Management of Ear-Canal Collapse
advertisement

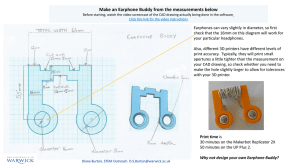
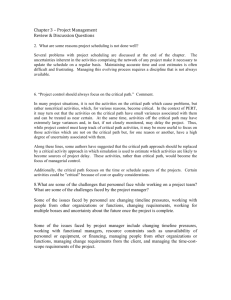
Management of Ear-Canal Collapse Lynne Marshall, PhD, Mary A. Gossman, MA • Thresholds were measured at 250, 500, 1,000, 2,000, 3,000, 4,000, 6,000, and 8,000 Hz in 20 normal adult ears and in ten ears from adults with varying amounts of ear-canal collapse. To alleviate the attenuation caused by ear-canal collapse, ear-canal inserts, postauricular pads, or circumaural cushions (Telephonics 510-020) were used with earphones (TDH-49). The circumaural cushions provided the lowest thresholds for the listeners with ear-canal collapse. Although thresholds with the ear-canal inserts were comparable to those with the circumaural cushions for many of the listeners, the ear-canal inserts were not suitable for listeners with more severe ear-canal collapse because the insert was displaced when the supra-aural cushion was placed on the pinna. Thresholds with the postauricular pinna pads were higher than with the circumaural cushions for most individuals. (Arch Oto/aryngo/1982;108:357-361) hanges often take place in the C dermis with increasing age,t particularly degeneration of the elastic fibers 2•3 and a decrease in collagen.' These changes cause the tissue to lose its elasticity and strength. As a result, the cartilaginous portion of the ear canal becomes more flexible and may constrict or completely close when an earphone is placed on the pinna. Schow and Randolph 5 reported a 36% incidence of ear-canal collapse in an elderly (aged .60 to 79 years) population, and the incidence for nursinghome residents is ·even higher. 6•7 Schow and Randolph 5 estimated Accepted for publication Oct 28, 1981. From the Department of Counseling and Special Education, University of Nebraska at Omaha (Dr Marshall); and Archbishop Bergan Mercy Hospital, Omaha (Ms Gossman). Reprint requests to Department of Counseling and Special Education, University of Nebraska at Omaha, Omaha, NE 68182 (Dr Marshall). Arch Otolaryngoi-Vol 108, June 1982 that ear-canal collapse may account for a 5-dB error in earphone threshold norms for the elderly. · Bowever, threshold shifts for individual listeners may be as large as 20 to 30 dB, especially at 1,000 Hz and above.' Several solutions have been suggested: Chaiklin and McClelland8 tried a hand-held earphone, a stock ear insert of the type used for hearing-aid evaluations, the NAF circumaural cushion with TDH-39 earphones, and sound-field assessment on 12 adults with no evidence of ear-canal collapse and on 12 subjects of all ages (including children) with collapsible ear canals. These various arrangements were compared with TDH-39 earphones with MX-41/ AR cushions. The hand-held earphone resulted in a leak of energy at 2,000 Hz and below, and the ear insert resulted in a highfrequency attenuation. These authors concluded that circumaural cushions or sound-field evaluation should be employed with individuals having collapsi'ble ear canals. However, there is no standard for calibration of earphones with circumaural cushions. Also, threshold evaluations in sound field often are not practical due to the need for a controlled acoustic environment and special signals (narrow-band noise or warbled tones). Additionally, there is no standard to specify the acoustic characteristics of these stimuli for commercial audiometers. Therefore, it would be advantageous to find a solution to ear-canal collapse that would be compatible with TDH-49 earphones with MX-41/ AR cushions, for which there are standards. Audiologists often use acousticimmitance probe tips as ear-canal inserts with standard earphones and cushions. These probe tips, however, result in an attem,J.ation of high fre- quencies similar to that found for stock ear-mold inserts. 