Effect of different load conditions on a DHS implanted human femur
advertisement

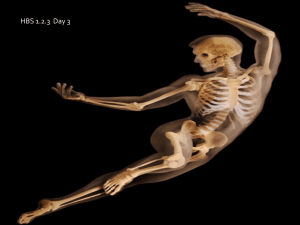
GSTF International Journal of Engineering Technology (JET) Vol.1 No.1, 2012 Effect of different load conditions on a DHS implanted human femur Nooshin S. Taheri, Aaron S. Blicblau, and Manmohan Singh load, with one of load conditions used being the fall loading condition [4]. Another study investigates strain distribution along the proximal femur under six different load conditions e.g. stumbling or mis-stepping [4]. Lotz et al have considered fall and gait loading conditions to interpret stress distribution along the femur in normal and osteoporosis bone [5]. Single leg stance condition is a configuration which is present in almost every daily activity, therefore by identifying the stress –strain state of this condition we will be able to have a better understanding of the implant behavior under such a load. Impact from a fall on the implanted femur is very crucial, by investigating this load configuration; we might be able to prevent the failure caused by impact from a fall on the hip. Identifying the cause of failure due to load conditions is very crucial to preclude post-operative fracture or failure of device and second operation especially when the targeted populations are the elderly. In a study comparing the gamma nail with DHS, the result relating stress distribution established no advantages of one to the other device [8]. It is worth mentioning that the Gamma locking nail is more suitable for subtrochanteric fractures along the shaft of femur. An assessment in performance of a short plate compression screw with DHS, found that DHS has better biomechanical function to minimize the credibility of mechanical failure [9]. DHS proved to offer better stability and prevention of fixation failure in proximal femur rotational osteotomy in a finite element study corresponding to the clinical observations [10]. However, the failure of this device is the main concern in choosing the proper implant for specific fracture. One of the complications involving DHS is the cut out of the lag screw from the head of femur [11]. The main factor of this problem is known to be the position of lag screw within the head of femur [12]. According to the research studies, dynamic Hip Screw ( DHS ) is the most commonly used implant for pertrochanteric fractures [6]. Dynamic Hip Screw is a type of extramedullary fixation device which is designed to stabilize stable fractures. There are a number of biomechanical, clinical and finite element studies which have compared intra and extramedullary implants [7]. The objective of present study is to establish the role of fall loading condition on the implanted femur in terms of stress distribution. This work is a follow up of work conducted on the selection of materials for a DHS [13] under fall conditions. Abstract— As a result of improving life expectancy, the number of elderly people affected by hip fracture is increasing. Hip fracture treatments are different due to different types of fractures. Internal fixation is one of the most reliable treatments for the hip fractures. Nearly half of the fractures are introchanteric fractures that are best treated by with a Dynamic Hip Screw (DHS). However, there are concerns in using DHS, due to the rate of the failure of up to a third of all operations due to the cut out of the lag screw from the head of the femur. Revision surgery is essential if the cut out of the lag screw happens. This study carried out a finite element analysis to establish the effects of different load conditions on the DHS implanted bone system for single-leg stance and fall and the conditions for failure. Index Terms—hip configurations; failure fracture; dynamic hip screw; load I. INTRODUCTION A S a result of population aging the number of hospitalization for hip fracture is still rising, according to data from statistics in Australia 41.9% increase in men and 31.2% in women. As for worldwide figures, it is likely that the numbers rise from 1.3 million hip fractures in 1990 to 7.3 – 21.3 million by 2050 [1]. Applying loads in specific directions on the hip joint after surgery would lead to failure of implant, or in a more traumatic situation often fall would cause postoperative fracture. Falls or stumbling causing hip fractures are causing 60 % of the injuries [2]. In particular, falls in persons aged 65 and over are the main source of their death, admission to hospital and emergency units. Commonwealth and state health authorities have considered fall prevention programs as one of their main concern areas in the elderly [2]. We chose linear analysis on implanted human femur to investigate the stress distribution under fall load condition and compare it with the single leg stance case as a reference. Keyak, et al. [3] performed a finite element analysis on the intact femur to determine the force directions related to the lowest fracture Manuscript received May 25, 2012. N.S.Taheri was a graduate student at Swinburne University of Technology, faculty of Engineering and Industrial Sciences, Hawthorn, Australia A.S.Blicblau is with Swinburne University of Technology, faculty of Engineering and Industrial Sciences, Hawthorn, Australia (e-mail: ablicblau@swin.edu.au). M.Singh is with the Swinburne University of Technology, faculty of Engineering and Industrial Sciences, Hawthorn, Australia. 