diagnostic tool for MI, thus allowing its
advertisement

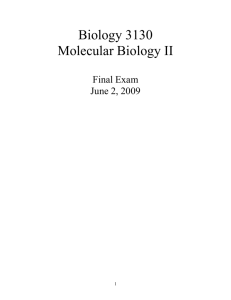
Clinical Chemistry 48, No. 10, 2002 diagnostic tool for MI, thus allowing its implementation in routine clinical practice where cardiac troponin tests are used for both purposes. This work was partially supported by First Medical (Mountain View, CA). The study design and data analysis were not influenced by First Medical. Drs. Apple and Collinson have served as consultants to First Medical. References 1. Ottani F, Galvani M, Nicolini FA, Ferrini D, Pozzati A, Di Pasquele G, et al. Elevated cardiac troponin levels predict the risk of adverse outcome in patients with acute coronary syndromes. Am Heart J 2000;140:917–27. 2. Heidenreich PA, Alloggiamento T, Melsop K, McDonald KM, Go AS, Tllatky MA. The prognostic value of troponin in patients with non-ST elevation acute coronary syndromes: a meta-analysis. J Am Coll Cardiol 2001;38:478 – 85. 3. Lindahl B, Diderholm E, Lagerqvist B, Venge P, Wallentin L. Mechanisms behind the prognostic value of troponin T in unstable coronary artery disease: a FRISC II substudy. J Am Coll Cardiol 2001;38:979 – 86. 4. Antman EM. Troponin measurements in ischemic heart disease: more than just a black and white picture. J Am Coll Cardiol 2001;38:1497– 8. 5. Apple FS, Wu AHB. Myocardial infarction redefined: role of cardiac troponin testing. Clin Chem 2001;47:377–9. 6. Apple FS. Cardiac troponin assays: analytical issues and clinical reference range cutpoints. Cardiovasc Toxicol 2001;1:93– 8. 7. Apple FS, Wu AHB, Jaffe AS. European Society of Cardiology and American College of Cardiology guidelines for redefinition of myocardial infarction: how to use existing assays clinically and for clinical trials. Am Heart J 2002;in press. 8. Jaffe AS, Ravkilde J, Roberts R, Naslund V, Apple FS, Galvani M, et al. It’s time for a change to a troponin standard. Circulation 2000;102:1216 –20. 9. Alpert JS, Thygesen K. Myocardial infarction redefined—a consensus document of the Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol 2000;21:959 – 69. 10. Wu AMB, Apple FS, Gibler WB, Jesse RL, Warshaw MM, Valdes R Jr. National Academy of Clinical Biochemistry standards of laboratory practice: recommendations for the use of cardiac markers in coronary artery disease. Clin Chem 1999;45:1104 –21. 11. Hamm CW, Goldmann BU, Heeschen C, Kregmann G, Berger J, Meinertz T. Emergency room triage of patients with acute chest pain by means of a rapid testing for cardiac troponin T or troponin I. N Engl J Med 1997;337:1648 – 53. 12. Apple FS, Anderson FP, Collinson P, Jesse RL, Kontos MC, Levitt MA, et al. Clinical evaluation of the First Medical whole blood, point of cure testing device for detection of myocardial infarction. Clin Chem 2000;46:1604 –9. 13. National Committee for Clinical Laboratory Standards. How to define and determine reference intervals in the clinical laboratory; approved guideline— 2nd edition, Vol. 20, No. 13. Protocol C29 –A2. Wayne, PA: NCCLS, 2000. 14. Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Assoc 1958;53:457– 81. 15. Newby LK, Christenson RH, Ohman EM, Armstrong PW, Thompson TD, Lee KL, et al. Value of serial troponin T measures for early and late risk stratification in patients with acute coronary syndromes. Circulation 1998; 98:1853–9. 16. Newby LK, Storrow AB, Gibler WB, Garvey JL, Tucker JF, Kaplan AL, et al. Bedside multimarker testing for risk stratification in chest pain units: the chest pain evaluation by creatine kinase-MB, myoglobin, and troponin I (CHECKMATE) study. Circulation 2001;103:1832–7. 17. Heeschen C, Deu A, Langenbrink L, Goldmann BU, Hamm CW. Analytical and diagnostic performance of troponin assays in patients suspicious acute coronary syndromes. Clin Biochem 2000;33:359 – 68. 