9 In the present study, we used earcanal inserts and postauricular pads with TDH-49 earphones and MX-41/ AR supra-aural cushions, and also Telephonics 510-020 circumaural cushions. The object was to find an earphone arrangement that would alleviate ear-canal collapse without introducing unwanted acoustic effects and that would provide minimal intrasubject and intersubject vanability. METHOD Subjects Two groups of subjects were used. The first group consisted of ten adults under age 35 years with normal tympanograms, acoustic reflexes at normal sensation levels, and no evidence of ear-canal collapse. Both ears were used for these subjects. The second group consisted of adults with highfrequency air-bone gaps whose ear canals appeared to collapse with pressure on the pinna. Each subject was identified as having ear-canal collapse by one of five audiologists. Thirteen subjects identified as having ear-canal collapse, aged 21 to 86 years, participated in the study. Nine of the subjects appeared to have monaural ear-canal collapse; four had binaural ear-canal collapse. Thus, 17 ears were selected for the experimental group. Equipment A Grason-Stadler 1704 audiometer was used for all threshold measurements. TDH-49 earphones were used for all airconduction conditions. They were calibrated" with MX-41/ AR cushions using a Bruel and Kjaer sound-level meter with a 6-cc coupler (General Radio 9A). Thresholds were measured with MX-41/ AR supra-aural cushions and Telephonics 510020 circumaural cushions. The ear-canal inserts were cutoff plastic otoscope tips with inside diameters of 5 or 6 mm and lengths of 4 to 7 mm. The postauricular pinna pads, made of rigid polystyrene plastic (Styrofoam) coated with varnish, were Ear-Canal Collapse-Marshall & Gossman 357 Table 1.-Sensitivity Change, in Decibels' tri of Frequency, Hz occ 750 -12.9 -14.4 500 -12.5 -9.4 Riedner and Shimizu," 1976 -5.7 -9.3 Riedner," 1980 .. . Schow et al," 1980 . .. . .. ... . .. Present study -6.0 . .. -7.4 -10.0 Source, yr Jerger· and Tillman." 1959 Chaiklin and McClelland,' 1971 250 -7.5 -8.5 -11.2 1,000 -11.6 -11.7 -11.7 .. . -11.6 -13.9 1,500 -8.9 -10.3 2,000 -10.7 -6.7 3,000 -10.4 -8.3 4,000 -1.9 -5.6 6,000 -5.4 0 8,000 +1.9 -1.7 . .. .. . ... -8.7 . .. -2.0 ... ... ... -6.2 ... -6.6 ... . .. . .. -12.0 -7.4 ... -3.5 . .. -3.4 -1.2 -1.9 +5.0 (P ~ .05 on a t test) were seen at the lowest and highest frequencies. Thresholds were raised by 4 dB at 250 Hz, and 2 dB at 500 Hz. These changes presumably were due to a leak of energy at low frequencies caused by a looser coupling between the ear cushion and the external ear. Sensitivity at 8,000 Hz was enhanced by 3 dB. Threshold differences between suGeneral Procedure. pra-aural and circumaural cushions Audibility thresholds were measured at are shown in Table 1 for several 250, 500, 1,000, 2,000, 3,000, 4,000, 6,000, and studies. Jerger and Tillman 13 used 8,000 Hz under four conditions: MX-41/ AR PDR-10 earphones with MX-41/ AR supra-aural cushions, MX-41/ AR cushions and Telephonics 510-020 circumaural with ear-canal inserts, MX-41/ AR cushcushions. Chaiklin and McClelland, 8 ions with postauricular pinna pads, and Riedner and Shimizu, 14 and Riedner 15 Telephonics 510-020 circumaural cushions. used TDH-39 earphones with MX-41/ Threshold measurements also were made AR and NAF 48490-1 cushions. Schow at 750 and 1,500 Hz for the MX-41/ AR and et al' 6 used TDH-39 earphones with Telephonics 510-020 cushions in order to obtain more complete data on supra-aural · MX-41/ AR and Telephonics 510-020 and circumaural cushion differences. circumaural cushions. As stated earliBone-conduction thresholds were meaer, we used TDH-49 earphones with sured at 500, 1,000, 2,000, 3,000, and 4,000 MX-41/ AR and Telephonics 510-020 Hz. Manual pure-tone audiometry with a cushions. The same general trend can 5-dB step size was used for threshold meabe seen across· all studies. For fresurements (American National Standards from 250 to 3,000 Hz, greater quenCies Institute 83.2 12 standard except that 200input to the earphones is required for ms pulsed tones were used). thresholds with circumaural cushions Contralateral masking was not used durin order to equal thresholds obtained ing air-conduction measurements unless with standard supra-aural cushions. there was a possibility of crossover of the test signal. Cont'ralateral masking was This result is to be expected since the used during all bone-conduction measurevolume under the ear cushion is larger ments unless there was a possibility of with the circumaural cushions, and crossover of the masker. sound pressure is inversely related to The order of presentation of the various volume at frequencies less than 1,000 earphone or bone vibrator conditions was Hz. The differences between circumrandomized. Following a rest, all ·conaural and supra-aural cushions disapditions were ·replicated once. Testing was pear .at higher frequencies. Here the completed in one