Preprint PDF - Department of Mathematics
advertisement

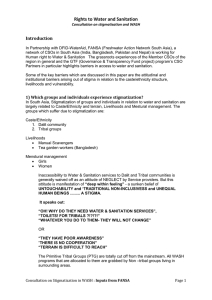
Good healthcare and leaky ostracism make stigmas against infectious disease maladaptive 2 4 Timothy C. Reluga1,* , Rachel A. Smith2 , David P. Hughes3 , 1 Department of Mathematics, Center for Infectious Disease Dynamics, The Pennsylvania State University, University Park, PA 16802 2 Department of Communication Arts and Sciences, Center for Infectious Disease Dynamics, and The Methodology Center, Pennsylvania State University, University Park, PA 16802 3 Departments of Entomology and Department of Biology, Center for Infectious Disease Dynamics, Pennsylvania State University, University Park, PA 16802 6 8 10 12 * timothy@reluga.org Abstract 14 Stigmas are a primal phenomena, ubiquitous in human societies past and present. Some evolutionary anthropologists have argued that stigmatization in response to disease is an adaptive behavior, that may help people and communities reduce the risks they face from infectious diseases and increase reproductive success. At the same time, cultural anthropologists and social critics have argued that stigmatization has strong negative impacts on community health. Recent analyses have resolved this conflict by hypothesizing that stigmas had individual and group-evolutionary benefits early in human evolution may now be mal-adaptive. Here, we present the first quantitative theory of infectious disease stigmatization and its consequences. We propose a four-state model of the stigmatization process driven by a transmissible disease creating chronic infections, and explore how rates of stigmatization can interact with social structure to impact the prevalence and lifetime risks of infection. The affects of stigmatization are revealed to be strongly dependent on health and cultural contexts. The asymmetries in secondary transmission between stigmatized and unstigmatized individuals can be represented with a dimensionless statistic Z , which we call the “stigma ratio”. When stigmatized people are strongly segregated from the rest of the population and there are no alternative interventions that reduce transmission (Z > 1), stigmatization can reduce lifetime risk of infection and overall disease prevalence. But when stigmatization is weakly enforce and reduces access to medical and behavioral interventions (Z < 1), stigmas increase lifetime risk and may increase prevalence. We further show fear of stigmas can exacerbated these negative effects and drive policy resistance against testing and treatment. We conclude that the deprecation of stigmas is a natural transition in the modern urban societies. Key words: Stigma; Ostracism; Infectious Disease Dynamics; Cultural Evolution Theory; Group Membership; Math Modelling; 1 16 18 20 22 24 26 28 30 32 34 36 1. Introduction Disease has been one of the strongest evolutionary pressures on Homo sapiens over the duration 38 of our species’ existence, and indeed on all mammalian species. Bacteria, fungi, protozoa, worms, and all manner of parasites have caused the untimely deaths of tens of billions of our potential ancestors, 40 driving us to evolve a complex immune system that learns about, adapts to, and remembers the infections we suffer over our lives [1, 2]. This same evolutionary pressure has also been operating 42 on human instinct for millennia, leading to innate behaviors like hygiene [3] and stigmatization [4]. However, while hygiene continues to be universally valued, stigmatization is now contentious. 44 Stigmas are considered a leading [e.g. 5] and poorly understood [e.g. 6] barrier to disease prevention, control, and treatment. Stigma has been linked to delayed diagnosis, poor treatment 46 adherence, prolonged risk of transmission, and increased risks of recurrence [e.g. 7] among other things. Stigmas are defined as simplified, standardized images of the profound disgrace of a particular 48 social group shared by a community at large [8]. But stigmas mark more than difference: they designate someone as profoundly devalued, discredited, and disgraced [9]. Among humans, stigmas 50 are socialized: community members need to be able to recognize those who pose threats to their group and how to limit this stigmatized group’s access to group resources and future interactions. 52 Consequently, humans developed messages to meet these goals. To stimulate stigma-related processes (creating beliefs, and inspiring actions to isolate and remove the labeled, and to socialize others), these 54 messages need to include content that quickly gains attention, encourages grouping and stereotyping, and provides reasons and emotional motivation to engage in devaluation and discrimination [10]. 56 Although stigmas can be a significant barrier to health, they are ubiquitous in human societies, globally and historically [8]. They even appear in other social species, from ants to chimpanzees 58 [11, 12, 13]. Scholars have proposed several hypotheses to explain this ubiquity of stigmas despite their costs. Some scholars [15] argue that stigmas defend group functioning. Some feel stigmas may 60 be a side effect of the evolution of discriminate sociality [4]. Others [16, 17] believe that they evolved as a defense against infectious diseases. Infectious diseases capitalize on the social nature of groups, 62 by spreading from one person to another via their interactions [14]. For social species who depend on each other for survival, stigmas may have functioned to protect uninfected members and the group, 2 64 by identifying infected members and ostracizing them from the group. For an infected person in a band or tribe millennia ago, ostracism meant swift and certain 66 death due to the infection, lack of resources and vulnerability to predators [13, 14]. For most of human history, particularly during the paleolithic period, humans lived in small, family-based groups, 68 with infrequent, intergroup interactions (typically for mating). This evolutionary advantage, then, occurred in pre-urban times (3000 years ago and older), when ostracized members would not be 70 brought into other groups. Ostracism, then, stopped the spread of infection and eliminated a reservoir for future infections. 