18. Venge P, Lagerqvist B, Diderholm E, Lindahl B, Wallentin L. Clinical performance of three cardiac troponin assays in patients with unstable coronary artery disease (a FRISC II Substudy). Am J Cardiol 2002;89:1035– 41. 19. Morrow DA, Cannon CP, Rifai N, Frey MJ, Vican R, Lakkis N, et al. Ability of minor elevations of troponins I and T to predict benefit from an early invasive strategy in patients with unstable angina and non-ST-elevation myocardial infarction: results from a randomized trial. JAMA 2001;286: 2405–12. 1787 Validation of a Recombinant DNA Construct (LCR and Full-Length -Globin Gene) for Quantification of Human -Globin Expression: Application to Mutations in the Promoter, Intronic, and 5ⴕ- and 3ⴕ-Untranslated Regions of the Human -Globin Gene, Leonid M. Irenge,1 Michel Heusterspreute,1 Marianne Philippe,2 Isabelle Derclaye,1 Annie Robert,3 and Jean-Luc Gala1,4* (1 Applied Molecular Technologies, Center for Human Genetics, Université Catholique de Louvain, Clos-Chapelle-aux-Champs, 30-UCL/30.46, B-1200 Bruxelles, Belgium; 2 Department of Biochemistry, Cliniques Universitaires Saint-Luc, Université Catholique de Louvain, Avenue Hippocrate, 30, B-1200 Bruxelles, Belgium; 3 Biostatistics and Epidemiology, Clos-Chapelle-aux-Champs, 30-UCL/30.34, Université Catholique de Louvain, B-1200 Bruxelles, Belgium; 4 Applied Molecular Technologies, Queen Astrid Military Hospital, Rue Bruyn, 2, B-1120 Bruxelles, Belgium; * address correspondence to this author at: Applied Molecular Technologies, Center for Human Genetics, Clos-Chapelleaux-Champs, 30-UCL/30.46, B-1200 Brussels, Belgium; fax 32-2-764-3959, e-mail gala@lbcm.ucl.ac.be) -Thalassemia is characterized by the reduced production of -globin chains as a result of mutations in the -globin gene (1 ). This reduction is predictable when mutations occur in the coding sequence, but not when they occur in the 5⬘- and 3⬘-untranslated regions (UTRs), the locus control region (LCR), the promoter, or the introns. Whether such mutations are involved in the reduction of the -globin chain production or are simple polymorphisms cannot always be inferred from clinical data. Transient transfection studies with a -globin promoter and an heterologous reporter gene have shown that promoter mutations can decrease transcription (2 ) and are then associated with the -thalassemia phenotype, as illustrated by the ⫺30T3 A mutation (3 ). However, such studies have often failed to provide clear-cut data regarding the transcriptional effect of a mutation or a deletion occurring in a noncoding sequence (4 ), and quantitative data are lacking. To bypass these limitations and to mimic as closely as possible the regulatory mechanisms of -human globin gene expression in vivo, we created a construct (pBLG), in which the entire human -globin gene was cloned behind the -LCR. Whereas previous assays used constructs bearing HS2 as a single LCR enhancer element (5, 6 ), we used the entire -LCR because it has been shown that the other three HS elements play also a key role in -globin transcription (7–11 ). Nucleotides changes in various untranscribed or untranslated parts of the -globin gene representing thalassemic mutations or deletions were introduced in the construct. All the mutations assessed in our study were found in members of proband families presenting with -thalassemia or were created by directed mutagenesis. In addition to the wild type, variant pBLG constructs carrying the following mutations were generated: ⫺101C3 T, ⫹20C3 T, IVS-I-108T3 C, and IVS-I-110G3 A mutations (12–16 ); ⫹10 (-T), ⫹40343, and ⫹156531577 deletions 1788 Technical Briefs (17–19 ); and two novel mutations (⫺223T3 C, and ⫺42C3 G). The ⫺30T3 A thalassemic mutation (3 ) was included as a control. The constructs were expressed in stably transfected mouse erythroleukemia (MEL) cells, and the amount of human -globin