session. circumaural earphone allows concha RESULTS AND COMMENT resonance to occur, with. an increase Normal Subjects in sound pressure at high frequencies somewhat offsetting the effect of the Thresholds were unaltered by the larger volume. ear-canal insert; all threshold changes lntersubj ect variability between were less than 1 dB. For the pinna pad, statistically significant changes conditions was measured separately 358 Arch Otolaryngoi-Vol 108, June 1982 otl pir boJ ( ga] pac • Caused by substituting circumaural for standard supra-aural cushion. Data are from 20 normal ears. shaped to fit behind the pinna. Boneconduction measurements were made with a Radioear B-70-A bone vibrator for the normal group. The bone vibrator was changed to a Radioear B-71 bone vibrator prior to data collection on the listeners with .ear-canal collapse. Calibration of both bone vibrators was accomplished with an artificial mastoid (Bruel and Kjaer), using values from Dirks et al." M~ for each frequency (Hartley's test for homogeneity of variance' 7 ) •. No differences were found between the MX -41/ AR cushions and any of the other conditions (MX-41/ AR cushions with insert, MX-41/ AR cushion with pinna pad, and circumaural cushions) at any frequency. Correlations (Pearson r) between thresholds on the two replications and the SEs of measurement were computed and are available from the authors. The lowest correlations were seen at lower (< 2,000 Hz) frequencies, probably due to the restricted range of thresholds in our young listeners at these frequencies. No earphone condition appeared to be clearly superior to any of the other conditions for listeners without ear-canal collapse. Subjects With Ear-Canal Collapse tiv res fa!: cri· air duE abi fal: ant er, pos bee por: ear: we~ whi On;E _cur~ whi and the anq ric1,1 8,0@ pla~ soui.J Some of the subjects identified as having ear-canal collapse by the audi: ologists did not show measurable earcanal collapse in our study. That is, we either found only a negligible air-bone gap or were unable to demonstrate much improvement in air-conduction thresholds using any of the methods to correct for ear-canal collapse. Thus, we were required to set a more definitive criterion for ear-canal collapse group selection. The criterion suggested by Chaiklin and McClelland8 and employed by Schow and Randolph,5 Schow and Goldbaum/ and Schow et a1 16 was a 15-dB lowering of threshold with circumaural cushions at any frequency. In order to ensure that we would not get false-positives using this criterion, we examined the data for the 20 normal ears. We treated each of the two replications as a separate trial, so that we had 40 ciaii Hz/ mig; by 1 mea fals; freq two! Ear-Canal Collapse-Marshall & Gossman Arch ql er t~ 10-d. adja a uri cusb daro The[ tWOf no gro~ SUSP mix€ air- W .for aif- the the , ons hh ns) een md il:n- the ere ented lisarrly ms :ol- ·as di: ar- we me ate ibn >ctS 1J.S, ni)se lg:ids LU- nd of ms t;re res ,he TVe as 40 trials in all. We counted the number of times a 15-dB lower threshold occurred between air conduction with MX -41/ AR cushions and each of the other conditions (insert, postauricular pinna pad, circumaural cushions, and bone conduction). Out of 40 measurements, air-bone gap, insert, and postauricular pinna pad each resulted in two false-positives, and the circumaural cushion resulted in· five false-positives. The false-positives for the air-bone gap criterion were not surprising since an air-bone gap of this magnitude can be due to test variability. 18•19 Test variability could also account for the false-positives found for the insert and postauricular pinna pad. However, we did not expect the higher falsepositive rate for circumaural cushions because Schow and Randolph 5 reported no false-positives in 40 normal ears. Their measurements, however, were at 500, 1,000, 2,000, and 4,000 Hz, while we used additional frequencies. One of the false-positives for the circumaural cushion was at 3,000 Hz, while the remaining four were at 6,000 and 8,000 Hz. The false-positives for the inserts were at 4,000 and 6,000 Hz, and the false-positives for the postauricular pinna pad were at 6,000 and 8,000 Hz. Because different earphone placements result in variations of the sound pressure in the ear canal, especially for frequencies above 3,000 Hz, 20"22 high-frequency thresholds might be expected to differ more often