurologic studies;
such as nerve conduction studies, blood tests, and genetic testing.
Hereditary Neuropathy Panel at GeneDx
Table 1: Sequencing and Del/Dup Testing
Charcot-Marie-Tooth
Disease
Hereditary Sensory
Neuropathies
Other Hereditary
Neuropathies
AARS, DNM2, DYNC1H1, EGR2,
FGD4, FIG4, GARS, GDAP1,
GJB1, HSPB1, HSPB8, LITAF,
LMNA, LRSAM1, MED25, MFN2,
MPZ, MTMR2, NDRG1, NEFL,
PDK3, PMP22, PRPS1, PRX,
RAB7A, SBF2, SH3TC2, TRPV4
ATL1, DNMT1,
FAM134B, IKBKAP,
KIF1A, NGF, NTRK1,
SCN9A, SPTLC1,
SPTLC2, WNK1
ATP7A, BSCL2, DNAJB2,
GAN, GLA, IGHMBP2,
PLEKHG5, REEP1,
SLC12A6, TFG, TTR
Large PMP22 deletions are responsible for approximately 80% of cases of
hereditary neuropathy with liability to pressure palsy (HNPP), and duplications
of the PMP22 gene are responsible for approximately 70% of Charcot-MarieTooth Type 1 (CMT1) cases. PMP22 deletion/duplication testing is available
as part of the panel and as a separate test.
G E N E T I C T E S T I N G F O R N E U R O PAT H Y: A G U I D E F O R C L I N I C I A N S
1
Genetics of Hereditary Neuropathies
Currently, over seventy genes have been described in the literature to cause
inherited neuropathies (Rossor et al., 2013). Genetic forms of neuropathy can
be inherited in autosomal dominant, autosomal recessive or X-linked inheritance
patterns. They can also be sporadic without a family history of neuropathy and
may be the result of a new (de novo) mutation in a patient. A genetic diagnosis
is identified in approximately 50-70% of individuals with Charcot-Marie-Tooth
disease (Vallat et al., 2013), 30% of individuals with hereditary sensory and
autonomic neuropathy (HSAN) (Rotthier et al., 2012), and 20% of individuals
with distal motor neuropathy (Rossor et al, 2012). Pathogenic mutations in some
genes have been associated with multiple phenotypes or clinical patterns. For
example, mutations in the GARS gene can be associated with Charcot-MarieTooth type 2D or with distal spinal muscular atrophy type V, and mutations
in the GDAP1 gene can be inherited in an autosomal dominant or autosomal
recessive manner and have been associated with axonal, demyelinating or
intermediate nerve conduction velocity tests (Barhoumi et al., 2001; Cuesta
et al., 2002).
Diagnosis of Hereditary Neuropathies
The diagnosis of a genetic neuropathy is based on a combination of personal
health history, family health history, complete neurological exam and neurological
tests.
• Clinical and Family History:
• The medical and family history may indicate whether the neuropathy is
likely due to an acquired or genetic cause
• The mode of inheritance can be helpful in differentiating possible
diagnoses
•Physical examination may reveal symptoms of sensory, autonomic or
motor neuropathy (see Table 2)
•Neurological testing can include:
• Nerve conduction velocity (NCV)
• Electromyography (EMG)
• Nerve biopsy
•Genetic testing:
• If the medical and family history, physical exam, or clinical evaluation
suggest a genetic cause, then genetic testing should be offered.
2
Table 2: Inherited Neuropathy Phenotypes
Phenotype
Description
Hereditary Motor and
Sensory Neuropathy
(HMSN) more commonly
known as Charcot Marie
Tooth (CMT)
•
Hereditary Motor
Neuropathy
•
•
•
•
•
•
•
•
•
•
•
Hereditary Sensory and
Autonomic Neuropathy
Progressive distal muscle weakness with feet
and legs most severely affected
Paresthesia and/or loss of sensation
Foot drop
Depressed deep tendon reflexes
Hammer toes
Pes cavus (high arches)
Primary motor symptoms and a lack of
sensory and autonomic symptoms
Progressive weakness and atrophy of the
distal muscles
Decreased or absent reflexes
Reduced motor amplitude potentials on NCV
Foot deformities
Less common features include: vocal cord
and diaphragm paralysis, pyramidal tract
signs
•
•
Progressive loss of sensation
Altered perception of pain, temperature,
and touch which can lead to hyperkeratosis,
chronic ulcers, dystrophic nails, osteomyelitis
• Distal muscle weakness
• Depressed reflexes
• Excessive sweating
• Gastroesophageal reflux
• Postural hypotension
•Apnea
•Incontinence
•Self-mutilation
•Deafness
G E N E T I C T E S T I N G F O R N E U R O PAT H Y: A G U I D E F O R C L I N I C I A N S
3
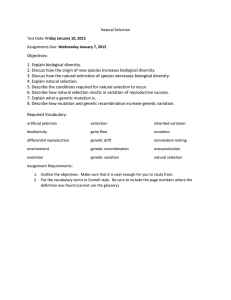
Algorithm for Peripheral Neuropathy Testing
Peripheral
Neuropathy
Acquired
CNS
+
peripheral features
Inherited
Mitochondrial disorder?
