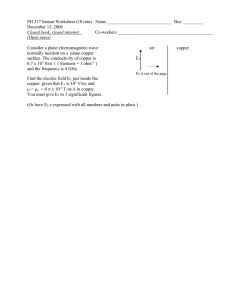
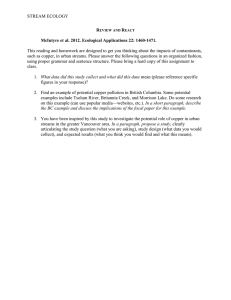
Hematopathology / ZINC-INDUCED COPPER DEFICIENCY Zinc-Induced Copper Deficiency A Report of Three Cases Initially Recognized on Bone Marrow Examination Monte S. Willis, MD, PhD,1 Sara A. Monaghan, MD,1 Michael L. Miller, DO,1 Robert W. McKenna, MD,1 Wiley D. Perkins, MD,2 Barry S. Levinson, MD,2 Vikas Bhushan, MD,2 and Steven H. Kroft, MD1 Key Words: Zinc toxicity; Copper deficiency; Cytoplasmic vacuoles; Sideroblastic anemia; Ringed sideroblasts DOI: 10.1309/V6GVYW2QTYD5C5PJ Copper deficiency is a rare cause of sideroblastic anemia and neutropenia that often is not suspected clinically. The morphologic findings in bone marrow, while not pathognomonic, are sufficiently characteristic to suggest the diagnosis, leading to further testing to establish the correct diagnosis. Excess zinc ingestion is among the causes of copper deficiency. We present 3 cases of zinc-induced copper deficiency in which the diagnosis first was suggested on the basis of bone marrow examination. The first patient was a 47-yearold man with a debilitating peripheral neuropathy that had progressed during the previous 18 months, mild anemia, and severe neutropenia. The second was a 21-year-old man receiving zinc supplementation for acrodermatitis enteropathica in whom moderate normocytic anemia and neutropenia developed. The third patient was a 42-year-old man with anemia, severe neutropenia, and a peripheral neuropathy that had progressed during 8 months. The bone marrow findings in all cases suggested copper deficiency, which was confirmed by further laboratory testing and determined to be due to zinc excess. The morphologic features, clinical manifestations, differential diagnosis, and pathogenetic mechanisms are discussed. Copper deficiency is a rare cause of anemia and neutropenia that is characterized morphologically by cytoplasmic vacuolization in erythroid and myeloid precursors and ringed sideroblasts. There are a variety of causes of copper deficiency, including dietary deficiency, hypoproteinemic states (kwashiorkor, celiac disease, tropical and nontropical sprue, idiopathic hypoproteinemia, and enteropathy in infancy), excess excretion (nephrotic syndrome), Wilson disease, Menkes syndrome, and excess ingestion of zinc.1 Given its low prevalence and nonspecific hematologic and clinical manifestations, the diagnosis of copper deficiency might be delayed. The bone marrow morphologic manifestations of copper deficiency are not widely appreciated. While not pathognomonic, the morphologic features are highly characteristic and might permit early diagnosis and correction of the deficiency state. We describe 3 patients with zinc-induced copper deficiency in whom the correct diagnosis first was suggested on the basis of bone marrow findings. Case Reports Case 1 A 47-year-old man initially sought care from his primary care physician in December 1999 because of the onset of progressive numbness and weakness in his lower extremities. Laboratory testing detected severe macrocytic anemia and leukopenia, and the patient was hospitalized. A serum B12 level was found to be low, and, therefore, the hematologic and neurologic manifestations were thought to be due to B12 deficiency. However, despite continued vitamin B12 treatment, he Am J Clin Pathol 2005;123:125-131 © American Society for Clinical Pathology 125 DOI: 10.1309/V6GVYW2QTYD5C5PJ 125 125 Downloaded from http://ajcp.oxfordjournals.org/ by guest on September 30, 2016 Abstract Willis et al / ZINC-INDUCED COPPER DEFICIENCY Copper supplementation for this patient was delayed for 3 months, and in August 2002, the patient’s blood counts had not changed significantly from his previous visits, with a WBC count of 1,800/µL (1.8 × 109/L), a hemoglobin concentration of 11.6 g/dL (116 g/L), an RBC distribution width of 19.8%, and a platelet count of 501 × 103/µL (501 × 109/L). The sensory neuropathy in his legs and loss of strength continued to progress. In