mRNA was measured in total RNA extracted from transfected MEL cells grown for 72 h in the presence of 5 mmol/L hexamethylene bisacetamide, a chemical inducer of erythroid differentiation (20 ). Quantification was performed by competitive reverse transcription-PCR, using synthetic calibrator obtained by directed mutagenesis and in vitro transcription. Reverse transcription and coamplification of mRNA extracted from transfected MEL cells and calibrator RNA were performed in the same tubes with various ratios of target to calibrator templates during cDNA synthesis and increasing numbers of PCR cycles during the exponential phase of amplification. After separation on an agarose gel, both DNA bands were photographed and quantified by image analysis software. Target mRNA copy number was calculated based on the number of copies generated in the exponential phase of the PCR. Data collected were analyzed with the Generalized Linear Model program of SPSS Win 10.0TM (SPSS Inc.). For the wild-type and mutated or deleted constructs, the copy number of human -globin mRNA per nanogram of total RNA from MEL cells was submitted to ANOVA with three trial factors (21 ) to assess the variability across PCR cycles (the first trial factor with three PCR cycles as levels), across the amount of calibrator RNA (the second trial factor with six levels), and across transfections (the third trial factor with three experiments as levels). Results are reported as the grand mean ⫾ SD across the levels of each trial factor, with the P value of the F-test. The CV (%) was used to express the variability within each trial factor of each construct. The reliability coefficient of the transfection factor is reported as the overall interassay reproducibility. Contrasts between mean values of -globin mRNA copy numbers were performed with the Scheffé method (21 ). (Details on the materials and methods used are available in a supplemental file accompanying the online version of this Technical Brief at http://www.clinchem.org/content/vol48/issue10/). Human -globin cDNA was consistently amplified from the wild-type construct (Fig. 1), as confirmed by sequence analysis the amplicon. Murine hemoglobin in different MEL cells cultured with hexamethylene bisacetamide as well as quantification of murine glyceraldehyde 3-phosphate dehydrogenase in total RNA were highly reproducible (see supplemental file for additional results). Quantitative data obtained with different constructs are shown in Table 1. Although expression of the ⫺223T3 C construct did not differ from that of the wild type, mild to markedly reduced expression was observed with the other constructs. Accordingly, the novel ⫺223T3 C mutation is a polymorphism as also confirmed by normal biological data in a single heterozygous patient. Despite “silent” phenotypic features (12, 22 ) and previous in vitro data suggesting a lack of binding activity (23, 24 ), the ⫺101C3 T mutation in the distal CACCC box has drastically reduced expression, like the known ⫺30T3 A mutation in the TATA box. These apparently discrepant conclusions lead to several comments: (a) a previous functional assay (12 ) produced in vitro results similar to ours; (b) the human cellular line used to show the lack of binding activity also lacks -globin expression (25, 26 ), suggesting a lack of transcriptional factors essential for -globin expression; (c) several of these factors, such as the erythroid Krüppel-like factor, bind to CACCC and are active at a level that can not be detected by binding assays (27–29 ); (d) whereas mutations in the proximal CACCC box are considered to be more severe, some, like ⫺92C3 T, can also be silent (30 ). Altogether, these data support our in vitro observations in favor of a transcriptional activity of the distal CACCC box rather than the alleged lack of such