by 15 dB or greater due to test-retest measurement error. We found no false-positives in normal. ears at any frequency if we used the mean across two replications for each ear. Our final criterion was a 15-dB lower threshold at any one frequency or a 10-dB lower threshold at any two adjacent frequencies for insert, postauricular pinna pad, or circumaural cushion in comparison with the standard MX-41/ AR supra-aural cushion. The thresholds were the mean across two replications. This criterion gave no false-positives for the normal · group. Since one of our listeners with suspected ear-canal collapse had a mixed hearing loss, we did not include air-bone gap in the criterion. When our final criterion was Arch Otolaryngoi-Vol 108, June 1982 applied to the 17 ears with suspected ear-canal collapse, seven were eliminated, a sizable number to eliminate when they had been identified by audiologists as having ear-canal collapse. As stated earlier, all subjects appeared byvisual inspection to have at least some degree of ear-canal collapse. However, the amount of hearing loss caused by the ear-canal collapse apparently was so small that it was obscured by test variabiljty. Had we used a smaller step size (eg, 2 dB) and a test procedure that results in less variability (eg, adaptive twointerval forced choice), we might have been able to document the small effects of ear-canal collapse in these individuals. For clinical purposes, however, such small effects are relatively unimportant. In some cases the audiologist's initial test results showed larger air-bone gaps than we found on either the initial test or the replication, which brings up the possibility that earphone placement may have played a role in air-bone gap size. In collapsing canals, not only does direct pressure on the pinna appear to push the posterior wall forward, but if the pinna is pushed forward, the closure of the meatus is even greater. Thus, careful placement of the earphones is important. Of equal importance is that a patient not readjust the earphones, which .may occur unbeknownst to the audiologist. Our final group of ten ears, selected by the above-stated criterion, was divided into two groups for purposes of data analysis. These two groups could be differentiated by two factors: (1) the amount of loss caused by the ear-canal collapse as well as the frequencies at which the air-bone gap occurred, and (2) the way in which the insert fit into the ear canal once an earphone was placed on the pinna. The first group consisted of eight ears with attenuation caused by ear-canal collapse no greater than 20 dB at one to four frequencies at 1,000 Hz and above, with 3,000 to 6,000 Hz being affected most often. Although in some of these subjects the insert became displaced slightly outward when pressure was placed on the pinna, in no case did the insert become completely dislodged. The data from these eight ~o~o~-L~~~~1~.o~o~o--~-L~~~ Frequency, Hz Fig 1.-Pure-tone thresholds for eight ears with ear-canal collapse under various earphone or bone-conduction conditions. Circles indicate MX-41 I AR cushion; squares, insert; triangles, pinna pad; diamonds, circumaural cushion; and asterisks, bone cond_uction. HL indicates hearing level. i, o.____ '-o-- L>,,_ ............c:..~~~~--6 ..........\, --~-- ..J I OJ "0 -c 0 .<:: ~ ¢: ·~ 0 ____ o_\',, 30 0, ··- ••L>.. ······o-- ----D-- ----a, o. __ ···o-.... -o ....• -o •••. .-~ Ins Pin Circ Bone Fig 2.-Pure-tone thresholds for eight ears with ear-canal collapse under various earphon.e or bone-conduction conditions at frequencies with significant differences across co,nditions. Circles indicate 2,000 Hz; squares, 3,000 Hz; triangles, 4,000 Hz; and diamonds, 6,000 Hz. To increase visual clarity, symbols for each frequency have been connected. MX-41 indicates MX-41 1 AR cushion; Ins, insert; Pin, postauricular pinna pad; Circ, circumaural cushions; and Bone, bone conduction. HL indicates hearing level. ears are presented as the group data in the following analyses. One of these eight ears had a mixed hearing loss. The second group consisted of two ears with more severe ear-canal collapse, and these data are presented separately. The attenuation caused by ear-canal collapse for these listeners was greater than 20 dB for some frequencies, and the frequencies affected were from 250 or 500 Hz up through Ear-Canal Collapse-Marshall & Gossman 359 I Table 2.