October 2002, 2 months after the initiation of copper supplementation, his blood counts returned to normal, with a WBC count of 7,100/µL (7.1 × 109/L), a hemoglobin concentration of 14.1 g/dL (141 g/L), RBC distribution width of 12.8%, and a platelet count of 322 × 103/µL (322 × 109/L; down from 501 × 103/µL [501 × 109/L]). However, no improvement in his peripheral neuropathy or loss of strength was observed. Case 2 This 21-year-old man was given a diagnosis of acrodermatitis enteropathica 5 years previously for which he was receiving therapeutic zinc supplementation. He sought care at the emergency department complaining of a 2- to 3-week history of fatigue and new onset fever (40.6°C). At the time of admission, the patient was taking approximately 600 mg/d of zinc, which was several times the dosage prescribed by his physician. ❚Table 1❚ Initial Patient Laboratory Values Test WBC count, /µL (× 109/L) Absolute count, /µL (× 109/L) Neutrophils Lymphocytes Monocytes Eosinophils Basophils RBC count, × 106/µL (×1012/L) Hemoglobin, g/dL (g/L) Hematocrit, % Mean corpuscular volume, µm3 (fL) Mean corpuscular hemoglobin concentration, g/dL (g/L) RBC distribution width (%) Reticulocyte count, % Absolute reticulocyte count, × 103/µL (× 109/L) Platelet count, ×103/µL (×109/L) Zinc, µg/dL (µmol/L) Serum copper, µg/dL (µmol/L) Urine copper (U/24 h) Ceruloplasmin, mg/dL (mg/L) Iron, µg/dL (µmol/L) Total iron binding capacity, µg/dL (µmol/L) Transferrin saturation (%) Ferritin, ng/mL (µg/L) Vitamin B12, pg/mL (pmol/L) Folate, serum, ng/mL (nmol/L) Homocysteine, mg/L (µmol/L) Case 1 Case 3 Reference Range Case 2 Reference Range 2,100 (2.1) 2,100 (2.1) 4,100-11,100 (4.1-11.0) 1,600 (1.6) 4,000-11,000 (4.0-11.0) 388 (0.4) 1,313 (1.3) 252 (0.25) 42 (0.04) 105 (0.11) 3.22 (3.2) 9.8 (98) 36.1 (0.36) 101 (101) 29.8 (298) 483 (0.5) 945 (0.9) 546 (0.55) 105 (0.11) 21 (0.02) 3.44 (3.4) 0.8 (80) 30.8 (0.31) 89.4 (89) 32.3 (323)* 2,000-7,500 (2.0-7.5) 900-4,700 (0.9-4.7) 100-900 (0.10-0.90) 0-500 (0.00-0.50) 0-200 (0.00-0.20) 4.27-5.99 (4.3-6.0) 13.2-16.9 (132-169) 39.6-50.2 (0.40-0.50) 82-105 (82-105) 31.6-35.4 (316-354) 512 (0.5) 752 (0.8) 240 (0.24) 64 (0.64) 32 (0.03) 4.2 (4.2) 8.5 (85) 25.5 (0.25) 92 (92) ND 2,400-7,400 (2.4-7.4) 1,000-4,000 (1.0-4.0) 100-800 (0.10-0.80) 0-450 (0.00-0.45) 0-180 (0.00-0.18) 4.27-5.99 (4.3-6.0) 13.5-17.5 (135-175) 39.6-50.2 (0.40-0.50) 80-100 (80-100) — 21.7 1.3 41.9 (42) 16.2* 0.8* 27.9 (28)* <14.5 0.5-2.8 32-147 (32-147) ND ND ND — — — 488 (488) 193 (29.5) 8 (1.3) 6 1.8 (18) 32 (5.7) 361 (64.6) 211 (211) 428 (65.5)* <10 (<1.6)* ND 1.1 (11)* 49 (8.8)* 589 (105.4)* 140-450 (140-450)† 66-110 (10.1-16.8) 70-145 (11.0-22.8) 15-60 22.9-43.1 (229-431) 60-200 (10.7-35.8) 262-474 (46.9-84.8) 209 (209) 145 (22.2) <15 (<2.4) ND <2 (<20) 5 (0.9) 224 (40.1) 150-400 (150-400) 55-150 (8.4-23.0) 70-140 (11.0-22.0) — 21-45 (210-450) 30-140 (5.4-25.1) 262-474 (46.9-84.8) 9 252 (252) 277 (204) 5.8 (13) 0.65 (4.8) 8* 170 (170)* 484 (357)* 17.9 (41)* 1.37 (10.1)* 20-50 22-300 (22-300)† 211-911 (156-672) 2.8-18.0 (6-41)† 0.68-2.03 (5.0-15.0)† 2 444 (444) 301 (222) 8.0 (18) ND 20-50 18-300 (18-300) 211-911 (156-672) 2.8-18.0 (6-41) — ND, not done. * Performed 24 days after initial bone marrow examination. † Reference ranges for case 3 were as follows: platelet count, 174-404 × 103/µL (174-404 × 109/L); ferritin, 10-322 ng/mL (10-322 µg/L); folate, 5.3-24.0 ng/mL (12-54 nmol/L); homocysteine, 0.68-1.88 mg/L (5.0-13.9 µmol/L). 