141 © 2012 GSTF GSTF International Journal of Engineering Technology (JET) Vol.1 No.1, 2012 In this paper we have considered implanted femur instead of the intact or fractured femur to investigate the effect of force direction in both single –legged stance and fall loading conditions. In no case have an implanted femur under fall loading condition been investigated in the literature. In particular we addressed the following tasks: identification of the location of peak stresses within the implanted femur in single-legged stance and impact from a fall; assessment of the effect of direction of load on the implanted femur under different load conditions; and analysis of the biomechanical behavior of dynamic hip screw during walking and fall. structural integrity of different implants against each other helps to give guidance to surgeons to make the right choice [9, 12, 15]. A three- dimensional FE model of the right femur to include DHS implant was considered, as shown in Fig 1 to assess the level of stress developing in the implanted bone. The model of DHS was created by means of Unigraphics using the geometry and dimensions from the DHS manufacturer, SYNTHES [16]. The implant has four distal screws which are in different planes to have better biomechanical performance compared to the previous designs. The angle of 135⁰ between the plate and the lag screw is there to ensure stability in fractured femur. The length of the plate is about 38 mm. DHS device generates minimum irritation to the soft tissue [7]. The geometry of a standard femur has been created from a series of CT images. The femur model was accurately modeled for screw dimensions and orientation of the DHS in the Pro Engineering program. Then the 3-D model of featured bone and DHS as an assembly was imported into an ANSYS pre-processor. Lotz et al have applied a modulus of 17 GPa to thickest layer of the bone and 0.45 as Poisson’s ratio [5]. In another study a modulus 14.217 GPa was chosen for the cortical bone and 0.10 GPa for trabacular bone, again 0.3 was employed for the Poisson's ratio [17]. Brown [12], similarly used a modulus of 17 GPa for cortical bone and 1.3 GPa for cancellous bone in the femoral head, as well as 0.3 for Poisson ratio. In work on using a Gamma nail for implants, the properties of the femur were Young’s modulus of 17.0 GPa for cortical bone and 0.3 for the Poisson`s ratio [18]. Although there are some other alternatives for the material of the implant, stainless steel was appointed to the DHS device for its material properties, with the value of 2l0 GPa for its modulus of elasticity and 0.3 for its Poisson`s ratio. In order to simplify the model and have a better mesh for the implant, the threads and the tips of implant screws were not modeled. The 3-D model of femur was considered homogeneous, linear, and elastic exhibiting isotropic properties. The loading simulation of the bone implant system was performed using ANSYS (version 11.) computer software. ANSYS provides a list of various contact types for such assemblies like femur-implant systems. Fully bonded contact is chosen for this case to allow load transfer between the plate and the femur model. The contact area of the bone DHS implant assembly body is shown in Figure 2. For convergence of the model, with mesh refinement, the von Misses stresses differed by less than 5%. Using this approach, the two requirements for the consistency of the model, compatibility, and stability are defined. According to Lax-Wendrof theorem, consistency and stability imply convergence [19]. II. MODELLING AND ANALYSIS A. Modelling Investigating biomechanical behavior of the femur to better understand its properties is a hard task since the femur is very complicated in shape, material properties, geometry, porosity, density and furthermore femur is a live part which is changing all the time. Among all methods finite element analysis is most reliable and its validity is supported by comparisons by other researchers’ work [7,8,9,17,18]. Experimental methods face shortcomings of the specimen and different types of analysis on different parts of femur which will cause specific limitation. To assess different material behavior like stress, strain and total deformation at the same time on one single specimen is only possible in finite element analysis. Finite element could also deal with complicated material properties linearity and nonlinearity of the analysis. Fig. 1. 