-Severe Ear-Canal Collapse• Frequency, Hz Test Condition Subject 1, 62 yr MX-41/AR 250 500 1,000 2,000 3,000 4,000 6,000 a,ooo 42.5 25.0 27.5 90.0 95.0 97.5 95.0 92.0 40.0 22.5 30.0 90.0 97.5 95.0 90.0 90.0 Pinna pad 15.0 10.0 7.5 67.5 80.0 75.0 77.5 75.0 Circumaural 15.0 2.5 5.0 60.0 72.5 70.0 65.0 67.5 Bone .. . 2.5 20.0 62.5 >65.0 62.5 . ·.· ... Insert Subject 2, 61 yr MX-41/AR 15.0 12.5 20.0 75.0 80.0 82.5 77.5 90.0 Insert 10-15 10-10 15-20 55-70 60-75 60-75 55-70 65-85 Pinna pad 20.0 25.0 15.0 60.0 55.0 55.0 67.5 72.5 Circumaural 15.0 5.0 15.0 62.5 65.0 57.5 60.0 70.0 Bone . .. 2.5 12.5 5:2.5 57.5 57.5 ... . .. *Thresholds for each ear represent the mean across two replications except for subject 2 in the insert condition. Thresholds for each replication are shown separaiely; for one replication the insert was in place, while for the other replication the insert was dislodged. in ad cu: as lin lm w. re: an wi pli cu be fa, ap WE 8,000 Hz. Another characteristic of these ears, which was the reason they were dealt with separately in the data analysis, was that the ear-canai insert became dislodged when the earphone was worn to the extent that the insert was completely ineffective in preventing the ear-canal collapse. Results for the eight ears in the ear-canal collapse group are shown in Fig 1. The thresholds for the pinna pad and circumaural cushions use the correction values established with the normal group to equate thresholds for these earphone arrangements to the standard earphones. Differences across condition$ were not significant (analysis of variance) for 250, 500; 1,000, and 8,000 Hz. The differences across conditions were significant (P :::::; .01) for 2,000 to 6,000 Hz. These frequencies are graphed separately in Fig 2 in a different format. To determine which test condition best alleviated ear-canal collapse, we first compared the threshold for the MX-41/ AR cushion with the ~ar-canal insert, postauricular pinna pad, and circumaural cushion. At 2,000, 4,000, and 6,000 Hz, only the circumaural cushion differed significantly (Bonferron! t test, P :::::; .05) . from the MX-41/ AR cushion. Thus, the circumaural cushion appeared superior to the other conditions. While at 3,000 Hz none of the earphone conditions differed significantly from the MX41/ AR condition, all three earphone conditions did result in lower thresholds than the MX-41/ AR condition. Another comparison determined 360 Arch Otolaryngoi-Vol 108, June 1982 which earphone condition resulted in closure of the air-bone gaps (significant at 2,000, 3,000, and 4,000 Hz) between MX-41/ AR cushions and bone conduction. Although not entirely valid because one ear had a mixed hel).ring loss, the air~bone gap (circumaural cushion and bone vibrator) for this listener was relatively constant (10 to 12.5 dB for the mean across two replications) at 2,000, 3,000, and 4,000 Hz. Results of this comparison at 2,000 Hz showed no significant differences between bone conduction and insert,. pinna pad, or circumaural cushion. Thus, all . earphone conditions successfully closed the air-bone gap at this frequency. At 3,000 Hz these three earphone conditions all differed significantly from the bone-vibrator condition. That is, none of the three earphone conditions successfully closed the airbone gap at 3,000 Hz. At 4,000 Hz the insert and pinna pad thresholds, but not the circumaural cushion thresholds, were significantly different from bone-vibrator. thresholds. Therefore, only the circumaural cushion resulted in closure of the air-bone gap at 4,000 Hz. A final comparison was made among insert, pinna pad, and circumaural cushion thresholds at the same four frequencies. No differences were found at 2,000, 3,000, and 4,000 Hz. At 6,090 Hz, circumaural cushion thresholds were significantly lower than the inse~t and pinna' thresholds. The correlations (Pearson r) between thresholds on the two replica- tions and the SEs of measurement for the eight ears with ear-canal collapse were computed. As with the normal group, no condition appeared to be clearly superior. Also, there were no significant differences in variability (homogeneity of variance) for the various test conditions at each frequency. Data for the two listeners (with sensorineural hearing loss) who had the most severe ear~canal collapse, and whose data were excluded from the group analysis, are shown individually