126 126 Am J Clin Pathol 2005;123:125-131 DOI: 10.1309/V6GVYW2QTYD5C5PJ © American Society for Clinical Pathology Downloaded from http://ajcp.oxfordjournals.org/ by guest on September 30, 2016 continued to have difficulties with balance and numbness in his lower extremities. Between the December 1999 hospitalization and August 2000, the patient’s neuropathy progressed to the point at which he became wheelchair-dependent. In May 2001, the patient no longer ambulated and used a scooter owing to bilateral flexion contractures. During this time, he received regular vitamin B12 injections, and his vitamin B12 levels were in the normal range. A bone marrow biopsy performed in January 2001 demonstrated a mildly hypocellular bone marrow with normal trilineage hematopoiesis. The patient was seen again 1 year later, and at that time, he had normocytic anemia with neutropenia ❚Table 1❚. A second bone marrow examination was performed in May 2002, and, based on the morphologic findings, serum copper, ceruloplasmin, and zinc levels were obtained (Table 1). Marked decreases in serum copper and ceruloplasmin levels were detected, along with an elevated serum zinc concentration. The results of antigliadin and antiendomysial antibody testing to rule out celiac sprue were negative. The results of vitamin B12 and folate studies were normal (Table 1). Serum iron was low, but total iron-binding capacity and ferritin levels were within normal ranges (Table 1). The cause of the zinc excess remains undetermined. Hematopathology / ORIGINAL ARTICLE Case 3 This 42-year-old man initially sought care from his primary care physician in August 2003 because of ascending tingling and numbness in his lower extremities, which later progressed to his fingertips. His symptoms continued to progress, and by January 2004, he had difficulty walking with a steady gait and holding objects in his hands owing to the lack of sensation. Nerve conduction studies revealed evidence of sensory neuropathy. However, the patient was noted at this time to be anemic and neutropenic (Table 1) and a bone marrow evaluation was performed in March 2004. After an initial interpretation of myelodysplastic syndrome was given at an outside hospital, the patient was referred to our institution for evaluation. Based on our review of the bone marrow biopsy specimen, additional laboratory testing was obtained, which revealed serum copper levels below the detectable range, extremely low ceruloplasmin levels, and high zinc levels (Table 1). The patient was asked further about possible zinc ingestion, and it was determined that he had been consuming an entire tube (68 g) of PoliGrip denture cream (containing polymethyvinylether maleic acid calcium-zinc salt) daily for the past 4 to 5 years. The patient was using the denture adhesive for his dentures and additionally eating “pellets” of it from the tube. The patient was advised to stop ingesting the denture cream, and copper sulfate supplementation was initiated. Approximately 3 weeks after the initiation of treatment, the patient’s serum copper levels increased to 20 µg/dL (3.1 µmol/L), and his hematologic values normalized completely (hemoglobin level, 13.0 [130 g/dL]; hematocrit, 39.9 [0.40]; WBC count, 7,900/µL [7.9 × 109/L]). However, the neuropathy showed no improvement. Materials and Methods Bone marrow core specimens were fixed in B-5 or Zenker solution, washed, decalcified, and processed. Paraffin-embedded sections of the core biopsy (4 µm sections) were stained with H&E. Direct smears, particle crush, buffy coat, and touch preparations were prepared and stained with Wright or WrightGiemsa and Prussian blue stains as previously described.3,4 Results Peripheral Blood Smears The peripheral blood smears in all cases demonstrated RBC changes. In case 1, the RBCs exhibited dimorphism with a minor population of microcytic, hypochromic RBCs, as well as scattered dacryocytes, target cells, and elliptocytes ❚Image 1A❚. The peripheral blood sample in case 2 showed less distinct RBC dimorphism but more pronounced anisopoikilocytosis, including variable hypochromia, dacryocytes, elliptocytes, and target cells ❚Image 1B❚. The peripheral blood sample in case 3 demonstrated nonspecific anisopoikilocytosis with occasional elliptocytes and dacryocytes. Although each patient was neutropenic, the WBC morphologic features were normal. The platelets in all cases were numerically and morphologically normal. Bone Marrow Aspirates In all 3 cases, the bone marrow aspirates demonstrated left-shifted granulocytic maturation