72 Over the past 3,000 years, many conditions for the human species have changed – the population has grown, transportation facilitated widespread contact between humans, and medical practices 74 provided treatments for infectious diseases, all of which have implications for slowly evolving behaviors [18]. Smith and Hughes [14] explained how these new conditions could eliminate any fitness advantage 76 provided by stigmas, and, in fact, damage public health. For example, ostracism from one group no longer guarantees isolation from others. In addition, humans are noted for their sensitivity to social 78 rejection, with initial reactions to it registering like physical pain [19]. The social cost may be so high that people will keep suspected infections secret and avoid interacting with medical systems 80 altogether, which eliminates their ability to access medical treatments for the infection [10]. However, to understand how stigmatization transitions from an advantageous to a disadvantageous 82 behavior, we have to quantify the impacts of each of these changes in behavior. When do stigmatization’s benefits from infectious disease risk reduction stop offsetting the it’s social costs? In this paper, 84 we propose a nonlinear 4-state compartmental theory for the interactions between stigmatization and infectious disease prevalence. Our theory projects disease prevalence and community size under 86 steady-state conditions using demographic parameters, infection risks, and behavior. We use this model to determine conditions when stigmatization hurts public health. The theory can be extended and applied in many contexts to estimate the public-health impact of stigmatization. 3 88 2. Materials and Methods 90 In this section, we will describe the mathematical model of our theory of the interactions between stigmatization and disease-transmission dynamics. Our model combines a 4-state Markov chain for 92 the changes in an individual’s disease state with a reaction-network of nonlinear ordinary differential equations for disease prevalence. Definitions of our variables are provided in Table 1, while definitions 94 of our parameters and estimates for model scenarios are shown in Table 2. Table 1. State variables used in our model. Without brackets, the variable is a probability, but with brackets, the variable is a density. Symbol Meaning t Time measured in years S(t) Probability of being susceptible C(t) Probability of being cryptically infected L(t) Probability of being labelled with infection Z(t) Probability of begin stigmatized with infection [S](t) Density of susceptible people [C](t) Density of cryptically infected people [L](t) Density of people labelled with infection [Z](t) Density of people stigmatized with infection Each person in our model is categorized in one of four possible states: susceptible, cryptically 96 infected, infected and labelled, or infected and stigmatized. The probabilities that a person is in each of these states is represented respectively by S(t), C(t), L(t), and Z(t), where t represents time, 98 measured in years. A person can also leave the system because of death. Each individual is initially susceptible, so S(0) = 1 while C(0) = L(0) = Z(0) = 0. Transitions between states are governed by a 100 continuous-time Markov chain summarized in Figure 1. A susceptible person can become cryptically infected (rate Λ), a cryptically infected person can become labelled (rate x), labelled person can be 102 stigmatized (rate y). Death rates may depend on the person’s state (mS , mC , mL , mZ ). In matrix form, the probabilities of being in each state change according to the matrix equation −mS − Λ dC/dt Λ = 0 dL/dt dZ/dt 0 dS/dt 0 0 −mC − x 0 x −mL − y 0 y 4 S 0 C . 0 L −mZ Z 104 0 (1) Table 2. Parameters used in our model, their meanings, and the estimated values used in Old and New Scenarios. To facilitate plot comparisons, we choose the transmission rate β so that in all scenarios in the absence of stigmatization or labelling (y = x = 0), the basic reproductive ratio R0 = 2. The stable population sizes in Scenarios 1 and 2 are respectively N = 100 and N = 10, 000. Meaning Immigration rate of susceptible people Death rate while susceptible Death rate while crypticly infected Death rate while labelled Death rate while stigmatized Rate infected become labelled Rate labelled become stigmatized Background infection hazard Transmission rate when crypticly infected Relative transmission rate once labelled Relative transmission rate once stigmatized Marginal value per time of being in state S Marginal value per time of being in state C Marginal value per time of being in state L Marginal value per time of being in state Z Stigma ratio Parameter b mS mC mL mZ x y β σ η uS uC uL uZ Z Scenario 0 (Non-infectious) 2 0.02 0.02 0.02 0.2 12.0 2 × 10−2 0 NA NA NA NA NA NA NA Scenario 1 (Pre-Urban) 2 0.02 0.1 0.1 0.2 1.0 10−3 2 × 10−3 1.0 0.01 1 0.8 1. 0. 