activity. The current discrepancy between in vitro and in vivo observations could rather be the consequence of a cosegregate mutation located in a negative transcriptional regulator, as suggested by other reports (31, 32 ). The novel ⫺42C3 G mutation has a very mild transcriptional effect. This mutation is located in the -globin direct-repeat element, a highly conserved element found in mammalian -globin promoters (33 ). This is the first report of a mutation in the human -globin direct-repeat element. The observed mild negative transcriptional effect in vitro correlates closely with previous experiments on single mutations in the mouse -globin direct-repeat element (33 ). In our patient, the phenotype observed with ⫺42C3 G/IVS-I-(⫺1)G3 C is comparable to the phenotype reported with ⫹33C3 G/codon 39C3 T mutations (28 ), whereas the IVS-I-(⫺1)G3 C or codon 39C3 T mutations are 0-thalassemia mutations (34 ). Several mutations or deletions found within the 5⬘-UTR are associated with -thalassemia (18 ), but are not always confirmed by transient transfection studies (4 ). Assessment of 5⬘-UTR mutations with this assay brought further insight in understanding of the 5⬘-UTR function and mechanisms of disease. We tested three 5⬘-UTR mutations. In vitro data with ⫹10(-T) pinpoint the lack of transcriptional defect associated with this mutation. This reproduces previous observations and supports the hypothesis that a translational defect may reduce globin chain synthesis in ⫹10(-T) heterozygotes (6 ). The ⫹20C3 T mutation and ⫹40343 deletion showed a twofold decrease in residual activity compared with the wild-type construct. The 5⬘-UTR ⫹20C3 T mutation has been observed only in cis with the IVS-II-745(C3 G) mutation (5 ), as hypothesized several years ago (13 ). Likewise and to the same extent, the 5⬘-UTR deletion ⫹40343 has also been shown to alter the -globin transcription, despite a lack of evidence from previous transient transfection assays (4 ). In addition to those quantitative data, our cell culture expression system was also used to assess the alleged abnormal mRNA splicing of the new IVS-I-108T3 C mutation (15 ). Discrepant conclusions have indeed been drawn regarding the role of the IVS-I-108T3 C mutation 1789 Clinical Chemistry 48, No. 10, 2002 Fig. 1. Amplification of human -globin cDNA and murine -actin performed with primers specific for each transcript. A 375-bp human -globin transcript was consistently amplified from human reticulocytes used as a positive control (huRet; lane 1) and from various cDNA samples from transfected MEL cells (lanes 3–9). No amplification was seen in untransfected MEL cells used as a negative control (Co; lane 2). A 645-bp fragment from murine -actin was amplified from the same cDNA samples (lanes 2–9), but not from human reticulocytes cDNA (lane 2). Perfect identity between the 375-bp amplicons and human -globin transcripts was confirmed by sequence analysis (not shown). (14, 15 ). We found no splicing abnormality in our study, whereas the well-known IVS-I-110G3 A mutation, used as a control, displayed abnormal splicing (16 ) as well as an unexpected retention of IVS-I (see supplemental file for additional results). Sequence analysis of both PCR bands showed either the insertion of 19 intronic nucleotides, as described previously (16 ), or full IVS-I retention. Quantitative data obtained with IVS-I-108T3 C showed de- Table 1. Human -globin mRNA copy number in the MEL cell line stably transfected with various -globin variants: means and CVs per trial factors. Mutation Mean (SD) copy number of target RNA/ng total RNA, ⴛ 105 Wild type 5.89 ⫾ 0.07 ⫺223T3C 5.90 ⫾ 0.10 ⫺42C3G 4.04 ⫾ 0.05 ⫹20C3T 2.97 ⫾ 0.04 ⫺30T3A 0.662 ⫾ 0.014 ⫺101C3T 0.622 ⫾ 0.010 Del ⫹40343 3.14 ⫾ 0.07 Del ⫹10 (⫺T) 5.62 ⫾ 0.08 IVS-I-108T3C 2.78 ⫾ 0.04 Del ⫹156531577 2.10 ⫾ 0.02 Source of variability (3 trial factors) Cycle PCR Calibrator RNA Transfection Cycle PCR Calibrator RNA Transfection Cycle PCR Calibrator RNA Transfection Cycle PCR Calibrator RNA Transfection Cycle PCR Calibrator RNA Transfection Cycle PCR Calibrator RNA Transfection Cycle PCR Calibrator RNA Transfection Cycle PCR Calibrator RNA Transfection Cycle PCR Calibrator RNA Transfection Cycle PCR Calibrator RNA Transfection SD, ⴛ 105 CV, % F-test P 0.10 0.08 0.08 0.15 0.28 0.03 0.09 0.41 0.12 0.12 0.07 0.07 0.04 0.10 0.04 0.02 0.09 0.01 0.06 0.23 0.32 0.04 0.28 0.08 0.04 0.13 0.14 0.01 0.04 0.11 1.6 1.3 1.4 2.5 4.7 0.56 2.3 10 2.9 4.0 2.4 2.5 6.3 15 5.4 3.0 14 1.6 1.8 7.3 10 0.80 5.2 1.3 1.4 4.9 5.1 0.20 1.9 5.4 0.39 0.95 0.52 0.38 0.25 0.75 0.16 ⬍0.001 0.05 0.01 0.60 0.16 0.02 ⬍0.001 0.05 0.17 0.001 0.60 0.28 ⬍0.001 ⬍0.001 0.051 ⬍0.001 0.001 0.33 ⬍0.001 ⬍0.001 0.99 0.94 0.02 1790 Technical Briefs creased -globin expression, which is consistent with the observed thalassemic syndrome and pinpoints the potential role of a currently unknown cis-acting regulatory element in this intron. Current in vitro and phenotypic data highlight the role of IVS-I in -globin gene regulation and open the way to the characterization of as yet uncharacterized cis-acting regulatory elements in this region. Functional effects of 3⬘-UTR mutations were also addressed with our assay. The 3⬘-UTR 13-bp deletion ⫹156531557, previously identified in the single heterozygous mother of a thalassemic Turkish child carrying a compound mutation (19 ), was assessed. The mother presented with a typical thalassemic trait, but no study was performed to assess the impact of this mutation on -globin transcription. In our assay, the deletion showed a strong negative transcriptional effect, consistent with the biological observation and confirming the importance of the 3⬘-UTR in the transcriptional regulation of the -globin gene. In conclusion, the combination of a cell culture expression system and competitive reverse transcription-PCR, as described here, enables one to assess and quantify the expression of wild-type and mutated human -globin genes. A full range of mutations can be introduced within the human -globin gene. Taking advantage of unique or double restriction sites to introduce the mutation allows answers to whether a particular sequence change is a mutation or a silent polymorphism. Accurately measuring the quantitative effect of single nucleotide changes or deletions on -globin gene expression should therefore help to unravel the complex genotype–phenotype relationships in -thalassemia, especially in complex cases of thalassemia intermedia. MEL cell lines and the pBluescript containing the human -globin LCR were kindly provided by Dr. F. Galacteros (Hôpital Henri Mondor, Créteil, France). We thank F. Lemaigre, G. Rousseau (Institute of Cellular Pathology, Brussels, Belgium), B. Lethé (Ludwig Institute for Cancer Research, Brussels, Belgium), and S. Loric (Hôpital St Antoine, Paris, France) for reading the manuscript and for helpful comments. We thank Dr. J. Billiet (AZ Brugge, Brugge, Belgium) for providing some clinical data. References 1. Weatherall DJ, Clegg JB. The thalassemia syndromes, 3rd ed. Oxford: Blackwell Scientific Publications, 1981:148 –78. 2. Takihara Y, Nakamura T, Yamada H, Takagi Y, Fukumaki Y. A novel mutation in the TATA box in a Japanese patient with ⫹-thalassemia. Blood 1986; 67:547–50. 3. Fei YJ, Stoming TA, Efremov GD, Efremov DG, Battacharia R, GonzalezRedondo JM, et al. -Thalassemia due to a T3 A mutation within the ATA box. Biochem Biophys Res Commun 1988;153:741–7. 4. Francès V, Morlé F, Godet J. Functional analysis of the 4 bp deletion identified in the 5⬘ untranslated region of one of the -globin genes from a Chinese -thalassaemic heterozygote. Br J Haematol 1993;84:163–5. 