with vacuolization of early granulocytes (myelocytes and promyelocytes) ❚Image 2❚. The shift to immaturity was most pronounced in case 1, in which there was little maturation beyond the myelocyte stage. The vacuoles ranged from 1 to 3 µm in size and were present in 18%, 21%, and 20% of granulocytes (mainly myelocytes) in cases 1 through 3, respectively. We found 3 to 12 vacuoles present in a given cell, generally 5 to 7 per cell in case 1 and 7 to 10 in cases 2 and 3. Myeloblasts were not increased in any case. However, subtle morphologic abnormalities were present in the maturing granulocytes, consisting mainly of dyssynchronous maturation with chromatin maturation lagging behind nuclear conformation. Left-shifted maturation, mild megaloblastoid changes, and mild terminal dyserythropoiesis were identified in the erythroid lineage in the bone marrow aspirates in each case (Image 2). The myeloid/erythroid ratios were 1.1:1, 2.1:1, and 1.3:1 in cases 1 through 3, respectively. Vacuoles ranging from 1 to 2 µm, mostly restricted to basophilic normoblasts and pronormoblasts, were present in 11%, 7%, and 37% of the erythroid precursors in cases 1 through 3, respectively. The number of vacuoles per erythroid cell ranged from 2 to 12 and most commonly numbered around 5 per cell. Megakaryocytes were normal in number and morphologic features in all cases. Iron staining of the aspirate smear with Prussian blue demonstrated the presence of storage iron and Am J Clin Pathol 2005;123:125-131 © American Society for Clinical Pathology 127 DOI: 10.1309/V6GVYW2QTYD5C5PJ 127 127 Downloaded from http://ajcp.oxfordjournals.org/ by guest on September 30, 2016 Laboratory testing revealed moderate normocytic anemia, leukopenia with severe neutropenia, and a normal platelet count (Table 1). Based on the morphologic examination of a bone marrow specimen, serum ceruloplasmin, copper, and zinc levels were obtained. The serum copper and ceruloplasmin were found to be extremely low, and the zinc level was high normal (Table 1). The patient stopped taking the zinc supplements before his hospital discharge and had a spontaneous recovery of his WBC count and hemoglobin level. One week after discharge, he had a WBC count of 2,100/µL (2.1 × 109/L) with 48% neutrophils (0.48), a hemoglobin concentration of 8.4 g/dL (84 g/L), and a platelet count of 297 × 103/µL (297 × 109/L). The patient was followed up by the gastrointestinal service to ensure a safe level of zinc supplementation. After 6 weeks, all hematologic values were within the normal range. This case has been reported previously in the ASCP Check Sample Program.2 Willis et al / ZINC-INDUCED COPPER DEFICIENCY A B A B ❚Image 2❚ Example of morphologic changes in marrow precursors in copper deficiency. A, Vacuolization of immature granulocytes. Mild dyssynchrony in nuclear maturation also is present. B, Vacuolization of an early myelocyte (lower left) and an early basophilic normoblast (upper right). In addition, mild megaloblastoid/macronormoblastic changes are evident in several late-stage erythroid precursors. C, Vacuolization in 2 pronormoblasts (A-C, Wright-Giemsa, ×330). C 128 128 Am J Clin Pathol 2005;123:125-131 DOI: 10.1309/V6GVYW2QTYD5C5PJ © American Society for Clinical Pathology Downloaded from http://ajcp.oxfordjournals.org/ by guest on September 30, 2016 ❚Image 1❚ Peripheral blood RBC morphologic features in patients with copper deficiency. A (Case 1), Dimorphic RBC morphologic features are evident, with a minor population of microcytic/hypochromic erythrocytes. There also is mild anisopoikilocytosis with scattered elliptocytes and dacryocytes (Wright-Giemsa, ×165). B (Case 2), Although RBC dimorphism is not apparent, there is more pronounced anisopoikilocytosis with scatted elliptocytes and dacryocytes (Wright, ×165). Hematopathology / ORIGINAL ARTICLE sideroblastic iron with scattered ringed sideroblasts (5% and 4% of erythroid precursors in cases 1 and 2, respectively) ❚Image 3❚. No stainable storage iron was identified