200 Scenario 2 (Modern) 200 0.02 0.1 0.04 0.04 1.0 10−5 2 × 10−5 0.1 0.5 NA NA NA NA 0.2 Our reaction network is an extension of classic compartmental models for epidemic dynamics [33, 34, 35]. It describes the change in the population health over time t under the assumption that 106 the population is strongly mixed, and all individuals have equal frequencies of contact with each other. Two new states are added to the classical compartmental epidemic model of chronic infectious disease 108 transmission to count when people have been labelled and stigmatized. We modify the notation slightly from standard practice for readability. Let [S](t) be the density of susceptible people who 110 without signs of infection. Let [C](t) be the density of infected people whose state has not yet been publicly identified. Let [L](t) be the density of people who are infected and have had their infection 112 publicly identified, and let [Z](t) be the density of infected people who have been stigmatized for their state. To avoid complications associated with demographic transients, we assume a constant 114 immigration rate of susceptible people (b). Over time, susceptible individuals may become infected through exposure to people in any of the infected compartments. We approximate the infection 5 116 pressure Λ, a.k.a. the “infection pressure”, as a linear function of the density of infected individuals. Λ = β ([C] + [L]σ + [Z]η) + , (2) where can be interpreted as the background risk of infection from an environmental reservoir, β is 118 the baseline transmission rate for cryptically infected people, and σ and η are relative transmission rates compared to the cryptically infected for labelled and stigmatized categories respectively. This 120 linear approximation is equivalent to the mass-action hypothesis in a strongly-mixed community with an environmental disease reservoir, but is also good approximation near equilibrium other 122 hypothetical forms of the infection pressure. Infected people become labelled at a constant rate, labelled people become stigmatized at a constant rate. This leads to a system of 4 ordinary differential 124 equations with one additional algebraic constraint: d[S] dt d[C] dt d[L] dt d[Z] dt = b − [S]mS − [S]Λ, (3a) = [S]Λ − [C]mC − [C]x, (3b) = [C]x − [L]mL − [L]y, (3c) = [L]y − [Z]mZ , (3d) Λ = β ([C] + [L]σ + [Z]η) + . (3e) Note that contact-reduction through stigmatization is a refinement of social distancing [36]. While 126 social-distancing is applied equally to all contacts, stigmatizing selectively reduces contacts with specific subpopulations. 128 The basic reproductive ratio, which determines the persistence of disease when background infection risks from reservoirs are very small ( ≈ 0) is R0 = bβ mS 1 σx ηxy + + mC + x (mC + x) (mL + y) mZ (mC + x) (mL + y) 6 130 . (4) When there is no stigmatization (y = 0), R0 = bβ (mL + σx) . mS mL (mC + x) (5) The steady-state lifetime risk ([LR], the probability of a person becoming sick over their lifetime) is 132 Λ/(Λ + mS ). We determine steady-state community sizes and disease prevalence by setting time-derivatives in 134 System (3) to zero and deriving a quadratic equation for Λ. Λ= ΛmS R0 + . Λ + mS (6) As long as there is some environmental reservoir seeding infection ( > 0), there is a single steady-state 136 infection pressure Λ∗ ∈ (0, βb/mS + ) which we calculate numerically and is monotone increasing with both the basic reproductive ratio (R0 ) and the reservoir pressure (). The steady-state densities 138 [S]∗ , [C]∗ , [L]∗ , and [Z]∗ can then all be calculated using linear algebra. The gross steady-state population density is [S]∗ + [C]∗ + [L]∗ + [Z]∗ , while the prevalence is P ∗ := [C]∗ + [L]∗ + [Z]∗ . 140 The effect of stigmatization on risk, infection pressure, and prevalence can be assessed through differentiation. The infection pressure depends on stigmatization only through the basic reproductive 142 ratio, according to Eq. (6). Differentiating the reproductive ratio, we find bβx (ηmL − mZ σ) dR0 = 2 dy mS mZ (mC + x) (mL + y) (7) The impact of stigmatization can be summarized by defining a dimensionless stigma ratio Z := σβ mL mZ ηβ 144 (8) which represents the ratio of the average cumulative transmission of a labelled but unstigmatized individual, and the average cumulative transmission of a stigmatized individual. Setting the derivative of the reproductive ratio with respect to the stigmatization rate to zero, we find that if Z = 1, 7 146 then basic reproductive ratio is independent of the rate of stigmatization. If Z < 1, then more 148 stigmatization increases the reproductive ratio, but if Z > 1, then more stigmatization decreases the reproductive ratio. Thus, the relationship between the stigmatization rate and the basic reproductive 150 ratio is monotone, with a sign determined by the stigma ratio. Since the infection pressure is a monotone function of the basic reproductive ratio, the same holds for it – if Z < 1, faster 152 stigmatization increases the infection risk, but if Z > 1, faster stigmatization decreases the infection risk. 154 The stigma ratio Z depends on the mortality rates mL and mZ which can be altered by medical treatment and state-correlated stresses. The value of the stigma ratio also depends on the relative 156 transmission rates σ (for the labelled) and η (for the stigmatized), which incorporate changes in contact rates and changes the probability of infection per contact. Changes in contact rate and 158 infectiousness can be attributed to differences in medical treatment and behavior because of social state. For example, the stigmatized might try to escape social stresses by avoiding medical treatment 160 and beneficial behaviors that reveal their disease state, leading to a relative increase in η over σ, so the stigma ratio Z will be small. On the other hand, if the stigmatized are ostracized (reducing η) 162 and have lower survivorship (increasing mZ ), then the stigma ratio will be large. Parameters are only summary statistics; the responses to stigmatization will be heterogeneous, with some people 164 conforming to social norms while others rebel against the same norms, so in practice we have to average over the effected population to estimate the stigma ratio. 