• Diabetes mellitus
• Autoimmune disorder
• Nutritional diseases
• Alcoholism
• Toxin exposure
Appropriate
laboratory testing
• PMP22 del/dup testing
• Hereditary neuropathy
panel
positive
negative
Comprehensive
mitochondrial disorder
panel
negative
Consider whole
exome sequencing
4
positive
Clinical Utility of Genetic Testing
Genetic testing in an individual with neuropathy
1. Can establish the genetic cause of neuropathy
2. Provides information about prognosis
3. May prevent the need for other costly and/or painful testing
4. Confirms the inheritance pattern and allows for more accurate risk
assessment of family members
5. Permits predictive testing for asymptomatic family members when
there is a known disease-causing mutation associated with a
genetic form of neuropathy
6. Enables clinical monitoring, follow-up, and optimal treatment when
symptoms develop in an individual with a positive genetic result
7. Enables prenatal diagnosis for known pathogenic mutations in
at-risk pregnancies
8. Allows accurate genetic counseling, recurrence risk determination,
and family planning
Possible Genetic Test Results and What They Mean
There are three possible outcomes of genetic testing: a positive result, a negative
result, or an inconclusive result.
Positive
A positive result indicates that a disease-causing mutation was identified in
the individual who was tested. This finding confirms the diagnosis as well as
identifying the genetic cause. A genetic diagnosis provides valuable information
to the physician and family members about treatment, prognosis, and recurrence
risk. First-degree relatives (e.g., children, siblings, and parents) of a patient with
a positive genetic test result can then be offered predictive genetic testing. If
a family member is found to be positive for the familial mutation(s), depending
on the mode of inheritance, this individual may also be at risk for neuropathy
and should be referred for further evaluation. It is important to note that there
can be variability in symptoms, age of onset, and disease severity even among
members of the same family who have the same genetic mutation.
G E N E T I C T E S T I N G F O R N E U R O PAT H Y: A G U I D E F O R C L I N I C I A N S
5
Negative
A negative genetic test result in an individual with neuropathy does not rule
out a genetic cause. Possible reasons for a negative result could be (1) the
patient has a mutation in a gene not included in the testing panel, (2) the patient
may have a mutation in a part of a neuropathy gene that was not covered
by the test, or (3) the patient does not have a heritable form of neuropathy.
A negative genetic test result in an individual with neuropathy indicates that
predictive testing of asymptomatic family members with the same test will not
be informative. However, family members of a clinically affected individual with
negative test results may still be at risk neuropathy based on the family history.
If an asymptomatic individual tests negative for a disease-causing mutation
identified in a family member with neuropathy, the individual is expected to have
the same risk to develop neuropathy as a person in the general population.
Specific clinical monitoring for the development of neuropathy may be reduced
or eliminated in these individuals.
Variant of Unknown Significance (VUS)
One of the most difficult results to interpret is the finding of a variant of unknown
clinical significance (VUS). This result indicates that the role of the genetic
change in causing neuropathies has not clearly been established. In some
cases, testing of other family members may help clarify the clinical significance
of a VUS. If other relatives with neuropathy are found to have the same variant,
it is more likely that the variant is disease-causing. The greater the number of
affected family members who carry the VUS, the greater the likelihood that
the identified variant is pathogenic. If, on the other hand, an individual is the
only affected family member, the finding that the VUS identified at GeneDx is
de novo (was not inherited from a parent) supports the interpretation that the
variant is likely disease-causing.
In some cases, an individual may be found to have a single mutation in a gene
associated with an autosomal recessive disorder. In this case, the results are
inconclusive as the individual may be a heterozygous carrier of a single mutation,
or they may have a second mutation in that gene which was not detected by
the test. For individuals who have a single mutation identified in an autosomal
recessive disorder, clinical correlation is required and additional testing may be
necessary.