in Table 2. All th;resholds repref;ent the mean across two replications with one exception. For subject 2, the ear-canal insert was in place during the iriitial testing. For the replication, we were unable to position the insert so that it remained in place with pressure ori the pinna. The two thresholds. shown for subject 2 in the insert condition were for the first test, with the insert in place, and for the replication, with the insert displaced. In conclusion, the Circumaural cushions best alleviated the effects of ear-ca11al collapse .because they resulted in the lowest thresholds for most listeners, in . agreement with Chaiklin and McClelland: 8 While the major disadvantage of these cushions is that the~e is no standard at present for their calibration, the earphones can be calibrated in a 6-cc coupler with supra-aural cushions. Correction values for circumaural cushions (Table 1) can then be applied. Calibration also can be accomplished reliably using a flat-plate coupler/2•23 although such a coupler is not readily available Ear-Canal Collapse-Marshall & Gossman Oli die eff stc Me USI of ca: in: th wi co,'.,,· OCi io1 ex pa f01 inl co. ly anc DR Bic G~i pp 2 · of 1 th~ 194 3 in I 4 ica: JI 5 lap JA 6 vic:j am He 7 can JS 8 rna lar Arc OWn for ~pse mal be no lity rar- lcy. rith b. ad ~se, ·om rid•reons the ing · on, ert ith :wo the lSt, the ed. ral cts tey f_or ith ;he ms mt 1es ler .on ms ~a­ Jly gh Jie in most clinical settings. Another disadvantage is that the circumaural cushions do not produce levels as high as the MX-41/ AR cushions, which limits the highest measurable hearing loss using commercial audiometers. We also should point out that our results apply only to adult listeners and not to young children or infants with tiny, flaccid ear canals. The coupling effects of standard circumaural cushions to small heads has not yet been established, so our· correction factors, as well as those of others, apply only to adults. Results with the ear-canal inserts were unsatisfactory. We succeeded in our goal of finding an insert that did not introduce unwanted .acoustic effects in normal ears, unlike the stock ear mold· used by Chaiklin and McClelland 8 or the impedance probe used by Bryde and Feldman. 9 For five of the eight ears with milder earcanal collapse, thresholds with the insert were comparable to those with the circumaural cushions. However, with increasing severity of ear-canal collapse, some slippage of the insert occurred when the supra-aural cush~ ion was placed on the pinna, which explains why the insert was not comparable to the circumaural cushions for the group data. For the ears having the greatest amounts of ear-canal collapse, the inserts became completely displaced. Thus, ear-canal inserts such as ours can be used only on ears with milder degrees of ear-canal collapse. The suitability of the insert for a particular ear is easy to discern visually by pressing on the pinna after the insert is in place to determine whether slippage of the insert occurs. Thresholds with the postauricular pad were higher than with circumaural cushions for most of the ears with ear-canal collapse. The reason for this is not entirely clear although we suspect that the pinna and posterior wall may be pushed forward when the pinna pad is placed snugly behind the ear. Additionally, the earphone is not coupled as closely to the head with the pinna pad in place, and the leakage of energy at low frequencies for individual listeners with ear-canal collapse can be considerable. Subject 2, whose thresholds are shown in Table 2, illustrates this problem. The pinna pad worked rather well for this listener at most frequencies. However, the threshold at 500 Hz was much higher with the pinna pad than for any of the other conditions. Similar problems would be expected with a hand-held earphone, and the coupling of the cushion to the pinna would be more variable, especially with the patient holding the earphone .. The frequencies most affected by ear-canal collapse were above 1,000 or 2,000 Hz for listeners with mild ear- L Kenshalo DR: Aging effects on cutaneous and kinesthetic sensibilities, in Han SS, Coons DH (eds): Special Senses in Aging: A Cun·ent Biolouical Assessment. Ann Arbor, Institute of Gerontology, University of Michigan, 1979, pp 189-217. 