166 The stigma ratio does not itself tell the whole story. The effect of stigmatization on prevalence is mathematically more complicated. The steady-state disease prevalence P ∗ has the matrix formula T 0 1 P∗ = 1 1 −mS − Λ Λ 0 0 0 0 −mC − x 0 x −mL − y 0 y 8 −1 b 0 0 0 0 −mZ 0 0 (9) 168 Differentiating prevalence with respect to the stigmatization rate, where dP ∗ ∂P ∗ ∂P ∗ ∂Λ dR0 = + dy ∂y ∂Λ ∂R0 dy ∂P ∗ Λbx (mL − mZ ) = 2, ∂y mZ (Λ + mS ) (mC + x) (mL + y) ∂P ∗ bmS (mL mZ + mZ x + mZ y + xy) = , 2 ∂Λ mZ (Λ + mS ) (mC + x) (mL + y) ∂Λ Λ2 mS ΛmS (Λ + mS ) = 2 = 2 2 ∂R0 (Λ + mS ) − R0 mS Λ + mS and dR0 /dy is given in Eq. (7). From inspection, we can tell that ∂P ∗ /∂Λ > 0 and ∂Λ/∂R0 ≥ 0 Since stigmatization is never expected to improve life-expectancy (µL ≤ µZ ), ∂P ∗ /∂y ≤ 0. It then 170 follows that whenever the stigma ratio Z > 1, faster stigmatization will reduce prevalence. There doesn’t appear to be such a simple general condition for when stigmatization increases prevalence, 172 but we can find some special cases. If stigmatization has no effect on mortality (µL = µZ ), for instance, then Z < 1 implies faster stigmatization increases prevalence. 174 The rate with which cryptically infected individuals are willing to seek out medical help and be “out” about their condition can depend on the rate of stigmatization and it’s consequences. In 176 communities where stigmatization is rapid and harsh, low rates of diagnosis and labelling (x small) may prevent people from taking advantage of effective treatments and educational programs even 178 when available. The rate at which people allow themselves to become labelled can be thought of as an optimization problem. Using Markov decision-process theory [24, 25], we can show that the expected utility of labelling at rate x in a population that stigmatizes at rate y is U(x, y) := 1 Λ + h + mS uS + Λ h + mC + x uC + x h + mL + y uL + yuZ h + mZ (10) where ui represents the marginal value per time of residing in state i and h is the discount rate. This expected utility is a hyperbolic function of the labelling rate x, so the best labelling rate will be 9 180 either the largest or smallest value possible. Explicitly, by differentiation we find xbest (y) := xmin + (xmax − xmin )H uC uL uC y uZ − − + mL + h mZ + h mC + h mL + h mC + h (11) where H() represents Heaviside’s step function. Commonly, the stigma state is less valuable than 182 the labelled state (uZ /mZ < uL /mL when h = 0). If it is also worse to be cryptically infected than labelled or stigmatized, (uC /mC < uZ /mZ ), then it’s best to maximize the labelling rate 184 (xbest (y) = xmax ). If cryptic infection is better than stigma and labelling (uL /mL < uC /mC ), then it’s best to minimize the labelling rate (xbest (y) = xmin ). If cryptic infection’s value falls between 186 the values of stigma and labelling, the best behavior depends on the risk of stigmatization, and slow labelling is optimal only if the stigmatization rate is large enough. 188 When people acting in their own self-interest counter-act a community policy, we call it “policy resistance”. When people’s actions reinforce and amplify a policy, we call it “policy reinforcement”. 190 In this case, the policy is a cultural norm, that is beneficial at the community scale, If the stigma ratio Z > 1 but the cryptic state is better for individuals than both labelled and stigmatized states, 192 we expect to observe policy resistance. On the other hand, if the stigma ratio Z < 1 and the cryptic state is worse than the labelled and stigmatized states, we expect to observe policy reinforcement. 194 Epidemic theories that account for population heterogeneity are more complicated than the homogeneous theory we have presented here, as they account for differences in health, age, and 196 contact rate [37, 38, 39]. For a baseline model of stigmatization in a heterogeneous population, we suggest a model where all individuals face the same risk, but may differ in all other parameters. Specifically, individuals are distributed over a type-space Ω according to a measure µ(ω; y) which 10 198 varies according to the stigmatization rate y. Then dynamically, d[Sω ] dt d[Cω ] dt d[Lω ] dt d[Zω ] dt 200 = b − [Sω ]mS − [Sω ]Λ, (12a) = [Sω ]Λ − [Cω ]mC − [Cω ]x, (12b) = [Cω ]x − [Lω ]mL − [Lω ]y, (12c) = [Lω ]y − [Zω ]mZ , Z Λ= β ([Cω ] + [Lω ]σ + [Zω ]η) dµ(ω; y) + , (12d) (12e) ω∈Ω where the parameter values (x, b, β, σ, η, uS , uC , uL , uZ ) are independent implicit functions of the type ω ∈ Ω. The steady-state infection pressure is the unique solution of the quadratic equation where ΛmS R0 (y) Λ= + Λ + mS Z bβ σx ηxy R0 (y) = 1+ + dµ(ω; y) mS (mC + x) (mL + y) mZ (mL + y) 202 (13a) (13b) ω∈Ω with R0 (y) being the expected basic reproductive ratio for a heterogeneous population. For small reservoir pressures ( → 0) and R0 > 1, 204 Λ = mS (R0 (y) − 1) + R0 (y) + O(2 ). R0 (y) − 1 (14) From this approximation, the sensitivity of the lifetime risk to changes in the stigmatization rate " # d [LR] 1 dR0 (2R(y) − 1) 2 = 2 1− +O dy R0 dy mS (R(y) − 1)2 (15) Thus, to minimize lifetime risk in a community without environmental reservoirs, it suffices to study 206 the effects of stigmatization on the basic reproductive ratio R0 . Our expression for the stigma ratio Z can be derived from this in the special case of a homogeneous population. 11 208 3. Modelling and Analysis Infectious disease stigmas have several complications that make their quantitative theory challeng- 210 ing. Foremost, the concept of a stigma is fuzzily defined. Unlike infection, which is a biological state that can be empirically tested using Koch’s postulates [20], a stigma is imposed on an individual 212 by their neighbors and not a testable property of the individual. A statement that a person is stigmatized is a communication about the perception of that person by the community, rather than 214 a statement about the person themselves. Moving a stigmatized person to a naive community may relieve them from experiencing stigmatization, at least temporarily. In addition, lay assignment of 216 infectious disease stigmas is imperfect. Humans rely on physical (often visual) and behavioral marks to identify targets of stigmatization [21], even though hosts are often infected and able to spread 218 disease to others before or even without showing