6
Interpretation of Variants of Unknown Significance
At GeneDx we have a multi-step process of evaluating variants that includes:
•Review of published literature
•Review of publicly available and internal mutation databases
•The frequency of the variant in the population
•Evolutionary conservation
•In silico prediction models
•Consideration of the reported mutation spectrum for the gene
•Segregation of the variant with the disease in the family
Resources for Patients
You can find more information at the following websites:
•Genereviews: www.ncbi.nlm.nih.gov/books/NBK1116/
•National Institutes of Health Genetics Home Reference(NIH/GHR):
http://ghr.nlm.nih.gov/
•National Institute of Neurological Disorders and Stroke:
www.ninds.nih.gov/disorders/neuropathy_hereditary/neuropathy_
hereditary.htm
•OMIM: http://www.omim.org/
Search for Research Studies for Neuropathy
•Clinical trials: http://clinicaltrials.gov/
•Inherited Neuropathies Consortium:
http://rarediseasesnetwork.epi.usf.edu/INC/about/mission.htm
Patient Support Organization
•Charcot-Marie-Tooth Association: http://cmtausa.org/
•Hereditary Neruopathy Foundation: www.hnf-cure.org
•Muscular Dystrophy Association: http://mda.org/
•The Neuropathy Association: http://www.neuropathy.org
Genetic Counseling
•National Society of Genetic Counselors: www.nsgc.org
G E N E T I C T E S T I N G F O R N E U R O PAT H Y: A G U I D E F O R C L I N I C I A N S
7
References
1. Barhoumi C, Amouri R, Ben Hamida C, Ben Hamida M, Machghoul S,
Gueddiche M, Hentati F. Linkage of a new locus for autosomal recessive axonal
form of Charcot-Marie-Tooth disease to chromosome 8q21.3. Neuromuscul
Disord. 2001 Jan;11(1):27-34.
2. Cuesta A, Pedrola L, Sevilla T, García-Planells J, Chumillas MJ, Mayordomo F,
LeGuern E, Marín I, Vílchez JJ, Palau F. The gene encoding ganglioside-induced
differentiation-associated protein 1 is mutated in axonal Charcot-Marie-Tooth
type 4A disease. Nat Genet. 2002 Jan;30(1):22-5. Epub 2001 Dec 17.
3. Dyck, P. J., Thomas, P. K., Griffin, J. W., Low, P. A. & Poduslo, J. F. (Eds)
Peripheral Neuropathy (WB Saunders, Philadelphia, 2005.
4. Rossor AM, Kalmar B, Greensmith L, Reilly MM. The distal hereditary motor
neuropathies. J Neurol Neurosurg Psychiatry. 2012 Jan;83(1):6-14. doi: 10.1136/
jnnp-2011-300952. Epub 2011 Oct 25.
5. Rossor AM, Polke JM, Houlden H, Reilly MM. Clinical implications of genetic
advances in Charcot-Marie-Tooth disease. Nat Rev Neurol. 2013 Oct;9(10):56271. doi: 10.1038/nrneurol.2013.179. Epub 2013 Sep 10.
6. Rotthier A, Baets J, Timmerman V, Janssens K. Mechanisms of disease in
hereditary sensory and autonomic neuropathies. Nat Rev Neurol. 2012 Jan
24;8(2):73-85. doi: 10.1038/nrneurol.2011.227.
7. Siskind CE, Panchal S, Smith CO, Feely SM, Dalton JC, Schindler AB, Krajewski
KM. A review of genetic counseling for Charcot Marie Tooth disease (CMT). J
Genet Couns. 2013 Aug;22(4):422-36. doi: 10.1007/s10897-013-9584-4. Epub
2013 Apr 21.
8. Vallat JM, Mathis S, Funalot B. The various Charcot-Marie-Tooth diseases. Curr
Opin Neurol. 2013 Oct;26(5):473-80. doi: 10.1097/WCO.0b013e328364c04b.
8
About GeneDx
GeneDx is a highly respected genetic testing company founded in 2000 by two
scientists from the National Institutes of Health (NIH) to address the needs of
patients and clinicians concerned with rare inherited disorders. GeneDx offers
sequencing and deletion/duplication testing for inherited cardiac disorders,
mitochondrial disorders, neurological disorders, inherited cancer disorders,
prenatal disorders and other rare genetic disorders. GeneDx also offers whole
exome sequencing, next-generation and microarraybased testing. At GeneDx, our
technical services are matched by our scientific expertise and customer support.
Our growing staff includes more than 70 geneticists and genetic counselors
specialized in clinical genetics, molecular genetics, metabolic genetics and
cytogenetics who are just a phone call or email away. We invite you to visit our
website www.genedx.com to learn more about us and the services we offer.
207 Perry Parkway
Gaithersburg, MD 20877
T 1 301 519 2100 • F 1 301 519 2892
E GeneDx@GeneDx.com • www.genedx.com
© 2014 GeneDx. All rights reserved. 91656 05/2014