2. Dick JC: Observations on the elastic tissue of the skin with a note on the reticular layer at the junction of the dermis and epidermis. J A nat 1947;81:201-211. 3. Ma CK, Cowdry EV: Aging of elastic tissue in human skin. J Gerontol1950;5:203-210. 4. Pearce RH, Grimmer BJ: Age and the chemical constitution of normal human dermis. J Invest De,·mato11972;58:347-36L 5. Schow RL, Randolph L: Prevalence of collapsible ear canals in an elderly population. J Acoust Soc Am 1979;66:61. 6. Zucher KD, Williams PS: Audiological services in an extended care facility. Read before the annual convention of the American Speech and Hearing Association, Chicago, November 1977. 7. Schow RL, Goldbaum DE: Collapsed ear canals in the elderly nursing home population. J Speech Hear Disord 1980;45:259-267. 8. Chaiklin JB, McClelland ME: Audiometric management of collapsible ear canals. Arch Otolaryngol1971;93:397-407. 9. Bryde ~L, Feldman AS: An approach to the management of the collapsing ear canal. ASHA 1980;22:734. 10. American National Standards Institute: Anw·ican National Standw·ds Specifications fen· Audiometers, ANSI-S3.6-1969. New York, American National Standards Institute, 1969. 11. Dirks DD, Lybarger SF, Olsen WO, et a!: Bone conduction calibration: Current status. J Speech Hero· Disord 1979;44:143-155. 12. American National Standards Institute. Amaican National Standard Methods for Manual PUJ·e-Tone Threshold Audiometry, ANSIS:J.:21-1.978. New York, American National Standards Institute, 1978. 13. Jerger JF, Tillman TW: Effect of earphone cushion on auditory threshold. J Acoust Soc Am 1959;31:1264. 14. Riedner E, Shimizu H: Collapsing ears and acoustic reflex measurement with circumaural ear cushions. A1·ch Otolarynyol 1976;102:358-362. 15. Riedner ED: Collapsing ears and the use of circumaural ear cushions at 3,000 Hz. Ear Hear 1980;1:117-118. 16. Schow RL, Randolph L, Nerbonne MA: Collapsible ear canal prevalence in an elderly clinical population. ASHA 1980;22:734. 17. Wike EL: Data Analysis. Chicago, Aldine- canal collapse. Only for more severe ear-canal collapse did the effect extend down to lower frequencies. Our results are in agreement with those of Chandler, 24 who systematically varied the effect of lumen size in an ear mold and found thresholds reduced by partial occlusion, primarily at high frequencies. When the occlusion was nearly complete, lower frequencies also were affected. Schow et al/ 6 however, found shifts due to ear-canal collapse most often at 500 and 4,000 Hz and least often at 2,000 Hz. The reason for this discrepancy is riot apparent. Our results are in agreement with those of Schow et aP 6 in that most threshold shifts due to earcanal collapse are 15 dB or less, although shifts as large as 30 dB also were observed. Thus, management of ear-canal collapse is an important clinical consideration. The results of this study as well as those by Chaiklin and McClelland8 indicate that the use of circumaural cushions provides the most practical solution to ear-canal collapse. This work was supported in part by the Nebraska Center on Aging, Omaha. Richard Lippman, PhD, made suggestions throughout the project and critiqued the maimscript; Walt Jesteadt, PhD, assisted with the data analysis and plots; Marjorie Leek, PhD, and John Brandt, PhD, made editorial comments; and Melanie Pruitt, MA, Roger McGargill, PhD, and Carl Thompson, PhD, helped locate individuals with earccanal collapse. References Atherton Inc, 1971. 18. Studebaker GA: Interest variability and the air-bone gap. J Speech Hear Disord 1967; 32:82-86. 19. Wilbur LA: Calibration: Pure-tone, speech, and noise signals, in Katz J (ed): Handbook of Clinical Audioloyy. Baltimore, Williams & Wilkins Co, 1972. 20. Shaw EAG: Ear-canal pressure generated by circumaural and supra-aural earphones. iAcoust Soc Am 1966;39:471-479. 21. Villchur E: Audiometer-earphone mounting to improve intersubject and cushion-fit reliability. J Acoust Soc Am 1970;48:1387-1396. 22. Michael PL, Bienvenue GR: Calibration data for a circumaural headset designed for hearing testing. J Acoust Soc Am 1976;60:944950. 23. Kruger B, Soloman B, Cohen R: Flat-plate coupler calibration of circumaural audiometric and hi-fi earphones. J Acoust Soc Am 1980; 67:91. 24. Chandler JR: Partial occlusion of the external auditory meatus: Its effect upon air and bone conduction acuity. Lill·ynr;oscope 1964;74:2254. ian Arch Otolaryngoi-Vol 108, June 1982 Ear-Canal Collapse-Marshall & Gossman 361