symptoms [22]. Other conditions having generic symptoms overlapping the specific disease can be mis-attributed. More insidiously, stigma criteria 220 can drift because of people exploiting the situation for personal gain. S Λ mS C x L y mL mC Z mZ Figure 1. State-transitions for stigmatization. Here, S denotes the probability of being in susceptible state, C is the probability of being in the cryptically infected state, L is the probability of being in the labelled state, and Z is the probability of begin in the stigmatized state. See Tables 1 and 2 for parameter definitions and values. While there are inherent challenges, the dynamic analysis of stigmas can still provide useful 222 insight. Our formal mathematical analysis is given in the Materials and Methods, and summarized in Figure 1. People are categorized among four mutually-exclusive states: susceptible (S), cryptically 224 infected (C), infected and labelled (L), or infected and stigmatized (Z). Susceptible people are at risk of infection when they interact with either other infected people or an environmental disease reservoir. 226 Infections are chronic and people remain infected for the rest of their lives, as in several current and historical diseases that have generated stigmas. Infected people interact with susceptible people in different ways, depending on whether the community is ignorant of their infection (cryptically 12 228 infected), or has labelled or stigmatized them. Cryptically infected individuals interact with other 230 people normally, can transmit disease. But when the community becomes aware of the diagnosis or identifies the symptoms or behavior change of a cryptically infected person, they transition to a 232 labelled state – our math assumes that gossip of this sort permeates a community quickly. Once people are labelled, they can still transmit infection but can also access doctors, hospitals, and 234 other medical resources publicly. However, the labelled are also at risk for stigmatization by their community. Stigmas result in ostracism and reduced contacts with susceptibles. They may also 236 correspond to higher removal and mortality rates. Since there is no consistent and reliable means by which to remove a stigma [14], stigmas persist indefinitely, although individuals may adopt a variety 238 of cooping mechanisms, with variable success and consequences. For simplicity and illustration, we assume the infection pressure Λ obeys the generalized mass-action law Λ = β ([C] + [L]σ + [Z]η) + , 240 where β is the per-capita transmission rate, σ is the relative infectivity of the labelled, η is the relative infectivity of the stigmatized, and is the background infection hazard created by disease reservoirs. 242 The instantaneous infection risk for a person is Λdt, and at steady-state, the cumulative probability that an individual becomes infected over their lifetime (a.k.a. lifetime risk) [LR] = Λ/(Λ + mS ). For 244 demographics, people immigrate into the community as susceptible at a known rate, and are removed from each of the four states at per-capita rates characteristic of their state. 246 We can now explore how the rate at which labelled individuals become stigmatized can impact the prevalence, community size, and life-time risk of infection. Consider three different scenarios 248 (see Fig. 2). Scenario 0 (Non-infectious). As a base-scenario, suppose the infection pressure is independent of the number of those already sick, individuals with the disease die sooner, and 250 the disease-state is easily identified in others. Then strong stigmatization rates reduce prevalence because of the high mortality among the stigmatized. Stigmatization correspondingly reduces the 252 population size and is consequently costly to the group (although benefits from selection for disease resistance may kick-in over longer time scales). Scenario 1 (Pre-Urban). Now, suppose the 254 infection pressure is primary from contact with those infected, a community is so small a stigma is inescapable, stigma increases a person’s mortality risk several fold, and there is no effective medical treatment or prophylaxis against transmission. Then cultural norms of stigmatization will decrease 13 256 prevalence and enlarge a community. Scenario 2 (Modern). But if we are considering a large 258 urban community where labelled and stigmatized individuals are diagnosed to receive treatment which prolongs their lives relative to un-diagnosed individuals, and labelled individuals who have 260 not been stigmatized can take prophylactic actions that reduce transmission, while stigmatized individuals can partially escape ostracism, then stigmatization will increase prevalence and reduce 262 community size. Specific parameter values for Scenarios 0, 1, and 2 are given in Table 2. Comparing Scenarios 0 and 1, we see that the major benefits of stigmatization for a community 264 appears only for transmissible diseases. For non-transmissible infections, stigmatization does not reduce lifetime risk, but does reduce prevalence and population size. Comparison of Scenarios 1 266 and 2 shows that the impacts of stigmatization against transmissible diseases are not universally good or bad, but depend on the specifics of the disease, environment, and medical development of a 268 community. These results are consistent with the arguments of Smith and Hughes [14]. The impact of stigmatization can be summarized by defining a dimensionless stigma ratio Z which represents the 270 ratio of the average cumulative transmission of a labelled but unstigmatized individual to the average cumulative transmission of a stigmatized individual. The relationship between the stigmatization 272 rate and the lifetime infection risk ([LR]) is monotone, with the stigma ratio determining the derivative’s sign – if Z > 1, then more stigmatization decreases lifetime risk, but if Z < 1, then 274 more stigmatization increases lifetime risk (see Materials and Methods). The general conditions for the impact of stigmatization can be obtained through differentiation of the reproductive ratio 276 (see Materials and Methods), and holds in both homogeneous and heterogeneous populations.