in several particles in case 3, but sideroblasts were identified easily, and ringed sideroblasts constituted 2% of the erythroid precursors. A B Trephine Biopsy Specimens The trephine biopsy specimen from case 1 was mildly hypocellular for age (~35%-40% cellularity; age 47 years) but otherwise was morphologically unremarkable with the exception of the presence of multiple lipogranulomas. The trephine biopsy specimen from case 2 was unavailable for review. The trephine biopsy specimen from case 3 was normocellular for age (~50% cellularity; age 42 years) and was morphologically unremarkable. We describe 3 patients with zinc-induced copper deficiency in whom the diagnosis first was suggested based on characteristic bone marrow findings. These findings include vacuolization of granulocytic and erythroid precursors and the presence of ringed sideroblasts. The serum copper level was decreased in each patient. In addition, an increased serum zinc level or a history of excessive zinc intake was present, implicating zinc-induced copper deficiency as the likely cause of the neutropenia and anemia. The hematologic findings that have been reported in copper deficiency include anemia with neutropenia5 and pancytopenia.6-8 Microcytic, normocytic, and macrocytic anemias have been described.9-15 The 3 cases presented herein demonstrated normocytic (cases 2 and 3) and macrocytic (case 1) anemia at initial examination. In the cases in which trephine biopsy specimens were available, mild hypocellularity (case 1) and normal marrow cellularity (case 3) were noted. As in the present cases, previous reports have described various hematologic abnormalities in zinc-induced copper deficiency, including vacuolization of erythroid and myeloid precursors, megaloblastic changes, and ringed sideroblasts.14,15 Dyserythropoiesis, dysmyelopoiesis, and prominent hemosiderin characteristic of myelodysplastic syndrome also have been reported.15 One of the patients described herein initially was given a diagnosis of a myelodysplastic syndrome. Bone marrow biopsy specimens in zinc-induced copper deficiency might be hypercellular, normocellular, or hypocellular,14 although hypercellularity has been a rare finding among the reported cases.16 Copper has an essential role in several enzymatic reactions in RBCs, and copper deficiency interferes with iron transport and utilization and, therefore, with heme synthesis. Specifically, ceruloplasmin (which incorporates copper) is a ferroxidase that converts ferrous (+2) to ferric (+3) iron, allowing it to bind transferrin and be transported. The copperdependent enzyme cytochrome-c oxidase also is required for the reduction of ferric iron to incorporate it into the heme molecule.17,18 In addition to interference with heme synthesis, there is approximately 85% reduction of superoxide dismutase in the RBC membrane in copper deficiency, which decreases RBC survival time.19 The mechanism for neutropenia in copper deficiency is unknown; neutropenia has been demonstrated experimentally in copper-deficient mice and is associated with arrested maturation.20 Knowledge of the details of the mechanism(s) by which copper is absorbed from the diet is incomplete. In physiologic ranges of intake, absorption occurs in the small intestine, and the amount absorbed depends on the copper content in the diet.21 Copper absorption occurs by the ATP7A protein on the basolateral surface of enterocytes; it is this protein that is defective in patients with Menkes disease, who cannot absorb copper.21 When large doses of copper are ingested over long periods, other mechanisms of uptake occur, involving the intracellular ligand metallothionein (MTO). MTO has a high affinity for transition metals, forming mercaptide bonds by its multiple cysteine residues.22 Multiple mechanisms have been proposed for the ability of zinc to interfere with the absorption of copper in enterocytes of the small intestine. Excess zinc levels induce the synthesis of the intracellular ligand MTO in