3-D model of femur included DHS Cheal et al [14] have performed a finite element analysis to establish the role of loads and prosthesis material properties on the proximal femur in total hip replacement. In most comparative studies using finite element to investigate the 142 © 2012 GSTF GSTF International Journal of Engineering Technology (JET) Vol.1 No.1, 2012 B. Loads Two load regimes were considered to analyze biomechanical behavior of implanted femur. Load condition 1 simulating single-legged stance phase of gait, borrowed from literature [10]. In all daily activities stance phase of the gait cycle is most seen, like stair climbing, stair descending, running ,walking and jogging; this is the main reason most studies consider single legged stance as a basic and important loading condition [20]. The load direction in the single leg stance case is shown in Figure 4. During the gait cycle, every muscle is active at a specific period. The muscle active in single-legged stance phase of gait is the Gluteus medius. The joint contact resultant force and muscular load are applied on two different locations. The muscular load created by the Gluteus medius muscle is applied on the great trochanter area and joint contact force is applied on the femoral head. The direction of two forces are opposite with an angle to the femoral shaft. (Table 2) Load condition 2 represents impact from a fall on the side from standing. The direction of loads to replicate impact from a fall is a medially directed load applied to the great trochanteric and an equal and opposite laterally directed load applied to the femoral head. This specific fall load condition was used by Backman to create fractures to represent real cases of fractures in vitro [21]. The fall is assumed to be from standing height and was carried out such that the lateral aspect of the hip came in direct contact with the floor. The average force evaluate over the great trochanter after experiencing fall from standing was nearly 11 times body weight (considering 7350N in this case) [5]. However, since our work is considering the implanted femur after the operation, we assumed the impact from fall to be 4.5 times body weight, with resulting failure of the implant, or the fracture of the femur. Another study collected similar values for the load of impact from a fall, under better conditions, which suggest that impact force for fall from standing height is in the range of 10 to 17 times body weight [22]. In our work, a global Cartesian axis set was defined with a z- axis parallel to the long axis of the femur shaft and implant plate, the x- axis along the anterial to posterial of the femur and the y-axis in medial to lateral directions. In Table 2 the direction and magnitude of loadings are shown. The femur is restrained at the distal end. The best result is achieved when the distance from the trochanter is about 38 mm. The boundary condition is defined in simulation by fixed support [13]. Fig. 2. The contact area of bone implant assembly A complicated geometry like femur will require a fine mesh prior to solving to verify mesh control setting after the convergence 3 mm size element was applied. We chose fournoded tetrahedral elements throughout the assembly. In total, for the model of the bone DHS implant system, the number of nodes of the DHS and the femur assembly were 45935 with 27147 elements, as shown in Figure 3. TABLE 2 FORCE APPLIED ON MODEL (N) Direction of loads A-P M-L Fig. 3. View of mesh on the bone implant system Moreover, the number of elements used for the intact bone and the DHS implanted bone model in the FEA simulation is listed in table 1 CASE S-I Stance phase1 1 Joint 211 453 2165 2 Trochanter 195 485 -1384 Impact from fall2 3 Joint 1690 -2700 1150 4 Trochanter -1690 2700 -1150 1 stance phase adapted from [10], 2fall data adapted from [5] M–L Medial to lateral, A–P anterior to posterior, I–S inferior to superior TABLE 1 NUMBER OF ELEMENTS AND NODES FOR BOTH 3D MODELS Item Intact bone Implanted bone Nodes 25544 62424 Element 14768 37061 143 © 2012 GSTF GSTF International Journal of Engineering Technology (JET) Vol.1 No.1, 2012 close. The deformation of the proximal femur during fall on the side of hip was much higher. In intact bone during fall, the deformation is 23.503 mm. If someone experiences a fall after the operation of internal fixation, total deformations would be around 54.794 mm in head of