[TCR: may need to change] 278 The relative infectiousness of labelled individuals plays a crucial role in determining the impact of stigmatization (see Fig. 3). If individuals who have been identified as infected receive good medical 280 treatment and counselling, the chance that they further transmit infection can be greatly reduced, and pre-empt the benefits of stigmatization. On the other hand, if labelled individuals maintain 282 relatively high transmission rates, stigmatization remains an effective method of reducing infection pressure by reducing contact rates. But even in scenarios where more stigmatization reduces the lifetime infection risk in the community, individuals’ efforts to conceal their disease state because of 14 284 Scenario 0 (Non-infect ious) 100 1.0 Com m unit y size Prevalence 0.8 Lifet im e Risk Populat ion 80 60 40 10 -3 10 -2 10 -1 10 0 10 1 10 Scenario 1 (Pre-Urban) 1.0 Lifet im e Risk Populat ion 60 40 -3 10 -2 10 -1 10 0 10 1 10 2 1 10 2 1 10 2 Scenario 1 (Pre-Urban) 0.6 0.4 0.2 20 10 -3 10 -2 10 -1 10 0 10 1 10 0.0 -4 10 2 Scenario 2 (Modern) 10 -3 10 -2 10 -1 10 0 10 Scenario 2 (Modern) 1.0 10000 0.8 Lifet im e Risk 8000 Populat ion 10 0.8 80 6000 4000 0.6 0.4 0.2 2000 0 -4 10 0.4 0.0 -4 10 2 100 0 -4 10 0.6 0.2 20 0 -4 10 Scenario 0 (Non-infect ious) 10 -3 10 -2 10 -1 10 0 10 1 10 2 Annual rat e of st igm at izat ion (y) 0.0 -4 10 10 -3 10 -2 10 -1 10 0 10 Annual rat e of st igm at izat ion (y) Figure 2. Comparison of stigma’s impact on prevalence and risk. In Scenario 0 (top), stigmas applied to a non-transmissible disease reduce both prevalence and community size. In Scenario 1 (middle), where no treatment is available and stigmatization is inescapable, increasing rates of stigmatization reduces prevalence and allows for larger communities. In Scenario 2 (bottom), where treatment is available and stigmatization can be escaped, stigmatization increases prevalence, leading to reduced community size. See Table 2 for parameter values. Note: stronger stigmas never increase both community size and prevalence simultaneously. 15 0.8 Prevalence (P) Lifetime risk of infection (LR) 1.0 0.6 0.4 0.2 0.0 -3 10 10-2 10-1 100 101 102 Annual rate of stigmatization (y) 4000 3500 3000 2500 2000 1500 1000 500 0 10-3 Stigma number =2.00 =1.50 =1.00 =0.50 =0.02 10-2 10-1 100 101 102 Annual rate of stigmatization (y) Figure 3. Stigma ratios. As the stigma ratio (Z ) decreases, the benefits of stigmatization are diminished and reversed. For the lifetime risk [LR], this change occurs exactly when Z = 1. Prevalence also responses this way, but a smaller value of the stigma ratio is needed before stigmatization increases prevalence, and the affect of the stigmatization rate may not be monotone for an intermediate interval of values. Parameters from Scenario 2, but with increasing stigma ratio corresponding to decreasing relative infectivity of labelled individuals and µZ = 0.06 (Table 2). fears of stigmatization may diminish and potentially reverse the utility of stigmas. This is called 286 “policy resistance” [23], and can be modelled by allowing individuals to change their labelling rate x to improve their life situation (see Fig. 4) using an objective function calculated with Markov 288 decision process theory [24, 25]. 4. Discussion 290 Here, we have presented a formal model of the arguments previously made by Smith and Hughes [14]. Our analysis identifies specific conditions, in terms of the stigma ratio Z , under which the 292 stigmas switch from evolutionarily beneficial to detrimental. Our formulas can clarify the growing rhetorical and policy arguments over the use of stigma as a tool to manage public health in this and 294 other health contexts [26]. Rather than falling back on unstated prior beliefs that bias discussions of stigmatization, the relative merits of stigmatization can now be directly estimated from empirical 296 data using the formulas we supply. This will help us move toward an evidence-based dialog about the reasons for stigmatization and the best approaches available for coping with it and the underlying infectious disease. 16 298 Lifetime risk of infection (LR) 1.0 Labelling rate x =1 1.0 Relative infectivity of Labelled(σ) σ =1.00 σ =0.75 σ =0.50 σ =0.25 σ =0.00 0.8 0.6 0.4 0.8 0.6 0.4 0.2 0.0 -3 10 Labelling rate x = xbest(y,ω) 0.2 10-2 10-1 100 101 102 Annual rate of stigmatization (y) 0.0 -3 10 10-2 10-1 100 101 102 Annual rate of stigmatization (y) Figure 4. Stigma can backfire into policy resistance. In situations like Scenario 1 where faster stigmatization uniformly leads to lower risk when the labelling rate is fixed (left), cryptically infected individuals can reverse the benefits of stigmatization by manipulting their labelling rate in their own self-interest and concealing their infection state (right). In the case shown here, the population has weakly heterogeneous beliefs about the values of each state. For high relative infectivity (σ = 1), the community is best off maximizing the stigmatization rate; for low relative infectivity (σ = 0), the community is best off minimizing stigmatization, and for intermediate relative infectivity, the best stigmatization rate is about 1/10 per year. Parameters from Scenario 1 (Table 2), with xbest ∈ (1/10, 12) per year. 17 Evolution of the stigma ratio Z from high to low values may well be a marker of a larger 300 transition in the modern era, where populations are concentrated in urban areas and while advances in public health have removed the threats from pestilences like cholera, tuberculosis, smallpox, and 302 plague that beset early cities. However, this transition is mediated by the institutional, cultural, demographic, and Darwinian components of societal evolution, the last two of which progresses more 304 slowly than the first two. The different time-scales create a tension within societies as some people struggle to reconcile their instincts with reason and social norms. Migrations that bridge gradients in 306 social norms between urban and rural communities may add to this tension. Modern outbreaks for stigmatization in response to new epidemics like HIV [27] and Ebola [28] may well be symptoms of 308 this tension – the initially lack ameliorating public health interventions and established social norms leaves people to revert to instinctual behavioral responses. 