enterocytes, which then binds zinc. The excess zinc bound to MTO then is excreted in the feces through enterocyte shedding. However, copper, with its higher affinity for MTO, displaces zinc and also is excreted, reducing the amount of copper delivered to the enterocyte.23 The exact mechanisms by which copper is absorbed, however, are just beginning to be elucidated. Am J Clin Pathol 2005;123:125-131 © American Society for Clinical Pathology 129 DOI: 10.1309/V6GVYW2QTYD5C5PJ 129 129 Downloaded from http://ajcp.oxfordjournals.org/ by guest on September 30, 2016 Discussion ❚Image 3❚ Two late-stage ringed sideroblasts (A and B, Prussian blue, ×330). Willis et al / ZINC-INDUCED COPPER DEFICIENCY 130 130 Am J Clin Pathol 2005;123:125-131 DOI: 10.1309/V6GVYW2QTYD5C5PJ causes of SA, including copper deficiency. Resolution of the hematologic changes found in alcoholic patients after alcohol abstinence occurs in days to weeks.38 Treatment with the tuberculosis medications isoniazid, pyrazinamide, or cycloserine also can result in an SA. A microcytic anemia and dimorphic RBC population also might accompany SA in this setting. Although most patients taking isoniazid are given supplemental vitamin B6, this finding is not seen commonly. Chloramphenicol can cause a reduction in erythropoietic activity and maturation. Bone marrow evaluation might identify vacuolization of the erythroid and granulocytic precursors with a maturation arrest at the proerythoblast stage. Aplastic anemia also can occur due to chloramphenicol use, with resultant pancytopenia. RARS is characterized by the insidious onset of moderate macrocytic or normocytic anemia with hypochromic or normochromic, often dimorphic, RBCs. It generally is found in patients older than 50 years. By definition, neutropenia and thrombocytopenia are not features of RARS, and, in fact, thrombocytosis sometimes is identified.40 Dyserythropoiesis with normal granulopoiesis and megakaryocytopoiesis generally are present.40 By definition, myeloblasts are fewer than 5% and ringed sideroblasts represent at least 15% of erythroid precursors; bone marrow iron stores usually are increased. We reported 3 cases of zinc-induced copper deficiency resulting in neutropenia, anemia, and severe progressive peripheral neuropathy (cases 1 and 3). The bone marrow manifestations of copper deficiency are characteristic, although not pathognomonic. It is important for pathologists to be aware of these rather subtle morphologic features in order to initiate timely laboratory evaluation to help reverse the cytopenias and prevent the progression of the neuropathy. From the Departments of 1Pathology and 2Internal Medicine, University of Texas Southwestern Medical Center, Dallas. Address reprint requests to Dr Kroft: Dept of Pathology, University of Texas Southwestern, 5323 Harry Hines Blvd, Dallas, TX 75390-9072. References 1. Lee GR, Herbert V. Nutritional factors in the production and function of erythrocytes. In: Lee GR, ed. Wintrobe’s Clinical Hematology. 10th ed. Baltimore, MD: Lippincott Williams & Wilkins; 1999:228-266. 2. Smith TA, Overmoyer BA, Miller ML. Sideroblastic anemia due to zinc-induced copper deficiency. Clinical Hematology Check Sample CH 98-6. Chicago, IL: ASCP Press; 1998;4:8195. 3. Brynes RK, McKenna RW, Sundberg RD. Bone marrow aspiration and trephine biopsy: an approach to a thorough study. Am J Clin Pathol. 1978;70:753-759. 4. Kaplan E, Zuelzer WW, Mouriquand C. Sideroblasts: a study of stainable nonhemoglobin in marrow normoblasts. Blood. 