5. Morley BJ, Abbott CA, Wood WG. Regulation of human fetal and adult globin genes in mouse erythroleukemia cells. Blood 1991;78:1355– 63. 6. Ho PJ, Sloane-Stanley J, Athanassiadou A, Wood WG, Thein SL. An in vitro system for expression analysis of mutations of the -globin gene: validation and application to two mutations in the 5⬘ UTR. Br J Haematol 1999;106: 938 – 47. 7. Skarpidi E, Vassilopoulos G, Li Q, Stamatoyannopoulos G. Novel in vitro assay for detection of pharmacologic inducers of fetal hemoglobin. Blood 2000;96:321– 6. 8. Bresnick EH, Tze L. Synergism between hypersensitive sites confers longrange activation by the -globin locus control region. Proc Natl Acad Sci U S A 1997;94:4566 –71. 9. Ellis J, Tan-Un KC, Harper A, Michalovich D, Yannoutsos N, Philipsen S, et al. A dominant chromatin-opening activity in 5⬘ hypersensitive site 3 of the human -globin locus control region. EMBO J 1996;15:562– 8. 10. Bungert J, Tanimoto K, Patel S, Liu Q, Fear M, Engel JD. Hypersensitive site 2 specifies a unique function within the human -globin locus control region to stimulate globin gene transcription. Mol Cell Biol 1999;19:3062–72. 11. Igarashi K, Hoshino H, Muto A, Suwabe N, Nishikawa S, Nakauchi H, et al. Multivalent DNA binding complex generated by small Maf and Bach1 as a possible biochemical basis for -globin locus control region complex. J Biol Chem 1998;273:11783–90. 12. Gonzalez-Redondo JM, Stoming TA, Kutlar A, Kutlar F, Lanclos KD, Howard EF, et al. A C3 T substitution at ⫺101 in a conserved DNA sequence of the promoter of the -globin gene is associated with ‘silent’ -thalassemia. Blood 1989;73:1705–11. 13. Öner R, Agarwal S, Dimovski AJ, Efremov GD, Petkov GH, Altay C, et al. The G3 A mutation at position ⫹22, 3⬘ to the cap site of the -globin gene as a possible cause for a -thalassemia. Hemoglobin 1991;15:67–76. 14. Badens C, Jassim N, Martini N, Mattei JF, Elion J, Lena-Russo D. Characterization of a new polymorphism, IVS-I-108 (T3 C), and a new -thalassemia mutation ⫺27 (A3 T), discovered in the course of a prenatal diagnosis. Hemoglobin 1999;23:339 – 44. 15. Muniz A, Martinez G, Lavinha J, Pacheco P. -Thalassaemia in Cubans: novel allele increases the genetic diversity at the HBB locus in the Caribbean. Am J Hematol 2000;64:7–14. 16. Fukumaki Y, Ghosh PK, Benz EJ Jr, Reddy VB, Lebowitz P, Forget BG, et al. Abnormally spliced messenger RNA in erythroid cells from patients with ⫹ thalassemia and monkey cells expressing a cloned ⫹-thalassemic gene. Cell 1982;28:585–93. 17. Athanassiadou A, Papachatzopoulou A, Zoumbos N, Maniatis GM, Gibbs R. A novel -thalassaemia mutation in the 5⬘ untranslated region of the -globin gene. Br J Haematol 1994;88:307–10. 18. Huang ZH, Xu YH, Zeng FY, Wu DF, Ren ZR, Zeng YT. A novel -thalassaemia mutation: deletion of a 4 bp (-AAAC) in the 5⬘ transcriptional sequence. Br J Haematol 1991;78:125– 6. 19. Basak AN, Özer A, Kirdar B, Akar N. A novel 13 bp deletion in the 3⬘UTR of the -globin gene causes -thalassemia in a Turkish patient. Hemoglobin 1993;17:551–5. 20. Campbell PL, Kulozik AE, Woodham JP, Jones RW. Induction by HMBA and DMSO of genes introduced into mouse erythroleukemia and other cell lines by transient transfection. Genes Dev 1990;4:1252– 66. 21. Fleiss JL. The design and analysis of clinical experiments. New-York: John Wiley, 1986:433pp. 22. Maragoudaki E, Kanavakis E, Traeger-Synodinos J, Vrettou C, Tzetis M. Molecular, haematological and clinical studies of the ⫺101C3 T substitution of the -globin gene promoter in 25 -thalassaemia patients and 45 heterozygotes. Br J Haematol 1999;107:699 –706. 23. Baysal E, Ribeiro MLS, Huisman THJ. Binding of nuclear factors to the proximal and distal CACCC motifs of the -globin gene promoter: implications for the ⫺101C3 T “silent” -thalassemia mutation. Acta Hematol 1994;91:16 –20. 