femur region, which might seem unrealistic. We changed the direction of load on the head of the femur to the z direction only, the displacement of the femur decreased by 4.17 % as a value of 13.011 mm. The result shows the direction of load has a significant role on the displacement of the femur compared to its magnitude. (Fig5). The yield criterion chosen was the von Mises criterion assuming isotropic behavior of cortical bone. The von Mises stress gives an indication of the elastic shear strain energy in element considered for elastic breakdown [12]. The implanted femur with DHS device is considered under the fall loading and stance phase to investigate the role of DHS in these conditions after the surgery to establish the strength of the implant and the level of stress it tolerates. Fig. 4. Load direction in single- legged stance case Fig. 5. von Mises stress in intact femur in fall case 3 III. RESULTS TABLE 3 A. von Mises Stress Distribution The von Mises stress distributions on the surface of the implanted femur are shown in Fig.5. The results show that the peak stress levels are on the DHS device: 128.05 MPa in stance and 1127.8 MPa in fall. It shows that DHS as a bearing load device carries the load in the system. Most of the load is carried by the DHS plate responding to the force transmission between the DHS devise and the femur at the contact point. Further analysis revealed that high stresses were located in the region of posterior – anterior of the neck as well as the distal end of the femur on impact from a fall. On the contrary, during stance phase of gait, the base of the neck and the area of the superior neck were stressed. The patterns of high stress in the femur increased as the axial plane moved distally along the femur in impact from a fall in intact bone. Interestingly, in the implanted femur system trend was towards high local stress in the area of the lateral plate of DHS and less at the distal end. COMPARISON OF THE VON MISES STRESS AND PRINCIPAL STRESSES Case1 Case2 Case3 Case4 von-Mises 78 154 554 923 Maximum principal -18 to52 -5 to 89 -102 to482 -33 to 398 Minimum principal -67 to12 -58 to 16 -602 to 60 -924 to 60 Stress (MPa) C. Principal Stress Distribution The principal stresses for all cases are shown in Table 3. In stance case, the principal stresses were concentrated within the intertrochanteric region of the femur. In contrast on impact from a fall maximum principal stress are located in contact area of the implant and bone as shown in Fig 7. However, during fall, intact bone experienced maximum principal stress around base of the neck and intertrochanteric region of the bone that makes sense, since most fractures are in that area. During fall, compressive stresses are also around anterior –superior area of the neck B. Deformation of the femur Representative deformation patterns of system and undeformed model are shown in figure 6. In case of stance phase of gait loading the overall deflection had a value of 3.607 mm in the implanted femur. The deflection of intact femur under the same loading was 2.911 mm, which are very D. Stress Distribution on Screws Lag screw insertion hole was heavily stressed during stance loading. 52.389 MPa, which is under the yield strength of the 144 © 2012 GSTF GSTF International Journal of Engineering Technology (JET) Vol.1 No.1, 2012 material. As for the distal screws, the topmost screw was under the highest stress when compared with the other screws. However, during fall the distal screws were under heavy stress: 281.36 - 462.76 MPa. Because of the load direction, stress distribution was the highest in anterior positioned screws. The lag screw hole and the lateral side of the plate had the peak stress values critical and weak parts of DHS are fourth distal screw and plate. The maximum principal stresses are in contact area of the plate and bone is shown in Figure 7. Lateral side of the plate generates the highest stress concentration especially in model-SS. [23]. Our results relating to the high stresses in lateral side of DHS plate is in consistent with the findings of other researchers [7, 24, 25]. The high stresses at the distal end of the intact femur and implanted femur observed in our study is similar to findings of other similar studies [14]. Our study revealed that around fourth distal screw the highest concentration of stress are developed which is in consistent with other DHS studies [24,25]. These results show the significant role of directions and magnitudes of loads applied on the implanted femur after internal fixation during daily activities. Better knowledge of the biomechanical factors that rules the risk of hip fracture and implant failure Identifying weak areas of implant under important load conditions also assists