1954;9:203-213. © American Society for Clinical Pathology Downloaded from http://ajcp.oxfordjournals.org/ by guest on September 30, 2016 Acrodermatitis enteropathica, which patient 2 had, is a rare autosomal recessive disorder characterized by the inability to absorb sufficient zinc from the diet. The most dramatic manifestations of acrodermatitis enteropathica are vesiculobullous, eczematous, dry, scaly, or psoriasiform skin lesions and kinky hair. Typically prescribed dosages of zinc range from 50 to 150 mg/d. Patient 2 reported ingesting an average of 600 mg/d of zinc to “control his symptoms.” Excess zinc ingestion also can occur in patients taking zinc therapeutically for decubitus ulcer healing, celiac disease, glucagonoma, hepatic encephalopathy, acne,24,25 and for reducing the duration of symptoms of the common cold.26-28 The ingestion of coins by psychiatric patients also has been reported as a source of increased zinc ingestion (leached from the coins) and subsequent copper deficiency.25,29,30 Since 1982, pennies have been composed of 97.6% zinc and 2.4% copper; other US coins do not contain zinc.29 Copper deficiency due to long-term hyperalimentation without trace mineral supplementation has been reported,7,31-34 as have 3 cases due to intestinal malabsorption after partial gastrectomy.15,35,36 Idiopathic hyperzincemia and hypocupremia associated with extensive central nervous system demyelination, similar to that seen in case 1, recently was reported for the first time.37 Furthermore, irreversible demyelination has been reported even after copper levels were stabilized through supplementation, although serum zinc levels remained high (unknown cause). In addition, 2 previous descriptions of patients with copper deficiency and concomitant severe progressive peripheral neuropathy have been reported.15,36 In both of these cases, copper supplementation improved the hematologic symptoms; however, the neuropathies were irreversible. The differential diagnosis of copper deficiency with ringed sideroblasts includes other forms of sideroblastic anemia (SA). SAs are a group of disorders having in common defects in iron utilization and heme synthesis, resulting in the accumulation of storage iron and abnormal iron deposition in mitochondria; inherited and acquired forms have been described. Inherited forms are rare and have variable but persistent manifestations throughout life. Acquired SA can be caused by chronic alcohol abuse, medications used to treat tuberculosis, chloramphenicol toxicity, lead poisoning, and copper deficiency. Moreover, refractory anemia with ringed sideroblasts (RARS; a myelodysplastic syndrome) also is classified as an SA. A patient’s history and hematologic parameters, as well as blood and bone marrow morphologic examination, are important in distinguishing these types of SAs, because all except RARS are reversible if accurately diagnosed and treated. It is estimated that approximately 25% of alcoholic patients have ringed sideroblasts.38,39 In SA due to the toxic effects of ethanol, erythroid but not granulocytic precursors can show vacuolization, helping to differentiate it from other Hematopathology / ORIGINAL ARTICLE 24. Porea TJ, Belmont JW, Mahoney DH Jr. Zinc-induced anemia and neutropenia in an adolescent. J Pediatr. 2000;136:688-690. 25. Broun ER, Greist A, Tricot G, et al. Excessive zinc ingestion: a reversible cause of sideroblastic anemia and bone marrow depression. JAMA. 1990;264:1441-1443. 26. Mossad SB, Macknin ML, Medendorp SV, et al. Zinc gluconate lozenges for treating the common cold: a randomized, double-blind, placebo-controlled study. Ann Intern Med. 1996;125:81-88. 27. Jackson JL, Peterson C, Lesho E. A meta-analysis of zinc salts lozenges and the common cold. Arch Intern Med. 1997;157:2373-2376. 28. McElroy BH, Miller SP. Effectiveness of zinc gluconate glycine lozenges (Cold-Eeze) against the common cold in school-aged subjects: a retrospective chart review. Am J Ther. 2002;9:472475. 29. Kumar A, Jazieh AR. Case report of sideroblastic anemia caused by ingestion of coins. Am J Hematol. 2001;66:126-129. 30. Hassan HA, Netchvolodoff C, Raufman JP. Zinc-induced copper deficiency in a coin swallower. Am J Gastroenterol. 2000;95:2975-2977. 31. Dunlap WM, James GW III, Hume DM. Anemia and neutropenia caused by copper deficiency. Ann Intern Med. 1974;80:470-476. 32. al-Rashid RA, Spangler J. Neonatal copper deficiency. N Engl J Med. 1971;285:841-843. 