24. Dierks P, van Ooyen A, Cochran MD, Dobkin C, Reiser J, Weissmann C. Three regions upstream from the cap site are required for efficient and accurate transcription of the rabbit -globin gene in mouse 3T6 cells. Cell 1983;32:695–706. 25. Enver T, Zhang J, Anagnou NP, Stamatoyannopoulos G, Papayannopoulou T. Developmental programs of human erythroleukemia cells: globin gene expression and methylation. Mol Cell Biol 1988;8:4917–26. 26. Martin P, Papayannopoulou T. HEL cells: a new human erythroleukemia cell line with spontaneous and induced globin expression. Science 1982;216: 1233–5. 27. Hartzog GA, Myers RM. Discrimination among potential activators of the -globin element by correlation of binding and transcriptional properties. Mol Cell Biol 1993;13:44 –56. 28. Miller IJ, Bieker JJ. A novel, erythroid cell-specific murine transcription factor that binds to the CACCC element and is related to the Krüppel family of nuclear proteins. Mol Cell Biol 1993;13:2776 – 86. 29. Perkins A. Erythroid Kruppel like factor: from fishing expedition to gourmet meal. Int J Biochem Cell Biol 1999;31:1175–92. 30. Rosatelli MC, Faa V, Meloni A, Fiorenza F, Galanello R, Gasperini D, et al. A promoter mutation C3 T at position ⫺92, leading to silent -thalassaemia. Br J Haematol 1995;90:483–5. 31. Samakoglu S, Philipsen S, Grosveld F, Lüleci G, Bagci H. Nucleotide changes in the ␥-globin promoter and (AT)xNy(AT)z polymorphic sequence of LCRHS-2 region associated with altered levels of HbF. Eur J Hum Genet 1999;7:345– 6. Clinical Chemistry 48, No. 10, 2002 32. Perichon B, Ragusa A, Lapoumeroulie C, Romand A, Moi P, Ikuta T, et al. Inter-ethnic polymorphism of the -globin locus control region (LCR) in sickle cell anemia patients. Hum Genet 1993;91:464 – 8. 33. Stuvé LL, Myers RM. A directly repeated sequence in the -globin promoter regulates transcription in murine erythroleukemia cells. Mol Cell Biol 1990;10:972– 81. 34. Huisman THJ, Carver MFH, Baysal E. A syllabus of thalassemia mutations. Augusta, GA: The Sickle Cell Anemia Foundation, 1997:29pp. Influence of Lepirudin, Argatroban, and Melagatran on Prothrombin Time and Additional Effect of Oral Anticoagulation, Tivadar Fenyvesi, Ingrid Joerg, and Job Harenberg* (Fourth Department of Medicine, University Hospital Mannheim, Ruprecht-Karls-University Heidelberg, Theodor-Kutzer-Ufer 1, 68167 Mannheim, Germany; * author for correspondence: fax 49-621-383-3308, e-mail j-harenberg@t-online.de) Oral anticoagulation (OAC) with coumarin derivatives decreases the activities of coagulation factors II, VII, IX, and X by inhibiting their vitamin K-dependent carboxylation (1 ). The effectiveness and safety of therapy with oral anticoagulants for primary or secondary prophylaxis of thromboembolism are usually monitored by the prothrombin time (PT), expressed as international normalized ratio (INR), prothrombin ratio, or percentage of normal (2, 3 ). INR was standardized through large international reference studies (4 –7 ). The direct thrombin inhibitors (DTIs) lepirudin and argatroban are used to achieve effective anticoagulation in patients with heparin-induced thrombocytopenia with or without thrombosis (type II) (8 –10 ). Melagatran is currently under investigation in clinical trials (11–14 ). DTIs prolong clotting times in PT assays and therefore interfere with oral anticoagulants (15–18 ). During treatment of deep venous thrombosis, heparins or DTIs are switched to oral anticoagulants. During treatment for invasive diagnostics or surgery, patients on oral anticoagulant therapy may temporarily be switched to a DTI. Decreased thrombin activity in the plasma of these patients leads to prolongations of the PT (15, 16, 18 ). These additive effects make it difficult to adjust dosage of either of the drugs during concomitant use. In the case of