in developing enhanced and improved design and materials of implants. Fig. 6. Deformation patterns of system and undeformed model. V. CONCLUDING COMMENTS The main objective of this study was to determine stress distribution in two different load conditions on femur-DHS system, during gait and impact from a fall. Results indicate that there are significant differences between gait and falls in both magnitude and pattern of stress in both intact and implanted femur. During gait, the stress patterns are within the infer-medial neck. On impact from a fall, however, the stress patterns were very different to the gait; it appears the principal source of strength is in sub-capital region of neck. In case of impact from a fall on implanted femur, it seems that the peak stresses are located mainly in the contact area of the DHS and the shaft of the femur less in the neck. This could mean the failure of the implant or even a second fracture, which we were not able to confirm as limitation of software is most likely. Our study faced potential limitation, which our finite element model was restricted to linear, isotropic material behavior. The data show significant post-yield non-linear performance for both cases, which this implicates failure of the implant or second fracture for the femur implant system. In intact bone, cases are comparable with the literature, which were used as reference, and our data was in agreement with their results. Fig. 7. Maximum principal stresses are in contact area of the plate and bone. IV. DISCUSSION This study provides a mechanical evaluation before and after internal fixation by means of finite element analysis and application of stance phase of gait and stair descent loading conditions. The results indicate the significant changes in biomechanical behavior of the proximal femur after internal fixation. During stance, stress rise is observed after internal fixation, however, maximum stress values are still below the yield stress values of implant and bone materials. Nevertheless, the stance case induces more stress on the implanted femur. The stress rise in implanted femur during stance is nearly more than that during stair descent replication. There are few studies relating to simulation of stair descent loading condition on the implanted femur with DHS. The present results can be used as a reference for the implanted femur with DHS for stair descent. As a result of an impact, the implanted femur experiences very high magnitudes of stress particularly in the DHS parts. The results reveal that the REFERENCES [1] [2] [3] 145 B. Gullberg, O. Johnell,and J. A. Kanis,"World-wide projections for hip fracture.," Osteoporos International, vol. 7, pp. 407-413, 1997. R. Hockey and E. Miles, "Falls in older people," Injury Bulletin, 1999, Available http://www.qisu.org.au/modcore/PreviousBulliten/backend/upload_file/i ssue056.pdf. J. H. Keyak, H.B.Skinner and J. A. Fleming, "Effect of force direction on femoral fracture load for two types of loading conditions," Journal of orthopaedic reserarch, vol. 19, pp. 539-544, Jul 2001. © 2012 GSTF GSTF International Journal of Engineering Technology (JET) Vol.1 No.1, 2012 [4] [5] [6] [7] [8] [9] [10] [11] [12] [13] [14] [15] [16] [17] [18] [19] [20] [21] [22] S. N. Robinovitch, W. C. Hayes, and T. A. McMahon, "Prediction of femoral impact forces in falls in the hip.," Journal of Biomechanical Engineering-Transactions of the Asme, vol. 113, pp. 366-374, Nov 1991. [23] N. Y. Otsuka and J. Schatzker, "Subcapital fracture of the hip after internal fixation of an intertrochanteric fracture," Archives of Orthopaedic and Trauma Surgery, vol. 112, pp. 69-70, 1993. [24] E. Sim, W. Freimuller, and T. J. Reiter, "Finite element analysis of the stress distributions in the proximal end of the femur after stabilization of a pertrochanteric model fracture: a comparison of two implant," Injury, vol. 26, pp. 445-449, 1995. [25] E. Peleg, R. Mosheiff, M. Leibergall, and Y. Mattan, "A short plate compression screw with diagnal bolts; A biomechanical evaluation performed experimentally and by numerical computation," Clinical Biomechanics, vol. 21, pp. 963-968, June 2006. L. Cristofolini, "Strain disribution in the proximal human femoral metaphysist," Journal of engineering in medicine, vol. 223, APR 2009 2009. J. C. Lotz, E. J. Cheal, and W. C. Hayes, "Stress distributions within the proximal femur during gait and falls- Implications for osteoporotic fracture.," Osteoporosis International, vol. 5, pp. 252-261, 1995. S. E. Brandt, S. Lefever, H. M. J. Janzing, P. L. O. Broos, P. Pilot, and B. J. J. Houben, "Percutaneous compression plating (PCCP) versus the dynamic hip screw for pertrochanteric hip fractures: preliminary results," Injury-International Journal