310 Of course, our stigma ratio theory does not account for all possibilities. We have not attempted to directly model the rich variety of events and behaviors that follow stigmatization. To the best of our 312 understanding, these can have strong dependences on population composition, culture, environment, and the particular infectious disease, and further study will be needed to extend our theory beyond 314 it’s current scope. Nor have we tried to account for costs associated with the common false-positive application or conflation of stigmas, or any possible side-effects. And there may well be additional 316 knock-on effects to public health or social structure. For applications, our theory should probably be extended by merging demographic components of population structure, including age, gender, and 318 race. Our measures of group success have only been group size and lifetime risk, and thus can interpreted 320 under either group selection [29] or cultural [30] theories of community evolution. We have not attempted to address the more complicated impacts of disease and stigma on group function or 322 productivity. Selective pressures for stigmatization may be offset in part by kin-selection in the scope of family units, that favors nursing and care of sick individuals as a means of improving survival 324 and reproductive success of ones own genes. Infectious disease prevalence can promote sociality [31]. Such behavior is, in fact, well documented [32], and we may expect further effects to emerge from larger-scale structures in social networks. However, sometimes kin-relationships accelerate 18 326 stigmatization as family members attempt to avoid “courtesy stigma” [9, 10], complicating the matter 328 further. Our analysis has only considered cases of chronic infectious diseases. While we expect the same 330 factors to be at play in a case of an epidemic of an acute immunizing infection, dynamic aspects of the epidemic and stigmatization will become very important, as the infection hazards will change 332 relatively quickly, ultimately receding entirely, while stigmas may persist long after the epidemic ends, and have negative impacts on both individuals and communities. In addition, care-giving by 334 family members and neighbors may have short-term costs and risks, but long-term benefits which will compete in decision processes. Our general conclusion should still hold: stigmas will help or 336 hurt individuals and communities, depending on the quality of health care and the effectiveness of stigmatization at reducing risk. But any benefits are likely to be short term, and to disappear as the 338 epidemic wains. However, scenario-specific analyses will be needed to make sense of all the moving parts. 340 5. Conclusion In conclusion, we have provided a quantitative theory of how stigmatization of infected individuals 342 can affect community health, and shown that while stigmatization may have had benefits historically, this may well not be the case in dense modern societies. We hope our theory will prove useful in 344 futures studies of infectious disease stigmas and will provide a foundation for future mathematical and computational studies, as well as policy planning. 346 6. Acknowledgements The research was in part supported by National Science Foundation grant CCF-12156822 (TR), 348 and the National Human Genome Research Institute of the National Institutes of Health under Award Number R21HG007111 (RS). 350 [1] Frank SA. Immunology and Evolution of Infectious Disease. Princeton University Press; 2002. Available from: http://amazon.com/o/ASIN/0691095957/. 19 352 [2] Kuby J. Immunology. New York, NY: W. H. Freeman and Company; 1994. [3] Curtis V, Biran A. Dirt, disgust, and disease: Is hygiene in our genes? Perspectives in biology 354 and medicine. 2001;44(1):17–31. [4] Kurzban R, Leary MR. Evolutionary origins of stigmatization: The functions of social exclusion. 356 Psychological Bulletin. 2001;127(2):187–208. Available from: http://dx.doi.org/10.1037/ 0033-2909.127.2.187. 358 [5] The world health report 2001 - Mental Health: New Understanding, New Hope. Geneva, Switzerland: World Health Organization; 2001. Available from: http://www.who.int/whr/ 360 2001/en/. [6] Epidemiological fact sheets on HIV/AIDS and sexually transmitted infections. Geneva, Switzer- 362 land: UNAIDS; 2004. [7] Heijnders M, Van Der Meij S. The fight against stigma: An overview of stigma-reduction 364 strategies and interventions. Psychology, Health and Medicine. 2006 Aug;11(3):353–363. Available from: http://dx.doi.org/10.1080/13548500600595327. 366 [8] Smith RA. Language of the Lost: An Explication of Stigma Communication. Communication Theory. 2007 Nov;17(4):462–485. Available from: http://dx.doi.org/10.1111/j.1468-2885. 368 2007.00307.x. [9] Goffman E. Stigma: Notes on the management of spoiled identity. Englewood Cliffs, NJ: 370 Prentice-Hall; 1963. [10] Smith RA. Stigma communication and health. Handbook of health communication. 2011;2:455– 372 468. [11] Goodall J. Social rejection, exclusion, and shunning among the Gombe chimpanzees. Ethology 374 and Sociobiology. 1986 Jan;7(3-4):227–236. Available from: http://dx.doi.org/10.1016/ 0162-3095(86)90050-6. 