heparins, additive effects are antagonized by addition of protamine or heparinase to PT reagents (19 ). For DTIs, such antagonists are missing. Antibodies against hirudin have been unsuitable for neutralizing the drug’s anti-factor IIa effects because of polyclonality, producing neutralizing or enhancing antibodies, depending on the individual (20, 21 ). Argatroban and melagatran are small molecules and have not been reported to be antigenic. Without the ability to eliminate the additive effects of DTIs and oral anticoagulants on PT, it is important to address the issue of handling these interactions in clinical practice and to individually investigate them for each drug in vitro and ex vivo. 1791 Here we describe the additive and synergistic actions of the DTIs lepirudin, argatroban, and melagatran on the effects of the oral anticoagulant phenprocoumon on PT. These synergisms interfere with the analysis and dose adjustment of oral anticoagulants during concomitant therapy periods. Data were derived from plasma from healthy volunteers and from patients treated with the vitamin K antagonist phenprocoumon. Blood from 6 healthy volunteers and 10 patients undergoing treatment with the vitamin K antagonist phenprocoumon (Hoffmann-La Roche) was collected by clean cubital vein puncture into plastic vials containing 38 mL/L sodium citrate (9 mL of plasma in 1 mL of citrate). All donors (volunteers and patients) gave informed consent in accordance with the current revision of the Helsinki Declaration. After centrifugation (1800g for 10 min), plasma samples were shock frozen in liquid nitrogen, stored at ⫺80 °C, and analyzed within 4 weeks. After thawing, plasma samples were supplemented with lepirudin (molecular mass ⬃6500 Da; obtained from Aventis) and argatroban (molecular mass 526.7 Da; kindly provided by Mitsubishi Chemical Corp., Tokyo, Japan) in concentrations ranging from 300 to 3000 g/L. Melagatran (molecular mass 473.6 Da; courtesy of Astra Zeneca, Mölndal, Sweden) was added at lower concentrations, between 30 and 1000 g/L, because of its higher gravimetric potency observed in preliminary experiments. Clotting time measurements were carried out in a KC 10a microdevice (22 ) from Amelung Co. PT was determined with a recombinant thromboplastin reagent (Aventis Behring; lot number 526935; international sensitivity index ⫽ 1.09). With this thromboplastin reagent, clotting times can be determined up to ⬃600 s with this device. Interassay CVs were 10%, 8.7%, and 9.9% at clotting times of 10, 50, and 300 s, respectively (n ⫽ 12). To start the clotting time assay, 50 L of plasma was incubated at 37 °C for 3 min (micromethod). To initiate clot formation, 100 L of PT reagent (dissolved according to the manufacturer’s instructions) was added. The clotting times (PT) were transformed into INRs with an equation appropriate for the KC 10a device, obtained from the manufacturer of the thromboplastin reagent: PT (in seconds) ⫻ 0.09 ⫹ 0.2 ⫽ INR. The mean value obtained for the healthy volunteers was 10.2 ⫾ 0.3 s, corresponding to an INR range of 1.1 ⫾ 0.03. All data are presented as the mean ⫾ SD. Calculation factors (ng ⫻ factor ⫽ nmol/L) for transformation of the data from gravimetric scaling to an equimolar scale were 0.154 for lepirudin, 1.901 for argatroban, and 2.11 for melagatran, respectively. For reverse transformation, the factors were 6.5 for lepirudin, 0.526 for argatroban, and 0.474 for melagatran. The PT was prolonged in OAC plasma (OACP; samples from patients undergoing a stable phase of OAC therapy) to 26.0 ⫾ 5.0 s. All DTIs prolonged PT values in a concentration-dependent manner in plasma from the controls and patients receiving OAC therapy. The results are displayed in Fig. 1 in double scaling (nmol/L and g/L). In Fig. 1, the upper therapeutic gravimetric concentrations