of the Care of the Injured, vol. 33, pp. 413-418, Jun 2002. S. Sowmianarayanan, A. Chandrasekaran, and R. K. Kumar, "Finite element analysis of a subtrochanteric fractured femur with dynamic hip screw, dynamic condylar screw, and proximal femur nail implants - a comparative study," Proceedings of the Institution of Mechanical Engineers Part H-Journal of Engineering in Medicine, vol. 222, pp. 117-127, 2008. E. Sim.,W. Freimuller., and T. J. Reiter., "Finite element analysis of the stress distributions in the proximal end of the femur after stabilization of a pertrochanteric model fracture: a comparison of two implant," Injury, vol. 26, pp. 445-449, 1995. E. Peleg, R. Mosheiff, M. Leibergall, and Y. Mattan, "A short plate compression screw with diagnal bolts-- A biomechanical evaluation performed experimentally and by numerical computation," Clinical Biomechanics, vol. 21, pp. 963-968, June 2006. W-P. Chen, C-L. Tai.,C-H. Shih.,P-H. Hsieh, M-C. Leou, and M. S. Lee, "Selection of fixation devices in proximal femur rotational osteotomy: clinical complications and finite element analysis," Clinical Biomechanics, vol. 19, pp. 255-262, December 2004. F. Bonnaire.,A. Weber,O. Bosl, C. Eckhardt, K.Schwieger,and B. Linke,"Cutting out in pertrochanteric fractures-problem of osteoporosis?," Unfallchrurg, vol. 110, pp. 425-432, May 2007. C. J. Brown, C. J. Wang, A. L. Yettram, and P. Procter, "Intramedullary nails with two lag screws," Clinical Biomechanics, vol. 19, pp. 519-525, 2004. N. S. Taheri, A. S. Blicblau, and M. Singh, "Comparative study of two materials for dynamic hip screw during fall and gait loading: titanium alloy and stainless steel," Journal of Orthopaedic Science, vol. 16, pp. 805-813, Nov.2011. E. J. Cheal, M. Spector, and W. C. Hayes, "Role of loads and prosthesis material properties on the mechanics of the proximal femur after total hip-arthroplasty.," Journal of Orthopaedic Research, vol. 10, pp. 405422, May 1992. C. J. Wang, C. J. Brown, A. L. Yettram, and P. Procter, "Intramedullary femoral nails: one or two lag screws? A preliminary study," Medical Engineering & Physics, vol. 22, pp. 613-624, 2000. SYNTHES (2012, May 15). DCS,DHS,LCP, stardrice and vario case. Available http://www.synthes.com/MediaBin/International%20DATA/036.000.68 6.pdf G. J. M. Seral B., J. Cegonino,M. Doblare, and F. Seral, "Finite element study of intramedullary osteosynthesis in the treatment of trochanteric fractures of the hip: Gamma and PFN," Injury, vol. 35, pp. 130-135, 2004. C. J. Wang, A. L. Yettram, M. S. Yao, and P. Procter, "Finite element analysis of a Gamma nail within a fractured femur," Medical Engineering & Physics, vol. 20, pp. 677-683, 1998. C. A. Felippa. (2001). Introduction to finite element methods.Available http://141.105.33.55/~lomov/%D0%B1%D0%B8%D0%B1%D0%BB %D0%B8%D0%BE%D1%82%D0%B5%D0%BA%D0%B0/bigdvd/D VD013/Felippa_C.A._Introduction_to_finite_element_methods_%282001 %29%28en%29%28489s%29.pdf. C.-L. Tai, C-H Shih, W-P Chen, S-S Lee, Y-L Liu, P-H Hsieh and W-J Chen, "Finite element analysis of the cervico- trochanteric stemless femoral prosthesis," Clinical Biomechanics, vol. 18, pp. s53-s58, 2003. S.Backman, " The proximal end of the femur: investigations with special reference to the etiology of femoral neck fractures; anatomical studies; roentgen projections; theoretical stress calculations; experimental production of fractures," Act RadiolSuppl., vol. 146, pp.1166, 1957. Nooshin S. Taheri (ME SUT) . Obtained her first degree in mathematics in Iran. She then completed a M.Eng at Swinburne University of Technology where she specialized in in the biomechanical behavior of human femur. Her areas of interest include mathematical modeling, finite element analysis and their applications. Aaron S.Blicblau (BE Monash, ME UNSW). Received his first degree in materials engineering and his second degree in civil engineering materials. He is currently a senior lecturer in the faculty of Engineering and Industrial Sciences at Swinburne University of Technology. His research interests are in Mathematical modeling of engineering processes, failure of engineering materials, engineering education, active learning, project based learning, and syllabus and curriculum development. He is a chartered member of both IE(Aust)and the IMMM well as a member of ASEE Manmohan Singh (MSc Roorkee, PhD Roorkee). Received his MSc and Phd from University of Roorkee in Applied Mathematics. He is currently a senior lecturer in the faculty of Engineering and Industrial Sciences at Swinburne University of Technology. His research interests are Mathematical Biology, Numerical Methods, and Theoretical Astrophysics. He is a member of the Australian Mathematical Society, and the Society for Mathematical Biology. 146 © 2012 GSTF