33. Pearson HA, Lobel JS, Kocoshis SA, et al. A new syndrome of refractory sideroblastic anemia with vacuolization of marrow precursors and exocrine pancreatic dysfunction. J Pediatr. 1979;95:976-984. 34. Naveh Y, Hazani A, Berant M. Copper deficiency with cow’s milk diet. Pediatrics. 1981;68:397-400. 35. Hayton BA, Broome HE, Lilenbaum RC. Copper deficiency–induced anemia and neutropenia secondary to intestinal malabsorption. Am J Hematol. 1995;48:45-47. 36. Schleper B, Stuerenburg HJ. Copper deficiency–associated myelopathy in a 46-year-old woman. J Neurol. 2001;248:705706. 37. Prodan CI, Holland NR, Wisdom PJ, et al. CNS demyelination associated with copper deficiency and hyperzincemia. Neurology. 2002;59:1453-1456. 38. Eichner ER, Hillman RS. The evolution of anemia in alcoholic patients. Am J Med. 1971;50:218-232. 39. Savage D, Lindenbaum J. Anemia in alcoholics. Medicine (Baltimore). 1986;65:322-338. 40. Brunning RD, Bennett JM, Flandrin G, et al. Refractory anaemia with ringed sideroblasts. In: Jaffe ES, Harris NL, Stein H, et al, eds. Pathology and Genetics of Tumours of Haematopoietic and Lymphoid Tissues. Lyon, France: IARC Press; 2001:69. World Health Organization Classification of Tumours. Am J Clin Pathol 2005;123:125-131 © American Society for Clinical Pathology 131 DOI: 10.1309/V6GVYW2QTYD5C5PJ 131 131 Downloaded from http://ajcp.oxfordjournals.org/ by guest on September 30, 2016 5. Summerfield AL, Steinberg FU, Gonzalez JG. Morphologic findings in bone marrow precursor cells in zinc-induced copper deficiency anemia. Am J Clin Pathol. 1992;97:665-668. 6. Fuhrman MP, Herrmann V, Masidonski P, et al. Pancytopenia after removal of copper from total parenteral nutrition. JPEN J Parenter Enteral Nutr. 2000;24:361-366. 7. Spiegel JE, Willenbucher RF. Rapid development of severe copper deficiency in a patient with Crohn’s disease receiving parenteral nutrition. JPEN J Parenter Enteral Nutr. 1999;23:169-172. 8. Wasa M, Satani M, Tanano H, et al. Copper deficiency with pancytopenia during total parenteral nutrition. JPEN J Parenter Enteral Nutr. 1994;18:190-192. 9. Klauder DS, Petering HG. Anemia of lead intoxication: a role for copper. J Nutr. 1977;107:1779-1785. 10. Hoffman HN II, Phyliky RL, Fleming CR. Zinc-induced copper deficiency. Gastroenterology. 1988;94:508-512. 11. Gyorffy EJ, Chan H. Copper deficiency and microcytic anemia resulting from prolonged ingestion of over-the-counter zinc. Am J Gastroenterol. 1992;87:1054-1055. 12. Tamura H, Hirose S, Watanabe O, et al. Anemia and neutropenia due to copper deficiency in enteral nutrition. JPEN J Parenter Enteral Nutr. 1994;18:185-189. 13. Hoogenraad TU, Dekker AW, van den Hamer CJ. Copper responsive anemia, induced by oral zinc therapy in a patient with acrodermatitis enteropathica. Sci Total Environ. 1985;42:37-43. 14. Fiske DN, McCoy HE III, Kitchens CS. Zinc-induced sideroblastic anemia: report of a case, review of the literature, and description of the hematologic syndrome. Am J Hematol. 1994;46:147-150. 15. Gregg XT, Reddy V, Prchal JT. Copper deficiency masquerading as myelodysplastic syndrome. Blood. 2002;100:1493-1495. 16. Prasad AS, Brewer GJ, Schoomaker EB, et al. Hypocupremia induced by zinc therapy in adults. JAMA. 1978;240:21662168. 17. Frieden E. The copper connection. Semin Hematol. 1983;20:114-117. 18. Williams DM. Copper deficiency in humans. Semin Hematol. 1983;20:118-128. 19. Williams DM, Lynch RE, Lee GR, et al. Superoxide dismutase activity in copper-deficient swine. Proc Soc Exp Biol Med. 1975;149:534-536. 20. Karimbakas J, Langkamp-Henken B, Percival SS. Arrested maturation of granulocytes in copper deficient mice. J Nutr. 1998;128:1855-1860. 21. Llanos RM, Mercer JF. The molecular basis of copper homeostasis copper-related disorders. DNA Cell Biol. 2002;21:259-270. 22. Kagi JH. Overview of metallothionein. Methods Enzymol. 1991;205:613-626. 23. Webb M, Cain K. Functions of metallothionein. Biochem Pharmacol. 1982;31:137-142.
 0
0
advertisement
Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users