376 20 [12] Hughes DP, Cremer S. Plasticity in antiparasite behaviours and its suggested role in invasion biology. Animal Behaviour. 2007 Nov;74(5):1593–1599. Available from: http://dx.doi.org/ 378 10.1016/j.anbehav.2006.12.025. [13] Wilson EO. Sociobiology: The new synthesis. Cambridge, MA: Harvard University Press; 2000. 380 [14] Smith RA, Hughes D. Infectious Disease Stigmas: Maladaptive in Modern Society. Communication Studies. 2014 Apr;65(2):132–138. Available from: http://dx.doi.org/10.1080/10510974. 382 2013.851096. [15] Neuberg SL, Smith DM, Asher T. Why people stigmatize: Toward a biocultural framework. In: 384 Heatherton TF, Kleck RE, Hebl MR, Hull JG, editors. The social psychology of stigma. New York: Guilford Press; 2000. p. 31–61. 386 [16] Park JH, Schaller M, Crandall CS. Pathogen-avoidance mechanisms and the stigmatization of obese people. Evolution and Human Behavior. 2007 Nov;28(6):410–414. Available from: 388 http://dx.doi.org/10.1016/j.evolhumbehav.2007.05.008. [17] Oaten M, Stevenson RJ, Case TI. Disease avoidance as a functional basis for stigmatization. 390 Philosophical Transactions of the Royal Society B: Biological Sciences. 2011 Oct;366(1583):3433– 3452. Available from: http://dx.doi.org/10.1098/rstb.2011.0095. 392 [18] Schaller M, Murray DR, Bangerter A. Implications of the behavioural immune system for social behaviour and human health in the modern world. Philosophical Transactions of the 394 Royal Society B: Biological Sciences. 2015 Apr;370(1669):20140105–20140105. Available from: http://dx.doi.org/10.1098/rstb.2014.0105. 396 [19] Eisenberger NI, Lieberman MD, Williams KD. Does rejection hurt? An fMRI study of social exclusion. Science. 2003;302:290–292. Available from: http://dx.doi.org/10.1126/science. 398 1089134. [20] Evans AS. Causation and disease – A chronological journey: The Thomas Parran lecture. 21 400 American Journal of Epidemiology. 1995;142(11):1126–1135. Available from: http://aje. oxfordjournals.org/content/142/11/1126.short. 402 [21] Park JH, Faulkneer J, Schaller M. Evolved Disease-Avoidance Processes and Contemporary AntiSocial Behavior: Prejudicial Attitudes and Avoidance of People with Physical Disabilities. Journal 404 of Nonverbal Behavior. 2003;27(2):65–87. Available from: http://dx.doi.org/10.1023/A: 1023910408854. 406 [22] Koelle DM, Wald A. Herpes simplex virus: the importance of asymptomatic shedding. Journal of Antimicrobial Chemotherapy. 2000 Apr;45:1–8. Available from: http://dx.doi.org/10. 408 1093/jac/45.suppl_4.1. [23] Sterman JD. Learning from Evidence in a Complex World. American Journal of Public Health. 410 2006;96:505–514. Available from: http://dx.doi.org/10.2105/AJPH.2005.066043. [24] Howard RA. Dynamic Programming and Markov Processes. Cambridge, MA: MIT Press; 1960. 412 [25] Reluga TC, Galvani AP. A general approach for population games with application to vaccination. Mathematical Biosciences. 2011;230(2):67–78. Available from: http://dx.doi.org/10.1016/j. 414 mbs.2011.01.003. [26] Vartanian LR, Smyth JM. Primum Non Nocere: Obesity Stigma and Public Health. Journal 416 of Bioethical Inquiry. 2013 Jan;10(1):49–57. Available from: http://dx.doi.org/10.1007/ s11673-012-9412-9. 418 [27] Bishop GD, Alva AL, Cantu L, Rittiman TK. Responses to Persons with AIDS: Fear of Contagion or Stigma? Journal of Applied Social Psychology. 1991 Dec;21(23):1877–1888. Available from: 420 http://dx.doi.org/10.1111/j.1559-1816.1991.tb00511.x. [28] Davtyan M, Brown B, Folayan MO. Addressing Ebola-related Stigma: Lessons Learned from 422 HIV/AIDS. Global Health Action. 2014 Nov;7(0). Available from: http://dx.doi.org/10. 3402/gha.v7.26058. 424 22 [29] Sober E, Wilson DS. Unto Others: The Evolution and Psychology of Unselfish Behavior. Harvard University Press; 1998. Available from: http://amazon.com/o/ASIN/0674930460/. 426 [30] Richerson PJ, Boyd R. Not by Genes Alone: How Culture Transformed Human Evolution. University Of Chicago Press; 2006. Available from: http://amazon.com/o/ASIN/0226712125/. 428 [31] Bonds MH, Keenan DC, Leidner AJ, Rohani P. Higher disease prevalence can induce greater sociality: a game theoretic coevolutionary model. Evolution; international journal of organic evo- 430 lution. 2005 Sep;59:1859–66. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/ 16261724/. 432 [32] Parsons T. The Sick Role and the Role of the Physician Reconsidered. The Milbank Memorial Fund Quarterly Health and Society. 1975;53(3):257. Available from: http://dx.doi.org/10. 434 2307/3349493. [33] Hethcote HW, Levin SA. Periodicity in epidemiological models. In: Applied mathematical 436 ecology. vol. 18 of Biomathematics. Springer-Verlag; 1989. p. 193–211. [34] Hethcote HW. The Mathematics of Infectious Diseases. SIAM Review. 2000 Jan;42(4):599–653. 438 Available from: http://dx.doi.org/10.1137/S0036144500371907. [35] Brauer F. Compartmental Models in Epidemiology. In: Brauer F, Wu J, , van der Driessche P, 440 editors. Mathematical Epidemiology. Lecture Notes in Mathematics. Springer-Verlag; 2008. p. 19–79. Available from: http://dx.doi.org/10.1007/978-3-540-78911-6_2. 442 [36] Reluga TC. Equilibria of an Epidemic Game with Piecewise Linear Social Distancing Cost. Bulletin of Mathematical Biology. 2013 Oct;75(10):1961–1984. Available from: http://dx.doi. 444 org/10.1007/s11538-013-9879-5. [37] Lindquist J, Ma J, van den Driessche P, Willeboordse FH. Effective degree network disease 446 models. Journal of Mathematical Biology. 2010 Feb;62(2):143–164. Available from: http: //dx.doi.org/10.1007/s00285-010-0331-2. 23 448 [38] Inaba H. Endemic threshold results in an age-duration-structured population model for HIV infection. Mathematical Biosciences. 2006 May;201(1-2):15–47. Available from: http://dx.doi. 450 org/10.1016/j.mbs.2005.12.017. [39] Nol PA, Davoudi B, Brunham RC, Dub LJ, Pourbohloul B. Time evolution of epidemic 452 disease on finite and infinite networks. Physical Review E. 2009 Feb;79(2). Available from: http://dx.doi.org/10.1103/PhysRevE.79.026101. 24 454